hap pv
TRANSCRIPT
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 1/22
By. Dr. Ihsan Affandi
Inhaled Anesthetics
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 2/22
y
• The discovery of the anesthetic properties of nitrous oxide,
diethyl ether, and chloroform in the 1840s
•
1951, fluroxene, was used clinically for several years beforeits voluntary withdrawal from the market due to its potential
flammability and increasing evidence that this drug could
cause organ toxicity
• Halothane was synthesized in 1951 and introduced for clinical
use in 1956
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 3/22
Enflurrane, the next methyl ethyl ether derivative, was
introduced for clinical use in 1973 In search of a drug with fewer side effects, isoflurane, the
isomer of enflurane, was introduced in 1981
Methoxyflurane, a methyl ethyl ether, being introduced for
clinical use in 1960
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 4/22
•Desflurane, a totally fluorinated methyl ethyl ether, was introduced in 1992
•Followed in 1994 by the totally fluorinated methyl isopropyl ether,
sevoflurane
•
The low solubility in blood of these newest anesthetics was desirable•Facilitate the rapid induction of anesthesia, permit precise control of
anesthetic concentrations during maintenance of anesthesia
•Favor prompt recovery at the end of anesthesia independent of the duration of
administration
•Desflurane and sevoflurane reflects in large part the impact of market forces
more than an improved pharmacologic profile on various organ systems as
compared will isoflurane
Inhaled Anesthetics for the Present & Future
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 5/22
•Commonly administered include the inorganic gas nitrous oxide and the
volatile liquids isoflurane, desflurane, and sevoflurane
•Halothane and enflurane are administered Infrequently but are included in the
discussion of the comparative pharmacology of volatile anesthetics since
halothane in particular has been studied extensively
•Available but rarely administered inhaled anesthetics include the volatile
liquids methoxyflurane and diethyl ether and the cyclic hydrocarbon gas
cyclopropane
•Xenon is an inert gas with anesthetic properties, but its clinical use is hindered
by its high cost
CLINICALLY USEFUL INHALED ANESTHETICS
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 6/22
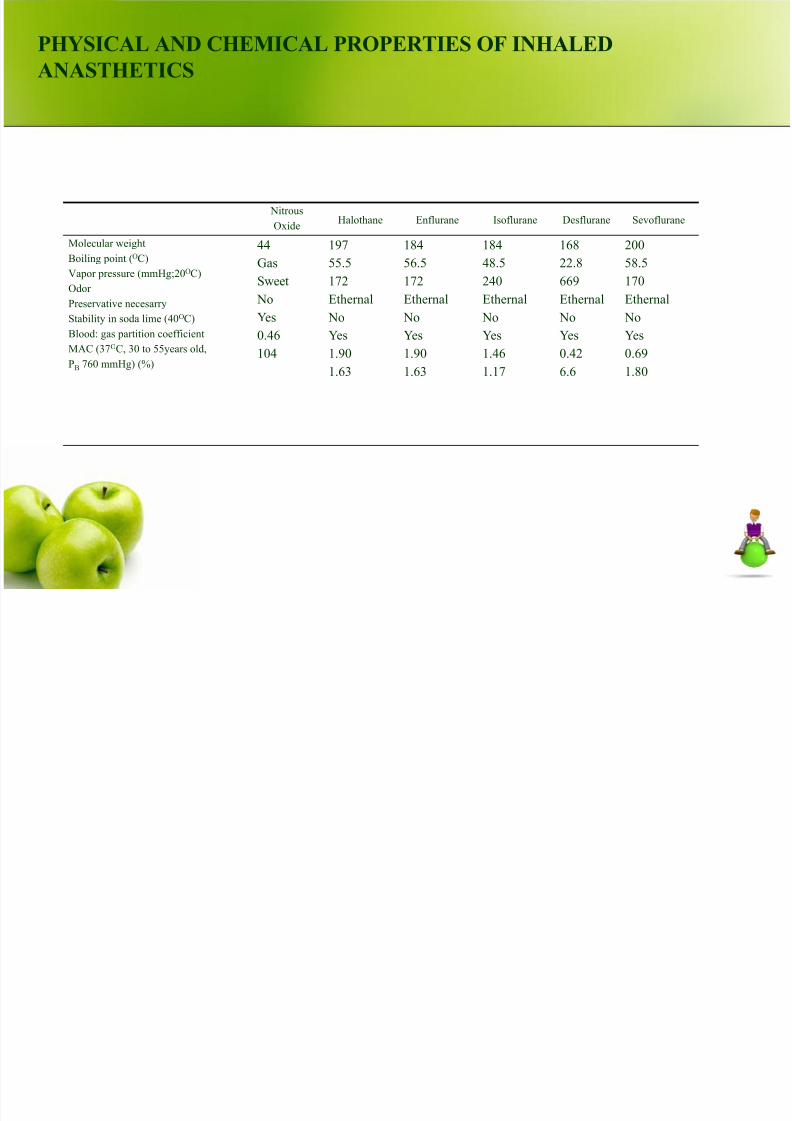
PHYSICAL AND CHEMICAL PROPERTIES OF INHALED
ANASTHETICS
Nitrous
Oxide Halothane Enflurane Isoflurane Desflurane Sevoflurane Molecular weight Boiling point (OC) Vapor pressure (mmHg;20
