gsha convention, 2015, athens, ga - … 2015 convention; j. coyle, phd 01/09/2015 (c) james l coyle...
TRANSCRIPT

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 1
What’s wrong with my patient?Sepsis, Congestive heart failure, esophageal
function and disorders
James L. Coyle, Ph.D., CCC‐SLP, BCS‐SUniversity of Pittsburgh
GSHA Convention, 2015, Athens, GA
Disclosures
• I have a job and they give me a salary• University of Pittsburgh
• I see patients 2‐3 times per week• So I am biased toward their health
• NIH funds 25% of my time on an RO‐1
• I give several conferences lectures annually• Honorarium
• No products, no conflicts of interest
Patients with dysphagia
• Pulmonary diseases
• Neurological causes
• Digestive conditions• Severe illness and its effects on other systems
• CHF, Esophageal function/disorders, sepsis

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 2
Congestive Heart Failure
CHF
5© Connexions
Public domain
©Creative Commons license
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 3
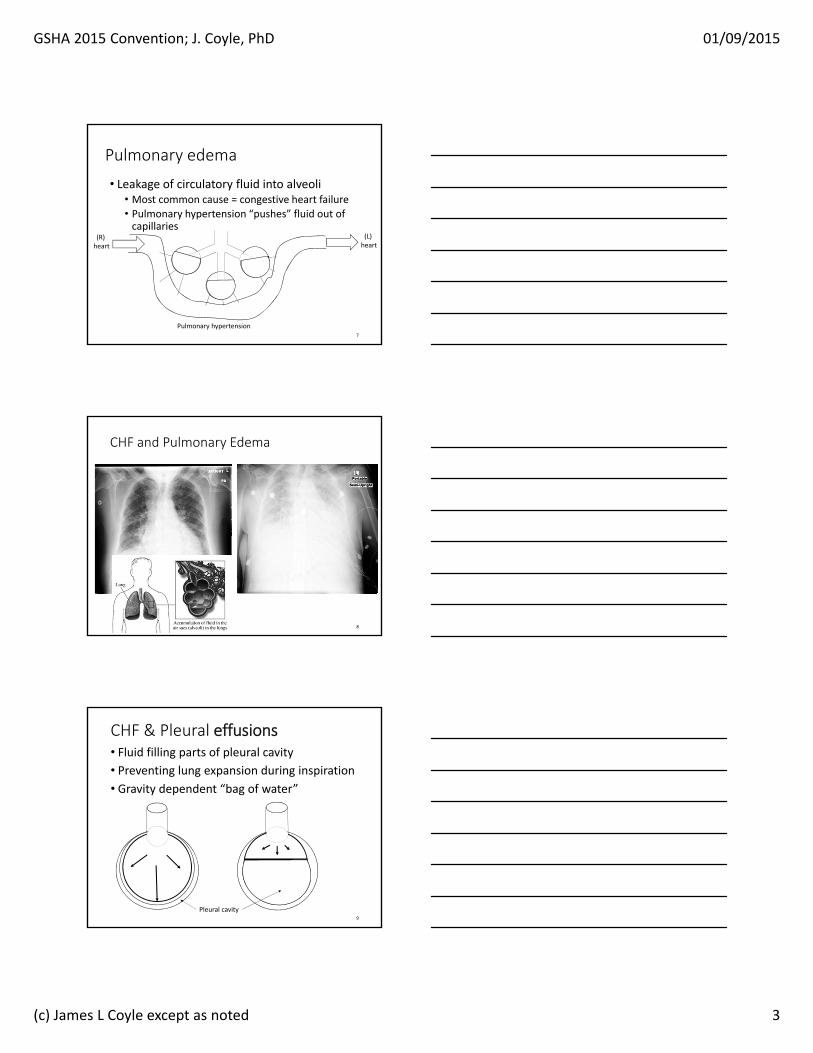
Pulmonary edema
• Leakage of circulatory fluid into alveoli• Most common cause = congestive heart failure• Pulmonary hypertension “pushes” fluid out of capillaries
Pulmonary hypertension7
(R) heart
(L) heart
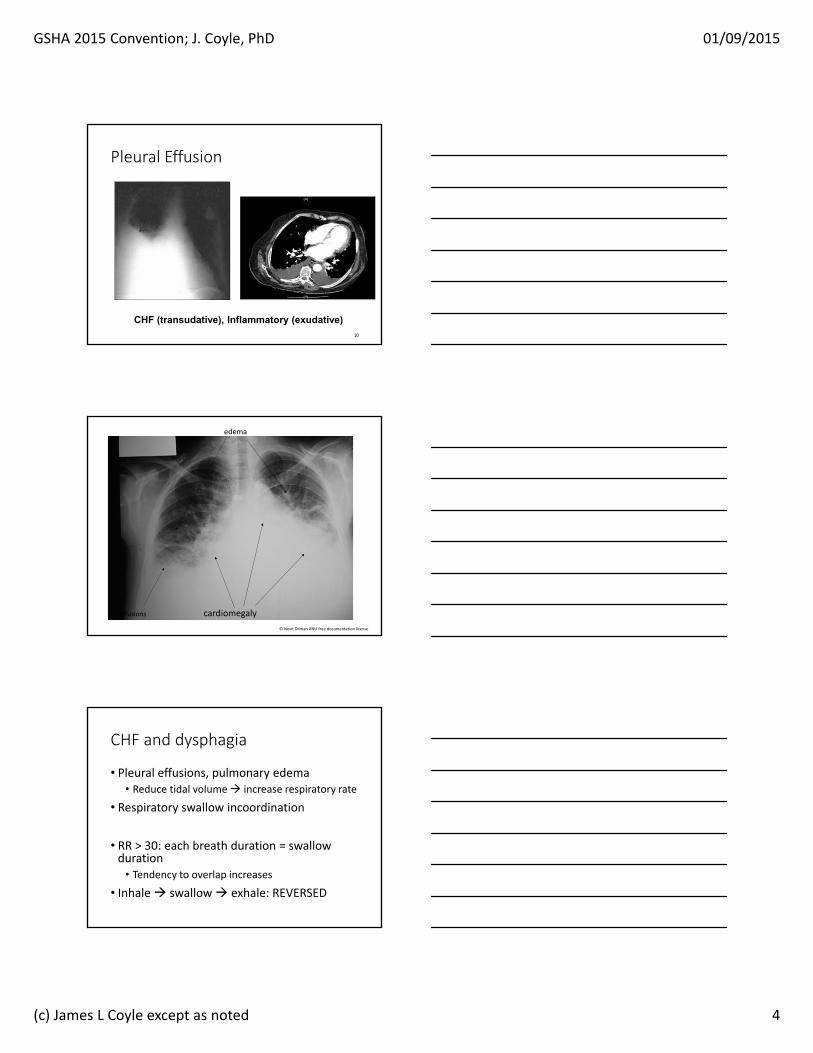
CHF and Pulmonary Edema
8
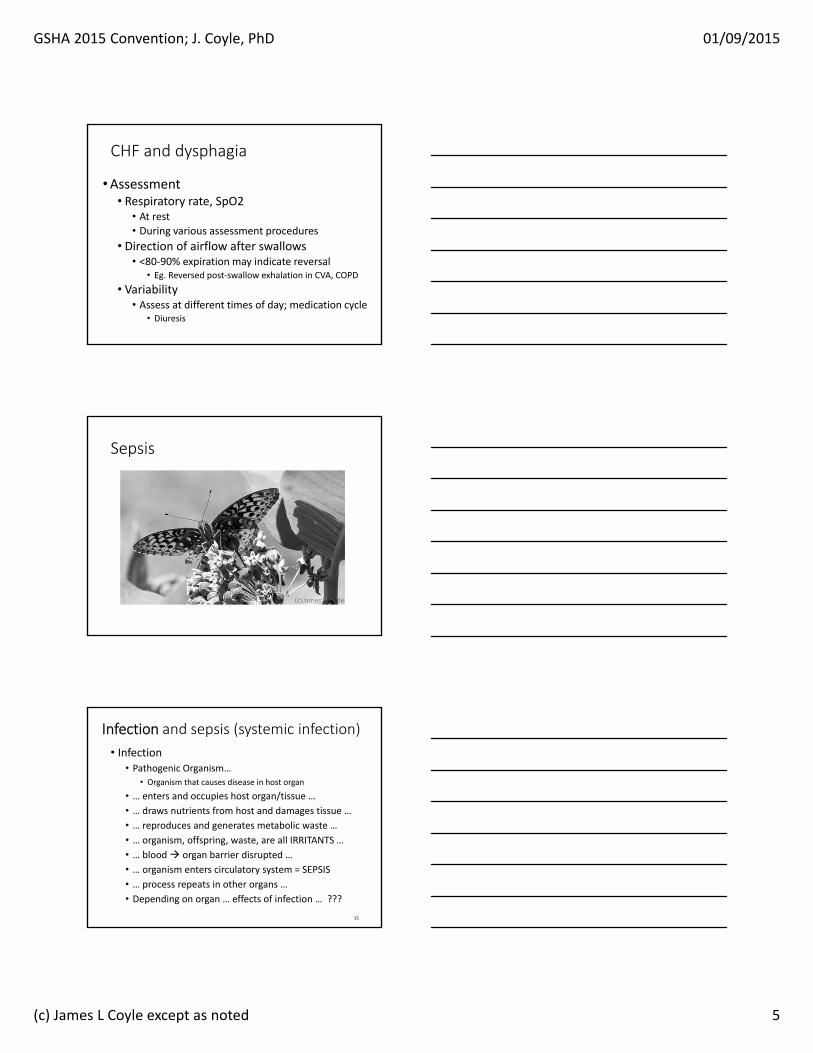
CHF & Pleural effusions• Fluid filling parts of pleural cavity• Preventing lung expansion during inspiration
• Gravity dependent “bag of water”
Pleural cavity9
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 4
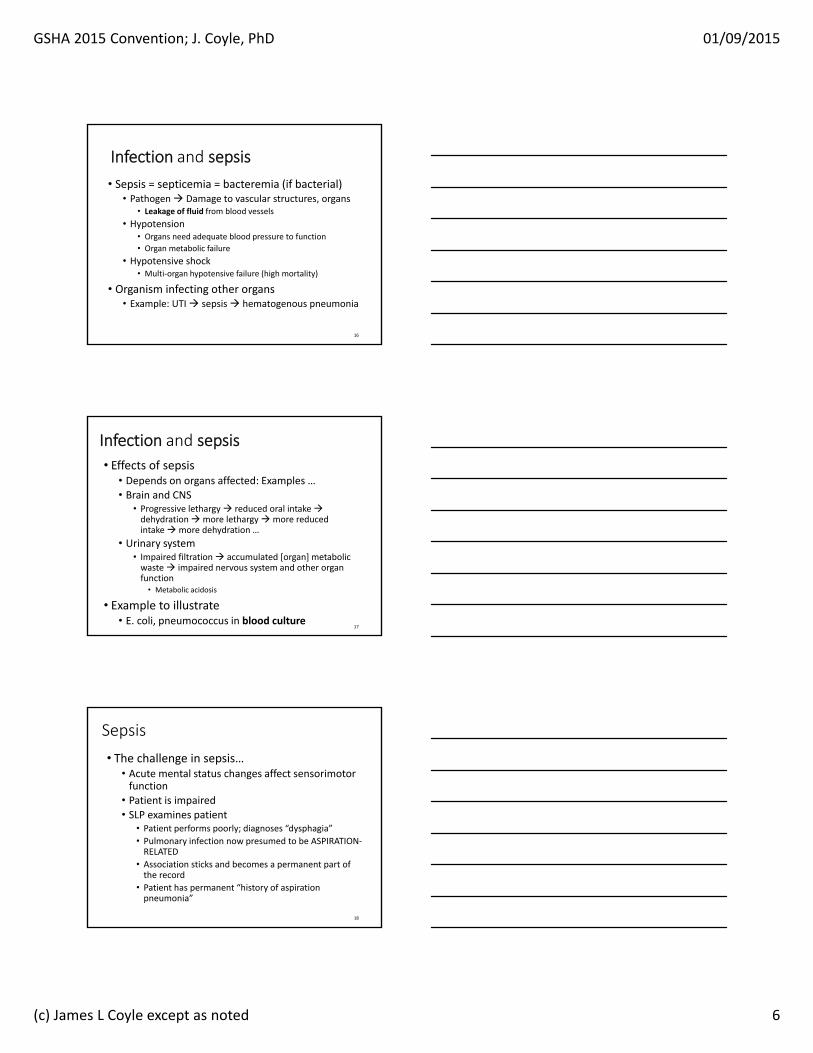
CHF (transudative), Inflammatory (exudative)10
Pleural Effusion
© Nevit Dilman GNU free documentation license
effusions cardiomegaly
edema
CHF and dysphagia
• Pleural effusions, pulmonary edema• Reduce tidal volume increase respiratory rate
• Respiratory swallow incoordination
• RR > 30: each breath duration = swallow duration
• Tendency to overlap increases
• Inhale swallow exhale: REVERSED
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 5
