hai-net icu results and perspectives. carl suetens (ecdc)
TRANSCRIPT
HAI-Net surveillance of HAIs in intensive care units (HAI-Net ICU): results and perspectives
Carl Suetens
Surveillance and Response Support Unit European Centre for Disease Prevention and Control
Healthcare-Associated Infections surveillance Network (HAI-Net)
Since 2000, as the HELICS project and then the IPSE project, both financed by grants from the European Commission (DG SANCO) to Claude Bernard University Lyon I, France
Coordinated by ECDC since July 2008
Coordination Committee (European experts) and contact points in participating countries
Modules:
Surgical site infections (SSIs): 16 countries HAIs in intensive care units: 15 countries Point prevalence survey (PPS): 30 countries HAI in long-term care facilities (LTCFs)
(HALT-2, outsourced), 24 countries C. difficile infections: pilot 14 countries
EU-wide CDI surveillance in 2016
Reports: Annual epidemiological reports 2007-2013;
PPS in acute care hospitals, 2011-2012; SSIs, 2008-2009, 2010-2011;
LTCFs (2010, 2013), ICU (in preparation); PPS interactive database
http://ecdc.europa.eu/en/activities/surveillance/HAI/Pages/default.aspx

HAI-Net ICU report 2008-2012
Number of years of participation, 2008-2012
Liechtenstein
Luxembourg
Malta
Non-visible countries
No participation
1 year
2 yrs
4 yrs
5 yrs
Not included
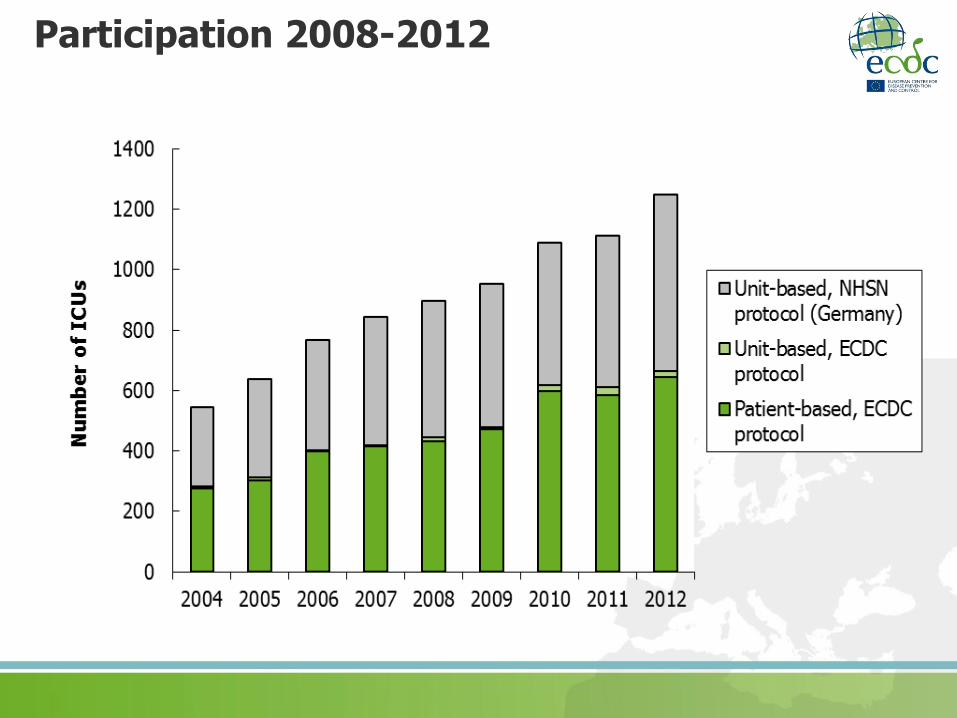
Participation 2008-2012
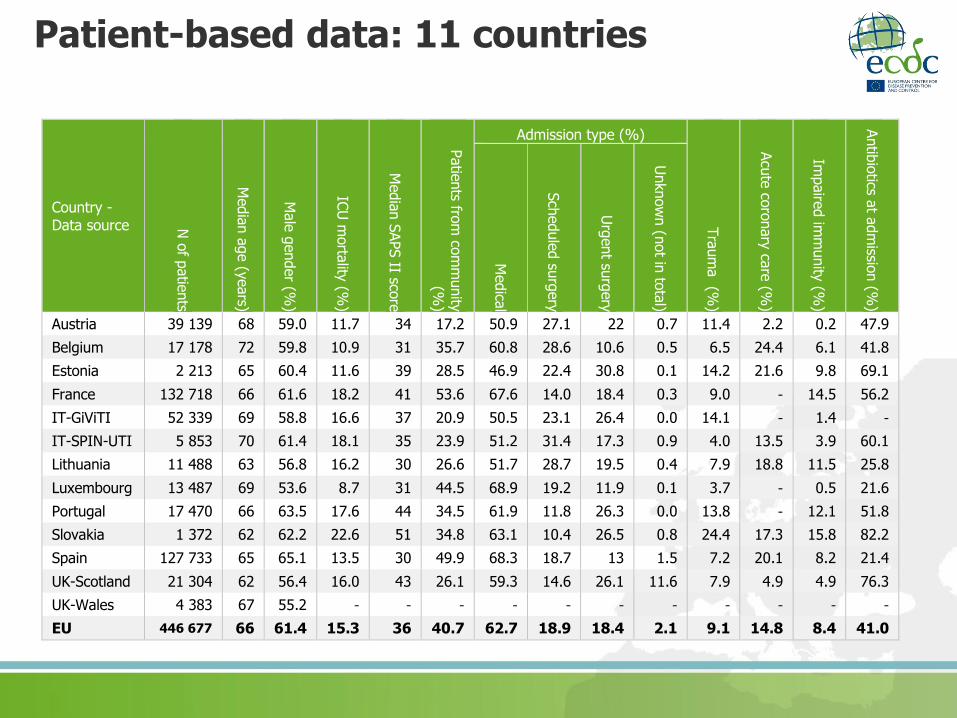
Patient-based data: 11 countries
Country - Data source N
of p
atie
nts
Media
n a
ge (y
ears)
Male
gender (%
)
ICU
morta
lity (%
)
Media
n S
APS II sco
re
Patie
nts fro
m co
mm
unity
(%)
Admission type (%)
Tra
um
a (%
)
Acu
te co
ronary
care
(%)
Impaire
d im
munity
(%)
Antib
iotics a
t adm
ission (%
)
Medica
l
Sch
edule
d su
rgery
Urg
ent su
rgery
Unknow
n (n
ot in
tota
l)
Austria 39 139 68 59.0 11.7 34 17.2 50.9 27.1 22 0.7 11.4 2.2 0.2 47.9
Belgium 17 178 72 59.8 10.9 31 35.7 60.8 28.6 10.6 0.5 6.5 24.4 6.1 41.8
Estonia 2 213 65 60.4 11.6 39 28.5 46.9 22.4 30.8 0.1 14.2 21.6 9.8 69.1
France 132 718 66 61.6 18.2 41 53.6 67.6 14.0 18.4 0.3 9.0 - 14.5 56.2
IT-GiViTI 52 339 69 58.8 16.6 37 20.9 50.5 23.1 26.4 0.0 14.1 - 1.4 -
IT-SPIN-UTI 5 853 70 61.4 18.1 35 23.9 51.2 31.4 17.3 0.9 4.0 13.5 3.9 60.1
Lithuania 11 488 63 56.8 16.2 30 26.6 51.7 28.7 19.5 0.4 7.9 18.8 11.5 25.8
Luxembourg 13 487 69 53.6 8.7 31 44.5 68.9 19.2 11.9 0.1 3.7 - 0.5 21.6
