happy hollow children’s camp€¦ · jacket or raincoat flashlight & batteries toiletries...
TRANSCRIPT
Happy Hollow Camp 2018 Dear Parent/Guardian, Thank you for your interest in Happy Hollow Children’s Camp, Inc. For over 60 years now, we have served the lower income families of Marion, Boone, Hamilton, Hancock, Hendricks, and Morgan counties. The camp experience combines recreational and educational programming centered on nature and the outdoors for children between the ages of 7 and 14. Our camp in Brown County is over 900 acres and includes a private lake for swimming, boating, and fishing. Children are housed in cabins with two staff and 6 to 9 campers.
KEEP THIS INFORMATION FOLDER
What is needed for Registration:
Application Form Summer Food Service Form Scope Forms Physical Form (Parent’s information) Physical Form (Physician form)** Bully Prevention Contract (One per Child) Behavior Expectations Contract (One per Child)
**The green physical form is required to fully register your child for camp. *** You will need one application packet per camper. Qualification for scholarship rate is based upon the Summer Food Service Program (SFSP) form (The School Free or Reduced Lunch Program). For those who financially qualify:
Dates For Early Bird Rate Prices Early Bird Rate January - May 4, 2018 $65.00
Full Rate May 7 - July 20, 2018 $85.00 **For those who do not qualify, please contact our office for further pricing.
Once ALL Forms AND PAYMENT are submitted a spot will be reserved for the child. Please note that some campers with special needs may be referred to other camps. In addition, up to $10 per camper may be deposited at Sunday check-in for use at our camp store. Please read over all of the information and feel free to contact the Office in Indianapolis if you still have questions (317) 638-3849.
HAPPY HOLLOW CHILDREN’S CAMP
FOUNDED IN 1951
615 N. Alabama Street, Ground Floor Suite C, Indianapolis, IN 46204 – (317) 638-3849 FAX (317) 686-0195 – e-mail: [email protected]
www.happyhollowcamp.net
“A hundred years from now it may not matter what my bank account was, or the sort of house I lived in, or the kind of car I drove, but the world may be different because I was important in the life of a
child” – Anonymous
INFORMATION TO KEEP IN MIND: 1) Campers will be enrolled in camp on a first come, first serve basis. Happy Hollow Camp is limited to 120 campers per session (60 males and 60 females). When all the camp sessions are full, all other applicants will be placed on a waiting list. To reserve a place for your child this summer, you must return application forms along with the PAYMNET to our Indianapolis office. Please note that $25.00 of the camper fee is considered an application fee and is non-refundable once your child is accepted to camp. YOUR CHILD’S NAME WILL NOT BE ADDED TO THE CAMP ROSTER UNTIL THE COMPLETED APPLICATION FORM, SUMMER FOOD SERVICE FORM, AND THE CAMP FEE IS RECEIVED. NO APPLICATIONS WILL ACCEPTED ONE WEEK PRIOR TO DEPATURE.
MAKE YOUR APPOINTMENT NOW WITH YOUR FAMILY DOCTOR. 2) Due to the actual physical size of the camp and the outdoors emphasis, it is important to realize that a lot of hiking and strenuous activity can take place. A physical examination by a licensed medical practitioner is required prior to attendance at camp: the green physical form included in this application must be used for the physical. The insert page of the green physical form must be completed by a doctor. Be sure to complete the first three pages of the physical form including immunization record. 3) Prescription Medications must be in original containers (no substitute bottles, no combined medications in the same bottle, no baggies, etc.). The label on the bottle or box must match the orders by the physician on the green Health Form. 4) Transportation
Indianapolis Check IN Check In Check Out
Opening Day 1pm-2:00pm Closing Day 12pm
***THOSE ARRIVING AFTER 2:00pm SUNDAY MAY NOT BE ACCOMMODATED BY BUS!!!
5.) NO NIT POLICY: Head lice is a communicable disease and can spread to others: The no nit policy is a public health standard intended to keep children lice free, nit free, in school, in camp, and other areas where children gather. On opening day at check-in all campers will be screened for head lice. Any camper found with head lice or nits will not be able to go to camp. The camper will be temporarily moved to another session and the child’s guardian must treat or have the child treated by medical personnel for this condition. Also, the child’s bedding and clothing must be treated. After treatment and an examination of the child, if no lice or nits are found the child may attend camp. For more information and proper treatment procedures about head lice please visit www.ridlice.com or call 1-800-RID-LICE. 6) Mail is always a great thing to receive at Camp. Please keep it positive and uplifting. It does take a few days to reach camp - you may want to mail any letters prior to your child’s departure for camp. Mail clearly marked with the camper’s name may be sent to:
Attn.: Camper’s Name Happy Hollow Camp
3049 Happy Hollow Rd. Nashville, IN 47448

CAMP REGISTRATION FORM HAPPY HOLLOW CHILDREN’S CAMP, INC. 615 N. ALABAMA ST. GROUND FLOOR SUITE C INDIANAPOLIS, IN 46204 (317)638-3849 FAX:(317)686-0195 Website: www.happyhollowcamp.net Complete both sides of this form and return along with the enclosed SCOPE form, Summer Food Program Form and
the Camp Fee to reserve a spot for your child at camp. PLEASE PRINT THE ANSWERS TO ALL OF THE QUESTIONS.