CHF and dysphagia
•Assessment• Respiratory rate, SpO2
• At rest• During various assessment procedures
• Direction of airflow after swallows• <80‐90% expiration may indicate reversal
• Eg. Reversed post‐swallow exhalation in CVA, COPD
• Variability• Assess at different times of day; medication cycle
• Diuresis
Sepsis
Infection and sepsis (systemic infection)
• Infection• Pathogenic Organism…
• Organism that causes disease in host organ
• … enters and occupies host organ/tissue …• … draws nutrients from host and damages tissue …
• … reproduces and generates metabolic waste …
• … organism, offspring, waste, are all IRRITANTS …
• … blood organ barrier disrupted …
• … organism enters circulatory system = SEPSIS
• … process repeats in other organs …• Depending on organ … effects of infection … ???
15
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 6
Infection and sepsis
• Sepsis = septicemia = bacteremia (if bacterial)• Pathogen Damage to vascular structures, organs
• Leakage of fluid from blood vessels
• Hypotension • Organs need adequate blood pressure to function
• Organ metabolic failure
• Hypotensive shock• Multi‐organ hypotensive failure (high mortality)
• Organism infecting other organs• Example: UTI sepsis hematogenous pneumonia
16
Infection and sepsis
• Effects of sepsis• Depends on organs affected: Examples …• Brain and CNS
• Progressive lethargy reduced oral intake dehydration more lethargy more reduced intake more dehydration …
• Urinary system• Impaired filtration accumulated [organ] metabolic waste impaired nervous system and other organ function
• Metabolic acidosis
• Example to illustrate• E. coli, pneumococcus in blood culture
17
Sepsis
• The challenge in sepsis…• Acute mental status changes affect sensorimotor function
• Patient is impaired
• SLP examines patient• Patient performs poorly; diagnoses “dysphagia”
• Pulmonary infection now presumed to be ASPIRATION‐RELATED
• Association sticks and becomes a permanent part of the record
• Patient has permanent “history of aspiration pneumonia”
18

