hcca pr 2015 health plan part d compliance plan part d compliance ... •in person meetings at least...
TRANSCRIPT

1
Health Plan Part D Compliance
Health Plan Part D Compliance
Hector W. Ramirez, RPh, PharmD, CHC
• Part D Compliance Director
• Medical Card System, Inc.
• San Juan, Puerto Rico
Carolyn Rodriguez, RPh, PharmD
• Pharmacy Senior Vice President
• Medical Card System, Inc.
• San Juan, Puerto Rico
2
Friday, May 1st, 2015

2
Objectives
• Gain insight into the relationship between PBMs and health plans
• Review processes to oversight PBMs and ensure Part D compliance
• Review best practices for capturing contract language to best meet audit and Part D compliance requirements
• Assess the challenges associated with PBM transparency and Part D compliance
3
Agenda
Introduction
Business Relationship between PBMs and Health Plans
Delegated Functions and PBM Contracting
Best Practices Stemming from Daily Operations
Oversight to Ensure Compliance
Regulatory Framework and FDR Monitoring
Common Part D Compliance Problems
4
3
Medical Card System, Inc.
• One of the largest managed care organizations in Puerto Rico, in both the Medicare Advantage and Commercial market segments
• Over 30 years of experience providing services to the Puerto Rico market
• Since 2005, our Medicare business has grown every year to achieve 175,000 lives as of today
• Since 2006, we have been managing Part D services
• First health plan in Puerto Rico to achieve 3.5 Star Rating
www.mcs.com.pr
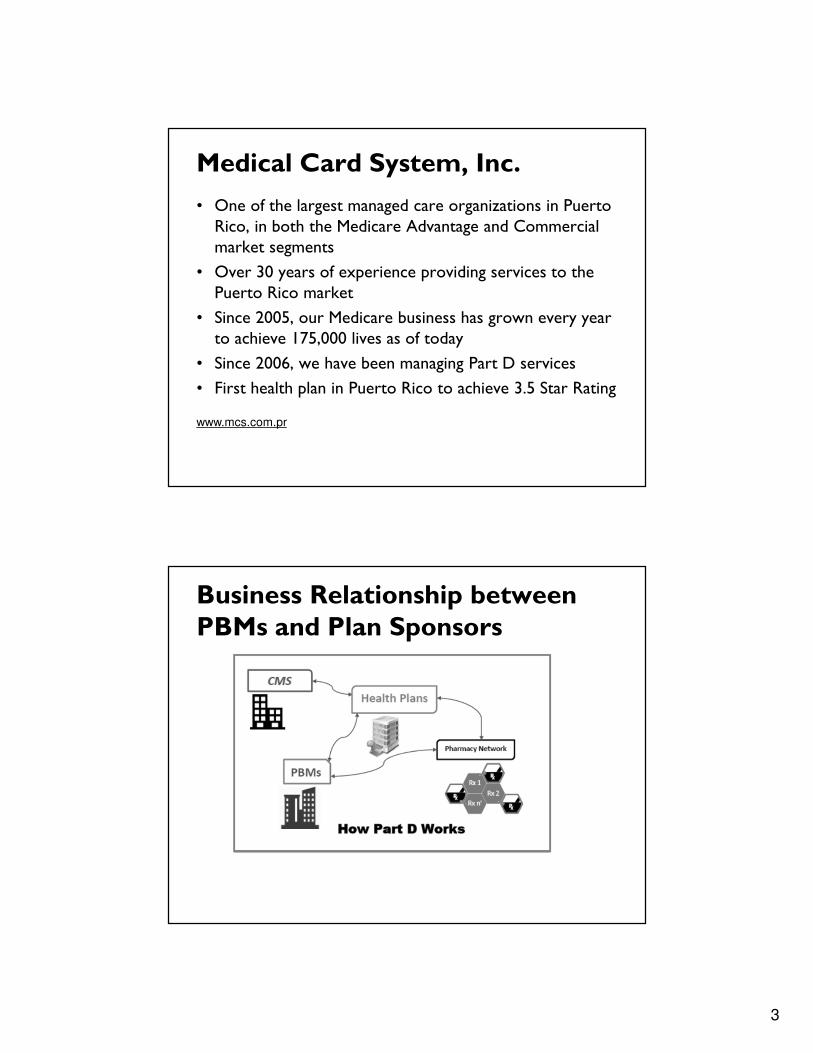
Business Relationship betweenPBMs and Plan Sponsors

