hcv treatment: before or after liver...
TRANSCRIPT

HCV TREATMENT:
BEFORE OR AFTER LIVER
TRANSPLANTATION?
The XI International Conference «White Nights of Hepatology 2017» EASL
Saint Petersburg , June 8 - 9 2017
Elena N. Bessonova Ph.D Sverdlovsk Regional Hepatological Center
SBHCE «Sverdlovsk Regional Clinical Hospital №1»
Ekaterinburg, Russia
INTRODUCTION
• HCV infection is the leading indication for liver transplantation throughout the world1
• Approximately 5,000 liver transplantations are performed annually in the USA, with 40% due to HCV-related cirrhosis2 in adults
• Patients who undergo liver transplantation with detectable HCV RNA levels will inevitably experience graft infection3
• Recurrence of HCV accounts for the majority of post-liver transplant deaths and for two-thirds of graft rejections4
• HCV-positive transplant recipients have a shorter survival than other recipients4
• Cirrhosis related to HCV occurs in 20–30% of transplant patients within 5 years of receiving liver graft5
1. Charlton M, et al. Liver Transpl 2004;10:1120–30
2. Wiesner RH, et al. Liver Transpl 2003;9:S1–9; 3. Garcia-Retortillo M, et al. Hepatology 2002;35:680–7
4. Berenguer M, et al. Heptology 2000;32:673–84; 5. Berenguer M. Curr Opin Organ Transplant 2005;10:81–89
73
86 85 83 83
92
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10
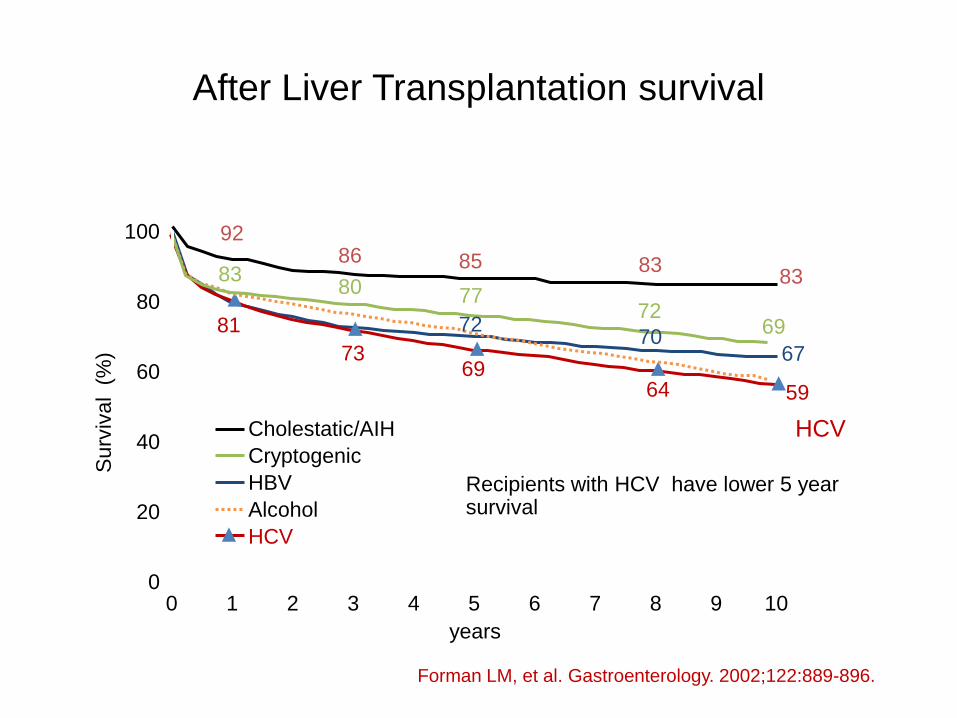
HBV
HCV
Alcohol
years
Surv
ival (
%)
81
67 69
64 59
83 80 77
72 69
Cholestatic/AIH
70 72
HCV
Recipients with HCV have lower 5 year survival
Forman LM, et al. Gastroenterology. 2002;122:889-896.
Cryptogenic
After Liver Transplantation survival
Liver
Transplantation
Waiting List
Patients with
HCV
HCV Treatment
HCV infection
recurrence After
Liver
Transplantation
HCV TREATMENT
BEFORE LIVER TRANSPLANTATION
The aim of HCV infection treatment in decompensated cirrhosis before liver transplantation
To prevent HCV recurrence
New DAAs with remarkable results
can be used in decompensated
patients To improve the
patient status and to
achieve delisting from LT
waiting list

ELITA Cohort Expansion Study
EASL 2017 Delisting of liver transplant candidates with chronic HCV infection after viral eradication and outcome after
delisting. A European cohort study. L.S. Belli, M. Berenguer, P. Cortesi, M. Strazzabosco, G. Perricone et al.
Regimen: SOF+RBV (46%)
SOF+DCV or LDV+SOF (54%) 12 weeks.