*Each child is only allowed to sign up attend ONE Session SESSION PREFERENCE (please number 1-5): I – June 10 – 15 ____ Asthma – June 24 – 29 ____ II – July 8 – 13 III – July 15 – 20 _____ IV – July 22 – 27 ____ *If your #1 session preference is full, your child will be placed in the next available session according to your preferences. CAMPER’S NAME __________________________________________ MALE FEMALE
DATE OF BIRTH ___________________ AGE _______ COUNTY ________________________
ADDRESS, APT. #__________________________________________________________________
CITY ______________________________________ STATE ____________ ZIP _______________
PLEASE CIRCLE ONE (ethnicity optional): AFRICAN-AMERICAN ASIAN-AMERICAN CAUCASIAN HISPANIC NATIVE-AMERICAN OTHER _________________________
CAMPER LIVES WITH: 2 PARENTS FEMALE PARENT MALE PARENT GRANDPARENT OTHER _________________ IS CAMPER A FOSTER CHILD __________
PARENT/GUARDIAN_______________________________ PHONE _________________
CELL PHONE __________________ EMAIL ____________________
EMPLOYER _______________________________ PHONE_________________
OTHER PARENT/GUARDIAN ________________________________ PHONE _________________
OTHER EMERGENCY CONTACT ____________________________ PHONE _________________
EMERGENCY CONTACT’S RELATIONSHIP TO CAMPER _______________________
HAS ATTENDED HAPPY HOLLOW CAMP NO YES If yes what year(s)? ___________________
WHAT SCHOOL DOES THE CAMPER ATTEND _____________________________________________________
*CAMPER PICK-UP RELEASE: When my child returns to Indianapolis from Happy Hollow Camp, I give permission for the following person/persons to pick him/her up.
_____________________________ _____________________________ ______________________ Name Relationship Phone
_____________________________ _____________________________ ______________________ Name Relationship Phone
_____________________________ ____________ ____________________ Parent/Guardian Signature Date Phone
2018 Office Use Only:
Date Received __________ Amount Received __________ Camp store Paid __________

Happy Hollow Children’s Camp Asthma Questionnaire
Parents, we are requiring the following questions be answered for all campers attending Happy Hollow Children’s Camp. If your child has Asthma or breathing difficulties, they will need to attend camp during our Asthma camp week. This is to better
provide your child with the medical care that may be required while your child is at camp. During Asthma week, we have more medical staff on site which includes a Doctor. Our camp requires a great deal of walking in heat and humidity. We need to be
sure our medical staff is prepared for your camper's needs. If the HHCC determines (up and including check in day) that it cannot provide adequate supervision or facilities for your child, it reserves the right to terminate enrollment of such campers. Please initial here you read this
1. Has your child ever been diagnosed with Asthma or any type of breathing struggles? yes no If yes, what is the diagnosis?
Continue if answered yes to Question 1
2. How many times a week does your child wake up wheezing/coughing? __________nights/week 3. How many days per week does your child use their reliever (rescue) inhaler? ____days/week 4. How much does your child’s asthma interfere with exercise? NONE SOME A LOT 5. In the past year, has your child been hospitalized due to their asthma or breathing? yes no
If yes, when were they hospitalized?
6. List all medications your child takes due to breathing or Asthma related problems.

WHAT TO BRING TO CAMP Prescription Medications in ORIGINAL CONTAINERS (turned in at Check-in)
Clothing (shorts, shirts, underwear, socks) for 6 days Bug Spray Swim Suit Towels (for swimming & shower) & washcloth Athletic shoes (2 pairs if possible) Sleeping bag or bedroll (sheets & blankets) Jeans or long pants Pillow Jacket or raincoat Flashlight & batteries Toiletries (soap, toothbrush, toothpaste, shampoo, deodorant)
*** Please remember this is camp - what is brought may get dirty, ruined, broken, or lost.
WHAT NOT TO BRING TO CAMP Negative attitude Weapons (including pocket-knives) Electronic games/MP3 Players Food or snacks Alcohol, Tobacco, Other Drugs Gang Apparel Personal Sports Equipment Cell Phones Due to limited phone lines, campers may not call home. If you need to reach your child in an emergency, please contact the office at (317) 638-3849 and we will relay the message.
In Accordance with Federal Law and U.S. Department of Agricultural policy, this institutional is prohibited from discriminating on the basis of race, national origin, sex, age, or disability.
REFUND POLICY FOR HAPPY HOLLOW CAMP
If the parent/guardian chooses to withdraw a camper from a camp session after being enrolled, a refund will be made LESS a $25.00 administrative fee if the parent/guardian notifies Happy Hollow Camps Indy Office within no less than one week (7 days) in advance. NO REFUNDS WILL BE MADE IF THE CAMPER IS WITHDRAWN IN LESS THAN SEVEN DAYS OF OPENING DAY OR IF CAMPER DOES NOT SHOW UP ON OPENING DAY.

