guidelines for the prevention of sepsis in patients …
TRANSCRIPT

GUIDELINES FOR THE PREVENTION OF SEPSIS IN PATIENTS WITH ASPLENIA OR FUNCTIONAL HYPOSPLENIA
Date: 19th August 2015 Version number: 3.1 final Author: Dr Sarah Taylor / Dr Susan Laidlaw This paper has been adapted from NHS Highland guidelines (ver 6.0). Review Date: August 2017 If you would like this document in an alternative language or format, please contact Corporate Services on 01595 743069.
Guidelines for the Prevention of Sepsis in Asplenic Patients
NHS SHETLAND DOCUMENT DEVELOPMENT COVERSHEET*
Name of document GUIDELINES FOR THE PREVENTION OF SEPSIS IN PATIENTS WITH ASPLENIA OR FUNCTIONAL HYPOSPLENIA
Registration Reference Number New X Review Author Dr Sarah Taylor / Dr Susan Laidlaw
Executive Lead Dr Sarah Taylor
Proposed groups to present document to: Infection Control Team Consultants Group Control of Infection Committee
DATE VERSION GROUP REASON OUTCOME
14/04/14 1 Consultants Group PO Agreed
01/05/14 1.1 Infection Control Team C/S MR
07/05/14 1.1 Control of Infection Committee C/S MR
6/08/2014 2.0 Control of Infection Committee C/S Agreed
3/09/2015 3.0 Control of Infection Committee FIO
Clarification required on one point but otherwise approved
Examples of reasons for presenting
to the group Examples of outcomes following meeting
• Professional input required re: content (PI) • Significant changes to content required – refer to Executive Lead for guidance (SC)
• Professional opinion on content (PO) • To amend content & re-submit to group (AC&R)
• General comments/suggestions (C/S) • For minor revisions (e.g. format/layout) – no need to re-submit to group (MR)
• For information only (FIO) • Recommend proceeding to next stage (PRO)
Page 2 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients
DATE CHANGES MADE TO DOCUMENT
15.04.14 Addition of reference to Haematology in Aberdeen as source of additional advice for clinicians.
July 2014 Summary table on page 6 completely re-written to reflect updated Green Book guidance which includes addition of meningitis B vaccination to the schedule
August 2015 New national patient information leaflets added in.
August 2015 Vaccination information updated to reflect introduction of Meningitis B and Meningitis ACWY to routine immunisation programme.
October 2015
Clarification re treatment of acute infection on page 10. Checked with Highland as wording ambiguous – they have reworded in new version of document (ver 6.0), and now added to this document.
October 2015
Added a section re Coeliac disease on page 5 as per Highland guidance version 6.0
October 2015 Images of patient information leaflet and Alert Card added
Page 3 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients BACKGROUND
The role of the spleen in protecting against overwhelming sepsis due to encapsulated bacteria has long been established.1 The absence of the spleen results in an increased risk of serious sepsis and associated mortality. The risk of death as a result of overwhelming post splenectomy infection (OPSI) has been calculated to be up to 600 times greater than that in the general population, and the estimated lifetime risk of OPSI is 5%.2 Although the greatest risk is in the first two years a degree of risk will be lifelong.3 There is some perception that the risk only applies to people in whom there is underlying haematological disease, but a review has concluded that OPSI after splenectomy for trauma in adults is indeed a potential risk.4 Analysis of Scottish data 5 indicates that:
• the risk of severe infection or death is highest in the first three years after
splenectomy and then declines significantly; • the risk of a second or third infection is particularly high among those who have a
first severe infection, particularly within six months of the first occurrence; • the greatest risk is amongst those who have had a splenectomy for haematological
malignancy. A review in 20076 suggests that factors associated with high risk of invasive pneumococcal disease include:
• aged less than 16 years or greater than 50 years • inadequate serological response to pneumococcal vaccine • a history of previous invasive disease • splenectomy for underlying haematological malignancy, particularly in the context of
on-going immunosuppression It has been known for several decades that immunisation, antibiotic prophylaxis and good advice can reduce the risk of sepsis. Despite this, there is ample evidence that management of asplenic patients is sub-optimal.7 In addition to patients who have undergone splenectomy, other categories of patients may be functionally hyposplenic; those suffering from sickle cell anaemia, thalassaemia major, essential thrombocythaemia, lymphoproliferative diseases and coeliac syndrome. Chronic graft versus host disease will also result in hyposplenia.