142 liver transplantation candidates, age: 37-71, 69% male, without HCC
69
58
15
MELD level at the DAA start
<16
16-20
>201
66
75
Child-Pugh at the start of DAA
A
B
C

ELITA Cohort Expansion Study
• DAA therapy improves liver function in patients with HCV infection and decompensated cirrhosis
• 1 in 5 (38 out of 142) liver transplantation candidates with chronic HCV infection
was delisted due to clinical improvement after DAA therapy • Low incidence of liver complications: 3 in 38 patients (1 redecompensated and relisted, 1 – TIPS for refractory ascitis, 1 – died with following
diagnosis of HCC)
2017 EASL
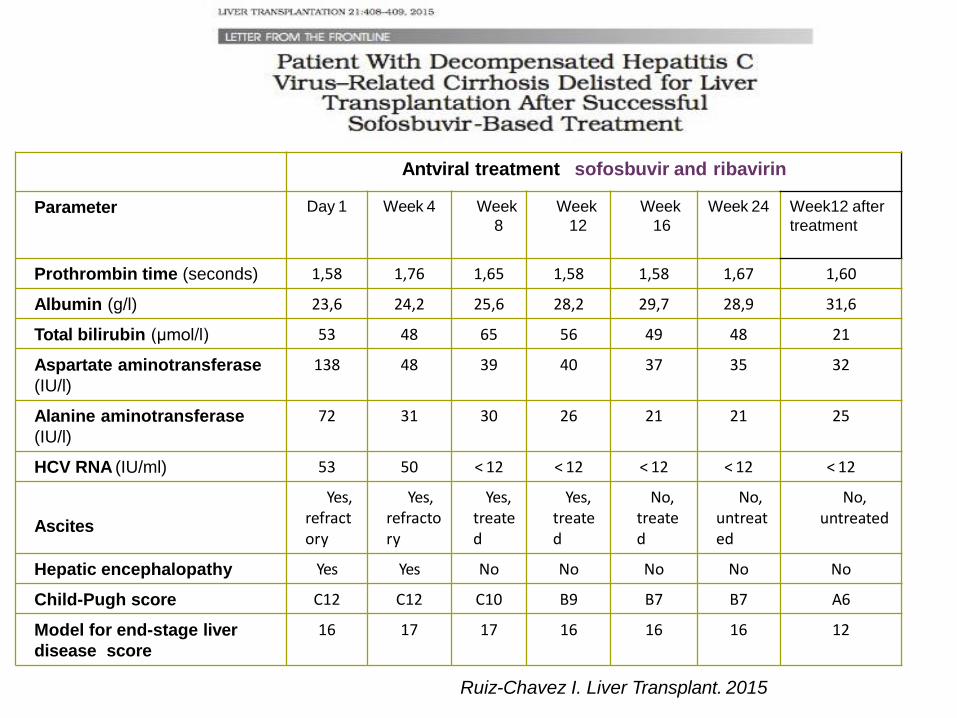
Ruiz-Chavez I. Liver Transplant. 2015
Antviral treatment sofosbuvir and ribavirin
Parameter Day 1 Week 4 Week
8
Week
12
Week
16
Week 24 Week12 after
treatment
Prothrombin time (seconds) 1,58 1,76 1,65 1,58 1,58 1,67 1,60
Albumin (g/l) 23,6 24,2 25,6 28,2 29,7 28,9 31,6
Total bilirubin (µmol/l) 53 48 65 56 49 48 21
Aspartate aminotransferase
(IU/l)
138 48 39 40 37 35 32
Alanine aminotransferase
(IU/l)
72 31 30 26 21 21 25
HCV RNA (IU/ml) 53 50 < 12 < 12 < 12 < 12 < 12
Ascites
Yes, refractory
Yes, refractory
Yes, treated
Yes, treated
No, treated
No, untreated
No, untreated
Hepatic encephalopathy Yes Yes No No No No No
Child-Pugh score C12 C12 C10 B9 B7 B7 A6
Model for end-stage liver
disease score
16 17 17 16 16 16 12
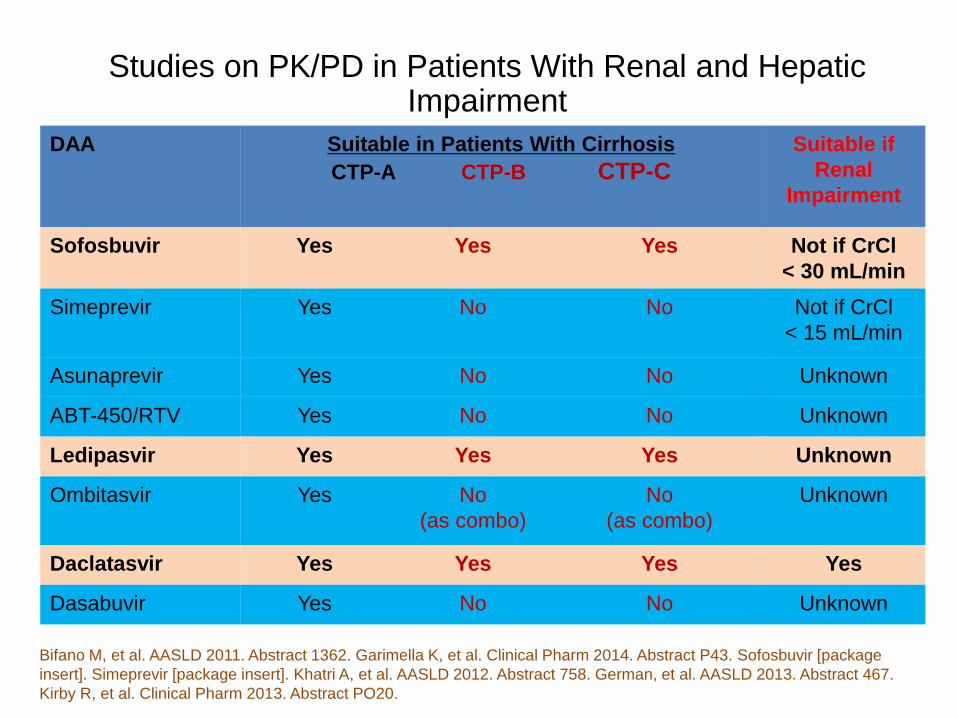
DAA Suitable in Patients With Cirrhosis
CTP-A CTP-B CTP-C
Suitable if
Renal
Impairment
Sofosbuvir Yes Yes
Yes
Not if CrCl
< 30 mL/min
Simeprevir Yes No No Not if CrCl
< 15 mL/min
Asunaprevir Yes No No Unknown
ABT-450/RTV Yes No No Unknown
Ledipasvir Yes Yes Yes Unknown
Ombitasvir Yes No
(as combo)
No
(as combo)
Unknown
Daclatasvir Yes Yes Yes Yes
Dasabuvir Yes No No Unknown
Bifano M, et al. AASLD 2011. Abstract 1362. Garimella K, et al. Clinical Pharm 2014. Abstract P43. Sofosbuvir [package
insert]. Simeprevir [package insert]. Khatri A, et al. AASLD 2012. Abstract 758. German, et al. AASLD 2013. Abstract 467.