GENERAL INFORMATION Happy Hollow Camp is accredited by the American Camp Association - a national organization that assesses program and property safety and the effectiveness of camps. Happy Hollow Camp is also a United Way of Central Indiana agency. All activities are conducted under the guidance of camp staff that has been trained in conducting the activity. Certified lifeguards are on duty during all activities at the lake; life-jackets are worn during all boating activities. Staff is trained in First Aid and CPR, and a nurse is available in camp during each session. Activities generally include one waterfront activity each day (swimming or boating). Other possible activities include: Arts & Crafts, Nature Study, Campouts/Sleep outs, Picnic Lunches, Archery, Gaga Ball, Campfires, Cooking Outdoors, Horseback Riding, Challenge Course, High Ropes Course, etc. Some activities may be limited to older groups due to scheduling or other reasons. Each camper is expected to hike with his/her group to and from activities as needed on our 900-acre property (the lake is not near the group cabins); those not wishing to be in the outdoors or hike with the group will need to discuss this with camp staff prior to applying for camp. A week at Happy Hollow Camp is fun and educational; we hope that you will join us this summer.
HAPPY HOLLOW CAMP GOALS The goals for growth of each camper are achieved through:
• Learning about and enjoying the out-of-doors • Educating participants for safe and healthful living • Modeling the constructive use of leisure time • Developing the unique personality of each person • Practicing democratic group living • Exploring values and meanings. • Strengthening family values by experiencing a cooperative living environment
Send or bring applications to: Happy Hollow Children’s Camp
615 N. Alabama St. Ground Floor Suite C Indianapolis, IN 46204
Thank you to our camp sponsors

CAMPER HEALTH HISTORY FORM 1
Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses
Mail this form to the address below by (date)
Dates will attend camp: from to Month/Day/Year Month/Day/Year
Camper Name: First Middle Last
□ Male □ Female Birth Date Age on arrival at camp: Month/Day/Year
C
amper N
ame ______________________________________________________________________ (For C
amp U
se) Cabin or G
roup____________________ (For Cam
p Use) S
ession Code(s): ________________
First M
iddle Last
To Parent(s)/Guardian(s): Please follow the instructions below. Attach additional information if needed.
1) Complete pages 1, 2 and 3 of this form (FORM 1) and make a copy. 2) Send the original, signed FORM 1 to camp by the requested date. 3) Complete the top of FORM 2 (CAMPER HEALTH-CARE RECOMMENDATIONS) and provide the
copy of FORM 1 with FORM 2 to your child’s health-care provider for review and completion. 4) After it has been completed and signed by your child’s health-care provider, return FORM 2 to
camp by the requested date.
Camper Home Address:
Street Address City State Zip Code
Parent/guardian with legal custody to be contacted in case of illness or injury: Relationship
Name: to Camper: Preferred Phones: ( ) ( ) Email:
Home Address: (If different from above) Street Address City State Zip Code
Second parent/guardian or other emergency contact: Relationship
Name: to Camper: Preferred Phones: ( ) ( ) Email:
Additional contact in event parent(s)/guardian(s) can not be reached:
Relationship Name(s): to Camper: Preferred Phones: ( ) ( )
Allergies: □ No known allergies. □ This camper is allergic to: □ Food □ Medicine □ The environment (insect stings, hay fever, etc.) □ Other (Please describe below what the camper is allergic to and the reaction seen.)
Diet, Nutrition: □ This camper eats a regular diet. □ This camper eats a regular vegetarian diet. □ This camper has special food needs. (Please describe below.)
Restrictions: □ I have reviewed the program and activities of the camp and feel the camper can participate without restrictions. □ I have reviewed the program and activities of the camp and feel the camper can participate with the following restrictions or adaptations. (Please describe below.)
Medical Insurance Information:
This camper is covered by family medical/hospital insurance □ Yes □ No
Include a copy of your insurance card if appropriate; copy both sides of the card so information is readable.
Insurance Company Policy Number
Subscriber Insurance Company Phone Number ( )
Parent/Guardian Authorization for Health Care:
This health history is correct and accurately reflects the health status of the camper to whom it pertains. The person described has permission to participate in all camp activities except as noted by me and/or an examining physician. I give permission to the physician selected by the camp to order x-rays, routine tests, and treatment related to the health of my child for both routine health care and in emergency situations. If I cannot be reached in an emergency, I give my permission to the physician to hospitalize, secure proper treatment for, and order injection, anesthesia, or surgery for this child. I understand the information on this form will be shared on a "need to know" basis with camp staff. I give permission to photocopy this form. In addition, the camp has permission to obtain a copy of my child’s health record from providers who treat my child and these providers may talk with the program’s staff about my child’s health status.