Guidelines were published in 19968 and updated in 20019, 200210 and most recently in 20116. Research indicates that even since their publication best practice preventive measures are not being followed.11
After splenectomy, patients are most at long-term risk of infection from Streptococcus pneumoniae, but other encapsulated organisms such as Haemophilus influenzae and Neisseria meningitidis have also been reported as significant pathogens. There is also a greater risk of infections with Escherichia coli and Pseudomonas aeruginosa; Capnocytophaga canimorsus (formerly DF-2) can cause fulminant sepsis following dog bites; blood-borne protozoal infections such as malaria and babesiosis. Salmonella is also a common pathogen in sickle cell disease.
Asplenia may be a congenital condition, or splenectomy can be performed electively or as an emergency procedure. Only emergency splenectomies are performed in Shetland, elective procedures would be done (usually) in Aberdeen.
Page 4 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients Recommended immunisations 1. Pneumococcal. Streptococcus pneumoniae is a bacterial pathogen that affects
children and adults world-wide. The organism colonises the upper respiratory tract, but severe infection can result from dissemination of the bacteria into the bloodstream and the central nervous system. Asplenic individuals are at the highest risk from pneumococcal infection due to reduced clearance of encapsulated bacteria from the bloodstream. Children in this group are at particular risk of fulminant pnemococcal sepsis and subsequent high mortality. Where possible, the vaccine should be given, together with advice about the increased risk of pneumococcal infection, four to six weeks (but at least two weeks) before splenectomy or the initiation of chemotherapy or other immunosuppressive treatment. In the case of splenectomy following trauma there is evidence that better functional antibody responses seems to occur if vaccination is delayed for 14 days after surgery. 12
Revaccination: Antibody levels are likely to decline rapidly in individuals who have asplenia or splenic dysfunction and therefore revaccination with 23-valent PPV is recommended every five years. Testing of antibodies prior to vaccination is not required.13
2. Hib Asplenic/hyposplenic children and adults may be at increased risk of invasive
disease caused by Haemophilus influenzae type b. 3. Meningococcal Disease. Asplenic/hyposplenic children and adults may be at increased
risk of invasive disease caused by meningococci, and require appropriate immunization against Men A,B,C, W.Y. Such individuals, irrespective of age or interval from splenectomy, may have a sub-optimal response to the vaccines. Meningitis C and Meningitis B are both now routinely included as part of the childhood immunisation programme (Men B since September 2015) . Meningitis ACWY was also introduced in August 2015 as part of the teenage booster, but is not yet given routinely to babies.
Re-inforcing doses:
• Meningococcal ACWY conjugate vaccine.: The need for, and the timing of, a booster dose of Men ACWY conjugate vaccine in at-risk individuals has not yet been determined.
• Meningococcal ACWY polysaccharide vaccine: MenACWY quadrivalent conjugate vaccine is preferred to the polysaccharide vaccine in all instances. Those who had received polysaccharide vaccines in the past should be vaccinated with conjugate vaccine as above.
• Meningococcal B vaccine.: There are no data to recommend a need for or timing of additional MenB doses in these risk groups
4. Influenza. In asplenic/hyposplenic patients, influenza vaccination is associated with a
54% reduced risk of death compared to unimmunised asplenic persons14. Annual vaccination against influenza is recommended, preferably in September. Asplenic/hyposplenic individuals are not thought to be at more risk of catching influenza but vaccination may reduce the risk of secondary bacterial infection.
In practice it is difficult to know whether some individuals (e.g. those with coeliac syndrome) are hyposplenic, as there is no readily available diagnostic test, and to some extent it therefore depends on clinical judgement. In the absence of evidence of hyposplenia, only influenza and pneumococcal vaccines are recommended for those with coeliac syndrome.
