head injuries
TRANSCRIPT

Common major trauma4 million people experience head trauma
annually Severe head injury is most frequent cause of trauma death
At Risk population Males 15-24 years Infants Young Children Elderly
INTRODUCTION TO HEADINJURIES

TIME IS CRITICAL Intracranial Hemorrhage Progressing Edema
Increased ICP Cerebral Hypoxia Permanent Damage
Severity is difficult to recognize Subtle signs Improve differential diagnosis
Improves survivability
INTRODUCTION TO HEAD INJURIES

Mechanism of Injury Blunt Injury
Motor vehicle collisions Assaults Falls
Penetrating Injury Gunshot wounds Stabbing Explosions
PATHOPHYSIOLOGY OFHEAD INJURY

Head InjuryCranial InjuryBrain Injury
DIFFERENT TYPES OF INJURY

HEAD INJURY
Open • Skull compromised
and brain exposed
Closed• Skull not compromised
and brain not exposed
5Head Trauma -

Contusions
Lacerations
Avulsions
Significant Hemorrhage
SCALP INJURY

HEAD INJURIES
Scalp wound
• Highly vascular, bleeds briskly Shock: child may develop Shock: adult another cause
• Management No unstable fracture:
direct pressure, dressings Unstable fracture: dressings, avoid direct pressure
7Head Trauma -

Skull fracture• Linear nondisplaced
• Depressed
• Compound
Suspect fracture• Large contusion or darkened swelling
Management• Dressing, avoid excess pressure
HEAD INJURIES
8Head Trauma -

Trauma must be extreme to fracture Linear Depressed Open Impaled Object
CRANIAL INJURY

Basal Skull Unprotected Spaces weaken
structure Relatively
easier to fracture

Basal Skull Fracture Signs Battle’s Signs
Retroauricular Ecchymosis Associated with fracture of
auditory canal and lower areas of skull
Raccoon Eyes Bilateral Periorbital
Ecchymosis Associated with orbital
fractures
CRANIAL INJURY

BASILAR SKULL FRACTURE
Battle’s sign Raccoon eyes
12Head Trauma -

Basilar Skull Fracture May tear dura
Permit CSF to drain through an external passageway May mediate rise of ICP Evaluate for “Target” or “Halo” sign
CRANIAL INJURY

CRAINIAL INJURIES
Penetrating trauma
14Head Trauma -
Bullet fragments

Head Trauma - 15
Forces that cause skull fracture can also cause brain injury.

As defined by the National Head Injury Foundation “a traumatic insult to the brain capable of producing physical,
intellectual, emotional, social and vocational changes.”
BRAIN INJURY

BRAIN INJURY
Response to injury
• Swelling of brain Vasodilatation with increased blood volume Increased ICP
• Decreased blood flow to brain Perfusion decreases Cerebral ischemia (hypoxia)
17Head Trauma -

Altered Mental Status Altered orientation Alteration in personality Amnesia
Retrograde Antegrade
Cushing’s Reflex Increased BP Bradycardia Erratic respirations
SIGNS & SYMPTOMS OF BRAIN INJURY
Vomiting Without nausea Projectile
Body temperature changes
Changes in pupil reactivity
Decorticate posturing

Pathophysiology of Changes Frontal Lobe Injury
Alterations in personality Occipital Lobe Injury
Visual disturbances Cortical Disruption
Reduce mental status or Amnesia Retrograde
Unable to recall events before injury Antegrade
Unable to recall events after trauma “Repetitive Questioning”
Focal Deficits Hemiplegia, Weakness or Seizures
SIGNS & SYMPTOMS OF BRAIN INJURY

ClassificationDirect
Primary injury caused by forces of trauma Indirect
Secondary injury caused by factors resulting from the primary injury

BRAIN INJURY
Direct brain injury
• Immediate damage due to force
• Coup and contracoup
• Fixed at time of injury
Management
• Directed at prevention
21Head Trauma -

Coup Injury at site of impact
Contrecoup Injury on opposite side
from impact
DIRECT BRAIN INJURY TYPES
BRAIN INJURY
Indirect brain injury
• Results from hypoxia or decreased perfusion
• Response to primary injury
• Develops over hours
Management
• Good prehospital care can help prevent
23Head Trauma -

