hd - berliner dialyseseminar
TRANSCRIPT

© 2008, Gambro Lundia AB 1
Future development of dialysisWhat is best?
*Berliner Dialyseseminar, 2009
Ingrid Ledebo, Ph.D.Gambro R&D, Lund, Sweden

© 2008, Gambro Lundia AB 2
What is the best dialysis treatment, today and in the future?Survey performed 2007 at:• WCN in Rio de Janeiro• ERA-EDTA in Barcelona• EuRoPD in Helsinki• EDTNA-ERCA in Florence• ASN in San Francisco
Ref: Ledebo, Ronco, NDT Plus, 2009

© 2008, Gambro Lundia AB 3
CAPD/APD
in-center HD/HDF
home and/or self-care HD/HDF
no opinion
What do you consider to be the best initialdialysis treatment for a patient with planned start,today and in the near future?(Assume also chosen by patient, 65 years, one comorbidity)
Q1: Best initial dialysis treatment
Dialysis Opinions 2007

© 2008, Gambro Lundia AB 4
CAPD/APD
in-center HD/HDF (3 times/week)
in-center HD/HDF (>3 times/week)
home and/or self-care HD/HDF (>3 times/week)
no opinion
Q2: Best long-term dialysis treatment
What do you consider to be the best long-termdialysis treatment for the majority of patients,today and in the near future?
Dialysis Opinions 2007
© 2008, Gambro Lundia AB 5
low-flux hemodialysis
high-flux hemodialysis
high-volume hemodiafiltration
high-volume hemofiltration
no opinion
Q3: Best extracorporeal form of dialysis
What do you consider to be the best extracorporeal form of dialysis?
synthetic membrane,ultrapure fluid
synthetic membrane,on-line prepared fluid
Dialysis Opinions 2007

© 2008, Gambro Lundia AB 6
hard evidence, i.e. improved survival
surrogate evidence, i.e. improved markers (CRP, LVH)
soft evidence, i.e. better quality of lifeown/colleagues´ experience
no opinion
Q4: Minimum level of evidence
In order to consider one form of dialysis superior to another, what is the minimum level of evidence you would require?
Dialysis Opinions 2007

© 2008, Gambro Lundia AB 7
What is the best initial dialysis treatment?
Is it…- PD or HD?- in-center or home dialysis?- full-care or self-care dialysis?
CAPD/APD
in-center HD/HDF
home and/or self-care HD/HDF