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 7
Sepsis• Assessment considerations
• Stage of recovery• Organs affected
• Pulmonary damage: alveolar noncompliance, debris from infiltrates ALL
• Increase respiratory rate
• Muscle damage• weakness, increased respiratory rate
• Brain damage• Cognitive impairments after sepsis
Sepsis
• Patient endurance• Weakness
• Effects of prolonged mechanical ventilation
• Depends on what organs suffered what damage…
• 40% survival … patient is not the same after surviving septic shock!
The Esophagus
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 8
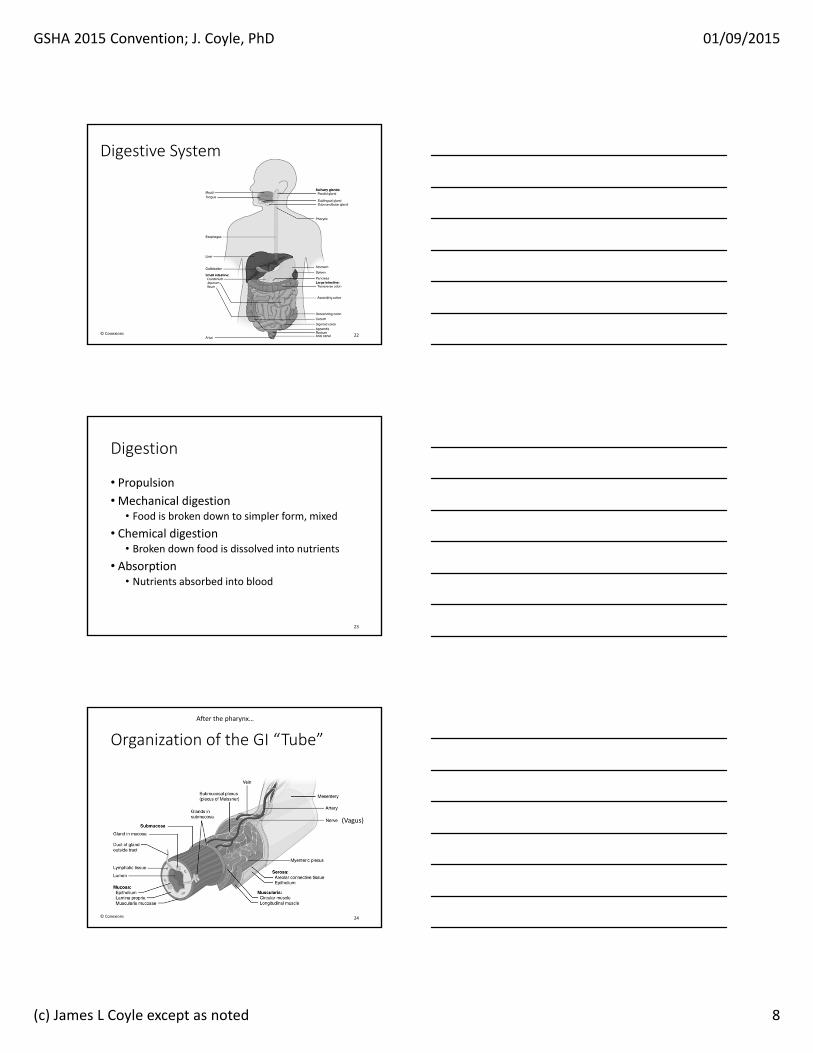
Digestive System
22© Conexions
Digestion
• Propulsion• Mechanical digestion
• Food is broken down to simpler form, mixed
• Chemical digestion• Broken down food is dissolved into nutrients
• Absorption• Nutrients absorbed into blood
23
Organization of the GI “Tube”
24© Conexions
After the pharynx…
(Vagus)

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 9
Esophagus
• Upper 1/3 striated muscle• Muscle diseases affect function
• Myositis, myasthenia gravis, myopathy/dystrophy
• Lower 2/3 progressive smooth muscle• Other disease mechanisms affect function
• Scleroderma
• Achalasia
• UES, LES differences
25
Anatomy of the gastroesophageal junction
26
Esophageal “peristalsis”
27Creative Commons 3.0, Gnu public

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 10
Esophageal disorders
28
Structural Disorders of Esophagus
• Hiatus Hernia• Stricture: Esophageal web, Schatzki ring
• + congenital, inflammatory, traumatic, reflux induced, narrowing of esophageal lumen
• Diverticulae• Pulsion• Traction
29
Hiatus Hernia
• A. Normal anatomy
• B. Flattened flexure
• C. Sliding hernia
• D. Irreducible hernia
30

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 11
Paraesophageal hernia
31©Copyright Science Press Internet Services
Hiatus hernia
Schatzki`s ring
32
on barium esophagogram
on endoscopy
‐ <13mm: always symptomatic‐ >20mm: rarely symptomatic
Esophageal web
33Creative Commons 3.0

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 12
Zenker Diverticulum
• Bulge in inferior constrictor
• Pulsion diverticulum
• Outpouching of mucosal envelope
• Superior to cricopharyngeal bar
• High pressure zone
34Coyle, 2009
Zenker’s Diverticulum
• Outpouching of mucosal tube of UES• Bulges through muscular layer• Pressure‐induced overstretching
• Incidence: 1 in 1,000 to 1 in 10,000• Subclinical signs present before diagnosis
• Excessive intraluminal pressure• Cricopharyngeal prominence or bar
• Elderly patients: about 1/3
• Typically left of midline
Coyle, 2009
Zenker diverticulum
36

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 13
Progression of symptoms
• Resistance multiple swallows regurgitation anorexia recurrent unexplained LRTI
Telltale observations on VFS• Unexplained pyriform sinus residue
• Barium filled defect rises into field
• Air‐fluid level
• Barium re‐enters pyriform sinuses from below
Coyle, 2009
Esophagitis
• Inflammation of esophageal mucosa
• Extrinsic• Irritants mucosal inflammation
• Intrinsic• Eosinophilic esophagitis
• Eosinophils infiltrate esophageal mucosa
• Stricture, impactions, dysmotility
• “Trachealization” of mucosa
39

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 14
Esophagitis
40Creative commons 3.0
Candida esophagitis (candidiasis)Herpetic esophagitis
Eosinophilic esophagitis
41Creative commons 3.0
Disorders of Esophageal Motility
• Gastroesophageal reflux• Esophageal dysmotility
• Mild dysmotility
• Diffuse esophageal spasm
• Achalasia
42

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 15
Disorders of Esophageal Motility
43
• Gastroesophageal Reflux• LES permits gastric contents to re‐enter esophagus
• food is normally reduced by acid, pepsin, bile
• all strong mucosal irritants
• mucosal injury, inflammation, re‐epithelialization, scarring
• Esophago‐laryngeal reflex (Shaker et al., 1992)
Gastroesophageal Reflux
44
Disorders Related to GER
45
• Esophagitis• Subglottic Stenosis
• Chronic laryngitis, hoarseness, cough• Aspiration Pneumonitis
• Chronic bronchitis, tracheobronchitis
• Globus‐relieved by swallowing• ? increased UES pressure in response to GER