O
C) Odor Preservative necesarry Stability in soda lime (40OC) Blood: gas partition coefficient MAC (37OC, 30 to 55years old, PB 760 mmHg) (%)
44 Gas Sweet
No Yes 0.46 104
197 55.5 172 Ethernal
No Yes 1.90 1.63
184 56.5 172 Ethernal
No Yes 1.90 1.63
184 48.5 240 Ethernal
No Yes 1.46 1.17
168 22.8 669 Ethernal
No Yes 0.42 6.6
200 58.5 170 Ethernal
No Yes 0.69 1.80
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 7/22
Riwayat Keluarga
Tidak ada keluarga pasien yang sakit seperti ini
Riwayat perkawinan : 1 x tahun 1998
Riwayat kehamilan / abortus / persalinan : 4/0/3
PEMERIKSAAN FISIK
KU : sedang Sianosis : -
Kes : sadar Ikterik : -
TD : 120/80 mmHg pucat : -
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 8/22
Nadi : 96 x/menit
Nafas : 22 x/menit
T : 37 C
Mata : tidak anemis, tidak ikterik, pupil isokor ki=ka
Telinga, hidung dan tenggorokan : tak ada kelainan
Leher : KGB tidak membesar
Dada : paru dan jantung dalam batas normal
Ekstremitas : akral hangat, edema -/-
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 9/22
STATUS OBSTETRI
Abdomen :
Inspeksi: tampak membuncit sesuai usia kehamilan aterm
Palpasi :
L I : FUT 3 jari bpx, teraba massa besar, lunak, noduler
L II : teraba tahanan terbesar di kiri
L III : teraba massa bulat, keras, floating
L IV : tidak dilakukan
Taksiran berat anak : 2945 gr, TFU : 32 cm, Hiss (-)
Perkusi : timpani
Auskultasi : BU (+) normal ; BJA : -
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 10/22
Genitalia : Inspeksi U/V tenangInspekulo : darah (+) warna merah segar, stosel (+)menutupi portio, laserasi (-)
Laboratorium : Hb : 10,7 g/dl Hematokrit : 35 %CT : 3’ BT : 4’
Leu : 12400 mm³ Trombosit : 178000/mm³
Diagnosis Kerja : G4P3A0H3 gravid aterm 38-39mgg + HAP ec susp placenta previa + susp IUFD
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 11/22
Terapi
O2 3 liter/’
IVFD RL tetesan cepatKONSUL SpOG
• Kontrol KU, VS, perdarahan pervaginam
•
Pasang kateter urine• Ceftriaxone inj 1 x1 gr iv
• Persiapkan contoh darah untuk crossmatch
•
Rencana sectio sesarea sito
Diagnosis BandingHAP ec solusio placenta
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 12/22
Laporan Operasi
Dilakukan SCTPP ai HAP ec placenta previa,lahir seorang bayi perempuan dengan BB :
2700 gr, PB : 47 cm, A/S : - (IUFD), sisa ketubanhijau kental, placenta lahir lengkap 1 buah,berat 500 gr, perdarahan selama tindakan 300
cc, BAK lancar via cateter 100cc/sewaktu
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 13/22