Focal Occur at a specific location in brain Differentials
Cerebral Contusion Intracranial Hemorrhage
Epidural hematoma Subdural hematoma
Intracerebral HemorrhageDiffuse
Concussion Moderate Diffuse Axonal Injury Severe Diffuse Axonal Injury
DIRECT BRAIN INJURY CATEGORIES

Cerebral Contusion Blunt trauma to local brain tissue Capillary bleeding into brain tissue Common with blunt head trauma
Confusion Neurologic deficit
Personality changes Vision changes Speech changes
Results from Coup-contrecoup injury
FOCAL BRAIN INJURY

BRAIN INJURIES
Cerebral contusion
• Bruising of brain tissue Swelling may be rapid and severe
• Level of consciousness Prolonged unconsciousness,
profound confusion or amnesia
• Associated symptoms Focal neurological signs May have personality changes
26Head Trauma -

Epidural Hematoma Bleeding between dura mater
and skull Involves arteries
Middle meningeal artery most common
Rapid bleeding & reduction of oxygen to tissues
Herniates brain toward foramen magnum
FOCAL BRAIN INJURYINTRACRANIAL HEMORRHAGE

INTRACRANIAL HEMORRHAGE
Acute epidural hematoma • Arterial bleed
Temporal fracture common Onset: minutes to hours
• Level of consciousness Initial loss of consciousness “Lucid interval” follows
• Associated symptoms Ipsilateral dilated fixed pupil, signs of increasing ICP, unconsciousness, contralateral
paralysis, death
28Head Trauma -

Subdural Hematoma Bleeding within meninges
Beneath dura mater & within subarachnoid space
Above pia mater Slow bleeding
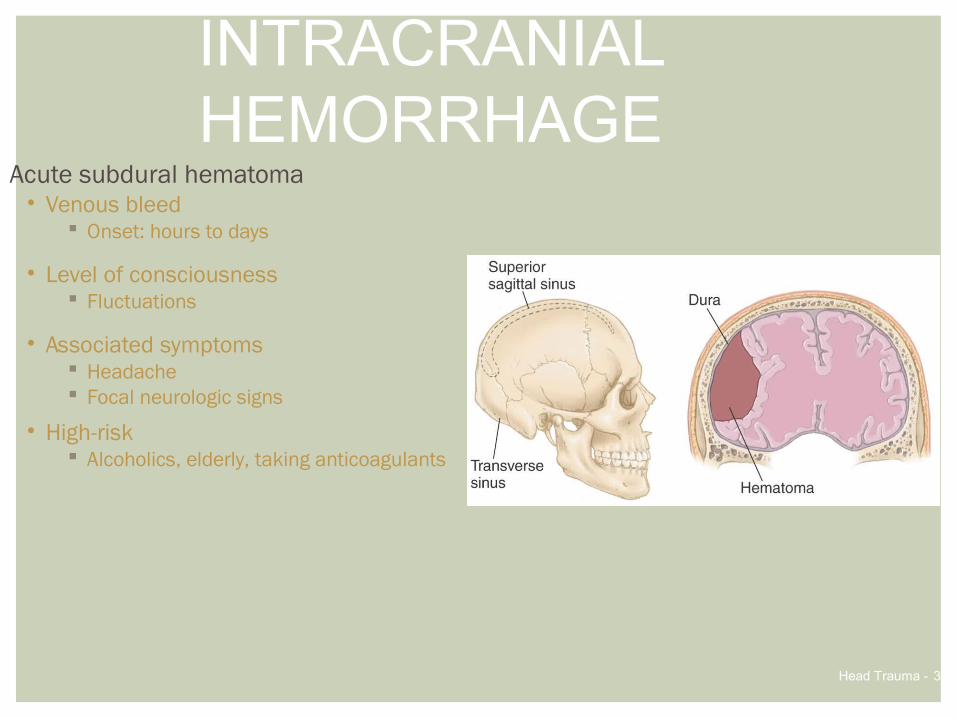
Superior sagital sinus Signs progress over several days
Slow deterioration of mentation
FOCAL BRAIN INJURYINTRACRANIAL HEMORRHAGE
INTRACRANIAL HEMORRHAGE
Acute subdural hematoma• Venous bleed
Onset: hours to days
• Level of consciousness Fluctuations
• Associated symptoms Headache Focal neurologic signs
• High-risk Alcoholics, elderly, taking anticoagulants
30Head Trauma -