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 16
Other Esophageal Motility Disorders
46
• Disordered peristalsis• disorganized esophageal clearance with residuals
• Reduced or absent peristalsis• stasis in esophagus
• increased esophagopharyngeal reflux risk• AKA extraesophageal reflux
• AKA L.P.R.
•Achalasia • absent peristalsis with absent LES opening
Achalasia
47
Other Esophageal Motility Disorders
48
• Diffuse Esophageal Spasm
• Nonspecific esophageal motility disorder
• 25‐50% of abnormal motility study results performed for chest pain and dysphagia
• Presbyesophagus• diminished peristalsis
• distal findings more prevalent
• impaired LES distension with proximal dilatation
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 17
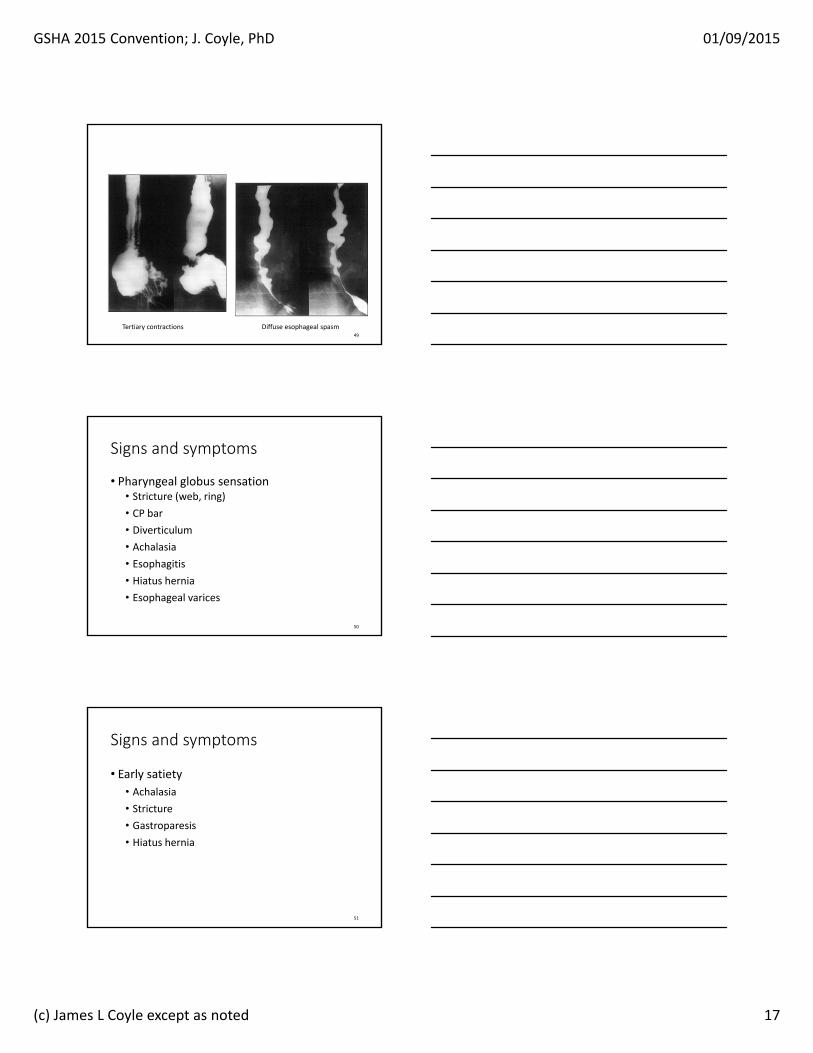
49
Tertiary contractions Diffuse esophageal spasm
Signs and symptoms
• Pharyngeal globus sensation• Stricture (web, ring)
• CP bar
• Diverticulum
• Achalasia
• Esophagitis
• Hiatus hernia
• Esophageal varices
50
Signs and symptoms
• Early satiety• Achalasia
• Stricture
• Gastroparesis
• Hiatus hernia
51

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 18
Signs and symptoms
• Cough• Esophagitis (esophagolaryngeal reflex)
• Achalasia• Filling of esophagus aspiration
• Zenker diverticulum• Regurgitation from pouch pharynx aspiration
52
Signs and symptoms
• “a funny squirting sound in my throat…”• Zenker diverticulum
• Need to swallow several times…• Zenker diverticulum
• Esophageal motility disorder
• Cricopharyngeal bar
• Esophageal varices
• Of course, oropharyngeal dysphagia
53
Signs and symptoms
• Postprandial burning
• Gastroesophageal reflux
• Nocturnal awakening with cough
• Gastroesophageal reflux
• Zenker diverticulum
54
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 19
Esophageal disorders
• Symptoms often mimic oropharyngeal dysphagia
• Negative oropharyngeal exam with persistent symptoms refer to GI
• Need to know when to refer!
Summary
• Diseases produce changes in patient function• They also explain what is wrong with my patient
• Dysphagia is a symptom!
• Assessing more than swallowing is essential!
Thank [email protected]

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 20
Dysphagia Treatment: Expected and Unexpected Results of Common
Interventions
58
James L. Coyle, Ph.D., CCC‐SLP, BCS‐SUniversity of Pittsburgh
GSHA Convention, 2015; Athens, GA
Disclosures
• I have a job and they give me a salary• University of Pittsburgh
• I see patients 2‐3 times per week• So I am biased toward their health
• NIH funds 25% of my time on an RO‐1
• I give several conferences lectures annually• Honorarium
• No products, no conflicts of interest
What is treatment?
• Are we treating the bolus, the patient, or something else?
60
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 21
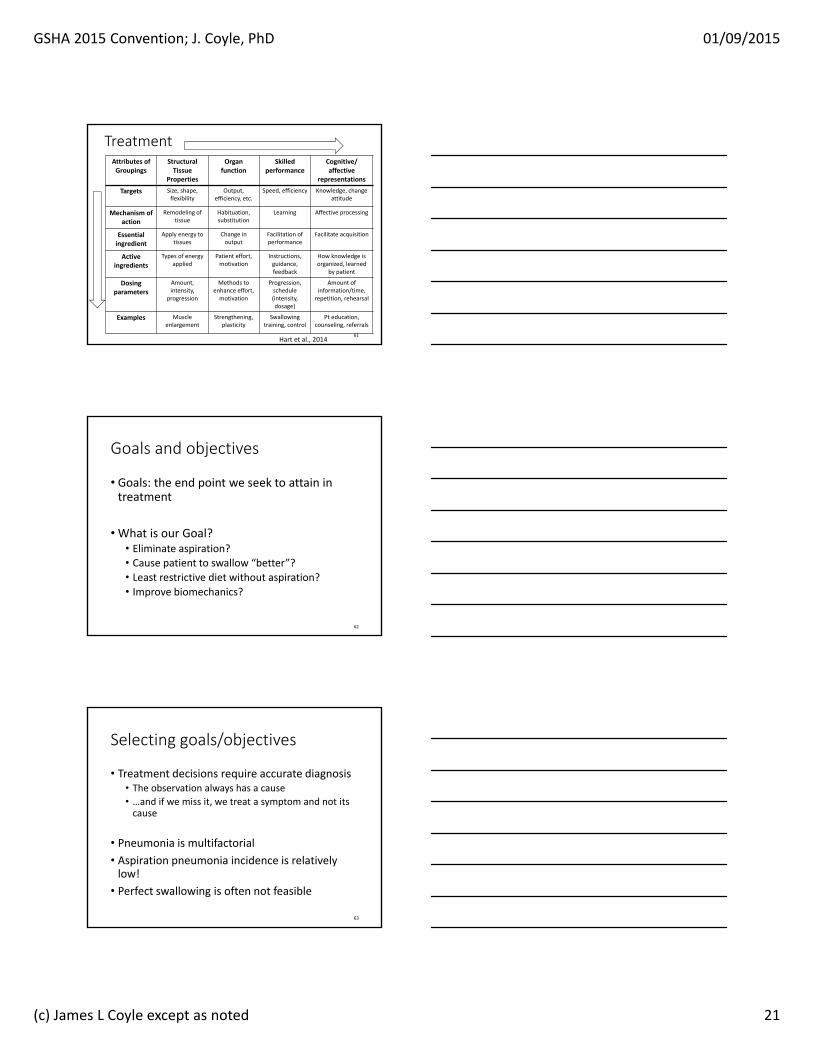
TreatmentAttributes of Groupings
Structural Tissue
Properties
Organ function
Skilled performance
Cognitive/ affective
representations
Targets Size, shape, flexibility
Output, efficiency, etc.
Speed, efficiency Knowledge, change attitude
Mechanism of action
Remodeling of tissue
Habituation, substitution
Learning Affective processing
Essential ingredient
Apply energy to tissues
Change in output
Facilitation of performance
Facilitate acquisition
Active ingredients
Types of energy applied
Patient effort, motivation
Instructions, guidance, feedback
How knowledge is organized, learned
by patient
Dosing parameters
Amount, intensity,
progression
Methods to enhance effort, motivation
Progression, schedule (intensity, dosage)
Amount of information/time, repetition, rehearsal
Examples Muscle enlargement
Strengthening, plasticity
Swallowing training, control
Pt education, counseling, referrals
Hart et al., 201461
Goals and objectives
• Goals: the end point we seek to attain in treatment
• What is our Goal?• Eliminate aspiration?• Cause patient to swallow “better”?• Least restrictive diet without aspiration?• Improve biomechanics?
62
Selecting goals/objectives
• Treatment decisions require accurate diagnosis• The observation always has a cause• …and if we miss it, we treat a symptom and not its cause
• Pneumonia is multifactorial
• Aspiration pneumonia incidence is relatively low!
• Perfect swallowing is often not feasible
63