Signature of Custodial Relationship Parent/Guardian Date: to Camper:
If for religious or other reasons you cannot sign this, contact the camp for a legal waiver which must be signed for attendance. Page 1/4
CAMPER HEALTH HISTORY FORM 1 Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses
Camper Name: First Middle Last
Birth Date: Month/Day/Year
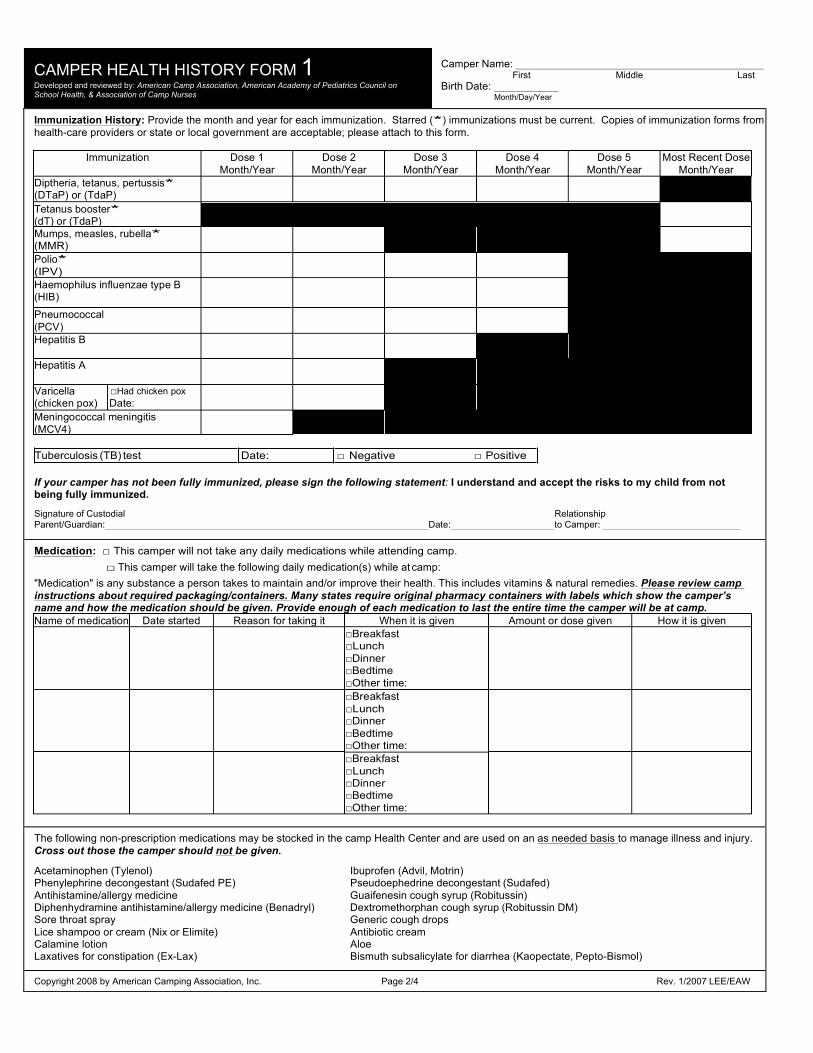
Immunization History: Provide the month and year for each immunization. Starred (*) immunizations must be current. Copies of immunization forms from health-care providers or state or local government are acceptable; please attach to this form.
Tuberculosis (TB) test Date: □ Negative □ Positive
If your camper has not been fully immunized, please sign the following statement: I understand and accept the risks to my child from not being fully immunized.
Signature of Custodial Relationship Parent/Guardian: Date: to Camper:
Medication: □ This camper will not take any daily medications while attending camp. □ This camper will take the following daily medication(s) while at camp:
"Medication" is any substance a person takes to maintain and/or improve their health. This includes vitamins & natural remedies. Please review camp instructions about required packaging/containers. Many states require original pharmacy containers with labels which show the camper’s name and how the medication should be given. Provide enough of each medication to last the entire time the camper will be at camp.
The following non-prescription medications may be stocked in the camp Health Center and are used on an as needed basis to manage illness and injury. Cross out those the camper should not be given.