Kirby R, et al. Clinical Pharm 2013. Abstract PO20.
Studies on PK/PD in Patients With Renal and Hepatic Impairment
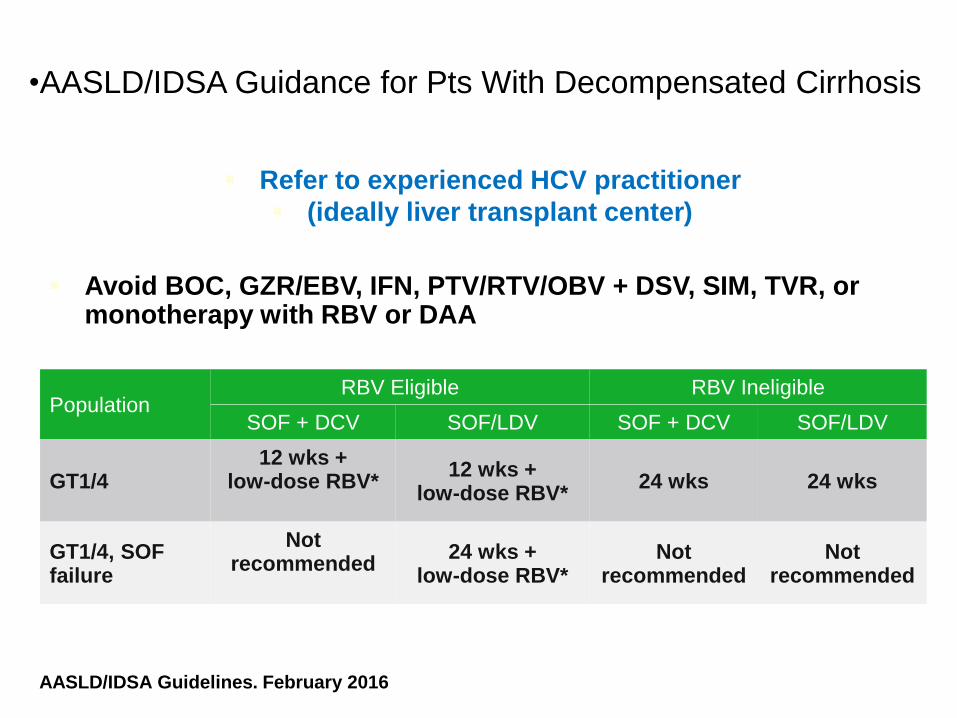
•AASLD/IDSA Guidance for Pts With Decompensated Cirrhosis
Refer to experienced HCV practitioner
(ideally liver transplant center)
Avoid BOC, GZR/EBV, IFN, PTV/RTV/OBV + DSV, SIM, TVR, or monotherapy with RBV or DAA
AASLD/IDSA Guidelines. February 2016
*Initial dose of 600 mg/day, increased as tolerated.
Population RBV Eligible RBV Ineligible
SOF + DCV SOF/LDV SOF + DCV SOF/LDV
GT1/4 12 wks +
low-dose RBV*
12 wks + low-dose RBV*
24 wks 24 wks
GT1/4, SOF failure
Not recommended
24 wks + low-dose RBV*
Not recommended
Not recommended

Treatment with DAA before liver transplantation
Patients with decompensated cirrhosis without HCC awaiting liver
transplantation and MELD score <18-20 can be treated prior to liver
transplantation
Patients with decompensated cirrhosis and an indication for liver
transplantation with a MELD score ≥18-20 should be transpanted first
and treated after LT
Treatment is not recommended in patients with limited life expectancy
due to non-liver-related comorbidities.
Protease inhibitors should not be used in patients with Child-Pugh B or C
decompensated cirrhosis
EASL 2017 recommendations
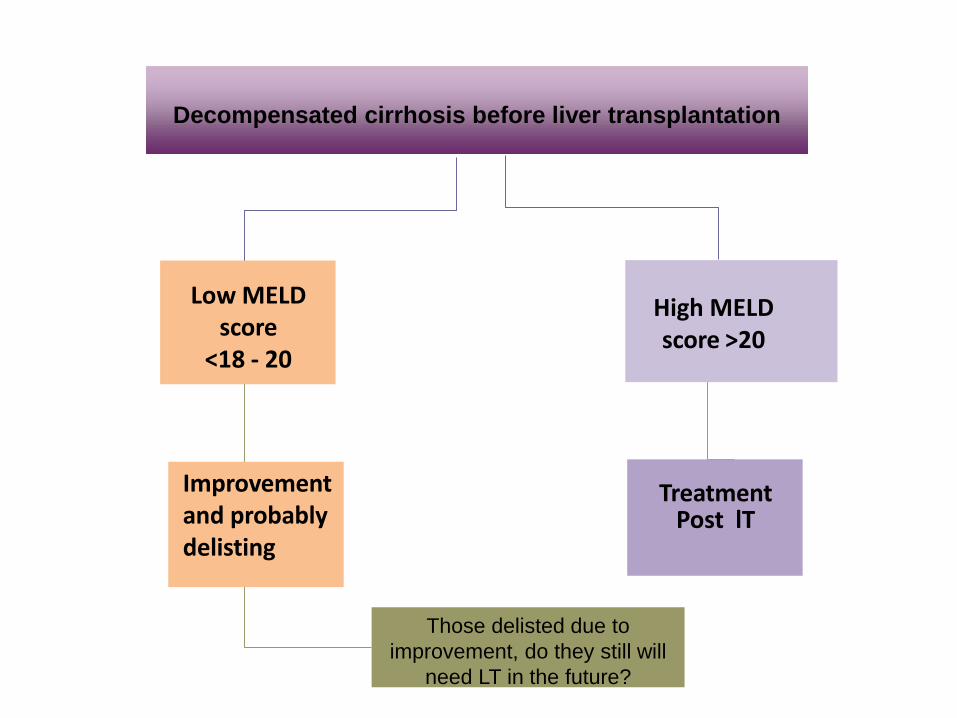
Decompensated cirrhosis before liver transplantation
Low MELD score
<18 - 20
Improvement and probably delisting
High MELD score >20
Treatment Post lT
Those delisted due to
improvement, do they still will
need LT in the future?