Portugal 17 470 66 63.5 17.6 44 34.5 61.9 11.8 26.3 0.0 13.8 - 12.1 51.8
Slovakia 1 372 62 62.2 22.6 51 34.8 63.1 10.4 26.5 0.8 24.4 17.3 15.8 82.2
Spain 127 733 65 65.1 13.5 30 49.9 68.3 18.7 13 1.5 7.2 20.1 8.2 21.4
UK-Scotland 21 304 62 56.4 16.0 43 26.1 59.3 14.6 26.1 11.6 7.9 4.9 4.9 76.3
UK-Wales 4 383 67 55.2 - - - - - - - - - - -
EU 446 677 66 61.4 15.3 36 40.7 62.7 18.9 18.4 2.1 9.1 14.8 8.4 41.0
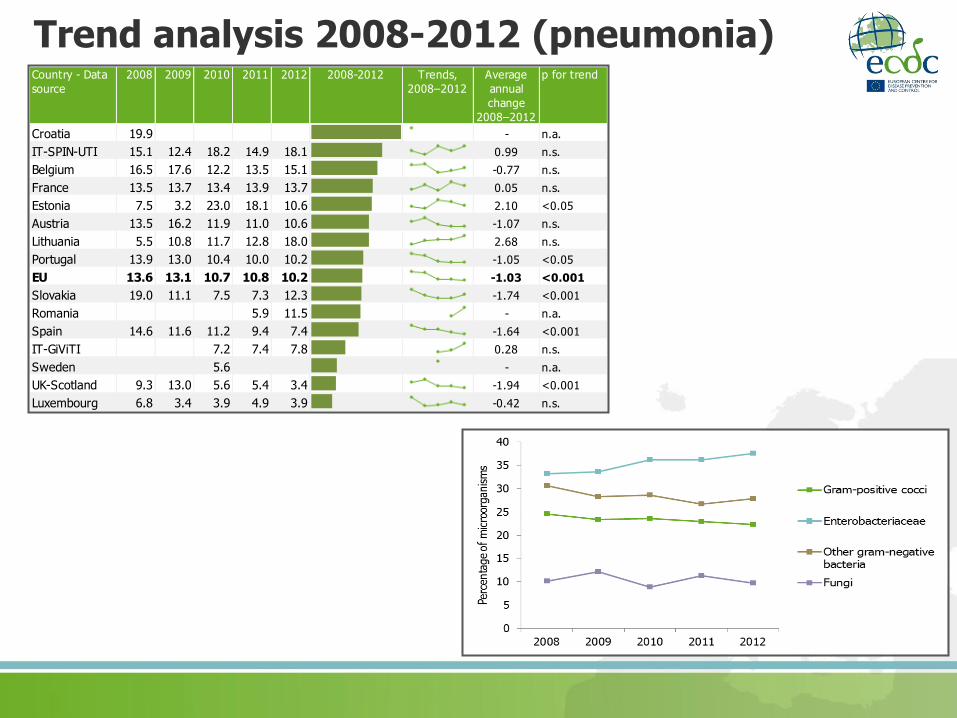
Trend analysis 2008-2012 (pneumonia) Country - Data
source
2008 2009 2010 2011 2012 2008-2012 Trends,
2008–2012
Average
annual
change
2008–2012
p for trend
Croatia 19.9 - n.a.
IT-SPIN-UTI 15.1 12.4 18.2 14.9 18.1 0.99 n.s.
Belgium 16.5 17.6 12.2 13.5 15.1 -0.77 n.s.
France 13.5 13.7 13.4 13.9 13.7 0.05 n.s.
Estonia 7.5 3.2 23.0 18.1 10.6 2.10 <0.05
Austria 13.5 16.2 11.9 11.0 10.6 -1.07 n.s.
Lithuania 5.5 10.8 11.7 12.8 18.0 2.68 n.s.
Portugal 13.9 13.0 10.4 10.0 10.2 -1.05 <0.05
EU 13.6 13.1 10.7 10.8 10.2 -1.03 <0.001
Slovakia 19.0 11.1 7.5 7.3 12.3 -1.74 <0.001
Romania 5.9 11.5 - n.a.
Spain 14.6 11.6 11.2 9.4 7.4 -1.64 <0.001
IT-GiViTI 7.2 7.4 7.8 0.28 n.s.
Sweden 5.6 - n.a.
UK-Scotland 9.3 13.0 5.6 5.4 3.4 -1.94 <0.001
Luxembourg 6.8 3.4 3.9 4.9 3.9 -0.42 n.s.