Acetaminophen (Tylenol) Ibuprofen (Advil, Motrin) Phenylephrine decongestant (Sudafed PE) Pseudoephedrine decongestant (Sudafed) Antihistamine/allergy medicine Guaifenesin cough syrup (Robitussin) Diphenhydramine antihistamine/allergy medicine (Benadryl) Dextromethorphan cough syrup (Robitussin DM) Sore throat spray Generic cough drops Lice shampoo or cream (Nix or Elimite) Antibiotic cream Calamine lotion Aloe Laxatives for constipation (Ex-Lax) Bismuth subsalicylate for diarrhea (Kaopectate, Pepto-Bismol)
Copyright 2008 by American Camping Association, Inc. Page 2/4 Rev. 1/2007 LEE/EAW
Immunization Dose 1 Month/Year
Dose 2 Month/Year
Dose 3 Month/Year
Dose 4 Month/Year
Dose 5 Month/Year
Most Recent Dose Month/Year
(DTaP) or (TdaP)
(dT) or (TdaP)
Haemophilus influenzae type B (HIB)
Pneumococcal (PCV)
Hepatitis B Hepatitis A Varicella (chicken pox)
□Had chicken pox Date:
Meningococcal meningitis (MCV4)
Name of medication Date started Reason for taking it When it is given Amount or dose given How it is given
CAMPER HEALTH HISTORY FORM 1 Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses
Camper Name: First Middle Last
Birth Date: Month/Day/Year
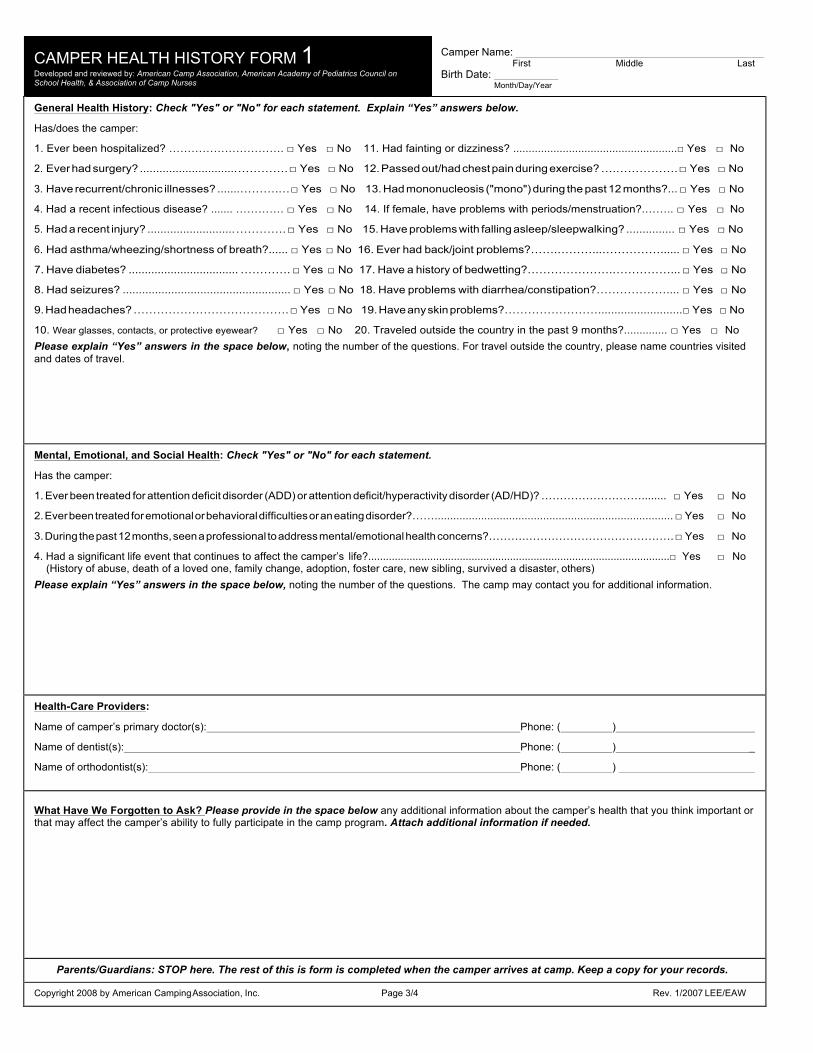
General Health History: Check "Yes" or "No" for each statement. Explain “Yes” answers below.
Has/does the camper:
1. Ever been hospitalized? …………………………. □ Yes □ No 11. Had fainting or dizziness? .....................................................□ Yes □ No
2. Ever had surgery? .............................. …………. □ Yes □ No 12. Passed out/had chest pain during exercise? ….……………. □ Yes □ No
3. Have recurrent/chronic illnesses? .......……….… □ Yes □ No 13. Had mononucleosis ("mono") during the past 12 months?... □ Yes □ No
4. Had a recent infectious disease? ....... …………. □ Yes □ No 14. If female, have problems with periods/menstruation?.…….. □ Yes □ No
5. Had a recent injury? ........................... …………. □ Yes □ No 15. Have problems with falling asleep/sleepwalking? ............... □ Yes □ No
6. Had asthma/wheezing/shortness of breath?...... □ Yes □ No 16. Ever had back/joint problems?…….………...……………...... □ Yes □ No
7. Have diabetes? .................................. …………. □ Yes □ No 17. Have a history of bedwetting?………………….……………... □ Yes □ No
8. Had seizures? .................................................... □ Yes □ No 18. Have problems with diarrhea/constipation?……………….... □ Yes □ No
9. Had headaches? …………………………………. □ Yes □ No 19. Have any skin problems?……………………..........................□ Yes □ No
10. Wear glasses, contacts, or protective eyewear? □ Yes □ No 20. Traveled outside the country in the past 9 months?.............. □ Yes □ No Please explain “Yes” answers in the space below, noting the number of the questions. For travel outside the country, please name countries visited and dates of travel.
Mental, Emotional, and Social Health: Check "Yes" or "No" for each statement.
Has the camper:
1. Ever been treated for attention deficit disorder (ADD) or attention deficit/hyperactivity disorder (AD/HD)? ………………………........ □ Yes □ No
2. Ever been treated for emotional or behavioral difficulties or an eating disorder?……............................................................................. □ Yes □ No
3. During the past 12 months, seen a professional to address mental/emotional health concerns?……….…………………………………. □ Yes □ No
4. Had a significant life event that continues to affect the camper’s life?......................................................................................................□ Yes □ No (History of abuse, death of a loved one, family change, adoption, foster care, new sibling, survived a disaster, others)
Please explain “Yes” answers in the space below, noting the number of the questions. The camp may contact you for additional information.
