hand-free stethoscope — method and instrument for more reliable blood pressure measurements
TRANSCRIPT
Journal o f ln te rna l Medicine 1991; 2 3 0 : 213-217
Hand-free stethoscope - method and instrument for more reliable blood pressure measurements
P. L J U N G V A L L & T. THULIN From the Deportment of Internal Medicine. Universitu Hospital Lund. Lund. Sweden
Abstract. Ljungvall P, Thulin T (Department of Internal Medicine, University Hospital Lund, Lund. Sweden). Hand-free stethoscope - method and instrument for more reliable blood pressure measurements. Journal of Internal Medicine 1991 : 2 3 0 : 2 13-21 7.
Measurement of blood pressure is subject to two sources of variation: biological and measurement variation. It is important to bear in mind that the ability to interpret the Korotkoff sounds correctly determines the levels of both systolic and diastolic blood pressure. To improve the ability to distinguish between the Korotkoff phases, the hand- free stethoscope and the hand-free method were developed. The improved stethoscope head was fixed under the edge of the cuff, thus reducing the noise generated from physiological tremor and other movements. This resulted in more distinct Korotkoff sounds. Furthermore, the new method reduced the spreading of blood pressure values. In 107 patients the average systolic ,blood pressure recording was 3.1 mmHg higher and the average diastolic blood pressure was 3.5 mmHg lower. We conclude that the new stethoscope and technique provide a means of significantly improving the indirect measurement of blood pressure.
Keywords: blood pressure measurement, hand-free method, hand-free stethoscope, Korotkoff sounds.
Introduction The stethoscope is one of the most widely used medical instruments, and has now become a symbol of the medical profession. When the French physician Rent! Laennec presented his innovation in 1819 it was given the name ‘stethoscope’ [l]. This word is derived from the Greek words stethos ( = chest) and skopeo ( = observe). The shape of the conventional stethoscope indicates that the instrument was orig- inally intended for auscultation in patients with heart and pulmonary diseases.
The Russian physician Nicolai Korotkoff found the stethoscope useful for the indirect measurement of blood pressure (BP) [ 2 ] . He reported that the first and last pulse sounds during auscultation of the brachial artery corresponded very closely to the systolic (SBP) and diastolic (DBP) blood pressure.
Abbreviations: BP = blood pressure. SBP = systolic blood pressure, DBP = diastolic blood pressure, HFS = hand-free stethoscope, SD = standard deviation.
The level of arterial BP is an important index both of cardiovascular function and of the risk of future cardiovascular morbidity and mortality. With time the overlap between normotension and hypertension has declined. It is therefore important that the BP values obtained do in fact provide an accurate indication of the patient’s true BP.
Indirect methods for BP measurement are based on work by Riva-Rocci [3] and Korotkoff [2]. Several factors may affect the measurement of BP, and much attention has been paid to the quality of the equipment, the recording technique and general standardization of the measurements [4]. However, the technique of BP determination still requires further improvement.
Sometimes the genuine beginning and disappear- ance of the Korotkoff sounds are difficult to detect due to the low level and frequency of the sounds [S] relative to the background noise. If one Korotkoff sound is lost at the beginning or the end, this will result in a falsely low SBP value and/or too high a DBP value. Noise from sources around the stetho-
213

214 P. L J U N G V A L L & T. THULIN
Table 1. Different sources of accessory sounds and noise during BP measurement
Physiological tremor from the hand Hand movements of the examiner Patient movements Finger and nail movements against the stethoscope Noise from the twist mechanism Light and thin material of the stethoscope head Rough surface of the stethoscope head Movements against the cuff
Fig. 1. The hand-free stethoscope placed under the edge of the cuff.
scope (Table 1) will also impair the observers’ ability to distinguish the Korotkoff sounds correctly.
The aims of the present study were firstly to manufacture a stethoscope more suitable for the hand-free method (Fig. l), and secondly to compare the BP values obtained with the hand-free stetho- scope (HFS) with the values obtained using the common technique of BP measurement.