Page 5 of 16
Guidelines for the Prevention of Sepsis in Asplenic Patients
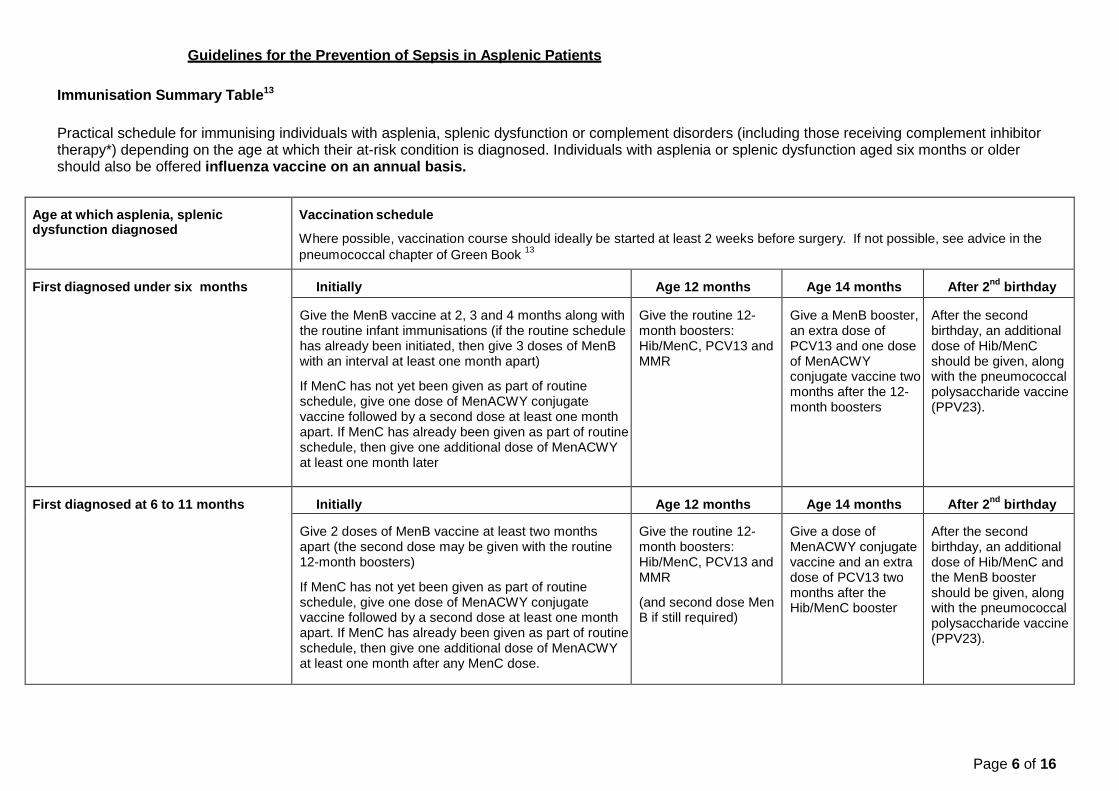
Immunisation Summary Table13
Practical schedule for immunising individuals with asplenia, splenic dysfunction or complement disorders (including those receiving complement inhibitor therapy*) depending on the age at which their at-risk condition is diagnosed. Individuals with asplenia or splenic dysfunction aged six months or older should also be offered influenza vaccine on an annual basis.
Age at which asplenia, splenic dysfunction diagnosed
Vaccination schedule
Where possible, vaccination course should ideally be started at least 2 weeks before surgery. If not possible, see advice in the pneumococcal chapter of Green Book 13
First diagnosed under six months
Initially Age 12 months Age 14 months After 2nd birthday
Give the MenB vaccine at 2, 3 and 4 months along with the routine infant immunisations (if the routine schedule has already been initiated, then give 3 doses of MenB with an interval at least one month apart)
If MenC has not yet been given as part of routine schedule, give one dose of MenACWY conjugate vaccine followed by a second dose at least one month apart. If MenC has already been given as part of routine schedule, then give one additional dose of MenACWY at least one month later
Give the routine 12-month boosters: Hib/MenC, PCV13 and MMR
Give a MenB booster, an extra dose of PCV13 and one dose of MenACWY conjugate vaccine two months after the 12-month boosters
After the second birthday, an additional dose of Hib/MenC should be given, along with the pneumococcal polysaccharide vaccine (PPV23).
First diagnosed at 6 to 11 months Initially Age 12 months Age 14 months After 2nd birthday
Give 2 doses of MenB vaccine at least two months apart (the second dose may be given with the routine 12-month boosters)
If MenC has not yet been given as part of routine schedule, give one dose of MenACWY conjugate vaccine followed by a second dose at least one month apart. If MenC has already been given as part of routine schedule, then give one additional dose of MenACWY at least one month after any MenC dose.
