hamstring strain mora modisette spaulding framingham - august 27, 2015
TRANSCRIPT

Hamstring StrainMora Modisette
Spaulding Framingham - August 27, 2015

Agenda• Anatomy quick review• Mechanisms of injury• Incidence• Risk factors• Evaluation• Treatment/Research• Prevention

Hamstring Quick Review7,16
• 2-joint stabilizing muscle
• Limits anterior & lateral tibial translation
• Biceps femoris – ER of semi-flexed knee– Dual nerve innervation

Mechanism of Indirect Injury 6,8,14,16
1. Terminal swing phase in high speed running
2. Overstretching
3. Repetitive micro trauma


Incidence6,8,10,18
• 37% of all soccer injuries with up to 33% recurrence rate
• 12% of Football players• Tendinopathies from overuse = rare
– No incidence reports

Risk Factors: Non-modifiable11,14,16-18
• Previously HS strain = 5x risk of reinjury• Previous injury proximal or distal to HS• Age
– 9-19 yo : training time / exposure– > 40 yo: of skeletal muscle mass
• Ethnicity: African American or Aboriginal• Male > female

Risk Factors: Modifiable6,11,16-8
• Contact sport (44-47% of all injuries)• Lack of flexibility• QS:HS imbalance• Fatigue• Poor neuromuscular control• Poor lumbopelvic control/stability
– (anterior pelvic tilt)
• Poor running technique

Evaluation of HS Strain3,7-8,14
• ROM: SLR and Supine 90/90• MMT
– Prone knee flexion with 15˚ and 90˚ knee flexion – Hip extension with knee at 0˚ and 90˚ flexion
Can bias medial or lateral hamstrings with IR or ER
• Palpation– Measure distance of max pain with knee in
extension from ischial tuberosity more proximal = longer recovery time
– Measure length of painful region

Special Test: Puranen–Orava2
• Actively stretching hamstring in standing with hip flexed 90°, knee fully extended and foot supported

Special Tests: Bent-Knee Stretch & Modified Bent-Knee Stretch2

Functional Tests8
• Squats• Single limb squat• Gait analysis• Running gait analysis• Outcome measures:
– LEFS– GROC

Differential Diagnosis7-8
• Neural Tension/Entrapment• Adductor Strain• Piriformis syndrome• Ischogluteal bursitis• Impingement• Lumbar disc dysfunction• Spondylosis• SIJ

Prognosis3,7,14
Longer Recovery• Close to ischial
tuberosity• Disruption of central
tendon• Surgery required• Larger lesion• Significant ROM• Time to walk > 24 hrs
Shorter Recovery• Far from ischial
tuberosity• Injury to adjacent
muscle fibers & intramuscular tendon
• Time to walk < 24 hrs

Interventions6,11,13-15,18
• No conclusive high level evidence • Currently treat eccentric and overstretch
injuries the same• Trunk stability and agility exercises = may
be effective in minimizing reinjury• Prevention: RCTs indicating eccentric
training prevents HS injury

Phase 17,12
• Goals: protect scar development, minimize atrophy• Protection: avoid excessive HS lengthening• Modalities
– Ice: 2-3x daily– US (duty cycle 50%, 1 MHz, 1.2 W/cm2)
• Therex (daily) – all pain free– Stationary bike – Fast side stepping – Grapevine – Fast stepping in place– Planks/Side plank– SLS progressions– Bridging– Submax isometrics at 3 angles (90˚, 60 ˚, 30 ˚)

Criteria for progression to Phase 27,12
• Normal walking, pain free• Slow speed jog without pain• Pain free submax HS MMT in prone with
90˚ knee flexion

Phase 27,12
• Goal: regain pain free HS strength, begin lengthening, develop lumbopelvic control with speed
• Protection: avoid end range HS lengthening while weakness persists
• Modalities: Ice post exercise– STM/IASTM– Dry needling
• Therex (5-7x a week)– Continue bike, side steps, grapevine, & SLS progressions– Boxer shuffle– Rotating side plank– Start eccentrics

Criteria for Progression to Phase 37,10,12
• 5/5 pain free MMT of HS in prone with 90˚ knee flexion
• Pain free fwd & bwd jog, medium intensity• Strength deficit < 20% of uninjured limb• Pain free max eccentric in non-lengthened
state

Phase 37,12
• Goal: symptom free, normal MMT & ROM, integrate sport-specific movements
• Protection: avoid full intensity if tight/stiff• Modalities: ice as needed, STM
• Therex (4-5x a week)– Progress eccentrics– Dynamic HS stretching– Plyometrics– Accelerations/decelerations (5-10 yards)

Criteria for Return to Sport7,12
• Full pain free strength in lengthened state
• Full pain free ROM• Symmetry in knee flexion
peak torque• Replication of sport
specific movements at competition speed without symptoms