Methods and study population
The hand-free stethoscope ( H F S )
The head of the stethoscope was manufactured of a chrome-plated and quite heavy bronze material in order to reduce friction. This had the effect of decreasing the sensitivity to environmental noise, particularly noise arising from direct contact. The thickness of the wedge-shaped head was 8 mm, while the conventional stethoscope is approximately 25 mm thick. Furthermore, the material used in the majority of conventional stethoscope-heads is light,
thin and/or rough. Consequently, such stethoscopes will take up and transmit more of the different sounds from the environment via the tube to the ears than will a stethoscope-head made of a chrome- plated bronze material. The thin, wedge-shaped head, with no projecting parts, allowed it to be simply placed between the cuff and the upper arm. In addition, the tube is connected directly to the stethoscope head to prevent noise from the ordinary twist mechanism. When the stethoscope-head is fixed under the edge of the cuff the measurements can be performed without the hand on the stetho- scope. Thus the tube can run freely between the stethoscope-head and the tube-ear connection. This prevents accidental contact with sensitive parts of the stethoscope, resulting in a reduction in noise.
Recording of noise with conventional stethoscope and H F S
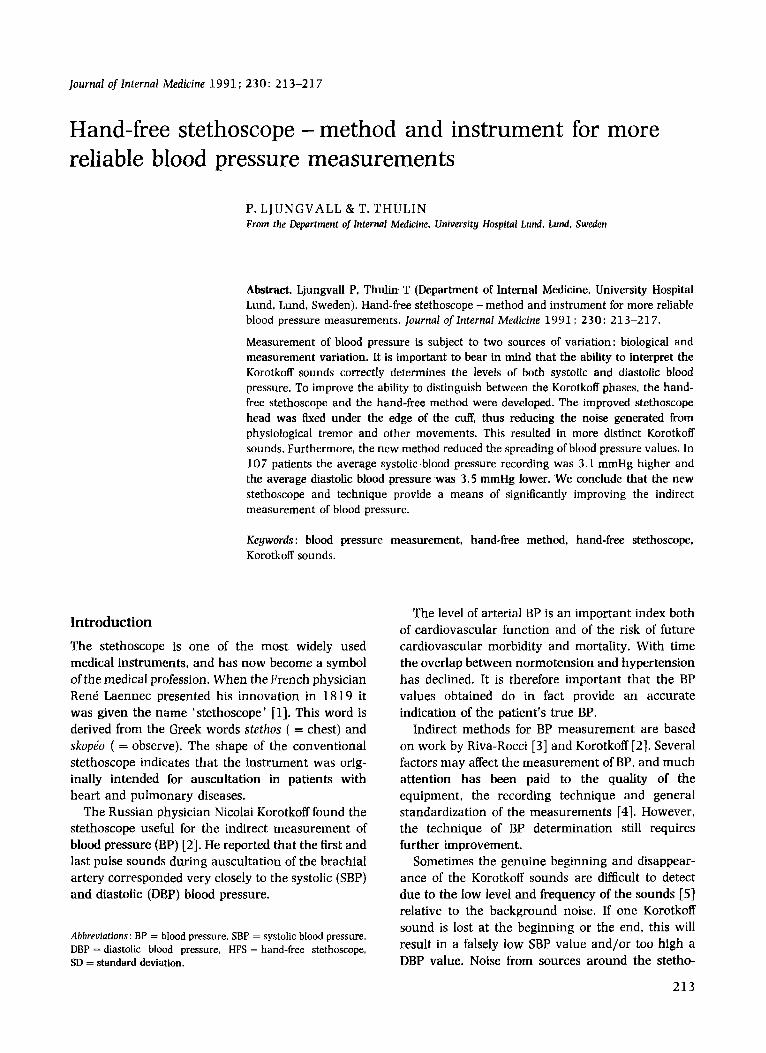
The conventional stethoscope and the HFS were used to compare the presence of noise in 10 subjects when the two methods were used. Electrocardiogram (ECG) and doppler were used as pulse indicators. The doppler was placed below the arm cuff over the brachial artery to indicate the appearance of the blood flow. This was done in order to study the correlation between the appearance of the blood flow and the first Korotkoff sound.
There was agreement between the first doppler signal and the first Korotkoff sound in all the measurements performed with the HFS. However, when the conventional stethoscope was used, the first doppler signal was missed in seven subjects, and in three of these the second signal was also lost.
As agreement was found between the first doppler signal and the first Korotkoff sound with the HFS, the study proceeded without doppler recording.
The tube from each of the two stethoscopes was attached via a Y-connection to a microphone. This was placed inside the tube 1 5 cm from the head of the stethoscope. The noise from the conventional stethoscope and the HFS was recorded simul- taneously on a printer. The printer graph showed a clear improvement of the signal-noise ratio in the case of the HFS in all 10 recordings (Fig. 2).