4
Delegation of Functions
�Claims Processing
� Formulary Management
� PDE management
� P&T Committee
�Rebates
� Pharmacy Network Contracting and Credentialing
� EOBs
�Reporting Requirements
• CMS monitors very closely these services in which beneficiary access could be impacted
• Among CMS priorities of patient care, FWA surveillance is also an essential element
Contract… Is the Key
• Build the PMB contract in a way that works for both parties– Clear description of delegated functions– Delegation agreement• Accountability• Expectations• Consequences
– Performance guarantees • Specific• Measurable
– Termination clause

5
Best Practices in PBM Contracting
• Claim pricing calculation– Include all definitions to guarantee calculations
– Disclose all fees
– Provision to use an independent evaluation for any dramatic cost change
• Cost sharing calculation
• Explain the dispute resolution process
• Formulary / Rebates
• Termination clause
Best Practices Stemming From Daily Operations• Establish a robust monitoring process in your day-to-day business relation with the PBM
• Frequent meetings that includes specific agenda items to discuss current major issues, compliance issues, CMS monitoring projects, workaround plans and reports
• Discuss and follow up on all delegated functions– Give priority to formulary and transition processes– Have separate discussions among the following functions
• Clinical issues• PDEs management• HPMS memos discussions• Financial issues

6
Tips That Can Help You
• Have a secure and organized shared folder to maintain key information
– Policies and procedures
– Operational reports (daily, weekly, monthly)
– Point of Contact (POC)
– Audits requests tracking log
– Documentation and evidence of oversight activities
Discuss and Document
• Understand your PBM structure and escalation process
• Create and promote a “self-disclosed / self-identified” culture
• Identify potential issues and act promptly upon them– Description of the issue with specific facts, dates, responsible parties, corrective actions, due dates, and preventive measures
– Identify impacted members and execute a mitigation plan

7
Discuss and Document (Cont.)
• Monitor operational reports (e.g. dashboards)
• Quick escalation of any operational issue that might have compliance risk
• Validate all the information received from the PBM, specially those that needs to be submitted to CMS
• Establish specific due dates and keep track of the progress
Common Part DCompliance Problems
• Timely TrOOP reporting
• Mid-year plan changes by patients
• Post-adjudication adjustments of the financial responsibilities
• Billed claim adjustments
14

8
CMS Targeted Compliance Issues
• CMS is now targeting several areas related to PBM compliance:
– Pharma grants to PBMs
– Remuneration from Pharma
– Payments and rebates from Pharma to PBMs
– Lump-sum payments for formulary inclusion or exclusivity
– Pharma funding for formulary support activities
Effective Compliance
• Robust oversight• Monitoring activities and audits should involve a thorough assessment of key Part D functions including– Accuracy and timeliness of cost controls, systems, and procedures
– Accuracy of management information (e.g. TrOOP, PDE records, DIR, claim data)
– Accuracy and timeliness of claim payments and rebates
– Effectiveness of internal controls

9
Regulatory Framework
• Compliance Program Guidelines– Prescription Drug Benefit Manual – Chapter 9
– Medicare Managed Care Manual – Chapter 21
• Effective Compliance Program– P&Ps and Code of Conduct
– Compliance and FWA trainings
– Communication
– Identification of Compliance Risks
– Prompt Response to Compliance Issues
Monitoring and Auditing of FDRs
• Plan sponsors are responsible for the lawful and compliant administration of the Medicare benefits, regardless of whether it has delegated some of that responsibility to FDRs
• Routine monitoring and auditing– Work Plan
• Risk Assessment• Conduct specific monitoring of FDRs• Corrective action plans• FWA• NBI MEDIC

10
Compliance Collaboration
• Dashboards
• Weekly Med D Meetings
• Monthly Compliance to Compliance Meetings
• Effective Lines of Communications
• Audit Support
• HPMS Memo Discussion Meetings
Compliance
PBMOperations
Thanks!

11
Part D Compliance
PBM Insight
May 2015
Confidential and Proprietary Information
Adriana Ramirez, Esq. General Counsel
&AVP Corporate, Quality and Regulatory
Affairs
© D
iamond M
anagement & Technology C
onsultants, Inc.
abarca health
Confidential
| 22| 22
Contents
Contents
I.• Our Company
II.• Ensuring Compliance with CMS
III.• Importance of Accountability and Oversight
IV• Transparency
V • Questions