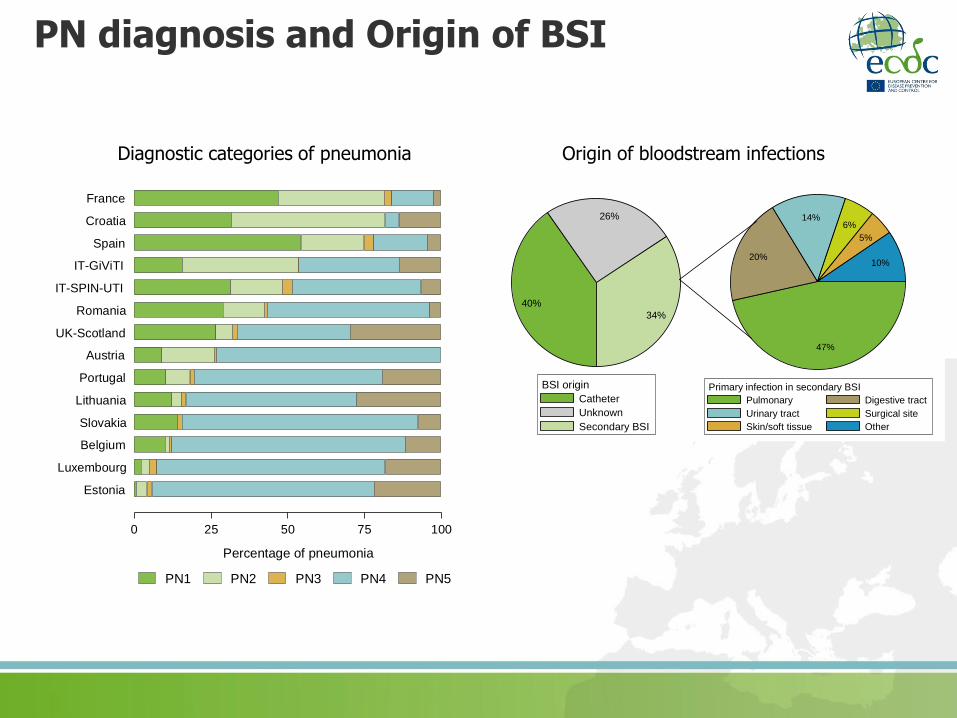
PN diagnosis and Origin of BSI
40%
26%
34%
Catheter
Unknown
Secondary BSI
BSI origin
47%
20%
14%6%
5%
10%
Pulmonary Digestive tract
Urinary tract Surgical site
Skin/soft tissue Other
Primary infection in secondary BSI
Origin of bloodstream infections
0 25 50 75 100
Percentage of pneumonia
Estonia
Luxembourg
Belgium
Slovakia
Lithuania
Portugal
Austria
UK-Scotland
Romania
IT-SPIN-UTI
IT-GiViTI
Spain
Croatia
France
PN1 PN2 PN3 PN4 PN5
Diagnostic categories of pneumonia

Attributable mortality analysis
One approach: matched case cohort using propensity score matching
More statistical approaches in future (multi-state, marginal structural models, cox regression + time-dependent co-variates…)
Pneumonia
No Yes
Number of patients 20 686 20 686
Median age (years) 66 65
Gender (% male) 70.1 71.0
Median propensity score 183 183
Median intubation days before onset* 8 8
Median length of stay (days) before onset* 11 9
Median SAPS II score 47 46
Trauma patient (%) 15.2 16.0
Impaired immunity (%) 13.4 12.5
Admission type:
Medical (%) 65.0 65.2
Scheduled surgery (%) 10.2 10.3
Urgent surgery (%) 24.1 24.0
ICU mortality 29.3 32.8
attributable mortality: 3.5% (95% CI 2.6-4.4%)
Pneumonia
Bloodstream infection
No Yes
Number of patients 12 294 12 294
Median age (years) 66 65
Gender (% male) 67.8 68.3
Median propensity score 158 158
Median CVC days before onset* 12 11
Median intubation days before onset* 10 10.5
Median length of stay (days) before onset* 14 13
Median SAPS II score 45 46
Trauma patient (%) 13.2 13.1
Impaired immunity (%) 13.9 14
Admission type:
Medical (%) 64.2 63.6
Scheduled surgery (%) 10.5 11.1
Urgent surgery (%) 24.3 24.7
ICU mortality 29.5 34.6
Bloodstream infections
attributable mortality: 5.1% (95% CI 4.0-6.2%)