Give the routine 12-month boosters: Hib/MenC, PCV13 and MMR
(and second dose Men B if still required)
Give a dose of MenACWY conjugate vaccine and an extra dose of PCV13 two months after the Hib/MenC booster
After the second birthday, an additional dose of Hib/MenC and the MenB booster should be given, along with the pneumococcal polysaccharide vaccine (PPV23).
Page 6 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients
First diagnosed at 12-23 months Initially 2 months after 12 month booster
After 2nd Birthday 12-23 months after primary MenB course
If not yet administered, give the routine 12-month boosters: Hib/ MenC, PCV13 and MMR
Give 2 doses of MenB vaccine at least two months apart (either of these doses can be given at the same time as the other vaccine visits)
PCV13 two months after the Hib/MenC and PCV13 boosters
After the second birthday, an additional dose of Hib/MenC should be given, along with the pneumococcal polysaccharide vaccine (PPV23)
This age group should also receive an additional dose of MenB vaccine with an interval of 12 to 23 months after the primary course
First diagnosed from 2 years onwards Initially 2 months later
Ensure that the child has been immunised according to national schedule, including the 12-month boosters
Give an additional dose of Hib/MenC and the first dose of MenB vaccine, along with the pneumococcal polysaccharide vaccine (PPV23)
Give a dose of MenACWY conjugate vaccine and the second dose of MenB two months after the Hib/MenC booster*.
PCV= pneumococcal conjugate vaccine PPV- pneumococcal polysaccharide vaccine
* In adolescents (from 11 years of age) and adults, this interval can be reduced to one month
Ideally vaccinations should be given four to six weeks before elective splenectomy or initiation of chemotherapy and/or radiotherapy. Where this is not possible they can be given up to two weeks before or at least two weeks post-splenectomy
Page 7 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients
Antibiotic prophylaxis
The 1996 Guidelines8 recommended that prophylactic antibiotics should be offered in all cases. There are no data to support or refute the previously published recommendations for antibiotic prophylaxis and treatment of infection in asplenic individuals10. However, it is recognised that compliance may be a problem, (and there has also been more recent discussion concerning the increase in penicillin resistance of pneumococci). Overall pneumococcal resistance to penicillins remains low in the UK10. Though not common in the UK, rates of up to 43% of isolates with some degree of resistance have been reported in Spain16 and travel will bring about increased exposure to resistant strains. The reluctance of some people to take antibiotics on a lifelong basis must also be taken into consideration. Given these factors, people in the following groups should be strongly recommended to receive prophylaxis:
• All people in the first three years after splenectomy5 • All children up to the age of 16 and those over 50 years6 • Individuals in whom there is underlying impaired immune function, (malignancy or
haematological condition) • Individuals who have suffered one severe infection
Regardless of whether prophylaxis is used, patient education is of paramount importance regarding:
• The fact that immunisation and antibiotic prophylaxis does not guarantee
protection against invasive disease. • The need for rapid medical assessment of suspected infections • The requirement to keep a course of antibiotics at home in order to commence
treatment prior to medical assessment when this is delayed.
Recommended doses for antibiotic prophylaxis:20,21
PENICILLIN (1st choice in adults) (phenoxymethylpenicillin): Adult and child over 5 years Child aged 1 to 5 years Child under 1
250mg twice daily 125mg twice daily 62.5mg twice daily
ERYTHROMYCIN: (2nd choice – for use in those with penicillin allergy) Adult and child over 8 years Child aged 2-8 Child 1 month to 2 years
500mg twice daily 250mg twice daily 125mg twice daily
AMOXICILLIN: (Preferred choice in children17) Adult and child over 12 year Child aged 5-12 Child 1 month to 5
500mg twice daily 250mg twice daily 125mg twice daily
Page 8 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients Antibiotic Treatment
Asplenic individuals should receive a supply of stand by antibiotic whether or not they receive prophylactic antibiotics17,18,19, with clear instructions on when to take. Recommended courses for adults include amoxicillin or levofloxacin for those with penicillin allergy.
Travel
Patients should be made aware of the need to seek travel advice early, even for travel in Europe and the potential risks of overseas travel particularly with regard to malaria and unusual infection such as those from animal bites10. Those not taking regular antibiotic prophylaxis should be advised to do so on holiday. Asplenics can have live vaccines unless there is an underlying immunosuppressive disorder.