© 2008, Gambro Lundia AB 8
Starting with HD or PD, the only RCT1232
773
38HD18
5Tx
9 †
PD20
3Tx
5 †
Ref:Korevaar et al, KI 2003
Conclusion: Non-significant difference in QUALY at start,significantly better survival in PD patients after 5 yrs.
HD
PD
© 2008, Gambro Lundia AB 9
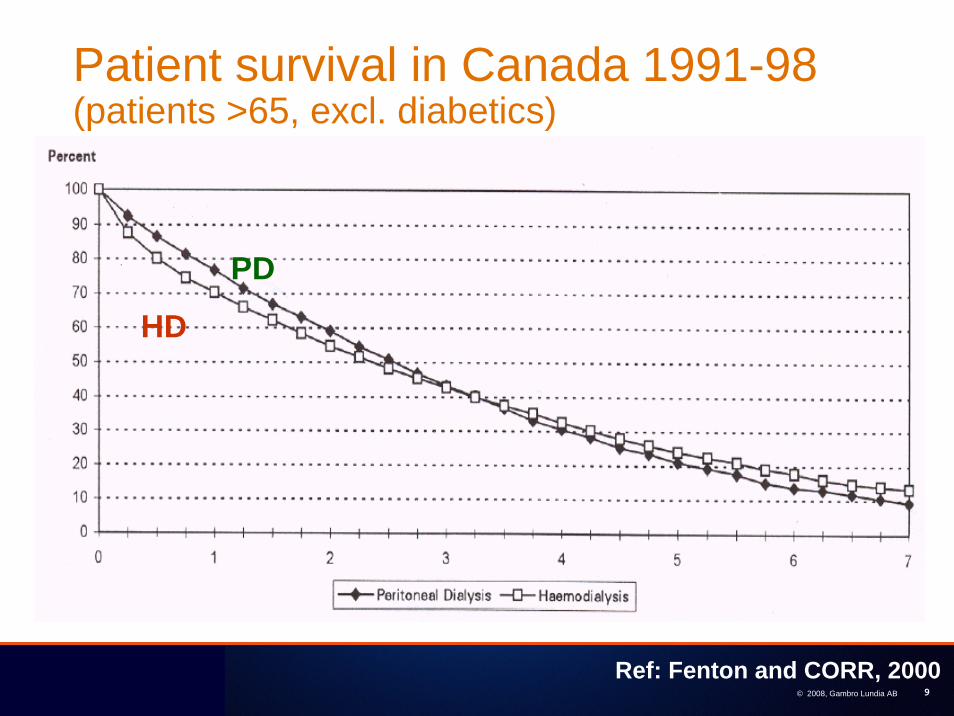
Patient survival in Canada 1991-98 (patients >65, excl. diabetics)
Ref: Fenton and CORR, 2000
PD
HD
© 2008, Gambro Lundia AB 10
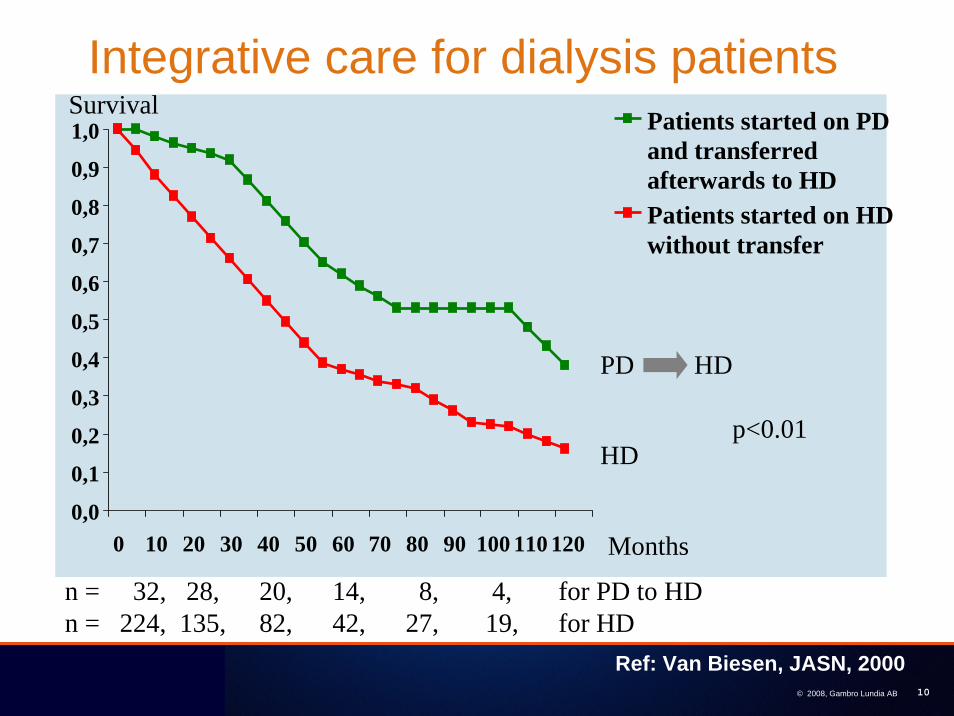
Integrative care for dialysis patients
Ref: Van Biesen, JASN, 2000
0,0
0,1
0,2
0,3
0,4
0,5
0,6
0,7
0,8
0,9
1,0
0 10 20 30 40 50 60 70 80 90 100 110 120
Patients started on PDand transferredafterwards to HDPatients started on HD without transfer
Survival
Months
PD HD
HD
n = 32, 28, 20, 14, 8, 4, for PD to HDn = 224, 135, 82, 42, 27, 19, for HD
p<0.01

© 2008, Gambro Lundia AB 11
Predictors of loss of RRF among incident dialysis patients
Variable Adjusted Odds Ratio
P-value
Female gender 1.45 <0.001
Non-white race 1.57 <0.001
Comorbidity - diabetes 1.82 0.006
- CHF 1.32 0.03
Therapy - PD vs HD 0.35 0.001
- ACE-inhibitor 0.68 <0.001
- Ca channel-blocker 0.77 0.01
Ref: Moist et al, JASN, 2000
National random sample of 1843 incident dialysis patients (1032 on PD) with control for baseline variables. Loss of RRF= urine volume< 200 ml/24 h after 1 yr.