INTRACRANIAL HEMORRHAGE
Intracerebral hemorrhage
• Arterial or venous Surgery is often not helpful
• Level of consciousness Alterations common
• Associated symptoms Varies with region and degree Pattern similar to stroke Headache and vomiting
31Head Trauma -

Intracerebral Hemorrhage Rupture blood vessel within the brain Presentation similar to stroke symptoms Signs and symptoms worsen over time
FOCAL BRAIN INJURYINTRACRANIAL HEMORRHAGE

Due to stretching forces placed on individual nerve cellsPathology distributed throughout brainTypes
Concussion Moderate Diffuse Axonal Injury Severe Diffuse Axonal Injury
DIFFUSE BRAIN INJURY

Mild to moderate form of Diffuse Axonal Injury (DAI) Nerve dysfunction without anatomic damage
Transient episode of Confusion, Disorientation, Event amnesia
Suspect if patient has a momentary loss of consciousness
Management Frequent reassessment of mentation ABC’s
DIFFUSE BRAIN INJURY
CONCUSSION

BRAIN INJURIES
Concussion
• No structural injury to brain
• Level of consciousness Variable period of unconsciousness or confusion Followed by return to normal consciousness
• Retrograde short-term amnesia May repeat questions over and over
• Associated symptoms Dizziness, headache, ringing in ears, and/or nausea
35Head Trauma -

“Classic Concussion”Same mechanism as concussion
Additional: Minute bruising of brain tissue
UnconsciousnessMay exist with a basilar skull fractureSigns & Symptoms
Unconsciousness or Persistent confusion Loss of concentration, disorientation Retrograde & Antegrade amnesia Visual and sensory disturbances Mood or Personality changes
DIFFUSE BRAIN INJURY
MODERATE DIFFUSE AXONAL INJURY

BRAIN INJURIES
Diffuse axonal injury
• Diffuse injury Generalized edema No structural lesion Most common injury from
severe blunt head trauma
• Associated symptoms Unconscious No focal deficits
37Head Trauma -

Brainstem InjurySignificant mechanical disruption of nerve
cells Cerebral hemispheres and brainstem
High mortality rateSigns & Symptoms
Prolonged unconsciousness Cushing’s reflex Decorticate or Decerebrate posturing
DIFFUSE BRAIN INJURY
SEVERE DIFFUSE AXONAL INJURY

BRAIN ANATOMY
Intracranial volume
• Brain
• CSF
• Blood vessel volume Dilatation with high pCO2
Constriction with low pCO2
Slight effect on volume
39Head Trauma -

Cranial volume fixed 80% = Cerebrum, cerebellum & brainstem 12% = Blood vessels & blood 8% = CSF
Increase in size of one component diminishes size of another Inability to adjust = increased ICP
INTRACRANIAL PERFUSION

Compensating for Pressure Compress venous blood vessels Reduction in free CSF Pushed into spinal cord
Decompensating for Pressure Increase in ICP Rise in systemic BP to perfuse brain
Further increase of ICP
INTRACRANIAL PERFUSION
ICP BP

Vasculature ConstrictionCerebral EdemaSystolic Blood Pressure
Low BP = Poor Cerebral Perfusion High BP = Increased ICP
Carbon DioxideReduced respiratory efficiency
FACTORS AFFECTING ICP

Role of Carbon Dioxide Increase of CO2 in CSF
Cerebral Vasodilation Encourage blood flow Reduce hypercarbia Reduce hypoxia
Contributes to ICP Reduced levels of CO2 in CSF
Cerebral vasoconstriction Results in cerebral anoxia
INTRACRANIAL PRESSURE


Increased pressure Compresses brain tissue
Herniates brainstem Compromises blood supply Signs & Symptoms
Upper Brainstem Vomiting Altered mental status Pupillary dilation
Medulla Oblongata Respiratory Cardiovascular Blood Pressure disturbances
PRESSURE & STRUCTURAL DISPLACEMENT

Upper Brainstem Compression Increasing blood pressure Reflex bradycardia
Vagus nerve stimulation Cheyne-Stokes respirations Pupils become small and reactive Decorticate posturing
Neural pathway disruption
SIGNS & SYMPTOMS OF BRAIN INJURYPHYSIOLOGICAL CHANGES