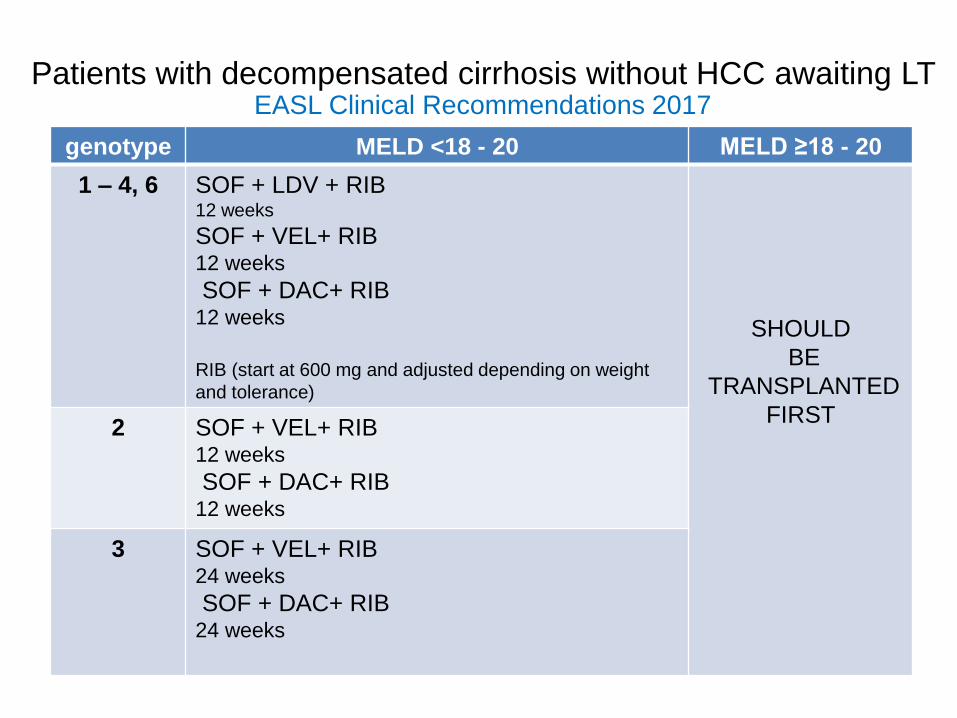
Patients with decompensated cirrhosis without HCC awaiting LT EASL Clinical Recommendations 2017
genotype MELD <18 - 20 MELD ≥18 - 20
1 – 4, 6 SOF + LDV + RIB 12 weeks
SOF + VEL+ RIB 12 weeks
SOF + DAC+ RIB 12 weeks
RIB (start at 600 mg and adjusted depending on weight
and tolerance)
SHOULD
BE
TRANSPLANTED
FIRST 2 SOF + VEL+ RIB
12 weeks
SOF + DAC+ RIB 12 weeks
3 SOF + VEL+ RIB 24 weeks
SOF + DAC+ RIB 24 weeks
HCV TREATMENT
AFTER LIVER TRANSPLANTATION
Impact of Post-Transplantation HCV Infection
Recurrent HCV infection is the leading cause of graft failure in recipients of liver transplant.
Infection of the graft occurs nearly universally in patients with untreated HCV infection who
receive liver transplantation.
Reinfection occurs as soon as reperfusion of the allograft takes place in the operating
room, and viral titers have been detected to reach pre-transplantation levels within 72
hours.
Until recently, attempts to prevent or treat HCV recurrence have been limited by poor
tolerability and responses to interferon-based antiviral therapy.
The availability of highly effective and safe all-oral DAAs will improve the ability to treat
HCV recurrence in liver transplantation.