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 22
• Objective measure of change(+ or ‐) ?
• Incremental reassessment
• Data collection – are we doing it?
• Termination criteria?
• Would you pay for this out of pocket?
• Is patient a good candidate for selected behavioral interventions?
64
Justifying Treatment
Some Common Interventions…
• They are designed for this…• Intended consequences
• But they also do this…• Unintended consequences
• Sometimes good…
• Sometimes not so good…
65
Some Common Interventions… compensate…
1. Head rotation posture* ‐ divert bolus Directs bolus to opposite side of pharynx Compensate for unilateral noncompliance
BUT IT ALSO: Increases UESO diameter (rotation to either side in normals)
Reduces UES pressure (either side, normals)
Increased intrabolus pressure Reduces contralateral pyriform sinus pressure**
66*Logemann et al (1989); **Takasaki et al., 2012
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 23
Some Common Interventions… compensate…
• 2. Chin‐down posture*‐ reduce aspiration• Patients with aspiration due to “pharyngeal delay”
• 50% did not aspirate with CDP (OR = 0.5)• Continued aspirators: pyriform sinus residue aspirated• Valleculae widened
• Anterior bolus position (phar. delay, oral containment)
• BUT IT ALSO:• Reduces intrabolus hypopharyngeal pressure**
• Contraindicated in patient with weak constrictors
67*Shanahan et al. (1993); **Bulow et al (2002)
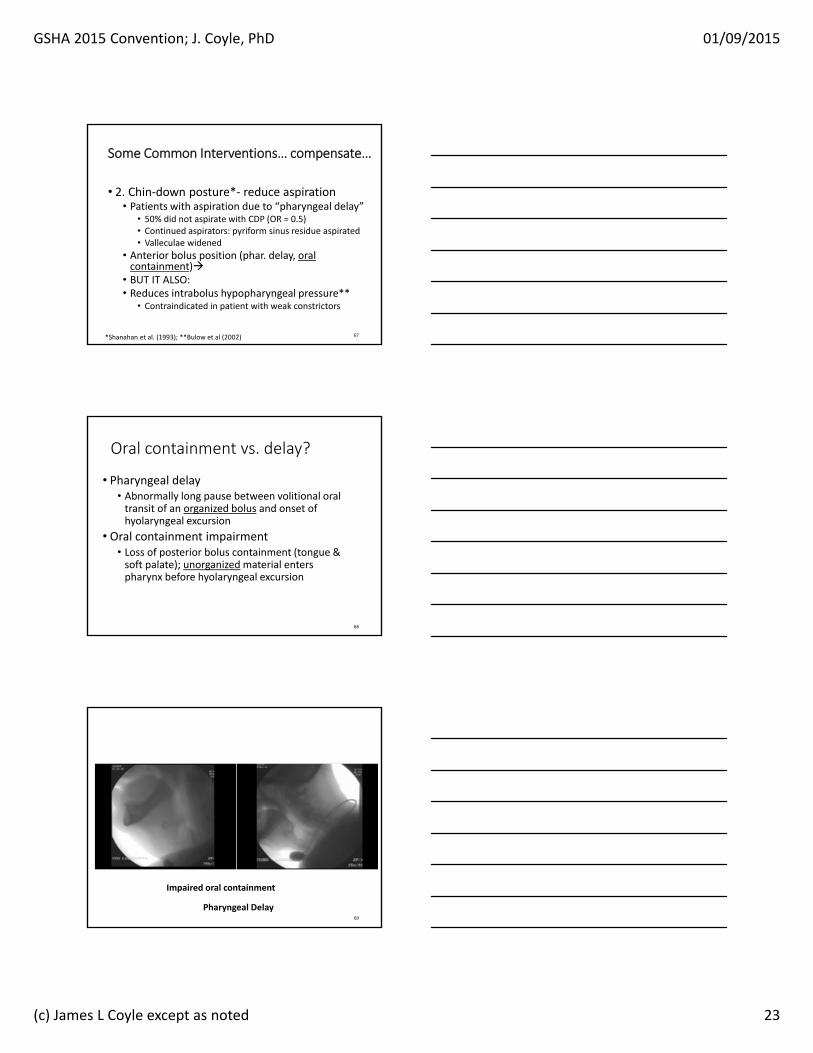
Oral containment vs. delay?
• Pharyngeal delay• Abnormally long pause between volitional oral transit of an organized bolus and onset of hyolaryngeal excursion
• Oral containment impairment• Loss of posterior bolus containment (tongue & soft palate); unorganized material enters pharynx before hyolaryngeal excursion
68
Pharyngeal Delay
Impaired oral containment
69
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 24
Some Common Interventions… compensate…
•3. Head/neck lateral flexion posture
• oral flow diversion toward side of flexion
• unilateral lingual, oral/facial motor, sensory deficits
• It does not affect pharyngeal physiology
70
Some Common Interventions… compensate…
• 4. Increase duration of UES opening*• Mendelsohn Maneuver
• maintains prolonged HLE
• BUT IT ALSO:• Is difficult to teach, difficult to perform
• SEMG biofeedback training improves treatment effect* **
71*Logemann et al (1990); ** Coyle (2008)
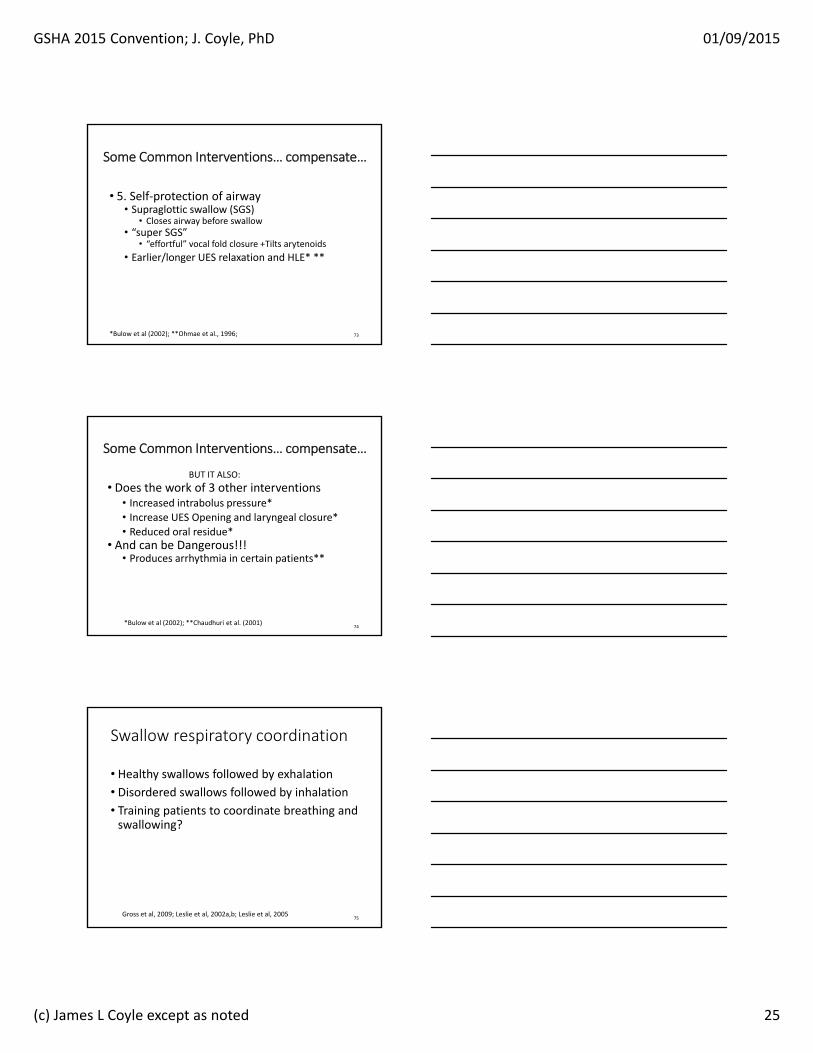
72
First VisitBaseline (A-1)
Second VisitPost-Treatment (B-2)
2‐Standard Deviation Band Sample Graphic
2 SD Band Test: p<0.05;C Statistic: p=0.00001.
p<0.05
UES OpeningDuration
seconds
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 25
Some Common Interventions… compensate…
• 5. Self‐protection of airway• Supraglottic swallow (SGS)
• Closes airway before swallow• “super SGS”
• “effortful” vocal fold closure +Tilts arytenoids
• Earlier/longer UES relaxation and HLE* **
73*Bulow et al (2002); **Ohmae et al., 1996;
• Does the work of 3 other interventions• Increased intrabolus pressure*• Increase UES Opening and laryngeal closure*• Reduced oral residue*
• And can be Dangerous!!!• Produces arrhythmia in certain patients**
74*Bulow et al (2002); **Chaudhuri et al. (2001)
BUT IT ALSO:
Some Common Interventions… compensate…
Swallow respiratory coordination
• Healthy swallows followed by exhalation• Disordered swallows followed by inhalation
• Training patients to coordinate breathing and swallowing?
75Gross et al, 2009; Leslie et al, 2002a,b; Leslie et al, 2005