© 2008, Gambro Lundia AB 12
Impact of dialysis mode before Tx
Ref: Goldfarb-Rumyantzev et al, AJKD 2005
RRT mode before Txin relation to HD
Graft survivalHR p
Recipient survivalHR p
PD immediately before Tx 0.97 <0.05 0.94 <0.001
PD predominantly (>50%) 0.97 <0.05 0.96 <0.05
PD only 0.93 <0.002 0.9 <0.001
PD + Tx 0.87 <0.05 0.98 ns
PD + HD 1.09 <0.001 1.1 <0.001
Cox model used for all USRDS data 1990-1999, n=92 844
Conclusion: PD before Tx has a protective effect on graft and recipient survival
© 2008, Gambro 13
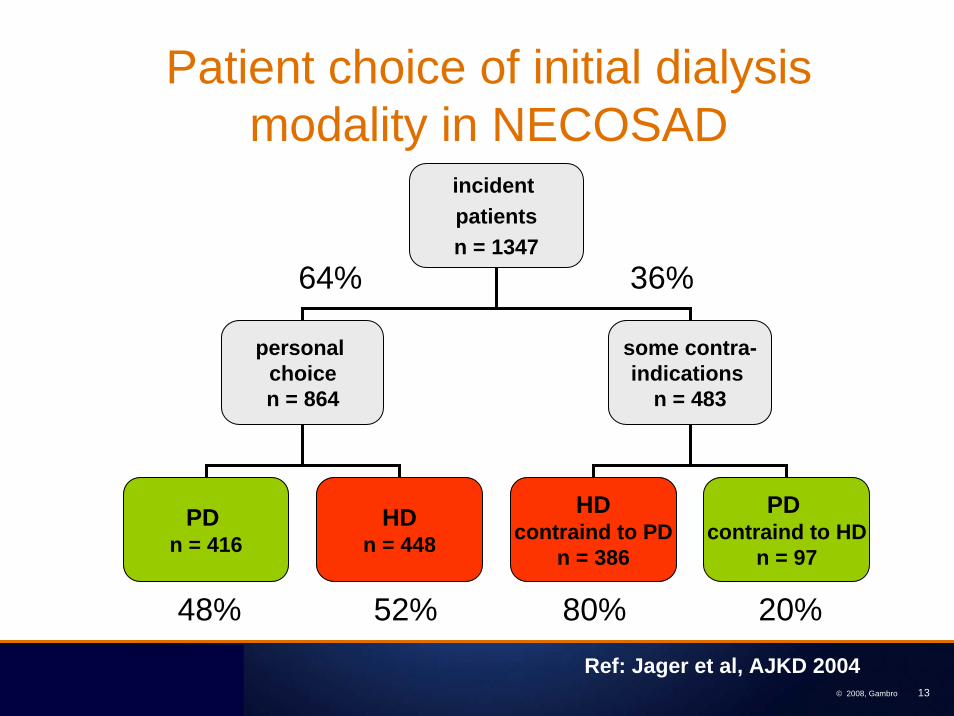
Patient choice of initial dialysis modality in NECOSAD
Ref: Jager et al, AJKD 2004
incident patientsn = 1347
personal choicen = 864
some contra-indications
n = 483
PD n = 416
HDn = 448
HDcontraind to PD
n = 386
PD contraind to HD
n = 97
64% 36%
48% 52% 80% 20%

© 2008, Gambro 14
Impact of predialysis eduction on modality choicein Brussels
incident patients n = 242
pre-dialysis
educationn = 185
in-center HDfor medical
reasonn = 57
preemptivetrans-
plantationn = 8
PDn = 55
HDself-care in satellite
n = 30
HDself-careat home
n = 17
in-center HD
n = 75
76% 24%
self-care dialysis, n = 102 (55%)
Ref: Goovaerts et al, NDT 2005
4% 40%

© 2008, Gambro Lundia AB 15
How are the incident patients treated? USRDS data by first modality
Ref: USRDS 2009 ADR
Total dialysis
HD
PDTx

© 2008, Gambro Lundia AB 16
Best initial dialysis treatmentaccording to 6 595 nephrology professionals
0
10
20
30
40
50
60
CAPD/APD
in-centerHD/HDF
home a/o self-care HD/HDF
no opinion
Ref: Ledebo, Ronco, NDT Plus, 2008

© 2008, Gambro Lundia AB 17
Best initial dialysis treatmentworldwide opinion by nephrology professionals
0
10
20
30
40
50
60
Total (6595)
W Europe(2071)
E Europe(1879)
Asia (888)
Americas(1107)
CAPD/APD in-center HD/HDF home/sc HD/HDF
Ref: Ledebo, Ronco, NDT Plus, 2008

© 2008, Gambro Lundia AB 18
Best initial dialysis treatmentin the world, in W Europe and in Germany in 2007
0
10
20
30
40
50
60
Total (6595) W Europe (2071) Germanic (266)
CAPD/APD in-center HD/HDF home/sc HD/HDF

19
49.5%
22.4%
24.9%
3.2%
CAPD/APD
in-center HD/HDF
home and/or self-care HD/HDF
no opinion
What do you consider to be the best initialdialysis treatment for a patient with planned start,today and in the near future?(Assume also chosen by patient, 65 years, one comorbidity)
Q1: Best initial dialysis treatment

© 2008, Gambro Lundia AB 20
What is the best long-term dialysis treatment?
Is it …- PD or HD/HDF?- in-center or home dialysis?- full-care or self-care dialysis?- conventional or more frequent dialysis?
CAPD/APD
in-center HD/HDF (3 times/week)
in-center HD/HDF (>3 times/week)
home and/or self-care HD/HDF (>3 times/week)

© 2008, Gambro Lundia AB 21
Adjusted five-year survival, by modality & primary diagnosis
Surv
ival
pro
babi
lity
Ref: USRDS 2009 ADR