Changes to the ICU protocol
Request of European Commission:
– Structure and process indicators of HAI prevention
– HAI mortality data
Process for identification of prevention indicators:
– Meeting HAI-Net ICU Network, Oct 2013
– Smaller expert meeting, February 2014
– HAI-Net Coordination Committee, May 2014
– Teleconferences HAI-Net ICU expert group
– Consultation of Infection Section of ESICM (Oct 2014)

http://ec.europa.eu/health/patient_safety/healthcare_associated_infections/index_en.htm
Council Recommendation of 9 June 2009 on patient safety, including the prevention and control of healthcare associated infections (2009/C 151/01)

ECDC PPS in acute care hospitals, 2011-2012: structure and process indicators
Infection prevention and control indicators in 2011-2012: single bed rooms, alcohol hand rub consumption
Mapping leads to action: e.g. measures to improve AHR data availability in UK-Scotland
Percentage of beds in single rooms Alcohol hand rub consumption
*Poor data representativeness; Source: ECDC PPS, 2011-2012. Report available from http://www.ecdc.europa.eu/en/publications/Publications/healthcare-associated-infections-antimicrobial-use-PPS.pdf
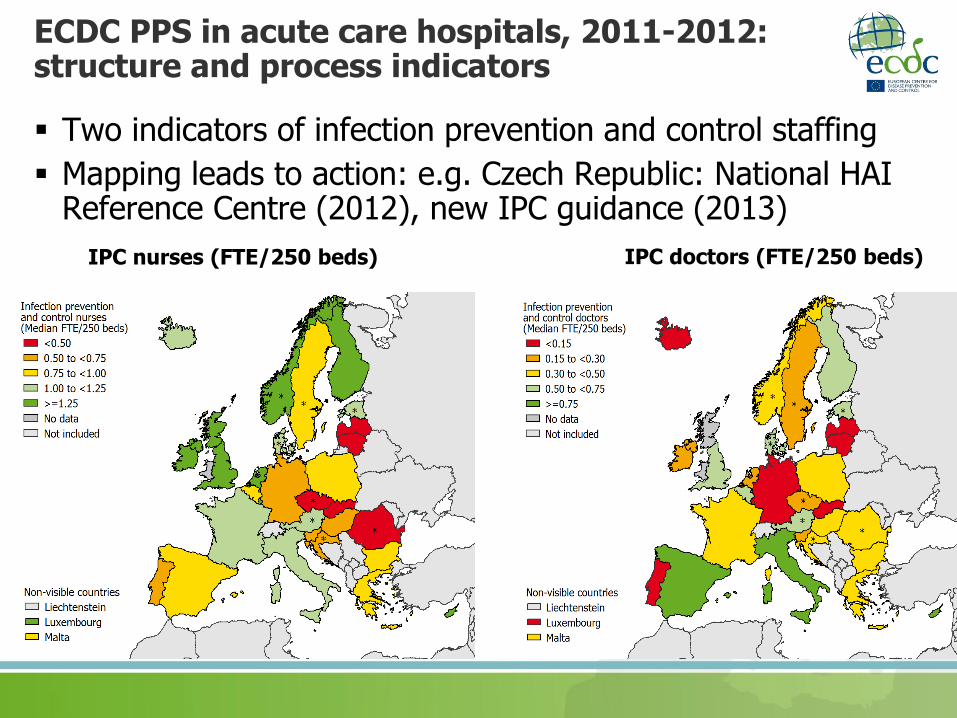
ECDC PPS in acute care hospitals, 2011-2012: structure and process indicators
Two indicators of infection prevention and control staffing
Mapping leads to action: e.g. Czech Republic: National HAI Reference Centre (2012), new IPC guidance (2013)
IPC nurses (FTE/250 beds) IPC doctors (FTE/250 beds)

Infection prevention and control indicators: objectives Increase awareness for HAI/AMR prevention through
surveillance/repeated PPS
Add local value to surveillance by inter-hospital comparison and follow-up of key preventive measures (=> increase participation to surveillance networks?)