Health-Care Providers:
Name of camper’s primary doctor(s): Phone: ( )
Name of dentist(s): Phone: ( ) _
Name of orthodontist(s): Phone: ( )
What Have We Forgotten to Ask? Please provide in the space below any additional information about the camper’s health that you think important or that may affect the camper’s ability to fully participate in the camp program. Attach additional information if needed.
Parents/Guardians: STOP here. The rest of this is form is completed when the camper arrives at camp. Keep a copy for your records.
Copyright 2008 by American Camping Association, Inc. Page 3/4 Rev. 1/2007 LEE/EAW
CAMPER HEALTH HISTORY FORM 1 Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses
Camper Name: First Middle Last
Birth Date: Month/Day/Year
Individual Health Record (For Camp Use Only)
Initial Screening Date/Time: Initials:
□ Screening has been conducted according to camp protocol and significant findings noted as follows:
A. Any signs/symptoms of illness or injury upon arrival?........................ □ No □ Yes as noted below
B. History of exposure to communicable disease?.................................. □ No □ Yes as noted below
C. Additions or corrections to information on this health history?............ □ No □ Yes as noted below
D. Medication given to health-care staff?.................................................. □ No □ Yes as noted below
E. Any signs/symptoms of head lice?...................................................... □ No □ Yes as noted below
Provider notes: (date/time/initial all entries)
Exit Note: Check one of the following:
□ Left camp this day with no reported illness or injury symptoms.
□ Left camp this day with the following problem/concern:
This person was told about the problem and instructed about follow-up as noted above:
Date/Time: Initials:
Copyright 2008 by American Camping Association, Inc. Page 4/4 Rev. 1/2007 LEE/EAW
CAMPER HEALTH-CARE RECOMMENDATIONS by LICENSED MEDICAL PERSONNEL FORM 2
Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses
Mail this form to the address below by (date)
To Parent(s)/Guardian(s): Complete this section and give this form (FORM 2) and a copy of your completed CAMPER HEALTH HISTORY FORM (FORM 1) to your child’s health-care provider for review.
Dates will attend camp: from to Month/Day/Year Month/Day/Year
Camper Name: First Middle Last
□ Male □ Female Birth Date Age on arrival at camp Month/Day/Year
Camper home address:
City State Zip Code
Custodial parent(s)/guardian(s) phone: ( ) ( ) Parent(s)/guardian(s) stop here. Rest of form to be completed by medical personnel.
Cam
per Nam
e ______________________________________________________________________ (For Cam
p Use) C
abin or Group____________________ (For C
amp U
se) Session C
ode(s): ________________ First
Middle
Last
The following non-prescription medications are commonly stocked in camp Health Centers and are used on an as needed basis to manage illness and injury. Medical personnel: Cross out those items the camper should not be given.
Acetaminophen (Tylenol) Ibuprofen (Advil, Motrin) Phenylephrine (Sudafed PE) Pseudoephedrine (Sudafed) Chlorpheneramine maleate Guaifenesin Dextromethorphan Diphenhydramine (Benadryl) Generic cough drops Chloraseptic (Sore throat spray) Lice shampoo or scabies cream (Nix or Elimite) Calamine lotion Bismuth subsalicylate (Pepto-Bismol) Laxatives for constipation (Ex-Lax) Hydrocortisone 1% cream Topical antibiotic cream Calamine lotion Aloe
Medical Personnel: Please review the CAMPER HEALTH HISTORY FORM (FORM 1) and complete all remaining sections of this form (FORM 2). Attach additional information if needed.
Physical exam done today: □ Yes □ No (If “No,” date of last physical: ) Month/Day/Year
ACA accreditation standards specify physical exam within last 24 months.
Weight: lbs Height: ft in Blood Pressure /
Allergies: □ No Known Allergies
□ To foods (list):
□ To medications: (list):
□ To the environment (insect stings, hay fever, etc.– list):
□ Other allergies: (list):
Describe previous reactions:
Diet, Nutrition: □ Eats a regular diet. □ Has a medically prescribed meal plan or dietary restrictions:(describe below)
The camper is undergoing treatment at this time for the following conditions: (describe below) □ None.
Medication: □ No daily medications. □ Will take the following prescribed medication(s) while at camp: (name, dose, frequency—describe below)
Other treatments/therapies to be continued at camp: (describe below) □ None needed.
Do you feel that the camper will require limitations or restrictions to activity while at camp? □ No □ Yes
If you answered “Yes” to the question above, what do you recommend? (describe below—attach additional information if needed)
“I have reviewed the CAMPER HEALTH HISTORY FORM (FORM 1), and have discussed the camp program with the camper’s parent(s)/guardian(s). It is my opinion that the camper is physically and emotionally fit to participate in an active camp program (except as noted above.) Name of licensed provider (please print): Signature: Title:
Office Address
Street City State Zip Code Telephone: ( ) Date:
Copyright 2008 by American Camping Association, Inc. Rev. 2/07 LEE/EAW

Happy Hollow Asthma Camp Asthma Symptom Information In addition to the regular Happy Hollow Camp Application and Health Form, please complete this information as well. It will allow our medical staff to understand your child’s asthma.