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 26
• 6. Tongue holding/tether• Bulge in PPW during swallow
• Inhibits tongue motion
• Increases oral residue in normals
• BUT IT ALSO:
• Is not intended for use by patients when swallowing!
76
Fujiu & Logemann (1996)
Some Common Interventions… compensate…
• 7. Bolus modification• Larger bolus
• Earlier HLE, tongue movement, UES opening*
• Taste, temperature, consistency• Earlier activation in some patients**
• Will patient eat/drink it???
77*Cook et al., 1989; Dantas et al., 1990; **Ding et al., 2003
Some Common Interventions… compensate…
• And when we combine maneuvers we treat multiple problems
• …but we need evidence that each is appropriate for the impairment
78

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 27
What about texture modification and Water?
79
Diet modification
• Should be the last compensatory method evaluated in testing
• Logemann, 1993
• Issues:• What does texture modification do for patient?
• Is patient amenable to modification?
• Will patient eat the prescribed diet • Malnutrition, dehydration
80
Diet modification
• Assuming that behavioral/compensation fails
• Increasing friction and reducing flow rate (thick)• When pharyngeal stage is delayed and dangerous
• Oral containment cannot be otherwise managed
• Some times when laryngeal closure is incomplete
• Decreasing friction and increasing flow rate (thin)
• Inability to propel bolus• UES does not distend adequately• Need good airway protection
81

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 28
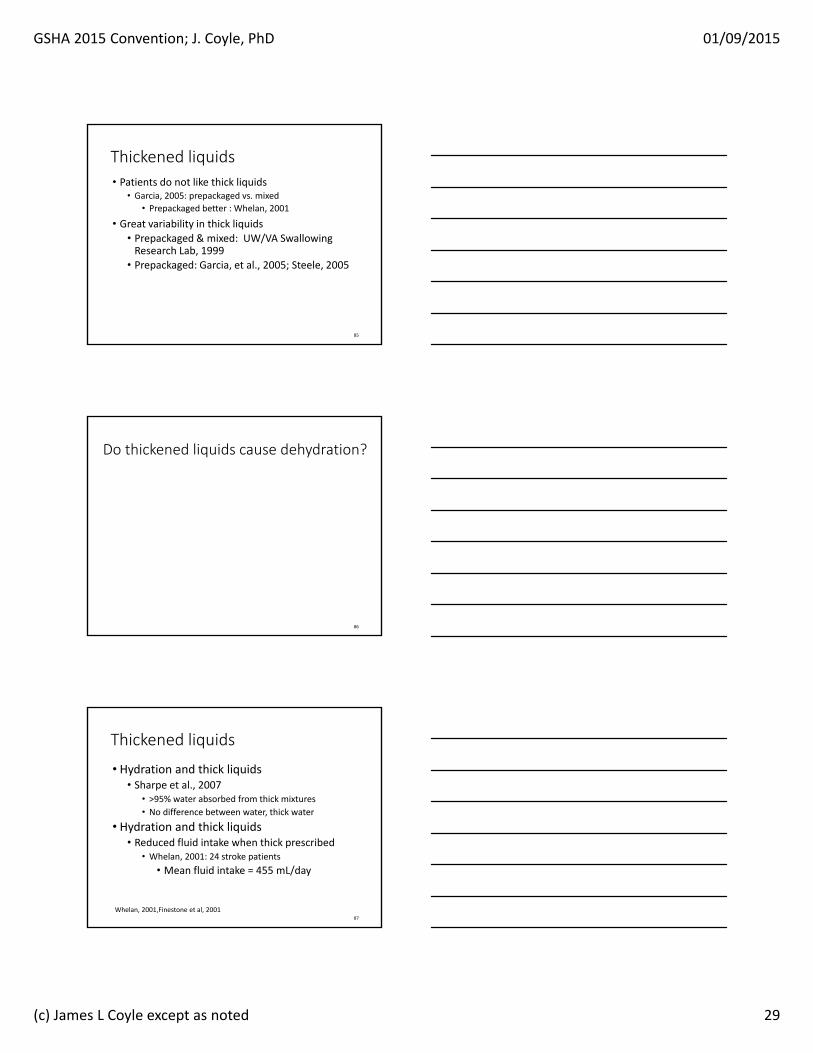
Thickened liquids
• Reduces aspiration of thin liquids• Kuhlemeier et al., 2001; Logemann et al., 2008
• Swallow apnea later/longer with thick liquids• Hiss et al., 2004; Butler et al., 2004
• More effort needed to clear thick• Nicosia et al., 2001
82
Thick liquids
• Thin liquids aspirated most frequently• Compared to other viscosities
• Spawned experimentation with thick liquids
• Theory for dysphagia use:• Slowing the flow
• Compensates for mistimed airway closure
• What do we know about them?
83
Water
• Intake of water: ~2300 mL per day• 2100mL through intake• 200 mL synthesized by body (CHO metabolism)
• Variations in water intake• Climate, habits, physical activity
84
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 29
Thickened liquids
• Patients do not like thick liquids• Garcia, 2005: prepackaged vs. mixed
• Prepackaged better : Whelan, 2001
• Great variability in thick liquids• Prepackaged & mixed: UW/VA Swallowing Research Lab, 1999
• Prepackaged: Garcia, et al., 2005; Steele, 2005
85
Do thickened liquids cause dehydration?
86
Thickened liquids
• Hydration and thick liquids• Sharpe et al., 2007
• >95% water absorbed from thick mixtures
• No difference between water, thick water
• Hydration and thick liquids• Reduced fluid intake when thick prescribed
• Whelan, 2001: 24 stroke patients
• Mean fluid intake = 455 mL/day
87
Whelan, 2001,Finestone et al, 2001

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 30
Thick liquids
• Protocol 201 (Logemann et al., 2007; Robbins et al., 2008)
• Problem: Thin liquid aspiration
• Chin Down Posture vs. Thick liquids• Nectar, honey
• Parkinson’s disease, dementia, both
88
89
Aspirate thin liquids on VFS (711)
VFS: 1. Thin/chin 2. Nectar
3. Honey
Aspirate thin liquids on VFS (711)
VFS: 1. Thin/chin 2. Nectar
3. Honey
Eligible, consent: VFS
PART 1:Do thick liquidsor chin‐down
posture preventaspiration?
Thin liquid Thin liquid‐chin‐down
Nectar Honey
Aspiration 100% 68% 63% 53%
Preference 1st 2nd 3rd last
Results
Some aspirated on 1Some aspirated on 2
Some aspirated on ALL 3
90
Thin/Chin259
Nectar133
Honey123
Pneumonia, death
Dehydration, UTI, compliance,
etc.
Randomization515 patients 3 months
Aspirate thin liquids on VFS (711)
VFS
Aspirate on 1 or 2 interventions
Excluded from Part 2: cannot randomize to a
condition
(166) (345)
Aspirate on NOinterventions (all
worked)
Aspirate on ALL 3interventions (all
failed)
PART 2:What is pneumonia
incidence in aspirators of thin
liquid randomized to drink:
nectar thick,honey thick,
chin‐down/thin for 3 months?