© 2008, Gambro 22
Survival on Home HD vs in-center HD
0 0,5 1 1,5
adjustment2
adjustment1
unadj.
home HD in-center HD
adj for age, race, sex and PRD
additionally adj for comorbid conditions
n = 3102n = 70
Relative mortality risk with 95% CI
Ref: Woods et al, KI,1996
© 2008, Gambro 23
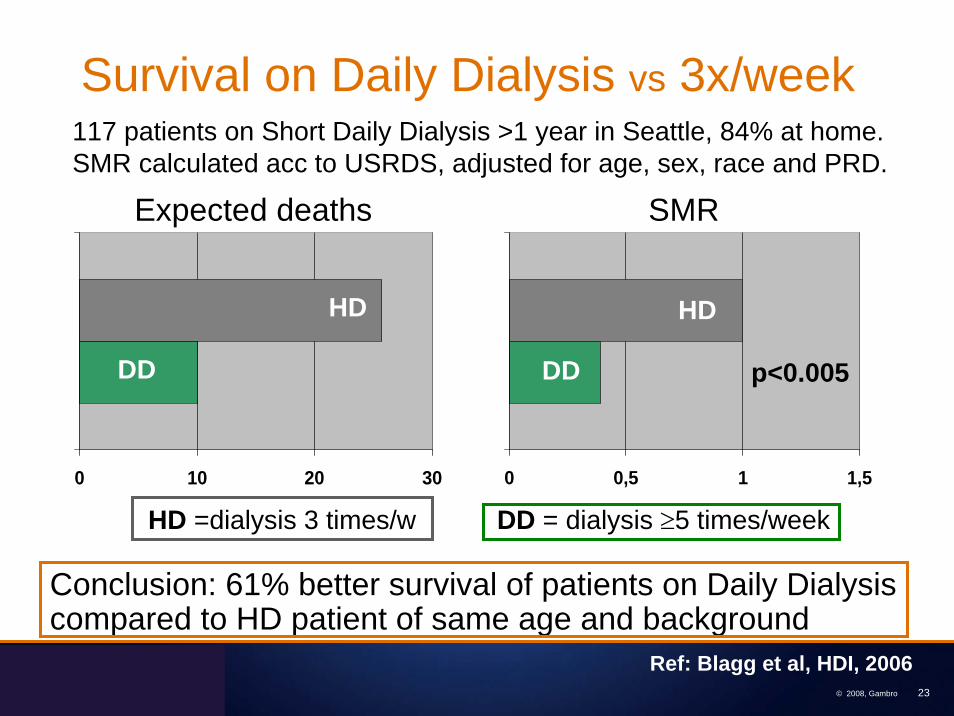
Survival on Daily Dialysis vs 3x/week
0 0,5 1 1,5
Ref: Blagg et al, HDI, 2006
0 10 20 30
Expected deaths SMR
p<0.005DD DD
HD HD
HD =dialysis 3 times/w DD = dialysis ≥5 times/week
117 patients on Short Daily Dialysis >1 year in Seattle, 84% at home. SMR calculated acc to USRDS, adjusted for age, sex, race and PRD.
Conclusion: 61% better survival of patients on Daily Dialysiscompared to HD patient of same age and background

© 2008, Gambro Lundia AB 24
Ref: Kjellstrand et al, NDT 2008
415 patients treated with Short Daily Dialysis
20 – 44 yrs 45 – 64 yrs
USRDSUSRDS
Daily Dialysis
Daily Dialysis
Survival on Daily Dialysis vs USRDS data

© 2008, Gambro Lundia AB 25
Survival on Daily Dialysis at home vs in-center
Daily at home
Daily in-center
USRDS all HD
Ref: Kjellstrand et al, NDT 2008

© 2008, Gambro 26
Survival on frequent nocturnal dialysis
Ref: Pauly et al, NDT 2009
NHD
DTXLTX
Canadian NHD patients amd matched USRDS transplant patients

© 2008, Gambro 27
Frequent dialysis – effect on the heartAuthor Study
typeN LVH (g/m2)
frequent vs conv. dialysis
Time(months)
p
Pierratos 2001
obs 21 162 =>117
no change
154 => 108
145 => 155
92.4 => 85.3
101.8 => 102.8
25 0.02
Ayus2005
cohort 26+51
12 0.001
Culleton2007
RCT 26 +25
6 <0.05

© 2008, Gambro 28
How are the prevalent dialysis patients treated around the world?
Ref: USRDS 2009 ADR

© 2008, Gambro Lundia AB 29
Best long-term dialysis treatmentaccording to 6 595 nephrology professionals
0
10
20
30
40
Ref: Ledebo, Ronco, NDT Plus, 2008
CAPD/APD in-center HD/HDF
home/self-care HD/HDF
no opinion
3x/w >3x/w >3x/w

© 2008, Gambro Lundia AB 30
Best long-term dialysis treatmentworldwide opinion by nephrology professionals
0
10
20
30
40
50
Total (6595)
W Europe(2071)
E Europe(1879)
Asia (888)
Americas(1107)
CAPD/APD in-center HD/HDF, 3x/win-center HD/HDF, >3x/w home/sc HD/HDF, >3x/w
Ref: Ledebo, Ronco, NDT Plus, 2008

© 2008, Gambro Lundia AB 31
Best long-term dialysis treatment?opinion vs reality
0
10
20
30
40
50
60
70
80
90
100
CAPD/APD
in-center HD/HDF
3x/w >3x/w
home/self-care HD/HDF
0
10
20
30
40
50
60
70
80
90
100
in-centerHD/HDF
3x/w
>3x/w
6 595 opinions 1.5 million patients
>3x/w
CAPD/APD
home/self-care HD/HDF
Ref: Ledebo, Ronco, NDT Plus 2008

© 2008, Gambro Lundia AB 32
Which dialysis option would you preferif you needed dialysis and could not be transplanted? Question to 70 Scottish nephrologists 2009
0
20
40
60
80
100
% o
f res
pond
ents
Where? Mode? How?
at home(94%)
HD(84%)
PD
HD
HDF
daily and/orlong duration
Ref: McManus et al, ASN abstract, 2009