12
© D
iamond M
anagement & Technology C
onsultants, Inc.
abarca health
Confidential
| 23| 23
abarca health – Key Facts
Our Company
Abarca Health has grown rapidly during the past three (3) years. We currently have more than 130 local employees and expect to grow to 150 in 2015.
We currently serve more than 2 million lives in Puerto Rico with pharmacy benefit and related services – including more than 150,000 with full Part D PBM Services. Recently signed an Agreement to provide certain services to over 100,000 Medicare Part D lives in the United States
Our proprietary claims adjudication platform (RxEngine™/RxPlatform™) processes over 32 million Rx claims transactions per year with over 18 million claims adjudicated at the point of sale.
In 2014 we have worked with our clients to manage over $950 million pharmacy spend, before more than $140 million in rebates, with $500 million adjudicated at the point of sale.
Four (4) CMS audits or validation exercises conducted in the past 24 months for clients with four (4) unqualified opinions or audits closed with no major issues.
© D
iamond M
anagement & Technology C
onsultants, Inc.
abarca health
Confidential
| 24| 24
What to Expect/Require from your PBM
Regulatory
•Manage and communicate HPMS memos and other regulatory and legal changes via at least weekly updates- summaries and action plans are a must;
•In person meetings at least bi-weekly (Compliance 2 Compliance;
•Require that they ensure employees and delegated entities comply with Compliance/FWA training requirements, receive general compliance information (Policies, and Procedures, Standards of Conduct, Conflict of interest and monthly OIG/GSA verifications);
•Prepare and provide Annual Readiness Checklist assessment;
•Ensure PBM has comprehensive and compliant P&Ps and regularly updates these based on regulatory change and new requirements (at a minimum, annually); and
•Management of the Compliance and FWA hotline.
•Compliance Plan
•Compliance should be across the organization
Monitoring/Auditing (Internal/FDRs)
•Annual Risk Assessment for Client’s review;
•Dedicated internal and FDRs audit and monitoring team;
•Ability to timely gather and QA Audit Universes for Client’s CMS Audits-available to support Client through entire process.
•Internal process for allowing third party audits and oversight-including CMS
•Timely Report issues to Clients that may impact beneficiaries or that are contrary to regulatory guidance to Clients
•Ensure PBM conducts Mock Audit prep; and
•Process to allow third parties to audit operations, claims, rebates, among others.
•Preferibly request that they have some form of Quality Team looking for gaps and improvement
Fraud, Waste and Abuse
•Investigate, track and log FWA potential cases;
•Reviews CMS reports of counties with high incidence of FWA;
•Ability to work directly with clients’ FWA units;
•Conduct Pharmacy Audits;
•Review and develop FWA training for Company/ Rx and other FDRs;
•Ensure potential FWA cases are referred to the Compliance Officer and are handled by FWA Group to evaluate and decide if a case needs to be referred to MEDICS/ determine the right documentation/information to be provided, among others); and
• Ensure Clients are provided with regular updates; and
•FWA division or the like should not limit findings to FWA but should also conduct quality and compliance audits.
Ensuring Compliance with CMS

13
© D
iamond M
anagement & Technology C
onsultants, Inc.
abarca health
Confidential
| 25| 25
The PBM Contract
-The Contract is very important because it sets out each parties’ expectations
but the Contract is only valuable if your relationship with your PBM stems from
trust and transparency- There needs to be openness to disclose.
-Operational Team of Plan cannot delegate this function to the Legal
Department:
– Complete input from the Operational Team is key, especially Compliance;
– Discuss “lessons learned” from prior experiences.
-One contractual term that is often left for interpretation or is vague and both
Parties would benefit from clearer language- avoid disappointments,
frustration, contractual breaches and non-compliance issues:
Report It
Report It
Ensuring Compliance with CMS
Accountability and Oversight
© D
iamond M
anagement & Technology C
onsultants, Inc.
abarca health
Confidential
| 26| 26
Accountability- One possible approach
Request from your PBM an Incident Reporting &
Management Process (include it in the Contract)
� Process must be in writing;
�Specific timeframes for reporting;
�Detail which events may trigger reporting (compliance and
beneficiary access are top priority-provide your PBM with
guidance on what you expect should be reported);
� Establish model format for reporting (description, root cause,
corrective action); and
�Request impact analysis with any relevant data to be
provided to CMS or for internal use (preferably CMS format-
See, CMS Program Audits documentation)
Impact Checklist
� Beneficiary Access Immediate action required
� Compliance Impact� Other
If any of these apply, the issue will require client notification
ReportR AnalyzeA CorrectC EvaluateE
Importance of Accountability and Oversight