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 31
91
Results of Part 2
Randomization515 patients 3 months
Aspirate on NO interventions
Aspirate on ALL interventions
Randomization515 patients 3 months
Aspirate on NO interventions
Aspirate on ALL interventions
Thin/ Chin
Nectar HoneyThin/ Chin
Nectar Honey
Pneumonia(52)
166(aspirated on NONE
on VFS)
345(aspirated on ALL 3
on VFS)
4210
11% of all patients
Pneumonia
Chin‐thin All thick liquid Nectar Honey
All patients (52)
24 (10%) 28 (11%) 10 (8%) 18 (15%)
Aspirated none in
Part 1 (10)6 (7%) 4 (5%) 0 (0%) 4 (10%)
Aspirated all 3 in
Part 1 (42)18 (9.8%) 24 (14%) 10 (11.5%) 14 (19%)
Patients who aspirated on ALL 3, drinking honey thick liquids,had twice as many pneumonias as those drinking thin liquids
Overall, patients drinking thin or thick liquids had similar pneumonia incidence
Pneumonia
92
Thick liquids
• Other results• Dehydration: Thin: 2%, Thick: 6%
• UTI: Thin: 3%, Thick: 6%
• Median hospital stay with pneumonia
• Honey (18 d.), nectar (4 d.), CDP (6 d.)
93

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 32
Thick liquids
• Do thick liquids reduce aspiration?• Yes
• Do thick liquids reduce pneumonia risk?• No
• Are aspirators more likely to get pneumonia?• Yes
• Do patients like thick liquids?• No
• Will they drink it if they don’t like it?• Probably not
94
Thick liquids
• So, what are we doing when we prescribe thick liquids???
• We think we are reducing risk…
• Are we just shifting risk to a different place?• Hydration kidneys? QOL?
95
Evidence Summary for using Free Water Protocols
“Free Water” Protocols
96
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 33
• Rationale of protocol per developers:• 1. Need for hydration – self evident
• 2. Poor compliance with thick liquids
• We have reviewed that data
• 3. Safety of water aspiration
• One study published before 2008!!!
97
“Free Water Protocol” Principles
Safety of water aspiration
• Bronchoalveolar lavage
• Whelan et al. (2001) reduced fluid intake in patients prescribed thick liquids
• Numerous citations on dehydration in dysphagia
• Animal studies of water aspiration
98
Evidence: one study before 2008
• Garon et al., 1997• 20 aspiration‐documented CVA patients
• Aspirated liquid only on VFSS
• Randomized to free water or no free water
• Duration: treatment + 30 day follow up
• Small and underpowered study• Yet the main evidence for protocol
99

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 34
• Results• No patient in either group developed pneumonia
• No dehydration, complications
• Intake of fluids comparable between groups
• 1210 mL (C) ‐ all thick• 1318 mL (E): 855mL thick, 463mL thin
• “Much less water than expected” by investigators (“we were surprised…”)
100
Half of daily needs
Water Protocol Evidence
• Randomization to water protocol or prescribed dietary fluid (26 patients)
• 17 patients requiring feeding assistance• 8 assigned to control, 9 to treatment
• 9 independent feeding patients• 3 assigned to control, 6 to treatment
• All received oral care four times per day
• Outcomes: pneumonia, death, UTI, FIM, LOS, intake
Becker, et al., 2008
101
• Results• Pneumonia: 1 patient in each group
• UTI: 2 patients in each group
• FIM: no significant difference
• FCM: no significant difference
• Length of stay: 29.1 days (control) vs. 15.8 (tx)
Water Protocol Evidence
102Becker, et al., 2008

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 35
Water Protocol Evidence
• Death: 2 treatment deaths, no control deaths
• Both patients that died had chronic pulmonary conditions
• Other findings:
• Independent patients consumed significantly less fluid than dependent patients (p<.01), regardless of group
103
Recent Evidence
• Karagiannis et al. (2011)• Significant increase in lung complications (6/42) vs. controls (0/34)
• Carlaw et al. (2011)
• No complications in either group
• More fluid intake in “protocol” patients
104
Using the /k/ phoneme
105
Perlman et al, 1989
Modified Valsalva:“make a /k/ as hardas you can and holdit for as long as you can, don’t let anyair escape.”
Hawk:“say the word ‘hawk’,make the /k/ as hardas you can.”

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 36
106
“Hawk”, modified valsalva produced ~20% of muscle activity seen during swallow
Carbonated thin liquid
• Order effects**?• Command swallow effects***?
• Cued swallows significantly shorter duration
107
*Bulow et al., 2003; ** Robbins et al, 1999; *** Daniels et al., 2007
*
NMES
• Most studies contain flaws• Most frequent
• No control for recovery• Lack of blinded judges• Subjective criteria for “success”
• Recent work with transoral NMES to pharynx• Interesting, need more data
• Patient selection? What are we treating?
108

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 37
• “This preliminary meta‐analysis revealed a smallbut significant summary effect size for transcutaneous NMES for swallowing. Because of the small number of studies and low methodological grading for these studies, caution should be taken in interpreting this finding. These results support the need for more rigorous research in this area.”
• Small = clinically insignificant
• Low grading = invalid results
109
Carnaby‐Mann & Crary, 2007
End of life intervention
• What is the goal?
• Medicine tries to achieve the best balance of risks and benefits to achieve the goal
• Patient comfort vs. adverse outcomes?
110
Feeding tubes?
• Unequivocal lack of benefit • At end of life
• In advanced dementia
• Imposes additional (and unintended) risks
• Increased aspiration risk from stomach
• Does not mitigate oral aspiration
111
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 38
What’s going on in the research?
• Exercise• Plasticity
• Diagnostic methods to assist with treatment
112
Restorative methods
• Emerging efficacy in the literature
• Exercise‐Preventive, Restorative, beyond?• physiologic logic, predicted baseline, target
• muscle strengthening requires repetition to modify contractile properties (hundreds, thousands…)
• Do range of motion exercises do anything?
113
Exercise
Tongue Press exercise
• AKA tongue press exercise• Device assisted with biofeedback
Lingual Strengthening Exercise
114