1. Malaria. All asplenic patients should be made aware of the increased risk of severe
falciparum malaria, and the requirement for antimalarial prophylaxis cannot be overemphasised. Travel to areas where malaria is endemic should be discouraged. Depending on sensitivities in the area of intended travel, doxycycline may offer a combination of antibiotic and antimalarial prophylaxis17.
2. Tick bites. Babesiosis is a rare potentially severe tick-borne disease caused by infection with
a protozoan parasite. Most infections are asymptomatic, though the clinical syndrome can include fever, chills, myalgia, fatigue and jaundice secondary to haemolytic anaemia that may last from a few days to several months. Geographic distribution of the species of ticks that carry the disease is worldwide. Asplenic patients should be educated about the need for protective clothing when walking in areas of forestry or long grass.
3. Meningococcal disease. There is an increased risk of serogroup A, W135 or Y disease in
some countries. Ensure that individuals have been immunised with MenACWY conjugate vaccine as per summary table page 4.
Animal Bites Capnocytophaga canimorsus can cause febrile illness in patients with impaired immune systems who have been licked, bitten or scratched by dogs or cats. Co-amoxiclav, the antibiotic of choice for these infections, should be given prophylactically to high risk individuals who are bitten by a dog or cat. Antivirals for treating influenza Guidance on the use of zanamivir, oseltamivir and amantadine for the treatment of influenza produced by the National Institute for Clinical Excellence (NICE) and endorsed by Health Improvement Scotland should be followed15. This advises that when there is evidence that influenza is circulating in the community at levels above the baseline, antiviral medication for the treatment of influenza in the community may be prescribed for those at risk, provided that treatment can be started within 48 hours of the onset of symptoms. The Scottish Government Health Department issues advice when prescribing of antivirals in general practice becomes appropriate.
Page 9 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients
Treatment of acute infection
General Practitioners attending a known asplenic patient with clinically significant infection should (provided there is no history of anaphylaxis to penicillin) give an immediate dose of intramuscular or intravenous ceftriaxone before transfer to hospital.
Age Dosage Dilution & administration
Children under 50kg 80mg/kg Dissolve each 1g vial in 3.5mLof 1% lidocaine hydrochloride, giving a total of 4mL.
Administer intra-muscularly.
IM injections of more than 1g should be divided between different sites
Adults and children over 50kg
2g
If ceftriaxone is not available, give benzylpenicillin as below:
Age
Dosage
Dilute with water or sodium chloride 0.9%
IM IV
Infant under 1 year 300mg 1mL 2mL
Child 1 to 9 years 600mg 2mL 4mL
Child 10 years and over and adult 1200mg 4mL 8mL
Intravenous administration should be at a rate of 300mg per minute maximum. So for example, 1200mg, reconstitute with 8mL and give over 4 minutes.
If there is a history of anaphylaxis to penicillin, then chloramphenicol may be used.
Page 10 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients General – Roles & Responsibilities
This guidance is provided to assist general practices and hospital consultants in providing appropriate treatment and prophylaxis to their patients who have asplenia or functional hyposplenia. Additional advice about the management of individual patients can also be obtained from the Haematology Dept in NHS Grampian. As historically management of patients in these categories has been found to be sub-optimal7 the Health Protection Team have agreed to assist General Practitioners by notifying them of patients potentially in this category, obtaining data by the following means:
• Patients undergoing elective or emergency splenectomy - Clinicians are requested to
ensure that the In-patient Report (Appendix 1) is completed and forwarded to the Health Protection Team.
• The Health Protection Team also actively seeks to identify relevant patients using data
supplied by the Pathology Department and SMR data.
All patients identified as described above will be sent a leaflet, Information about splenectomy for patients (Appendix 2) which includes an alert card (Appendix 3) to be carried in a purse/wallet.
Some patients may additionally wish to purchase a MedicAlert bracelet and details are available at www.medicalert.org.uk , or by telephoning 0800 581420. Patients may also be encouraged to obtain further information on splenectomy: http://www.patient.co.uk/health/Splenectomy-Ongoing-Prevention-of-Infection.htm
References
1. Hazelwood M, Kumararathe DS (1992) The Spleen? Who needs it anyway? Clin Exp Immunol 89: 327-9
2. Lynch AM, Kapila R. (1996) Overwhelming postsplenectomy infection. Infect Dis Clin North
Am; 10:693-707 3. Deodhar HA, Marshall RJ, Barnes JN (1993) Increased risk of sepsis after splenectomy.