FOLLOW UP POST OP
Pukul 18.00 WIB
S / Demam (-), BAK (+) terpasang kateter
0 / Ku : sedang Kes : sadar
Nfs : 20 x/’ TD : 120/80 mmHg T: afebris Nadi : 82 x/’
Abdomen, I : tampak sedikit membuncit,
luka operasi tertutup verbanPa : FUT 2 jari bawah pusat
kontraksi uterus baik
NT (-), NL (-), defans muscular (-)
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 14/22
Genitalia : V/U tenang, PPV (+)↓ A/ P4A0H3 Post SCTPP ai placenta previa, ibu dalamperawatan + anak meninggalP /Awasi KU, VS, PPV post SCTPPDiet TKTPMobilisasi bertahap
IVFD RL 20 tetes/’ Ceftriaxon inj 1 x 1 gr ivMetronidazole infus/8 jamInvitex/ 4 jam suppositoria 2 x pemberian
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 15/22
Pukul 23.00 WIB
Hb post op : 8,1 gr/dlRencana : transfusi darah, namun keluargabelum mendapatkan pendonor
Tanggal 5-10-2010 S / Demam (-), BAK (+) terpasang kateter
BAB (+), PPV (-)0 / Ku : sedang TD 120/100 mmHgKes : sadar Nfs : 20 x/’ T: afebris Nadi : 80 x/’
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 16/22
Abdomen, I : tidak tampak membuncitluka operasi tertutup verban
Pa : FUT 2 jari bawah pusat
kontraksi uterus baikNT (-), NL (-), defans muscular (-)Genitalia : V/U tenang, PPV (-)Kesan : perbaikan
A/ P4A0H3 Post SCTPP ai placenta previa, ibu dalamperawatan + anak meninggal + Nifas hari ke-1
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 17/22
P /Breast careMobilisasi bertahap
IVFD RL 20 tetes/’ Transfusi darah 2 kolf pukul 13.00 dan 22.00Ceftriaxon inj 1 x 1 gr ivCiprofloxacin 2 x1 po
Metronidazole aff ganti oral 3 x 1 tabViliron 1 x1 poAsam mefenamat 3 x 1 poLinoral 3 x 1 po
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 18/22
Tanggal 6-10-2010
S / Demam (-), BAK (+), BAB (+), PPV (-)0 / Ku : sedang TD 120/100 mmHgKes : sadar Nfs : 20 x/’T: afebris Nadi : 80 x/’
Abdomen, I : tidak tampak membuncitluka operasi tertutup verban
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 19/22
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 20/22
Tanggal 7-10-2010
S / Demam (-), BAK (+), BAB (+), PPV (-)0 / Ku : sedang TD 120/100 mmHg
Kes : sadar Nfs : 20 x/’T: afebris Ndi : 80 x/’ Abdomen I : tidak tampak membuncit
luka operasi tertutup verbanPa : FUT 2 jari bpst
kontraksi uterus baikNT (-), NL (-), defans muscular (-)
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 21/22
Genitalia : V/U tenang, PPV (-)A/ P4A0H3 Post SCTPP ai placenta previa, ibudalam perawatan + anak meninggal + Nifashari ke-3P / Terapi lanjut
7/27/2019 HAP PV
http://slidepdf.com/reader/full/hap-pv 22/22
TERIMA KASIH