Inter-country comparison and follow-up of implementation of key preventive measures in EU/EEA countries
Follow-up of implementation of ECDC guidance and Council Recommendation 2009/C 151/01
At the longer term: linking evolution of prevention indicators with outcome indicators trends

Indicators: criteria
Should measure:
- Capacity/Preparedness
AND
- Behaviour/Practices
Evidence-based
Feasible
Valid & reproducible
Sufficient variability
Allow change over time
Limited number, best selection for EU-level surveillance
Infection Prevention and Control
Surveillance process
Antimicrobial Stewardship
Hospital denominator data

Common indicators for ARHAI surveillance networks
EARS-Net
HAI-Net
Lab001
Lab002
ESAC-Net
Hospital-based
antimicrobial
consumption
PPS
ICU
SSI
CDI
Hosp12
Hosp34
Hosp56
Hosp78
Standardised
hospital
codes
Specific
indicators
Hospital indicators
and denominator data (1 record per hospital and per
surveillande period/ year)
HAI-Net ICU structure and process indicators
1-2 weeks data collection & aggregated reporting per year/surveillance period, Unit based (aggregated), at least 30 opportunities per indicator
Current proposal:
– Hand hygiene: alcohol handrub consumption (L/1000 pt days) in ICU
– ICU staffing: registered nurses and nurse aides
– Antimicrobial stewardship: systematic review of AM after 48-72 hrs
– IAP prevention: cuff pressure control, oral decontamination, patient position
– CR-BSI prevention: CVC maintenance – dressing observation and/or clinical surveillance of insertion site (chart review)
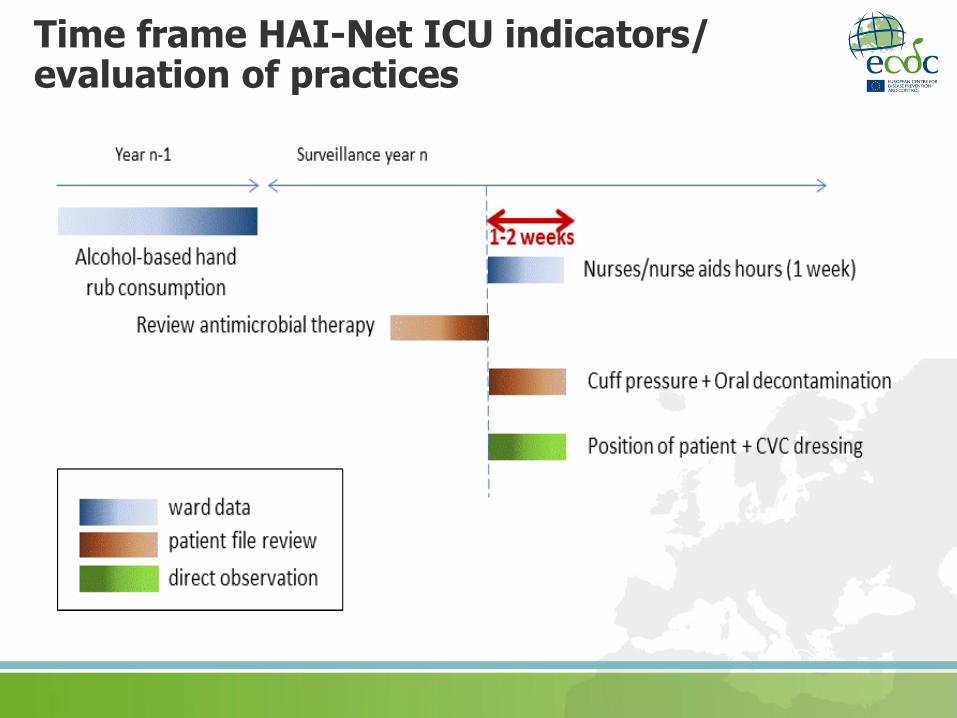
Time frame HAI-Net ICU indicators/ evaluation of practices

Forms: hospital/ICU data 1/2
Hospital data
Hospital Code Year:
Hospital Type: O primary O secondary O tertiary O specialised
ICU characteristics
ICU Id
ICU size Number of beds in the ICU
ICU specialty
Percentage of intubated patients in year (true or estimated %): %
HAI types included in surveillance: O Pneumonia (PN) O Bloodstream Infections (BSI)
O Urinary tract infections (UTI) O Catheter-related infections (CRI1+2+3)
ICU indicators and denominators (one sheet per surveillance period)
Start date
N of
admissions
N of patient-
days
N of
admissions
N of patient-
days
Recommended minimal surveillance period = 3 months, maximum 1 year; add one form for each period
O Mixed O Medical O Surgical O Coronary O Burns O Neurosurgical
O Pediatric O Neonatal O Other O Unknown
Surveillance Period Patients staying >2 days All Patients
European Surveillance of ICU-acquired infections
Hospital / ICU form (standard & light protocol)
Hospital size
(n of beds)
Unique identif ier for each intensive care unit w ithin an hospital
End date
STRUCTURE AND PROCESS INDICATORS
Alcohol hand rub consumption during the previous year: Litres
Number of patient days (all) in the previous year patient days
ICU staffing
Number of hours of nurses present in the ICU in 7 days nurse hours
Number of hours of nurses' aides present in the ICU in 7 days nurse hours
Number of patient days in these 7 days patient days
Practice evaluation: Start date __ / __ / _____ End date __ / __ / _____
N of files /
observations
N
compliance
Intubation: Position of the patient not supine (observation)
CVC: Catheter site dressing is not damp, loose or visibly soiled
(observation)
Antimicrobial stewardship: Review antimicrobial therapy after 48-
72 hours (chart review)
Intubation: Endotracheal cuff pressure controlled and/or corrected