BMJ 307:1408-9 4. Zarrabi HA, Rosner F Serious Infections in Adults
5. Kyaw MH, Holmes EM, Toolis F et al (2006) Evaluation of Severe Infection and Survival After
Splenectomy The American Journal of Medicine 119, 276.e1-276.e7 6. Davies JM, Lewis MPN et al (2011) Review of guidelines for the prevention and treatment
of infection in patients with an absent or dysfunctional spleen: Prepared on behalf of the British Committee for Standards in Haematology by a Working Party of the Haemato-Oncology Task Force. British Journal of Haematology 155:308-317
7. Cummins A, Millership S, (2001) Local review of the provision of prophylaxis and advice to
patients without functioning spleens. Communicable Disease and Public Health 4:2 144-5 8. Working Party of the British Committee for Standards in Haematology Clinical
Haematology Taskforce (1996) Guidelines for the prevention and treatment of infection in patients with an absent or dysfunctional spleen. BMJ 312:430-434
9. Davies JM (2001) The prevention and treatment of infection in patients with an absent or
dysfunctioning spleen. British Committee for Standards in Haematology Guideline up- date.
Page 11 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients (on-line) Available: www.bmj.com/cgi/eletters/312/7028/430 (19.11.01)
10. Davies JM, Barnes R and Milligan D (2002) Update of Guidelines for the prevention and
treatment of infection in patients with and absent or dysfunctional spleen. Clinical Medicine Vol 2 No 5 Sept/Oct 2002.
11. Waghorn DJ (2001) Overwhelming infection in asplenic patients: current best practice
preventive measures are not being followed. J Clin Pathol 54:214-218 12. Shatz DV, Schinsky MF, Pais LB, Romero-Steiner S, Kirton OC, Carlone GM. (1998)
Immune responses of splenectomised trauma patients to the 23-valent pneumococcal polysaccharide vaccine at 1 versus 7 versus 14 days after splenectomy. Journal of Trauma-Injury Infection and Critical Care, 44:5, 760-5.
13. Department of Health (2006) Immunisation against Infectious Disease (The “Green Book”)
Available at: www.dh.gov.uk/greenbook 14. Langley J et al (2010) Pneumococcal and influenza immunization in asplenic persons: a
retrospective population-based cohort study 1990-2002. BMC Infectious Diseases 2010, 10:219.
15. NICE (Multiple) Technology Appraisal Guidance No 168 - Amantadine, oseltamivir and
zanamivir for the treatment of influenza (review of NICE technology appraisal guidance No. 58) Available: http://www.healthcareimprovementscotland.org/default.aspx?page=12891
16. Garcia-Leoni ME, Cercenado E, Rockno P, Bernaldo de Quiros JCL, Martinez- Hernandez
D, Bouza E. (1992) Susceptibility of Streptococcus pneumoniae to penicillin: a prospective microbiological and clinical study. Clin Infect Dis 14:427-35
17. Davidson R.N. and Wall R.A. (2001) Prevention and management of infections in patients