Fagiuoli S, Ravasio R, Lucà MG, World J Gastroenterol. 2015

HCV RECURRENCE OUTCOMES
In 5 years post-LT, 30% of LT patients have graft cirrhosis
LT
Death Retransplantation
Patient HCV RNA+
after LT
Adapted from Mc Caughan
20%
70%
10%
Asymptomatic
hepatitis
Fibrosing
cholestatic
hepatitis
Chronic
Hepatitis
Cirrhosis Acute Hepatitis
Chronic
hepatitis
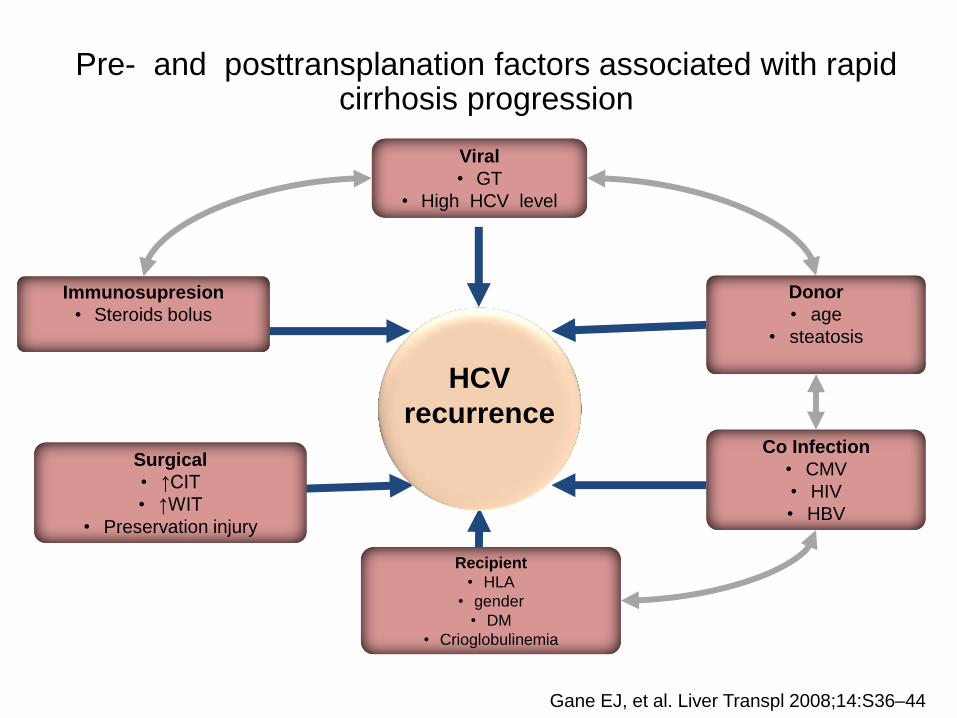
Pre- and posttransplanation factors associated with rapid cirrhosis progression
Gane EJ, et al. Liver Transpl 2008;14:S36–44
Recipient
• HLA
• gender
• DM
• Crioglobulinemia
Immunosupresion
• Steroids bolus
Viral
• GT
• High HCV level
Co Infection
• CMV
• HIV
• HBV
HCV
recurrence
Surgical
• ↑CIT
• ↑WIT
• Preservation injury
Donor
• age
• steatosis
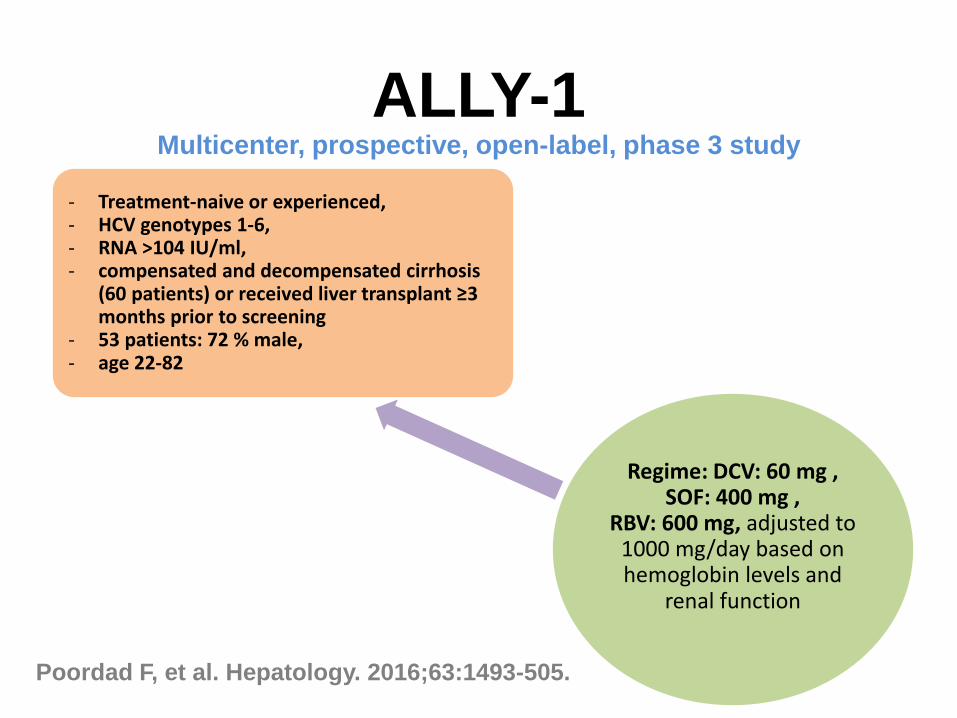
ALLY-1 Multicenter, prospective, open-label, phase 3 study
Regime: DCV: 60 mg , SOF: 400 mg ,
RBV: 600 mg, adjusted to 1000 mg/day based on hemoglobin levels and
renal function
- Treatment-naive or experienced, - HCV genotypes 1-6, - RNA >104 IU/ml, - compensated and decompensated cirrhosis
(60 patients) or received liver transplant ≥3 months prior to screening
- 53 patients: 72 % male, - age 22-82
Poordad F, et al. Hepatology. 2016;63:1493-505.

ALLY-1
SVR-12 results for post-liver transplant
Poordad F, et al. Hepatology. 2016;63:1493-505.