1. Does your child try and hide their asthma attacks and/ or deny symptoms? Always Sometimes Never
2. Does your child spend nights with friends, grandparents or other relativities?
Yes No
3. Does your child have a fear of particular situation? Yes No If yes, please explain:
4. Asthma History • How long has your child had asthma? years • Do you think your child’s asthma is well controlled? Yes No
Explain, if yes:
• WITH IN THE LAST 3 MONTHS (ON THE AVERAGE): A. How many times a week does your child wake up wheezing/ coughing? nights/ week B. How many days per week does your child use their reliever (rescue) inhaler? days/ week C. How much does your child’s asthma interfere with exercise? NONE SOME A LOT
• WITHIN THE PAST YEAR
A. How many days of school has your child missed due to asthma? Days B. Went to their doctor’s office because of asthma? Times C. Been to the emergency room or urgent care center because of asthma? Times D. Benn on oral steroids (Prednisone, Prelone, Prediapred) because of asthma? Times
• WITHIN THE LAST 5 YEARS
A. Admitted to the hospital for asthma? Yes No How many times? Most Recent B. In an intensive care for asthma? Yes No How many times? Most Recent C. Incubated for asthma? Yes No How many times? Most Recent
AUTHORIZATION TO REALEASE MEDICAL DATA I do hereby release Happy Hollow Children’s Camp to release medical data for the purpose of compiling and assessing national asthma medical information. I understand that all data will be analyzed in aggregate form protecting the confidentiality of my child.
Name: relationship to child Date:
Signature Phone: Work Phone:

Camper’s Name
1.) The HHCC reserves the right to deny participation to any activity, or overnight in which the HHCC, in its sole discretion, deems the participation or presence of the camper would be dangerous or distracting to the camper, to other campers, or to staff members.
2.) For the safety and general welfare of all campers, the HHCC reserves the unrestricted right to
dismiss the camper and terminate the enrollment of the camper if his or her conduct or influence, in the sole opinion of the HHCC is not in the best interests of the HHCC or other campers without providing any refund.
3.) For the benefit of the camper, the HHCC should be made aware of any treatment for emotional,
neurological, physical or psychiatric disorders and/or any restrictions of the camper's activities and the Parent agrees to give written notice to the HHCC of any such conditions. If the camper presents a risk to himself/herself or others, the camper may be discharged at the sole discretion of the HHCC.
4.) Medical forms and Authorization for Medical Treatment must be submitted to the HHCC prior to
June 1, 2017. These forms will be reviewed Medical Professionals to determine which camp session they may attend. The camper will not be allowed to begin camp without up-to-date and complete medical forms and Authorization for Medical Treatment on file with the HHCC.
5.) If the HHCC determines (up and including check in day) that it cannot provide adequate
supervision or facilities for your child, it reserves the right to terminate enrollment of such campers.
6.) The HHCC has the right to share medical information with all staff members whenever the
HHCC deems necessary.
7.) If the camper has Asthma medication medical personal may refer them to our Asthma Camp.
8.) Due to the overwhelming number of requests for campers to be grouped with their friends, it is not possible to honor all requests. The HHCC will therefore be able to process one request per camper. The HHCC shall have the sole right to make final determinations as to bus assignments and grouping arrangements for all campers.
9.) The HHCC will not be responsible for loss of valuables or personal articles including, but not
limited to, cash, jewelry, clothing, electronic devices and athletic equipment.
10.) The HHCC shall have the right to terminate this Agreement in the event that the Parent has made any misrepresentation on the camper registration or medical form. The HHCC will not make refunds if this occurs.
11.) The Parent executing this Agreement acknowledges and agrees that if the camp season is
cancelled or shortened due to Acts of God (by way of example and without limitation: flood, hurricane, earthquake, tornado or other natural disaster), war, terrorism, strike, order of civility, epidemic illness or any other reason beyond the HHCC’s control or if the HHCC determines not

to open camp or to terminate the camp season before the scheduled closing date of the camp season, the HHCC shall not be liable for any consequential or other damage of any kind or nature. The refund of tuition, if any, in whole, or in part, shall be in the sole discretion of the HHCC.
12.) Happy Hollow reserves the right to cancel or modify any camp program because of insufficient
enrollment. The HHCC may, at the HHCC’s sole discretion, attempt to accommodate registered campers in alternate programs operated by the HHCC.
13.) This Agreement constitutes the full understanding of the parties hereto and no change,
modification or waiver of any of the terms shall be effective unless in writing and signed by the Parent and by an authorized representative of the HHCC.
14.) The Parent who signs this agreement represents that he/she has full authority to do so and will be
responsible for payment of all camp fees.
15.) I hereby grant permission for my child to participate in the activities of Happy Hollow Children’s Camp, Inc. [HHCC]. I recognize that, while precautions will be taken for the safety of my child and other campers, children’s outdoor camping includes physical activity and no activity can be rendered completely without risks. My child will be expected to participate in activities chosen by his/her group and to cooperate with and be courteous to fellow campers as well as staff and volunteers. I understand that inappropriate behavior will not be tolerated and that my child may be barred from future participation and/or returned home for serious reasons (fighting, failure to follow rules, etc.). I release and hold harmless HHCC, its board, staff, agents, and volunteers from any damage resulting from the actions of my child. I also grant permission to staff, volunteers, or agents of HHCC to transport my child as necessary for reasons of the camping program or safety while attending HHCC.