© 2008, Gambro Lundia AB 33
Best long-term dialysis treatmentin the world, in W Europe and in Germany, 2007
0
10
20
30
40
Total (6595) W Europe (2071) Germanic (266)
CAPD/APD in-center HD/HDF, 3x/win-center HD/HDF, >3x/w home/sc HD/HDF, >3x/w

34
8.0%
9.1%
23.6%
58.0%
1.3%
CAPD/APD
in-center HD/HDF (3 times/week)
in-center HD/HDF (>3 times/week)
home and/or self-care HD/HDF (>3 times/week)
no opinion
What do you consider to be the best long-term dialysis treatment for the majority of patients,today and in the near future?
Q2: Best long-term dialysis treatment

© 2008, Gambro Lundia AB 35
low-flux hemodialysis
high-flux hemodialysis
high-volume hemodiafiltration
high-volume hemofiltration
What is the best extracorporeal form of dialysis ?
Is it to use…- low-flux or high-flux membrane? - diffusion or convection?- how much convection?

© 2008, Gambro 36
Membrane permeability
© 2008, Gambro 37
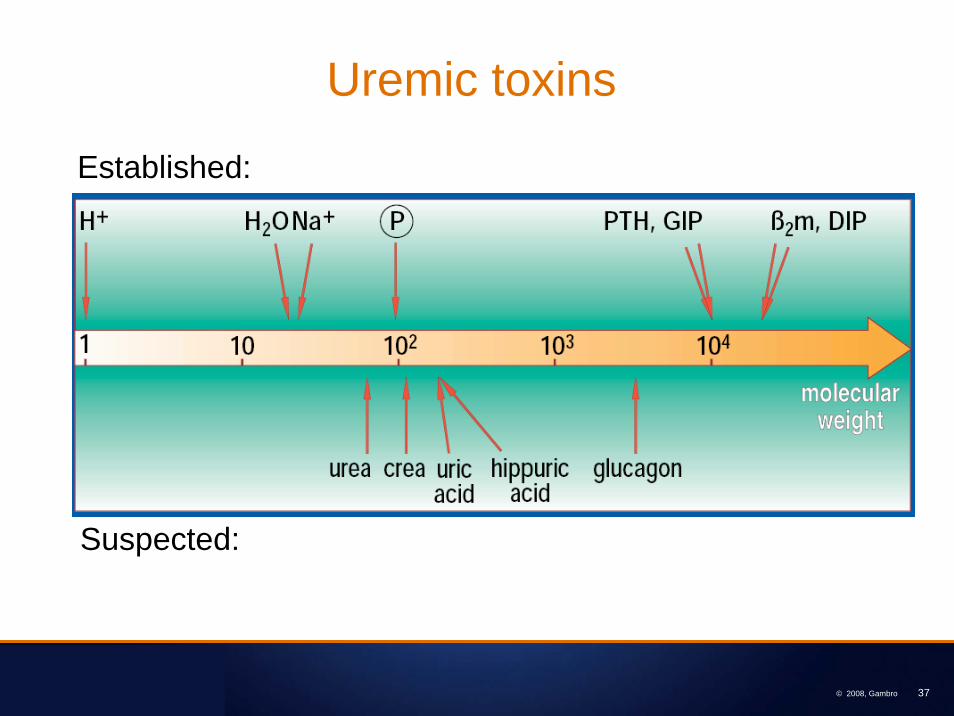
Uremic toxins
Established:
Suspected:

© 2008, Gambro 38
EuTox: Known uremic retention solutes
Ref: Vanholder el al. KI Suppl, 2003
Small, water-soluble Protein-bound Middle molecules