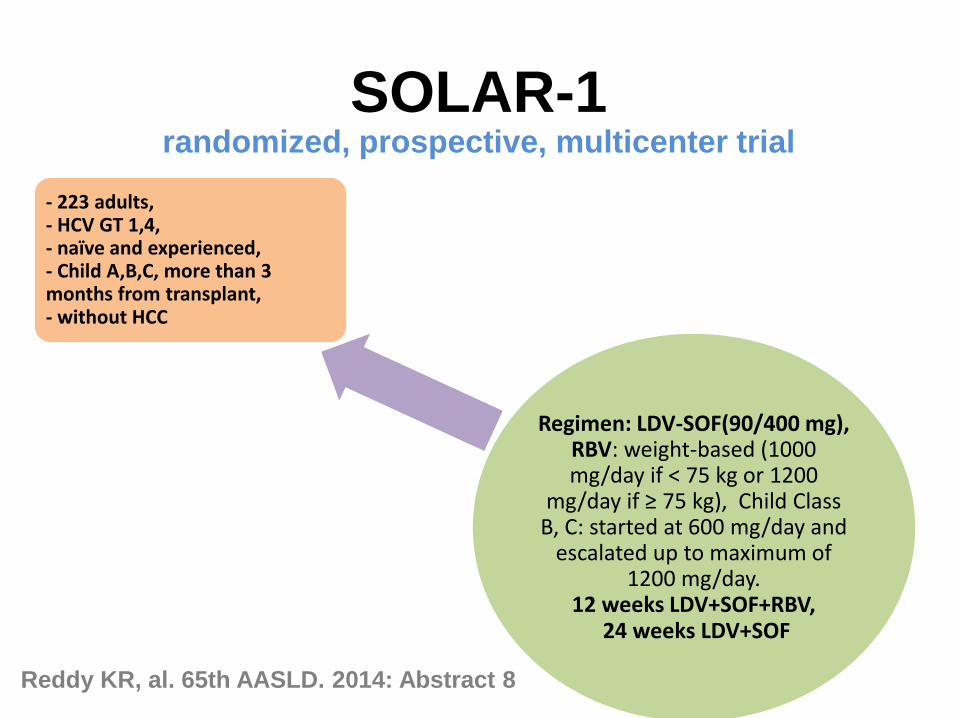
SOLAR-1 randomized, prospective, multicenter trial
Regimen: LDV-SOF(90/400 mg), RBV: weight-based (1000 mg/day if < 75 kg or 1200
mg/day if ≥ 75 kg), Child Class B, C: started at 600 mg/day and
escalated up to maximum of 1200 mg/day.
12 weeks LDV+SOF+RBV, 24 weeks LDV+SOF
- 223 adults, - HCV GT 1,4, - naïve and experienced, - Child A,B,C, more than 3 months from transplant, - without HCC
Reddy KR, al. 65th AASLD. 2014: Abstract 8

SOLAR-1 SVR12
Fatigue, anemia, headache and nausea were the most common adverse events, and serious adverse events were rare.
Reddy KR, al. 65th AASLD. 2014: Abstract 8
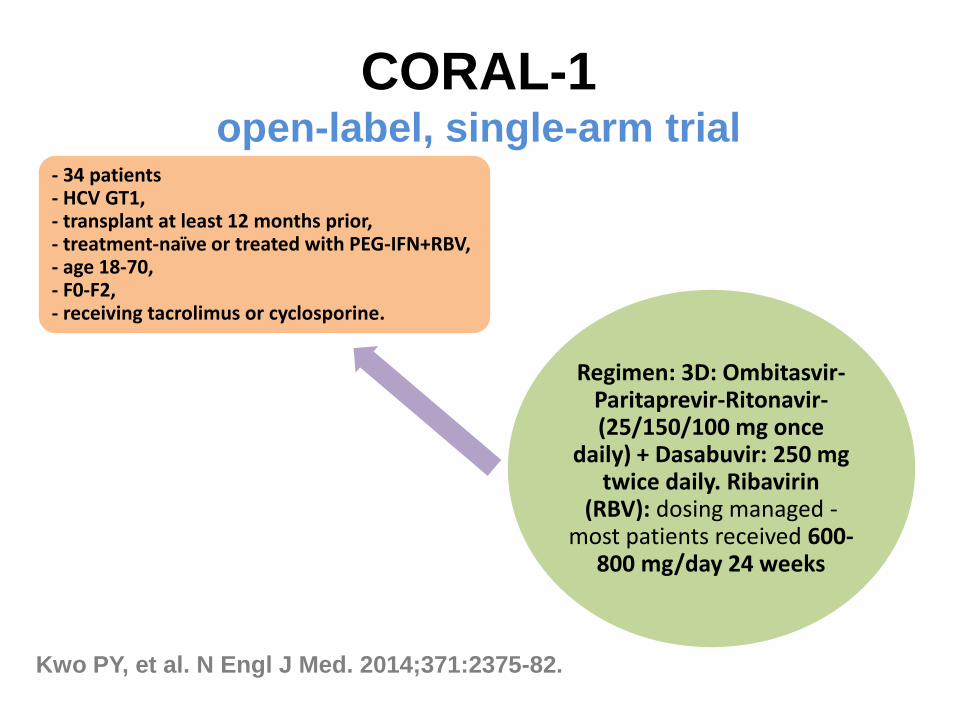
CORAL-1 open-label, single-arm trial
Regimen: 3D: Ombitasvir-Paritaprevir-Ritonavir- (25/150/100 mg once
daily) + Dasabuvir: 250 mg twice daily. Ribavirin
(RBV): dosing managed - most patients received 600-
800 mg/day 24 weeks
- 34 patients - HCV GT1, - transplant at least 12 months prior, - treatment-naïve or treated with PEG-IFN+RBV, - age 18-70, - F0-F2, - receiving tacrolimus or cyclosporine.
Kwo PY, et al. N Engl J Med. 2014;371:2375-82.

CORAL-1 Results
No episodes of rejection
5 patients received EPO and no blood transfusions.
Adjustment of doses tacrolimus: reduction 0,2 mg every 3 days.
Adjustment of doses cyclosporine: reduction of 20 % pretreatment dose.
Kwo PY, et al. N Engl J Med.
2014;371:2375-82.