at least twice a day (chart review)
Intubation: Oral decontamination using oral antiseptics at least
twice a day (chart review)

Forms: hospital/ICU data 2/2
STRUCTURE AND PROCESS INDICATORS
Alcohol hand rub consumption during the previous year: Litres
Number of patient days (all) in the previous year patient days
ICU staffing
Number of hours of nurses present in the ICU in 7 days nurse hours
Number of hours of nurses' aides present in the ICU in 7 days nurse hours
Number of patient days in these 7 days patient days
Practice evaluation: Start date __ / __ / _____ End date __ / __ / _____
N of files /
observations
N
compliance
Intubation: Position of the patient not supine (observation)
CVC: Catheter site dressing is not damp, loose or visibly soiled
(observation)
Antimicrobial stewardship: Review antimicrobial therapy after 48-
72 hours (chart review)
Intubation: Endotracheal cuff pressure controlled and/or corrected
at least twice a day (chart review)
Intubation: Oral decontamination using oral antiseptics at least
twice a day (chart review)

HAI-Net ICU other protocol changes: attributable mortality HAI-related mortality, direct measurement of relationship of HAI to
death:
– Measured at HAI data level (Light and Standard protocol)
– In addition to statistical approach for countries with patient-based (standard protocol) data
– Proposal: for each patient with HAI, record outcome:
No death in ICU Death in ICU, HAI definitely contributed to death Death in ICU, HAI possibly contributed to death Death in ICU, no relationship to HAI Death in ICU, relationship to HAI unknown/ not verified
Methodology:
– Algorithm/cause analysis in ICU by clinician(s) and/or ICP?
– Consider: expected death on ICU admission/SAPS II score/McCabe score, other causes of death, active (complication of) HAI at time of death, antimicrobial resistance, appropriateness of treatment

HAI-Net ICU other protocol changes
Removal variables standard protocol (too many missing data):
– date of hospital admission
– coronary care
– previous surgery site
– parenteral nutrition
Change APACHE II in “Other severity score type” (APACHE II, SAPS III, McCabe, MPM …) and “Other severity score value”
Antimicrobial resistance data:
- request to change markers from ‘non-susceptible’ to ‘resistant’ (no change for ICU protocol – S/I/R/U collected)
- colistin (+tigecycline?) for Enterobacteriaceae, remove ESBL (only keep C3G), remove AMC?
- add PDR (pandrug-resistance)? (no PDR – possible PDR – confirmed PDR – Unknown)

Forms: patients/HAIs European Surveillance of ICU-acquired infections
Patient-based risk factor form (standard protocol)
Hospital code Date of admission in hospital: ___ / ___ / _______
ICU code (abbr name) Patient Counter
Patient data
Age in years: ____ yrs Gender: M F UNK Date of admission in ICU: ___ / ___ / _______
Date of ICU discharge ___ / ___ / _______ Outcome at ICU discharge: Alive Dead UNK
Origin of the patient O Ward this/oth hosp O Other ICU O Community O LTCF O Other O UNK
SAPS II score: Other severity score name*:
Other severity score value:
Type of admission: O medical O scheduled surgical O unscheduled surgical O UNK
Trauma: O Yes O No O UNK Impaired immunity: O Yes O No O UNK
Antimicrobial treatment +/- 48 Hrs around admission : O Yes O No O UNK*Other severity score name: APACHE II, APACHE III, APACHE IV, SAPS 3, MPM II, MPM III, McCabe score
Exposure to invasive devices in the ICU
Central vascular catheter in ICU: O Yes O No O Unk