© 2008, Gambro 39
Convection in dialysis therapies
chronic dialysis therapy
membrane UF volume convection
low-flux dialysis (HD)
low-flux weight loss very little
high-flux dialysis (HD)
high-flux weight loss + backfiltration
little, uncontrollable
hemodiafiltration (HDF)
high-flux weight loss + substitution
considerable, controllable
hemofiltration (HF)
high-flux weight loss + substitution
considerable, controllable
© 2008, Gambro 40
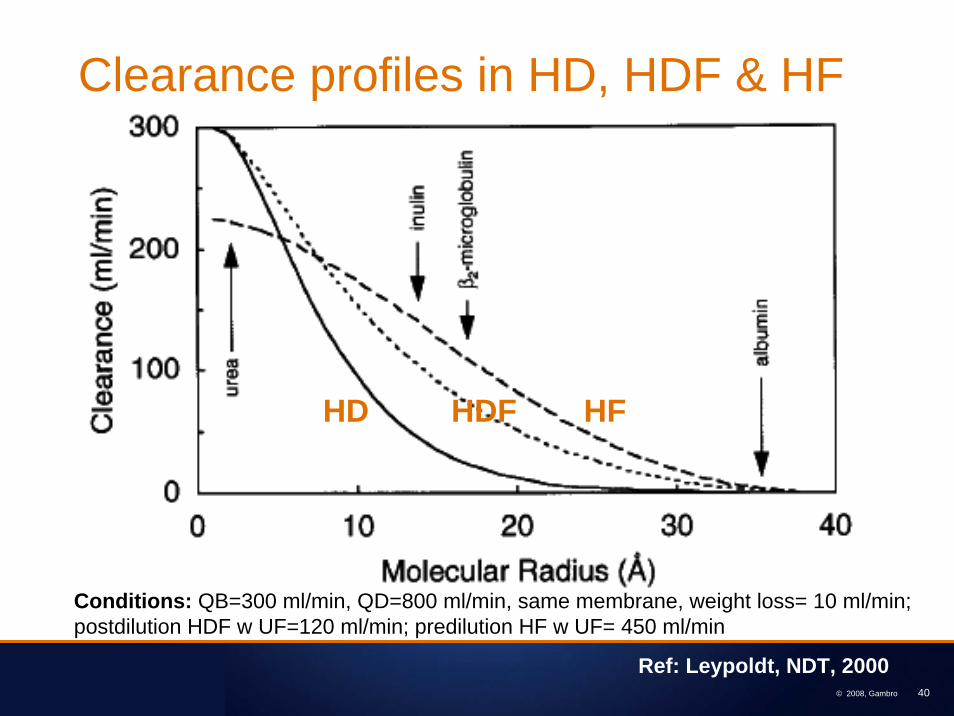
HD HFHDF
Clearance profiles in HD, HDF & HF
Conditions: QB=300 ml/min, QD=800 ml/min, same membrane, weight loss= 10 ml/min; postdilution HDF w UF=120 ml/min; predilution HF w UF= 450 ml/min
Ref: Leypoldt, NDT, 2000

© 2008, Gambro Lundia AB 41
Outcome with high-flux dialysisLarge RCT, all patients• HEMO Study, RCT• MPO Study, RCT
Large RCT, secondary & subgroup analysis• HEMO Study, RCT• MPO Study, RCT
Large prospective studies• French nutrition study• 4D, German RCT, statin & diabetics, post-hoc analysis

© 2008, Gambro Lundia AB 42
Outcome with high-flux dialysis
Large RCT, all patients• HEMO Study, RCT • MPO Study, RCT
Ref: Locatelli et al, JASN 2009Ref: Eknoyan et al, NEJM, 2002

© 2008, Gambro Lundia AB 43
Outcome with high-flux dialysisLarge RCT, secondary & subgroup analysis• HEMO Study, RCT • MPO Study, RCT
factors subgroups dose effectp - value
flux effectp - value
age ≤ 58 yrs >58 0.92 0.69
gender male female 0.014 0.27
race black non-black 0.06 0.24
diabetes + - 0.35 0.87
dialysis yrs ≤ 3.7 yrs >3.7 0.12 0.005
albumin ≤ 3.6 g/dl >3.6 0.16 0.65
comorbidity ≤ 2 units >2 0.96 0.96
long-term dialysis patients
Ref: Locatelli et al , JASN 2009
high-flux
low-flux
p=0.032
dialysis patients with alb < 4.0 g/dL
high-flux
p=0-039
low flux
diabetic patients
Ref: Eknoyan et al, NEJM, 2002

Survival benefit with high-flux HD, version 1.2 © 2008, Gambro Lundia AB 44
Ref: Cheung et al, JASN 2003
Ref: Delmez et al, AJKD 2006
High-flux dialysis – certain mortality causes

© 2008, Gambro Lundia AB 45
Outcome with high-flux dialysisLarge prospective studies• French nutrition study • 4D, German RCT
Ref: Krane et al, AJKD 2007
high-fluxsynthetic
low-fluxsynthetic
Ref: Chauveau et al, AJKD 2005
high-flux
low-flux

Survival benefit with high-flux HD, version 1.2 © 2008, Gambro Lundia AB 46
High-flux dialysis and outcome
0 0,2 0,4 0,6 0,8 1
Krane 06
Chauveau 05
Delmez 06
Cheung 05
Locatelli 09
Locatelli 09
Cheung 03
Locatelli 09
Eknoyan 02
ReferenceLow-flux
HEMO
MPO
HEMO
MPO
MPO
HEMO
HEMO
French
4D
p-values
n.s.
n.s
0.001
0.01
0.056
0.042
0.016
0.01
0.0006
>3.7 yrs
alb<4.0
diab.
cardiac †CBV †
all
all

© 2008, Gambro 47
<20 20 - 27.5 Cumulative mean predialysis serum ß2m (mg/L)
Rel
ativ
e R
isk
personal extrapolation
Serum β2m levels and mortality in the HEMO study
Based on: Cheung et al, JASN 2006

Survival benefit with high-flux HD, version 1.2 © 2008, Gambro Lundia AB 48
Pre-dialysis β2m and treatment mode
Conclusion: The more convection the lower plasma level of β2m
© 2006 Gambro

© 2008, Gambro 49

© 2008, Gambro Lundia AB 50
Outcome with HDF/HFLarge observational trials• on-line HDF vs hf HD in Euclid database• on-line HDF vs HD in DOPPS European database• on-line HDF vs hf HD in UK center• double-hf HDF vs all other in US center
RCT• on-line, predilution HF vs lf HD• on-line HDF vs lf HD, CONTRASTstudy ongoing