Progression of Eccentrics10
1. Open chain, NWB– Low velocity eccentrics
3. Closed chain, WB, multi-joint
4. Plyometrics / higher speed eccentrics
5. Sport specific movements:
uni→multi-directional

Beginning Eccentrics7,12,14
• Bridge walk outs• Nordic curls• Prone HS curls• SLS windmills• Walking lunge with T-lift

Nordic Curl10

Possible Progressions• Single leg dead lifts• Split squats/box lunges• Windmills with wt or standing
on ½ foam roll• SLS with fwd trunk lean and
opposite LE hip ext

Multi-joint, Closed Chain Eccentrics10
A: Resisted forward pull
B: Resisted backward push
C: Lunge Drops
A
B
C
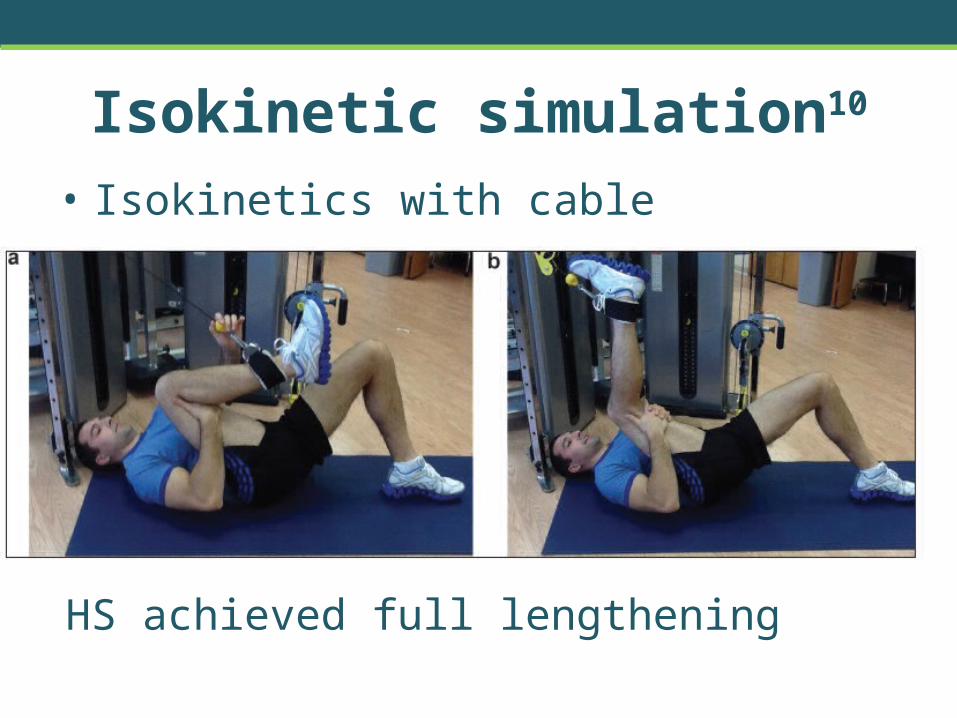
Isokinetic simulation10
• Isokinetics with cable
HS achieved full lengthening

High-speed Eccentrics7,13
• A-skip– Video 1– Video 2
• B-skip• Prone foot catches with ankle weight • Standing 1 leg foot catches

Treadmill Eccentrics Case4
• 34 yo triathlete• 4 weeks of symptoms, insidious onset• Minimal improvement after 4 weeks open chain eccentrics• Post treadmill eccentrics
– Pain at 2 weeks– Pain free running at 4 weeks (8 total rehab weeks)
Return to high speed running at 12 weeks
– Ultrasound analysis: tendon diameter

How to load the tendon?7,10-12,18
• No set standard• Dependent on tendon tolerance (i.e. pain)• Need to have pain onset with eccentric
HEP• Increase load or intensity, but not both at
the same time

Questions/Comments
• Clinical experiences with treating the HS• Try special tests or hamstring exercises• Go on to discuss RCTs on prevention

References1. Ahmad CS, Redler LH, Ciccotti MG, Maffulli N, Longo UG, Bradley J. Evaluation and
Management of Hamstring Injuries. Am J Sports Med 2013; 41: 2933-2947.
2. Cacchio A, Borr F, Severinin G, Foglia A, Mussara F, Taddio N, de Paulis F. Reliability and Validity of Three Pain Provocoation Tests Used for the Diagnosis of Chronic Proximal Hamstring Tendinopathy. Br J Sports Med. 2012;46(12):883-887.
3. Comin J, Malliaras P, Baquie P, Barbour T, Connell D. Return to Competitive Play After Hamstring Injuries Involving Disruption of the Central Tendon. Am J Sports Med 2013 41: 111
4. Cushman D, Rho M. Conservative Treatment of Subacuter Proximal Hamstring Tendinopathy Using Eccentric Exercises Performed with a Treadmill: A Case Report. JOSPT July 2015; 45: 557-562.
5. Emami M, Massoud A, Ghamkhar L. The activity pattern of the lumbo-pelvic muscles during prone hip extension in athletes with and without hamstring strain injury. The International Journal of Sports Physical Therapy 2014; 9 (3): 312-319.
6. Goldman E and Jones D. Interventions for preventing hamstrings injures: a systematic review. Physiotherapy 2011; 97: 91-99.
7. Heiderscheit BC, Sherry MA, Silder A, Chumanov E, Thelen DG. Hamstring Strain Injuries: Recommendations for Diagnosis, Rehabilitation, and Injury Prevention. JOSPT 2014; 40 (2): 67-81.