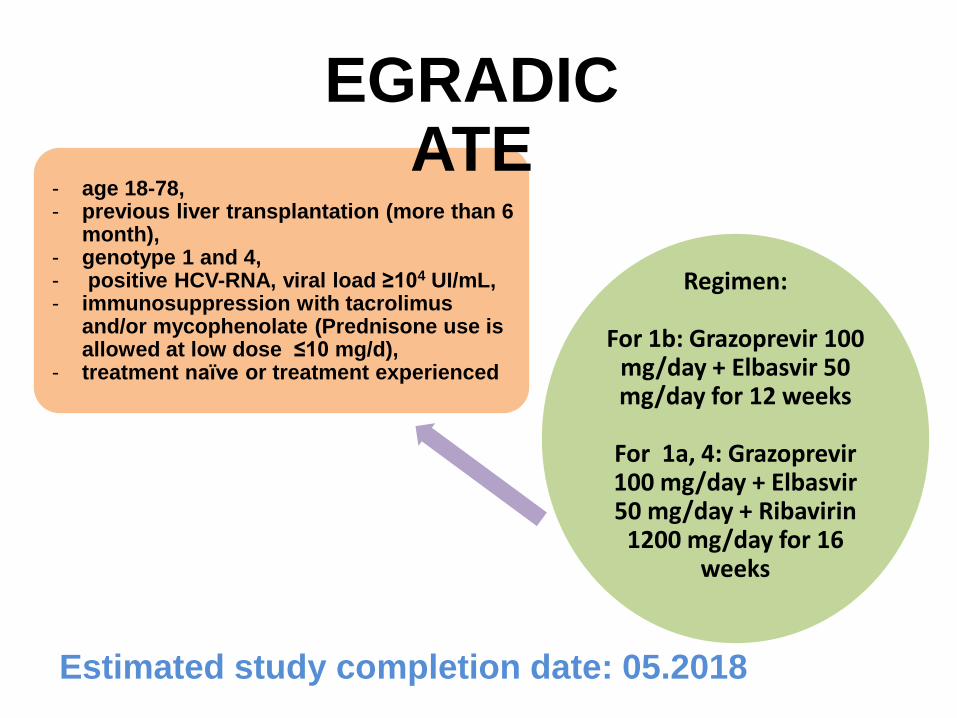
Estimated study completion date: 05.2018
Regimen:
For 1b: Grazoprevir 100 mg/day + Elbasvir 50 mg/day for 12 weeks
For 1a, 4: Grazoprevir 100 mg/day + Elbasvir 50 mg/day + Ribavirin
1200 mg/day for 16 weeks
- age 18-78, - previous liver transplantation (more than 6
month), - genotype 1 and 4, - positive HCV-RNA, viral load ≥104 UI/mL, - immunosuppression with tacrolimus
and/or mycophenolate (Prednisone use is allowed at low dose ≤10 mg/d),
- treatment naïve or treatment experienced
EGRADICATE
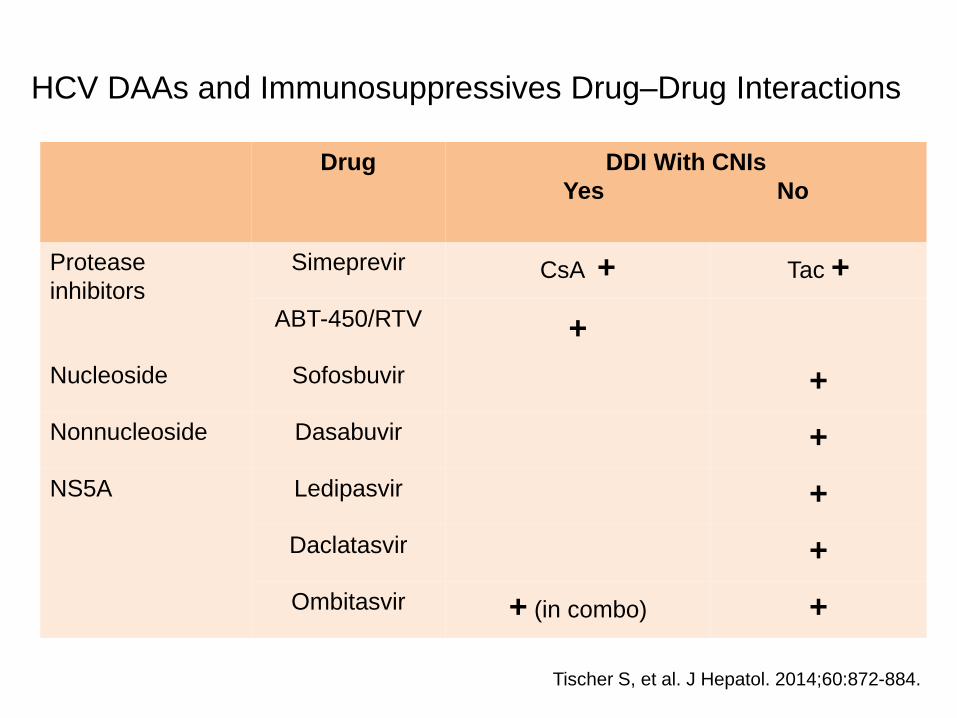
HCV DAAs and Immunosuppressives Drug–Drug Interactions
Drug DDI With CNIs
Yes No
Protease
inhibitors
Simeprevir CsA + Tac +
ABT-450/RTV +
Nucleoside Sofosbuvir +
Nonnucleoside Dasabuvir +
NS5A Ledipasvir +
Daclatasvir +
Ombitasvir + (in combo) +
Tischer S, et al. J Hepatol. 2014;60:872-884.