If Yes: Start Date 1 : ___ / ___ / _______ End Date 1: ___ / ___ / _______
Start Date 2 : ___ / ___ / _______ End Date 2: ___ / ___ / _______
Intubation in ICU: O Yes O No O Unk
If Yes: Start Date 1 : ___ / ___ / _______ End Date 1: ___ / ___ / _______
Start Date 2 : ___ / ___ / _______ End Date 2: ___ / ___ / _______
Urinary catheter in ICU: O Yes O No O Unk
If Yes: Start Date 1 : ___ / ___ / _______ End Date 1: ___ / ___ / _______
Start Date 2 : ___ / ___ / _______ End Date 2: ___ / ___ / _______
Patient received antimicrobial(s) during ICU stay O Yes O No O Unkown
Antimicrobial (generic or brand name) or ATC5 Indication
Patient had at least one ICU-acquired infection included in surveillance O Yes O No O Unknown
(if yes, fill out HAI form)
Indication: P: prophylaxis E: empiric treatment M: documented treatment S: SDD (Selective Digestive
Decontamination)
Start Date End Date
Patient Counter
Case definition code
Relevant device in
situ before onset*
Date of onset
BSI: source of BSI***
Micro-organism 1
Micro-organism 2
Micro-organism 3
Patient ICU outcome: O discharged alive O death, HAI definitely contributed to death
O death, HAI possibly contributed to death O death, no relation to HAI O death, relationship to HAI unknown
HAI1: AB1 SIR1 AB2 SIR2 AB3 SIR3 AB4 SIR4
Staphylococcus aureus OXA GLY
Enterococcus spp. AMP GLY
Enterobacteriaceae AMC C3G ESBL CAR
AMC C3G ESBL CAR
P.aeruginosa PIP CAZ CAR COL
Acinetobacter spp. CAR COL SUL
HAI2: AB1 SIR1 AB2 SIR2 AB3 SIR3 AB4 SIR4
Staphylococcus aureus OXA GLY
Enterococcus spp. AMP GLY
Enterobacteriaceae AMC C3G ESBL CAR
AMC C3G ESBL CAR
P.aeruginosa PIP CAZ CAR COL
Acinetobacter spp. CAR COL SUL
HAI3: AB1 SIR1 AB2 SIR2 AB3 SIR3 AB4 SIR4
Staphylococcus aureus OXA GLY
Enterococcus spp. AMP GLY
Enterobacteriaceae AMC C3G ESBL CAR
AMC C3G ESBL CAR
P.aeruginosa PIP CAZ CAR COL
Acinetobacter spp. CAR COL SUL
Bold=minimal resistance data (as in PPS); SIR: S sensitive, I intermediate resistance, R resistant, U unknow n
Antibiotic codes: AMC: amoxicillin/clavulanate, AMP: ampicillin, C3G: cephalosporins of third generation (cefotaxim/
cetriaxone/ceftazidim), CAR: carbapenems (imipenem/meropenem/doripenem), CAZ: ceftazidim, COL: colistin,
GLY: glycopeptides (vancomycin, teicoplanin), OXA: oxacillin, SUL: Sulbactam; PIP: piperacillin/ticarcillin w ith or w ithout
enzyme inhibitor; ESBL: Extended Beta-Lactamase producing, Yes=R, No=S, U=Unknow n
MO-Code
European Surveillance of ICU-acquired infections
HAI and AMR form, standard protocol
MO-Code
MO-Code
*relevant device use (intubation for PN, CVC for BSI, urinary catheter for UTI) in 48 hours before onset of infection (even
intermittent use), 7 days for UTI; ** C-CVC, C-PER, C-ART, S-PUL, S-UTI, S-DIG, S-SSI, S-SST, S-OTH, UNK
MO-code MO-code MO-code
___ / ___ / ______
ICU-acquired infections
O Yes O No
O Unknown
___ / ___ / ______ ___ / ___ / ______
O Yes O No
O Unknown
O Yes O No
O Unknown
Target antimicrobial resistance data in ICU-acquired infections
HAI 1 HAI 2 HAI 3
Perspectives for integration of prevention indicators in EU surveillance
Pilot indicators for prevention of ICU-acquired infections
Pilot: 20 countries, min 1 hospital per country
Discussion at meeting of ECDC ARHAI networks, Stockholm, 11-13 February
Gradual implementation in national surveillance protocols
HelicsWin.Net software + new ICU protocols available 5/5/2015

Website: http://antibiotic.ecdc.europa.eu Facebook: EAAD.EU Twitter: @EAAD_EU (#EAAD)
18 November 2015