Middle Brainstem Compression Widening pulse pressure Increasing bradycardia CNS Hyperventilation
Deep and Rapid Bilateral pupil sluggishness or inactivity Decerebrate posturing
SIGNS & SYMPTOMS OF BRAIN INJURYPHYSIOLOGICAL CHANGES

Lower Brainstem Injury Pupils dilated and unreactive Ataxic respirations
Erratic with no pattern Irregular and erratic pulse rate ECG Changes Hypotension Loss of response to painful stimuli
SIGNS & SYMPTOMS OF BRAIN INJURYPHYSIOLOGICAL CHANGES

Physiological Issues Indicate pressure on
CN-III (Oculomotor Nerve) Pressure on nerve causes eyes to be sluggish, then dilated, and finally fixed
Reduced peripheral blood flow
Pupil Size & Reactivity Reduced Pupillary Responsiveness
Depressant drugs or Cerebral Hypoxia Fixed & Dilated
Extreme Hypoxia
SIGNS & SYMPTOMS OF BRAIN INJURYEYE SIGNS

HEAD TRAUMA ASSESSMENT Initial Assessment
Rapid Trauma Exam
Limit patient agitation, straining• Contributes to elevated ICP
Airway• Vomiting very common within first hour• Endotracheal intubation
50Head Trauma -

Head Trauma - 51
Decreased level of consciousnessis an early indicator of
brain injury or rising ICP.

Reactive: ICP increasing
Nonreactive (altered LOC): increased ICP
Nonreactive (normal LOC): not from head injury
PUPILS
Both dilated Nonreactive: brainstem Reactive: often reversible
Unilaterally dilated
52Head Trauma -
Eyelid closure• Slow: cranial nerve III
• Fluttering: often hysteria
Anisocoria

GLASGOW COMA SCALE
Suspect severe brain injury GCS <9
53Head Trauma -
*Decorticate posturing to pain**Decerebrate posturing to pain

EXTREMITY POSTURING
Decorticate• Arms flexed
and legs extended
Decerebrate• Arms extended
and legs extended
54Head Trauma -

INCREASING ICP
55Head Trauma -
Vital Sign Change with Increasing ICP
Respiration Increase, decrease, irregular
Pulse Decrease
BP Increase, widening pulse pressure
Cushing’s response• As ICP increases, systolic BP increases• As systolic BP increases, pulse rate decreases

Head Trauma - 56
Early effortsto maintain brain perfusion
can be life-saving.

THE INJURED BRAIN
Hypoxia• Perfusion decrease causes cerebral ischemia• Hyperventilation increases hypoxia
significantly more than it decreases ICP
Assist ventilation• High-flow oxygen• One breath every 6–8 seconds• SpO2 >95%
• Maintain EtCO2 at 35 mmHg
57Head Trauma -

THE INJURED BRAIN
Hypotension• Single instance increases mortality
Adult (systolic <90 mmHg) 150% Child (systolic < age appropriate) worse
Fluid administration for traumatic brain injury, GCS <9• Titrate to 110–120 mmHg systolic
with or without penetrating hemorrhage to maintain CPP
58Head Trauma -

THE INJURED BRAIN
Cerebral herniation syndrome
• Brain forced downward CSF flow obstructed, pressure on brainstem
• Level of consciousness Decreasing, rapid progression to coma
• Associated symptoms Ipsilateral pupil dilatation, out-downward deviation Contralateral paralysis or decerebrate posturing Respiratory arrest, death
59Head Trauma -

CEREBRAL HERNIATION
Is ICP severe enoughto outweigh cerebral ischemia?
60Head Trauma -

HYPERVENTILATION
Cerebral herniation syndrome• Herniation danger outweighs hypoxia
Indications for hyperventilation• TBI GCS <9 with decerebrate posturing• TBI GCS <9 with dilated or nonreactive pupils• TBI initial GCS <9, then drops >2 points
If signs resolve, stop hyperventilation.
61Head Trauma -

HYPERVENTILATION RATES
Capnography • Maintain EtCO2 <30 mmHg, but >25 mmHg
62Head Trauma -
Age Group Normal Rate Hyperventilation
Adult 8–10 per minute 20 per minute
Children 15 per minute 25 per minute
Infants 20 per minute 30 per minute

THANK YOU