without a spleen. Clinical Microbiology and Infection, Volume 7 Number 12. 18. Dorset Healthcare NHS Foundation Trust, Summary of Guidelines For The Prevention of
Infection In Patients With an Absent or Dysfunctional Spleen. Ref CP-031-05 19. Spelman D., Buttery J. and Daley A et al. (2008) Guidelines for the Prevention of Sepsis in
Asplenic and Hyposplenic Patients. Internal Medicine Journal 38 (2008) 349-356. 20. British Medical Association & Royal Pharmaceutical Society of Great Britain British National
Formulary Available at: www.bnf.org
21. British Medical Association, Royal Pharmaceutical Society of Great Britain, Royal College of Paediatrics and Child Health, Neonatal and Paediatric Pharmacists Group British National Formulary for Children Available at: www.bnfc.org
Page 12 of 16
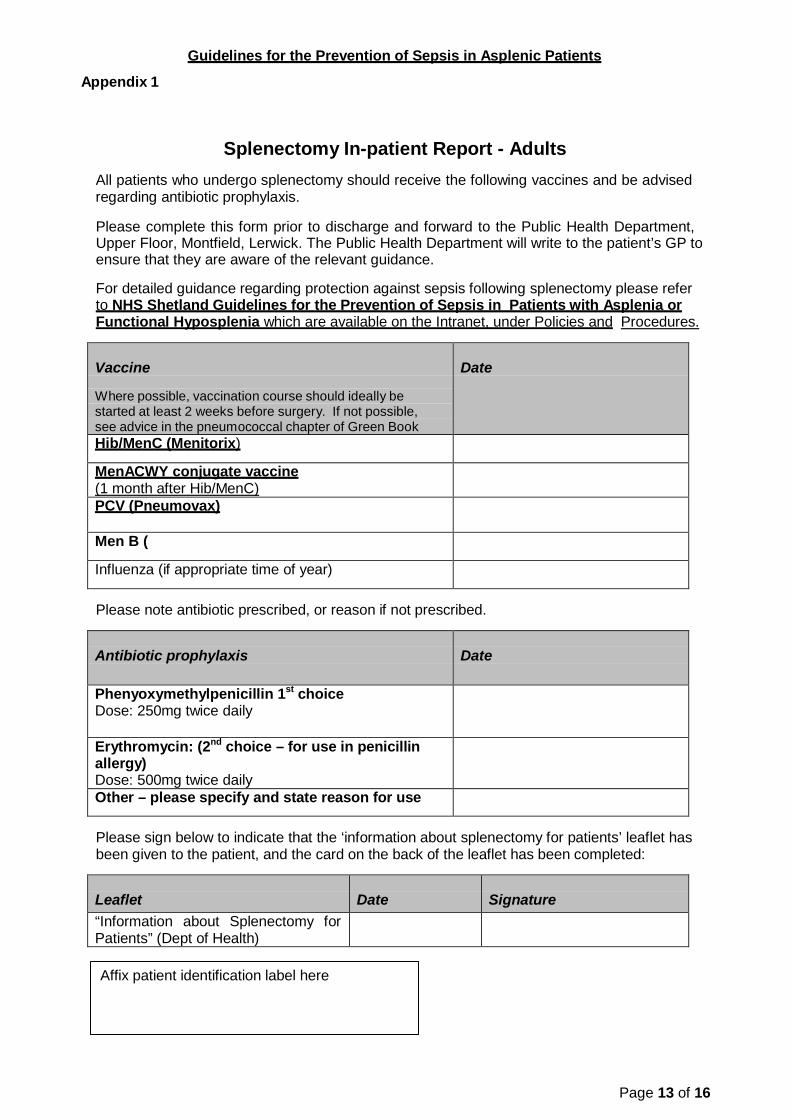
Guidelines for the Prevention of Sepsis in Asplenic Patients Appendix 1
Splenectomy In-patient Report - Adults
All patients who undergo splenectomy should receive the following vaccines and be advised regarding antibiotic prophylaxis.
Please complete this form prior to discharge and forward to the Public Health Department, Upper Floor, Montfield, Lerwick. The Public Health Department will write to the patient’s GP to ensure that they are aware of the relevant guidance.
For detailed guidance regarding protection against sepsis following splenectomy please refer to NHS Shetland Guidelines for the Prevention of Sepsis in Patients with Asplenia or Functional Hyposplenia which are available on the Intranet, under Policies and Procedures.
Vaccine
Where possible, vaccination course should ideally be started at least 2 weeks before surgery. If not possible, see advice in the pneumococcal chapter of Green Book
Date
Hib/MenC (Menitorix)
MenACWY conjugate vaccine (1 month after Hib/MenC)
PCV (Pneumovax)
Men B (
Influenza (if appropriate time of year)
Please note antibiotic prescribed, or reason if not prescribed.
Antibiotic prophylaxis
Date
Phenyoxymethylpenicillin 1st choice Dose: 250mg twice daily
Erythromycin: (2nd choice – for use in penicillin allergy) Dose: 500mg twice daily
Other – please specify and state reason for use
Please sign below to indicate that the ‘information about splenectomy for patients’ leaflet has been given to the patient, and the card on the back of the leaflet has been completed:
Leaflet
Date
Signature
“Information about Splenectomy for Patients” (Dept of Health)
Affix patient identification label here
Page 13 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients
Appendix 2 –Patient Information Leaflet
Page 14 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients
Appendix 2 –Patient Information Leaflet
Page 15 of 16

Guidelines for the Prevention of Sepsis in Asplenic Patients Appendix 3 Alert Card
Page 16 of 16