14
© D
iamond M
anagement & Technology C
onsultants, Inc.
abarca health
Confidential
| 27| 27
Accountability- One possible approach
Why is reporting important?
It gives PBM and Client the opportunity to improve current processes and solve any issues in a timely fashion- reducing beneficiary impact and
non-compliance risks
It gives Client opportunity to report issue to CMS as a Sponsor Disclosed Issue in accordance with the Part C and Compliance Effectiveness Program
Area (2015)
If correctly and timely reported to CMS, CMS may include the identified claims as an observation noting correction and will NOT negatively impact
the audit score
It’s OK to make mistakes, but let’s make sure we report them!
Importance of Accountability and Oversight
© D
iamond M
anagement & Technology C
onsultants, Inc.
abarca health
Confidential
| 28| 28
• Request from your PBM an Audit Processes for the different types of
audits and ensure PBM has a contact person for each type of audit;
• Request timeframes prior to the submission deadlines for proper QA
of Accountability and Oversight
Importance of Accountability and Oversight
DVA Audits
CMS & Federal
Government Entities
Client Audits
Internal Audits
Data Reporting Requirements provided to Clients/CMS (E.g., Coverage Determinations, Redeterminations, MTMP, LTC Utilization, and Pharmacy Access.)
Timing: On an Annual Basis (Usually March through May of Contract Year)
1. Compliance (Documentation)2. Performance (E.g., TMPA, Coverage Determinations/Redeterminations, Clinical Formulary)3. Financial Appropriateness (E.g., Attestation 1/3 Audits, FIR, PDE, Rebates, Coverage Gap, COB)
Timing: #1 & #2 on Annual Basis (Usually August). #3 on Annual Basis usually in Q3-Q4 of Contract Year.
1. Compliance 2. Pricing (Claims)3. Rebates4. Quality Management and Star Ratings
Timing: As agreed to contractually- Make sure these terms are clear in scope, timing and recovery procedures.
1. Internal Controls2. Internal Monitoring – Compliance or otherwise3. Quality Assurance initiatives4. Quality Management Activities
Timing: As determined by PBM or agreed to with Client
1
4
3
2
Oversight- Audits

15
© D
iamond M
anagement & Technology C
onsultants, Inc.
abarca health
Confidential
| 29| 29
Transparency- Where the market is going
- More sophistication in contractual language and expectations
due to industry pressures;
- Further budgetary restraints/control from Plan Sponsors of
PBM operations as a result of drug price increases and
Specialty Trend;
- More CMS, OIG and other regulatory agency (including State
legislation) oversight; and
- Government payers will set the standard (recent examples:
MAC List publication legislation, provider audit requirements,
transparency or licensing requirements in 11 States)
Transparency
All these factors will increase transparency in the PBM industry
© D
iamond M
anagement & Technology C
onsultants, Inc.
abarca health
Confidential
| 30| 30
QUESTIONS?
Reference

16
© D
iamond M
anagement & Technology C
onsultants, Inc.
abarca health
Confidential
| 31| 31
General Checklist for Contractual Terms For reference only
-Clear definitions (Rebates, Generics, Brands, Specialty);
-Accountability and Oversight (42 CFR 423.505(i)(4))- include issue reporting and resolution provisions as well as clear audit
rights;
-Pharmacy Oversight (Section 6005 of the Affordable Care Act);
-Prompt payment to Network Pharmacies;
-Clear Policies and Procedures and right to review;
-Compliance Offering- HPMS memo and other regulatory change summaries as well as any necessary support
-Frequent performance meetings
-Reporting, Data Submissions and Accuracy- list different reports required and timeframes prior to submission to CMS;
-Record Retention requirements;
-Confidentiality provisions- including ownership of materials;
-BAAs in place, including subcontractors.
-Performance Guarantees not limited to financial terms;
-Compliance with training requirements;
-List of delegated entities and right to audit;
-Execution of BAA from PBM and any delegated entities;
-OIG/GSA monthly verification of employees and contractors;
-Contract should be flexible to adapt to law and regulatory changes without terminating contract;
-Clear process for requesting and documenting any changes to benefit set-up, formulary design, among others; and
-Compliance with (a) applicable Federal laws and regulations designed to prevent fraud, waste and abuse, including but not
limited to applicable provisions of Federal criminal law, the False Claims Act (31 U.S.C. §§ 3729 et seq.), and the anti-kickback
provision of Section 1128B of the Social Security Act; (b) applicable HIPAA Administrative Simplification Security and Privacy
rules at 45 C.F.R. parts 160, 162, and 164; and (c) all other applicable Federal statutes and regulations
Reference