References• 8. Jayaseelan DJ, Moats N, Ricardo CR. Rehabilitation of Proximal Hamstring
Tendinopathy Utilizing Eccentric Training, Lumbopelvic Stabilization, and Trigger Point Dry Needling: 2 Case Reports. JOSPT 2014; 44 (3): 198-205.
• 9. Kraemer R and Knoblock K. A Soccer-Specific Balance Training Program for Hamstring Muscle and Patellar and Achilles Tendon Injuries: A n Intervention Study in Premier League Female Soccer. Am J Sports Med 2009; 37(7):1384-1393.
• 10. Lorenz D and Reiman M. The Role and Implementation of Eccentric Training in Athletic Rehabilitation: Tendinopathy, Hamstring Strains, and ACL Reconstruction. IJSPT 2011 (1): 27-44.
• 11. Sebelien C, Stiller CH, Maher SF, Qu X. Effects of Implementing Nordic Hamstring Exercises for Semi-professional Soccer Players in Akershus, Norway. Orthopedic Practice 2014; 26 :90-97.
• 12. Schmitt B, Tyler T, McHugh M. Clinical Commentary: Hamstring Injury Rehabilitation and Prevention of Reinjury Using Lengthened State Eccentric Training: A New Concept. IJSPT 2012; 7 (3): 333-341.
• 13. Sherry M, Best T. A Comparison of 2 Rehabilitation Programs in the Treatment of Acute Hamstring Strains. JOSPT March 2004; 34: 116-125.

References• 14. Sherry MA, Johnston TS, Heiderscheit BC. Rehabilitation of Acute Hamstring
Strain Injuries. Clin Sports Med 2015; 34: 263–284. • 15. Silder A, Sherry M, Sanfilippo J, Tuite M, Hetzel S, Heiderschiet. Clinical and
Morphological Changes Following 2 Rehabilitation Programs for Acute Hamstring Strain Injuries: A Randomized Clinical Trial. JOSPT May 2013; 43: 284-299.
• 16. Turner AN, Cree J, Comfort P, Jones L, Chavda S, Bishop C, Reynolds A. Hamstring Strain Prevention in Elite Soccer Players. National Strength and Conditioning Association. 2014; 36 95): 10-20.
• 17. Opar DA, Williams MD, Timmins RG, Hickey J, Duhig SJ, Shield AJ. The effect of previous hamstring strain injuries on the change in eccentric hamstring strength during preseason training in elite Australian Footballers. Am J Sports Med 2014; 43: 377.
• 18. Van der Horst N, Smits D, Petersen J, Goedhart E, and Backx FJ. The Preventative Effects of the Nordic Hamstring Exercise on Hamstring Injuries in Amateur Soccer Players: A Randomized Control Trial. Am J Sports Med 2015; 43: 1316.

Back Up Slides

Prevention: The Nordic Curl11,18
• 2 RCTs – 2014 & 2015

Nordic Curl in Amateur Soccer Players 18
• Nordic curls performed right before cool down
Nordic Curl Control During Intervention
11 25
Post intervention
6 18
Week x/week Duration
1 1 2x5
2 2 2x6
3 2 3X6
4 2 6, 7, 8(3 sets)
5 2 8, 9, 10 (3 sets)
6-13 2 10, 9,8 (3 sets)
• Results:• incidence• injury
severity not affected

Nordic Curl in Semi-Pro Soccer Players11
• After warm-up: HS self stretch, HS partner stretch, then Nordic curls
Week x/week Duration
1 1 2x5
2 2 2x6
3 3 3x6-8
4 3 3x8-12
5 3 3x8-12
• Results: no difference in strength or sprint speed
Nordic Curl Control
Year prior to intervention
11 7
Year of intervention
0 6

Pharmacological Interventions7,14
• NSAIDS– Negative effect on muscle recovery– Acetaminophen is better
• Corticosteroid Injections

How do eccentrics work?8,10
• Eccentric work requires less oxygen• tendon volume and intratendinous
signal– pain – type I collagen synthesis
• Normalizes disorganized tendon structure

Chronic Tendinopathy Case Report8
• Started eccentrics in phase 1 due to chronicity– Leg curl, single leg deadlift, bridge walk outs
• Dry Needling in phase 2• 70 and 69 yo male runners• Symptoms for 7-9 months• Back to running pain free in 8-10 weeks