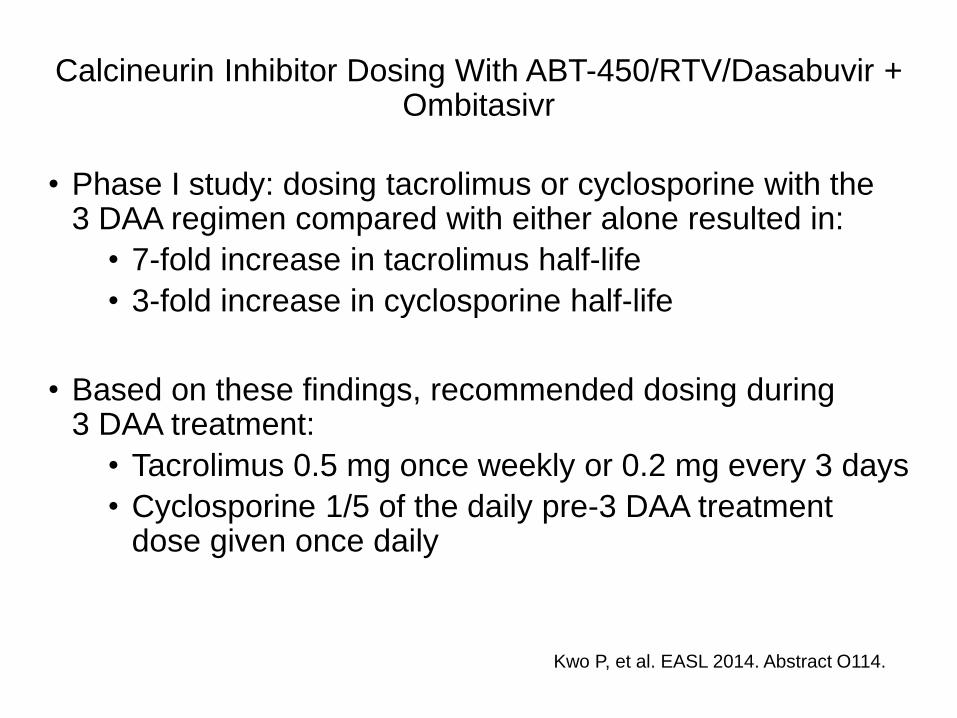
Calcineurin Inhibitor Dosing With ABT-450/RTV/Dasabuvir + Ombitasivr
• Phase I study: dosing tacrolimus or cyclosporine with the 3 DAA regimen compared with either alone resulted in:
• 7-fold increase in tacrolimus half-life
• 3-fold increase in cyclosporine half-life
• Based on these findings, recommended dosing during 3 DAA treatment:
• Tacrolimus 0.5 mg once weekly or 0.2 mg every 3 days
• Cyclosporine 1/5 of the daily pre-3 DAA treatment dose given once daily
Kwo P, et al. EASL 2014. Abstract O114.
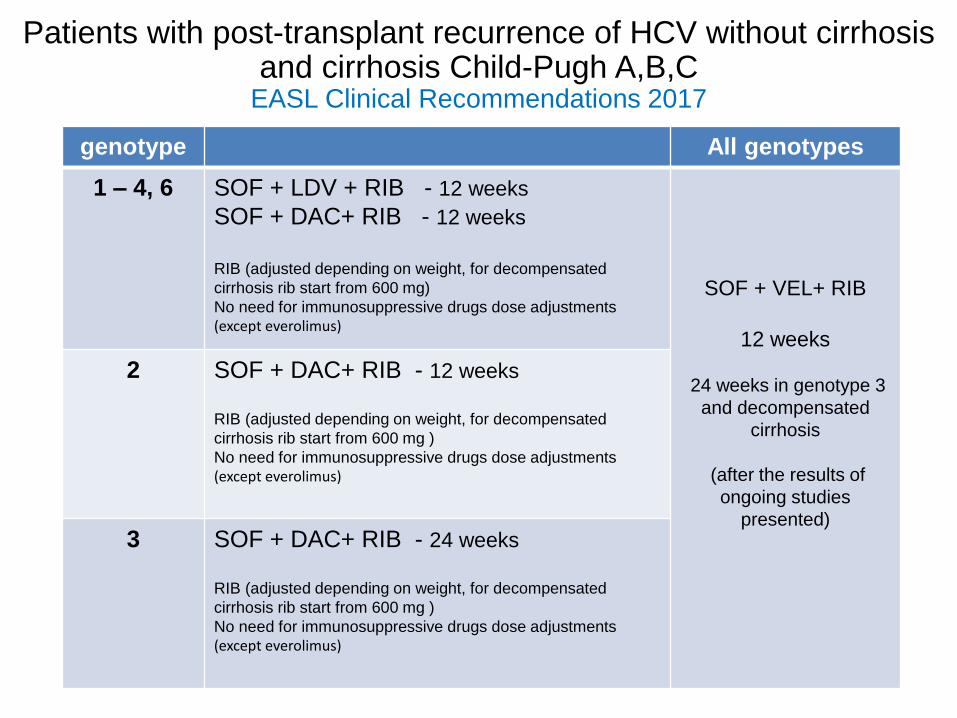
Patients with post-transplant recurrence of HCV without cirrhosis and cirrhosis Child-Pugh A,B,C
EASL Clinical Recommendations 2017
genotype All genotypes
1 – 4, 6 SOF + LDV + RIB - 12 weeks
SOF + DAC+ RIB - 12 weeks
RIB (adjusted depending on weight, for decompensated
cirrhosis rib start from 600 mg)
No need for immunosuppressive drugs dose adjustments (except everolimus)
SOF + VEL+ RIB
12 weeks
24 weeks in genotype 3
and decompensated
cirrhosis
(after the results of
ongoing studies
presented)
2 SOF + DAC+ RIB - 12 weeks
RIB (adjusted depending on weight, for decompensated
cirrhosis rib start from 600 mg )
No need for immunosuppressive drugs dose adjustments (except everolimus)
3 SOF + DAC+ RIB - 24 weeks
RIB (adjusted depending on weight, for decompensated
cirrhosis rib start from 600 mg )
No need for immunosuppressive drugs dose adjustments (except everolimus)

Post-transplant recurrence of HCV Summary
All patients with post-transplant recurrence of HCV infection
should be considered for antiviral therapy
Treatment should be initiated as early as possible when recipient
is stabilized (optimal after 3 months post transplant)
Cholestatic hepatitis or the presence of portal hypertension one
year after transplantation predict rapid disease progression and
graft loss and is indication for immediate antiviral treatment
Guidelines of Treatments Hepatities C, EASL 2016
Conclusion
In the liver transplantation settings the patient must be treated before or after transplantation. The decision should be individualized depending of the disease progression HCV infected LT candidates or recipients of the graft should be prioritized in all antiviral treatment programs Using of protease inhibitors in sever decompensated patient are not recommended New DAAs with good safety and tolerability profile are coming and HCV recurrence after LT probably will not be a problem any more