© 2008, Gambro Lundia AB 51
HDF is associated with 37% lower mortality in the EUCLID database
variable reference odds ratio 95% cilower
95% ciupper
p-value
age per year 1.054 1.045 1.063 <0.001
gender female 1.207 0.990 1.470 0.063
diabetes absent 1.664 1.323 2.094 <0.001
neoplasm absent 1.387 1.037 1.856 0.027
time on RRT
per year 1.041 1.021 1.062 <0.001
on-line HDF
HD 0.626 * 0.426 0.921 0.017
Ref: Jirka et al, NDT 2005, Suppl 5
* adjusted for age, gender, co-morbidities and time on RRT444 patients on on-line HDF compared to 3331 patients on hfHD

© 2008, Gambro Lundia AB 52
Mortality risk HDF vs HD
0
0,2
0,4
0,6
0,8
1
1,2
1,4
low-flux HD high-flux HD low-effic HDF high-effic HDF
Rel
ativ
e ris
k of
mor
talit
y
reference p=0.83 p=0.68 p=0.01
1.030.93
0.65
(1366) (546) (156) (97)
Ref: Canaud et al, KI 2006Ref: Canaud et al, KI 2006
n = 2165, adjusted for age, sex, time on dialysis, comorbidity, weight, catheter, Hb, alb, nPCR, lipids, Kt/V, EPO, QoL

© 2008, Gambro Lundia AB 53
Ref: Vilars et al, CJASN, 2009
Cox prop hazards model• HR = 0.454 p= 0.000 for patients predominantly treated with HDF• HR = 1.030 p=0.000per year of increasing age• HR = 1.848 p= 0.000 for malignancy• HR = 1.339 p= 0.006for diabetes
152 000 session of on-line HDF in 232 patients compared to 291 000 sessions on hfHD in 626 patients

© 2008, Gambro Lundia AB 54
Convective therapies and outcome
0 0,2 0,4 0,6 0,8 1 1,2
Santoro, 2008
Bosch, 2006
Vilar, 2009
Canaud, 2006
Jirka, 2005
Reference, HD p n
0.017 3828
0.01 4504
0.001 858
<0.005 183
<0.05 64
Relative risk of death
HDF
HDF
HDF
HF, RCT
HDF

© 2008, Gambro Lundia AB 55
CONTRASTThe Dutch Convective Transport StudyProspective, randomized, multicenter trialApprox. 780 patients randomized to on-line HDF & low-flux HD followed for up to 3 yearsPrincipal Investigators:Dr PJ Blankestijn, Utrecht MCProf Dr PM ter Wee, Free University MC, Amsterdam

© 2008, Gambro 56
Evidence for outcome benefits with high-flux/convective therapies
• long-term dialysis patients• hypoalbuminemic patients• diabetic patients• reduced cardiac death• reduced cerebrovascular death

© 2008, Gambro Lundia AB 57
Best extracorporeal form of dialysisaccording to 6 595 nephrology professionals
0
10
20
30
40
50
Ref: Ledebo, Ronco, NDT Plus, 2008
low-flux HD
high-flux HD
high-volume HDF
high-volume HF

© 2008, Gambro Lundia AB 58
Best extracorporeal form of dialysisworldwide opinion by nephrology professionals
0
10
20
30
40
50
60
Total (6595)
W Europe(2071)
E Europe(1879)
Asia (888)
Americas(1107)
low-flux HD high-flux HD high-volume HDF high-volume HF
Ref: Ledebo, Ronco, NDT Plus, 2008

© 2008, Gambro Lundia AB 59
Best extracorporeal form of dialysisin the world, in W Europe and in Germany in 2007
0
10
20
30
40
50
60
Total (6595) W Europe (2071) Germanic (266)
low-flux HD high-flux HD high-volume HDF high-volume HF

60
3.3%
25.3%
63.6%
1.9%
5.9%
low-flux hemodialysis
high-flux hemodialysis
high-volume hemodiafiltration
high-volume hemofiltration
no opinion
What do you consider to be the best extracorporeal form of dialysis?
Q3: Best extracorporeal form of dialysis
synthetic membrane,ultrapure fluid
Syntheticmembrane,on-line prepared fluid

© 2008, Gambro Lundia AB 61
hard evidence, i.e. improved survival
surrogate evidence, i.e. improved markers (CRP, LVH)
soft evidence, i.e. better quality of lifeown/colleagues´ experience
Which level of evidence do we require?