During this part of the study, when the HFS was compared with the conventional stethoscope, dif- ferent tests were performed in order to determine the optimum procedure for evaluation of the two methods. All attempts showed that it was impossible
M O R E RELIABLE BLOOD PRESSURE MEASUREMENTS 215
ECG
Doppler
Conventional stethoscope
Hand-free stethoscope
Fig. 2. The printer graph reveals a distinct improvement in the signal-noise ratio with the use of the HFS.
to accomplish a blind evaluation of the two stetho- scopes. Although the examiners were unaware of what was at the other end of the stethoscope tube, the HFS was always recognized, owing to its noiseless background.
Study population
In a sample of 107 hypertensive patients (67 men and 40 women) aged 20-76 years, three experienced nurses performed 428 measurements of BP. The nurses were instructed to measure the BP with the same accuracy and care as usual, and they were not informed of any possible differences between the stethoscopes with regard to detection of the Korotkoff sounds. The BP recordings were made after resting for approximately 10 min with the patient lying horizontal and the arm resting on the heart level pillow [6]. The cuff size was adjusted to the arm circumference, and the readings were made on a mercury manometer. The first and fifth Korotkoff phases were taken as the SBP and DBP, respectively
The head of the HFS was placed over the brachial artery and fixed just under the edge of the cuff, and the BP was measured without the hand on the stethoscope. The conventional stethoscope was posi- tioned manually over the artery in the fossa cubiti. In
~71.
each patient the BP was measured four times on the same arm by one nurse using a single-headed stetho- scope.
The conventional stethoscope and the HFS were used in the following order : conventional +
HFS + conventional + HFS. After each BP measurement the results were
recorded separately according to a protocol that avoided observer bias before the results were com- pared and interpreted.
Statistical analyses
The data are expressed as mean valuesf SD. Statis- tical analyses were performed using Student’s t-test.
Results The ranges for systolic and diastolic blood pressure were 102-200 and 52-120 mmHg, respectively. The differences between SBP and DBP recorded by the conventional stethoscope and the HFS were significant (P < 0.001) for both comparisons. The mean values ( f SD) for SBP and DBP, respectively, with the conventional stethescope and the HFS were 1 3 4 f 1 9 / 7 9 + l l and 137+21/76+11 mmHg at the first recording and 1 3 2 f 1 9 / 7 9 f l l and 13 5 f 20/ 76 f 10 mmHg, at the second recording.
216 P. L J U N G V A L L & T. THULIN
Thus, at the first comparison, SBP and DBP recordings were on average 2.6 mmHg higher and 3.4 mmHg lower, respectively, when the HFS was used. At the second comparison SBP and DBP were 3.5 mmHg higher and 3.6 mmHg lower, respect- ively, when the HFS was used.
When the two methods were compared, the HFS showed higher SBP values in 13 1 (6 1 %) and lower DBP values in 15 5 (73 %) of the 2 14 measurements.
Discussion Our results confirm that the BP values obtained are influenced by the ability to hear the weak Korotkoff sounds. When using the conventional method of auscultation, different sources of accessory sounds are present. This may impair the accuracy of the BP recordings. In general the noise is caused by move- ments against the stethoscope-head, but it can also be due to noise in the room.
The frequency and amplitude of the accessory sounds are often similar to the Korotkoff sounds. This implies an obvious risk of the sounds becoming masked by disturbances at the beginning and end of the BP measurements. The most common disturb- ance probably emanates from the physiological tremor in the hand of the examiner. The frequency of the tremor ranges from 8-12 Hz [8]. This vibration is transformed into audible sound waves in the stetho- scope. Experienced examiners are generally adapted to the existence of such noise and will for that reason barely be affected by it. This also means there is a risk of losing one or more of the rather Korotkoff-like sounds. Other sources of accessory sounds and noise during BP measurement are shown in Table 1. These disturbances are more or less involved during the conventional measurement of BP. Electronic ampli- fication of the signal from the stethoscope will also result in a linear increase in noise. One effective way of decreasing the background noise is to avoid touching the stethoscope-head during BP measure- ment.
A further advantage of not holding the hand over the stethoscope head is that the examiner has one hand free to palpate the pulse and so eliminate the potential risk of a ‘silent gap’ during the BP measurement. The design of the stethoscope head makes it easy to place between the edge of the cuff and the upper arm.