PHOTO RELEASE (optional): I hereby give permission for my child to be interviewed, photographed, videotaped, and/or recorded while participating in the programs of Happy Hollow Children's Camp, Inc. and for her/his image/comments to be used for purposes of camp reporting, promotion, advertisement or illustration. Use of any such photographs, videotapes, or interviews may include, but are not limited to, use on Internet Web sites promoting or reporting on American Camp Association or Happy Hollow Children's Camp, Inc. If you agree please initial here
CAMPER FUNDING RELEASE (OPTIONAL): Happy Hollow receives donations to fund our program. Our funders often request data about our campers. For Happy Hollow to receive grant funding for camp programs, I hereby authorize Happy Hollow Children’s Camp to release the following information: Child’s name and last initial, address, dates attended camp and camp evaluation. I understand that the information will be handled confidentially will all applicable federal laws. I understand that I revoke the authorization at any time by written, dated communication. If you agree please initial here
I have read the above Agreement and understand its terms and consent and agree to the same.
Parent Signature Dat

Happy Hollow Children’s Camp Bully Prevention Parent and Camper Contract
(Parent/ Guardian Name) (Child’s Name)
We agree that he/she will not participate or engage in any bullying activity on or off camp property in which the conduct may reasonably carry-‐over into the camp setting and/or interfere with the safety of all children attending camp.
We understand the definition of bullying 1. Any aggressive or negative gesture, or written, verbal or physical act that places another student in reasonable fear of harm to his or her person or property;
2. Any aggressive or negative gesture, or written, verbal or physical act that has the effect of insulting or demeaning any camper in such way as to disrupt or interfere with the Happy Hollow’s educational mission;
3. Any assertion of physical or psychological power over, or cruelty to, another camper; 4. Any behaviors including but not limited to pushing, hitting, threatening, name-‐calling or other physical or verbal conduct of a belittling or intimidating nature;
We, the undersigned, acknowledge and understand the expectation and potential consequences for my child in the above parent and camper contract. We further understand that if my child demonstrates and/or participates in bullying behavior, the behavior will result in the following disciplinary action: 1st Offense: Camper’s name will be reported to a camp administrator. The (Parent/ Guardian) will be contacted to discuss the situation. 2nd Offense: Camper’s name will be reported to a camp administrator and my child will be asked to leave camp.
I (Parent/ Guardian) will arrange for the transportation for my child to leave camp and return home. If I (Parent/ Guardian) or emergency contact cannot be reached within a 24 hour period of time Happy Hollow Children’s Camp Inc. a camp administrator has the right to contact Child Protective Services.
Camper Signature Date
Parent Signature Date

Happy Hollow Children’s Camp Behavior Rules and Expectations
Parent and Camper Contract
(Parent/ Guardian Name) (Camper’s Name) We agree that he/she will be expected to follow rules and expectations while on or off camp property in which the behavior may reasonably carry-over into the camp setting and/or interfere with the safety of all campers attending Happy Hollow Children’s camp. These expectations help to ensure a pleasant experience for all of our campers, volunteers, and staff.
CAMP RULES APPLY FROM CHECK-IN UNTIL CAMPER IS PICKED UP.
BEHAVIOR RULES AND EXPECTATIONS Treat all others with courtesy and respect. Fighting is not allowed. Use appropriate language (no cursing). Everyone helps to keep camp clean. Everyone is expected to take turns with chores. Everyone participates in activities chosen by the cabin group. The buddy system is used for safety.
Each camper is evaluated by his/her counselor, other counseling staff, and program staff in order to assess eligibility for camp next summer and for special activities through the year. You will be mailed your camper’s evaluation.
BUS RULES All camp rules and expectations apply during transportation to and from camp. In addition, the following rules apply:
Campers may not enter or leave the bus without permission from a staff member. No eating, drinking, or use of electronic devises is not permitted on the bus. All campers are to remain seated, facing forward, with head and hands inside the bus at all times. Yelling on the bus or outside the bus or anything that might distract the bus driver or cause harm to another bus rider is not allowed.
We, the undersigned, acknowledge and understand the expectation and potential consequences for my child in the above parent and camper contract. We further understand that if my child demonstrates and/or participates in inappropriate behavior, the behavior will result in the following disciplinary action: 1st Offense: Camper’s name will be reported to a camp administrator. The (Parent/ Guardian) will be contacted to discuss the situation. 2nd Offense: Camper’s name will be reported to a camp administrator and my child will be required to leave camp.
I (Parent/ Guardian) will arrange for the transportation for my child to leave camp and return home. If I (Parent/ Guardian) or emergency contacts cannot be reached within a 24 hour period of time a Happy Hollow Children’s Camp Inc. administrator has the right to contact Child Protective Services.
Camper Signature Date
Parent Signature Date