© 2008, Gambro Lundia AB 62
Lowest number of RCT in nephrology
Ref: Strippoli, JASN 2004

© 2008, Gambro Lundia AB 63
Minimum level of evidenceaccording to 6 595 nephrology professionals
0
10
20
30
40
50
hard evidence surrogate evidence soft evidence experience
Ref: Ledebo, Ronco, NDT Plus, 2008

© 2008, Gambro Lundia AB 64
Minimum level of evidenceworldwide opinion by nephrology professionals
0
10
20
30
40
50
60
Total (6595)
W Europe(2071)
E Europe(1879)
Asia (888)
Americas(1107)
hard evidence surrogate evidence soft evidence experience
Ref: Ledebo, Ronco, NDT Plus, 2008

© 2008, Gambro Lundia AB 65
Minimum level of evidencein the world, in W Europe and in Germany in 2007
0
10
20
30
40
50
Total (6595) W Europe (2071) Germanic (266)
hard evidence surrogate evidence soft evidence experience
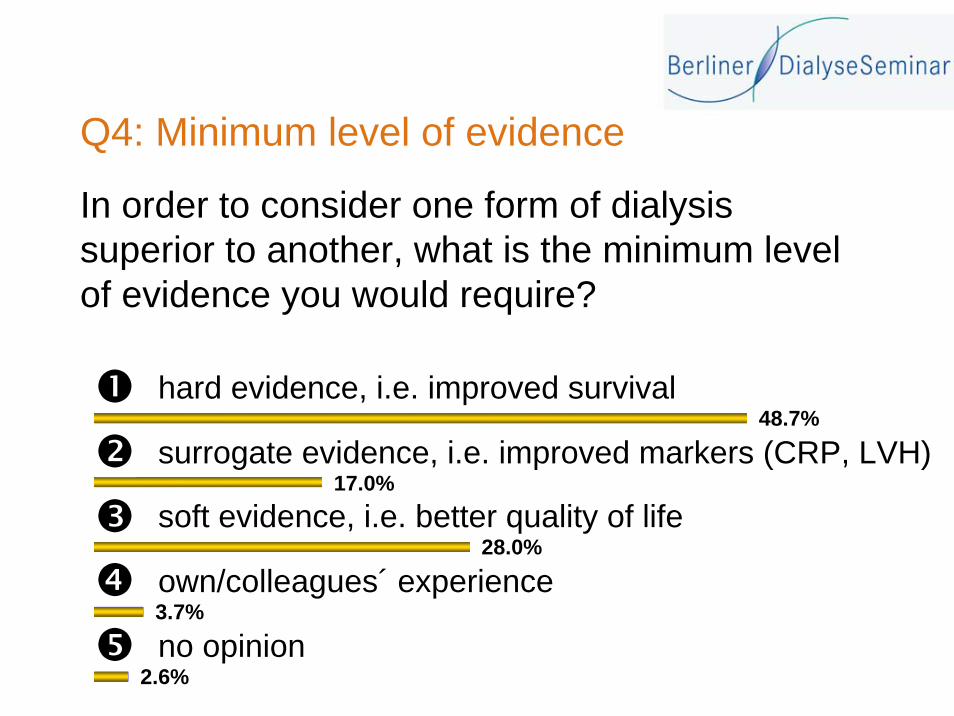
66
48.7%
17.0%
28.0%
3.7%
2.6%
hard evidence, i.e. improved survival
surrogate evidence, i.e. improved markers (CRP, LVH)
soft evidence, i.e. better quality of life
own/colleagues´ experience
no opinion
In order to consider one form of dialysis superior to another, what is the minimum level of evidence you would require?
Q4: Minimum level of evidence

© 2008, Gambro Lundia AB 67
Future development of dialysis Conclusions from survey 2007
• The opinion of nephrology professionals on the value of therapies follows scientific discussions in spite of lack of hard evidence• PD considered best therapy for incident patients• Self-care dialysis at home, frequently applied, considered best long-term therapy• High-flux membranes strongly preferred to low-flux membranes • When possible use high-flux membranes for maximum convective transport, i.e. in HDF• Opinions differ greatly from present situation and can be seen as indication of future development of dialysis

© 2008, Gambro Lundia AB 68
multiple drug therapy that stops progressionstem cell therapy that restores renal functionprepare for dialysis with miniaturized, wearable, bionic kidney that works continuouslyprepare for dialysis similar to what we have todayother/no opinion
Q5: Best ESRD treatment in 2025Which ESRD treatment do you think you will be able to recommend to a close family member in 2025, when he/she turns 60 and is found to have CKD stage 4?
Dialysis Opinions 2007

69
19.5%
31.5%
28.9%
16.0%
4.2%
Which ESRD treatment do you think you will beable to recommend to a close family member in 2025,when he/she turns 60 and is found to have CKD stage 4?
Q5: Best ESRD treatment in 2025
multiple drug therapy that stops progression
stem cell therapy that restores renal function
prepare for dialysis with miniaturized, wearable, bionic kidney that works continuously
prepare for dialysis similar to what we have today
other/no opinion

© 2008, Gambro Lundia AB 70
Best ESRD treatment in 2025according to 6 595 nephrology professionals
0
10
20
30
40
50
preventive drugs stem cells bionic WAK dialysis no opinion
Dialysis Opinions 2007

© 2008, Gambro Lundia AB 71
Best ESRD treatment in 2025worldwide opinion by nephrology professionals
0
10
20
30
40
50
Total (6595)
W Europe(2071)
E Europe(1879)
Asia (888)
Americas(1107)
preventive drugs stem cells bionic WAK dialysis
Dialysis Opinions 2007

© 2008, Gambro Lundia AB 72
Best ESRD treatment in 2025in the world, in W Europe and in Germany in 2007
0
10
20
30
40
50
Total (6595) W Europe (2071) Germanic (266)
preventive drugs stem cells bionic WAK dialysis