During a BP measurement the closing of the brachial artery occurs in a circular region along the
cuff where the greatest capacity for expansion is located. As the head of the HFS is placed just under the edge of the cuff, it does not alter the blood flow and/or the Korotkoff sounds.
In the indirect method of BP measurement the SBP usually corresponds to Korotkoff phase 1 and the DBP corresponds to phase 5. However, simul- taneously performed measurements of the intra- arterial BP indicate that the SBP is underestimated by 5-10 mmHg and the DBP is overestimated by approximately the same amount [9]. This may be due to the fact that the examiner often fails to detect the very first and last Korotkoff sounds because they may be too weak to be audible. In fact, when BP is determined, only the first and last Korotkoff sounds are of value. Therefore all other accessory sounds are disturbances that may impair the accuracy of the BP recording.
The doppler equipment was used to indicate the start of blood flow in the brachial artery as the cuff pressure was gradually reduced. The doppler showed a correlation between the first blood flow and the first audible Korotkoff sound, i.e. the SBP, in all measure- ments when the HFS was used.
However, the doppler is limited to indicating the start and end of blood flow. For this reason, only the first Korotkoff sound could be compared to the first doppler signal. The determination of DBP is totally dependent on the ability to identify the fifth Korotkoff phase or, when necessary, the change in sound character between the fourth and fifth phase. An increased ability to detect the weaker Korotkoff sounds as well will shift the SBP values upwards slightly and, consequently, the DBP values will decrease slightly.
Another effect of detecting the weak Korotkoff sounds is a reduction in spreading of the BP values due to variations in the hearing ability of the examiners. Using the HFS and hand-free method, more examiners will detect the genuine beginning and disappearance of the Kortokoff sounds.
If the examiner fails to detect one or two Korotkoff sounds in the beginning, the SBP will be under- estimated. If he fails to detect one or two Korotkoff sounds at the end of the measurement, the DBP will be overestimated.
Another well-known problem in BP measurement is the never-ending Korotkoff sounds due to an increased blood flow. In such situations the HFS can make it easier to detect the change in sound character between the fourth and fifth Korotkoff phases.

MORE RELIABLE BLOOD PRESSURE MEASUREMENTS 217
An improved ability to distinguish the Korotkoff sounds will not just move the BP values obtained by the indirect method in the direction of the intra- arterial BP values, but it will also reduce the spreading of these values, and consequently improve the reliability of the recordings. For these reasons we consider that the new HFS technique provides a means by which the indirect measurement of BP can be significantly improved.
REFERENCES Laennec RTH. De Lauscultation Mediate. ou Trait6 du Diagnostic des Maladies des Pournons et du Coeur. Fond6 Principlernent sur ce Nouveau Moyen dExploratin. Paris: JA Brosson & jS Chaude. 1819. Riva-Rocci S. Un nuovo sfigmomanometro. Cazz Med Torino
Korotkoff NS. A Contribution to the Problem of Methods for the 1896: 47: 981-96.
Determination of the Blood Pressure. II. St Petersburg : Bull Imp Military Med Acad. 1905: 365-67.
4 The 1988 Report of the joint National Committee on Detection, Evaluation. and Treatment of High Blood Pressure. Arch Intern Med 1988: 148 (5): 1023-38.
5 Gupta R. Miller JW, Yoganathan AI’. Udwadia FR. Corcoran. WH. Kim BM. Spectral analyses of arterial sounds. Non- invasive methods of studying arterial disease. Med Biol Eng Cornput 1975: 1 3 : 700-5.
6 Ljungvall P. Thorvinger B. Thulin T. The influence of the heart level pillow on the result of blood pressure measurement. ] H u m Hypertens 1989: 3 : 471-4.
7 Thulin T. Andersson C. Schersten B. Measurement of blood pressure, a routine test in need of standardization. Postgrad Med ] 1975: 51: 390-95.
8 Elbe RJ. Physiologic and essential tremor. Neurology 1986:
9 Burch E. De Pasquale NP. Primer of Clinical Measurement of Blood Pressure. St Louis: The C.V. Mosby Company, 1962:
36: 225-31.
102-3.
Received 5 November 1990, accepted 7 February 1991.
Correspondence : Thomas Thulin. MI) Phl). Department of Internal Medicine, University Hospital of Lund, S-221 85 Lund. Sweden.