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 39
Testing/measurement Exercise protocol
115
Significant Differences
• Reduced oropharyngeal residue• Pharyngeal (p = .03), overall (p = .01 ‐ .02)
• Improved PA scores (3mL, 10mL liquid)• 4 weeks: p = .02; 8 weeks: p = .005
• Increased isometric pressure• Anterior 4‐8 wk:(p = .001); posterior (p = .01, .001)
• Increased swallowing pressure• All consistencies/volumes at 4, 8 weeks.
Lingual Strengthening Exercise
116
Restorative Methods
• Exercise• Resistive expiratory exercise
• Increase force of expiratory effort
Sapienza et al.
117
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 40
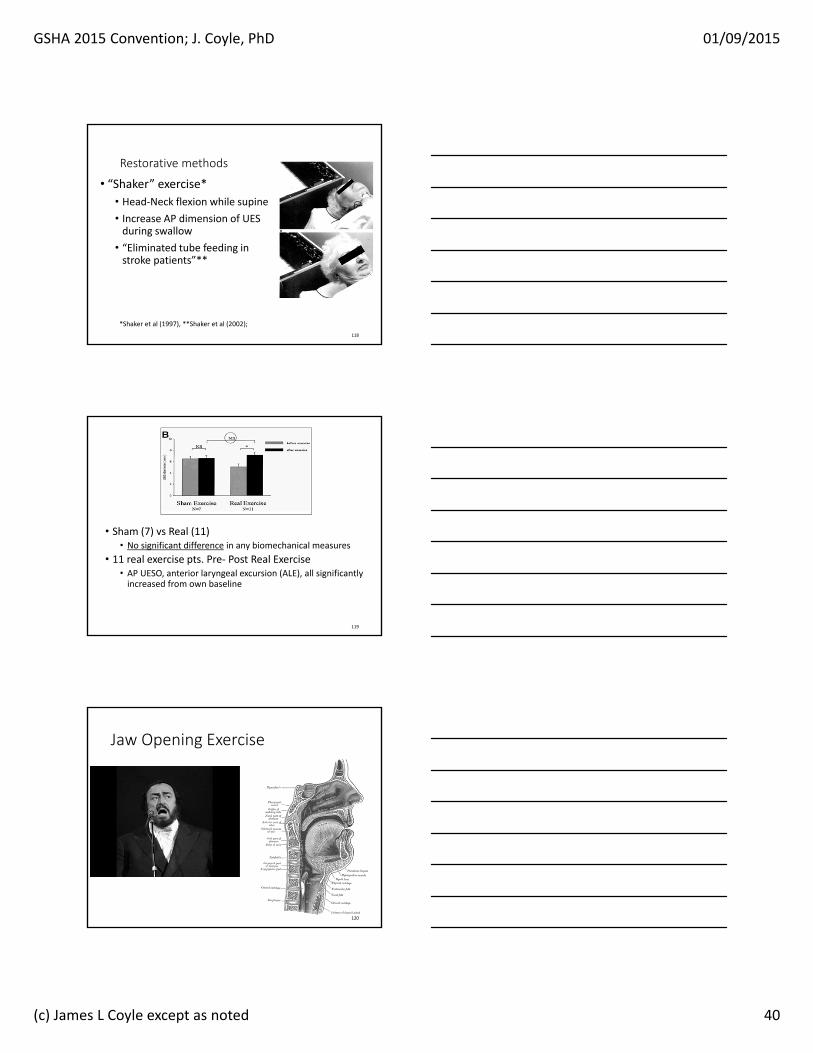
• “Shaker” exercise*• Head‐Neck flexion while supine
• Increase AP dimension of UES during swallow
• “Eliminated tube feeding in stroke patients”**
118
*Shaker et al (1997), **Shaker et al (2002);
Restorative methods
• Sham (7) vs Real (11)• No significant difference in any biomechanical measures
• 11 real exercise pts. Pre‐ Post Real Exercise• AP UESO, anterior laryngeal excursion (ALE), all significantly increased from own baseline
119
Jaw Opening Exercise
120
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 41
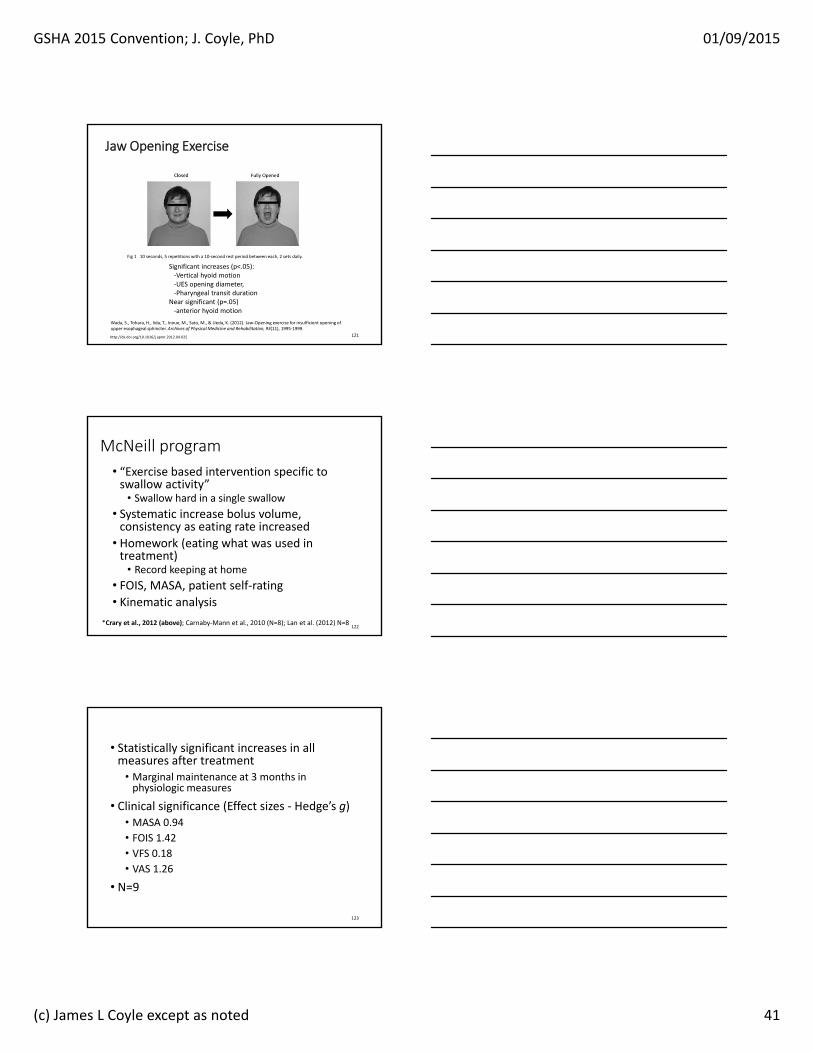
Fig 1 10 seconds, 5 repetitions with a 10‐second rest period between each, 2 sets daily.
Wada, S., Tohara, H., Iida, T., Inoue, M., Sato, M., & Ueda, K. (2012). Jaw‐Opening exercise for insufficient opening of upper esophageal sphincter. Archives of Physical Medicine and Rehabilitation, 93(11), 1995‐1999.
http://dx.doi.org/10.1016/j.apmr.2012.04.025
Jaw Opening Exercise
Significant increases (p<.05): ‐Vertical hyoid motion‐UES opening diameter, ‐Pharyngeal transit duration
Near significant (p=.05)‐anterior hyoid motion
121
• “Exercise based intervention specific to swallow activity”
• Swallow hard in a single swallow
• Systematic increase bolus volume, consistency as eating rate increased
• Homework (eating what was used in treatment)
• Record keeping at home
• FOIS, MASA, patient self‐rating
• Kinematic analysis
122*Crary et al., 2012 (above); Carnaby‐Mann et al., 2010 (N=8); Lan et al. (2012) N=8
McNeill program
• Statistically significant increases in all measures after treatment
• Marginal maintenance at 3 months in physiologic measures
• Clinical significance (Effect sizes ‐ Hedge’s g)• MASA 0.94
• FOIS 1.42• VFS 0.18• VAS 1.26
• N=9
123

GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 42
Measure Baseline Post‐treatment
Post tx 3 months
Significance measure
g P g P
MASA 0.94 <0.02 0.13 0.67
FOIS 1.42 0.01 0.74 0.17
VFS 0.18 0.37
VAS 1.26 <0.01 ‐0.21 0.38
LP pressure 0.05 NS124
• Thermal Tactile Stimulation
• Thought to stimulate afferent pathways *
• No evidence supports sustained effects• High dosage over long term produced momentarily quicker onset of HLE (reduced DST)**
• Taste‐sour bolus (50% lemon juice/barium)
• Reduced aspiration in neuro patients***
• Reduced DST in stroke patients***
125*Fujiu et al. (1994); **Rosenbek et al (1991, 1996, 1998); ***Logemann et al (1994)
Facilitative Methods
Facilitative Methods• Interest in manipulating other sensory modalities
• Taste, vibratory sense, electrical stimulation (?)
• Can the brain be rewired in adults?• Emerging evidence that “something” is happening upstream
• MEG, EEG (record the effects), MRI
• TCMS (stimulate motor effects)
• Direct current stimulation
• Exercise
• Implantable intramuscular ES
Jayasekeran et al., 2010, 2011; Pelletier & Lawless, 2003; Malandraki et al., 2011 126
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 43
• What is plasticity?• Alteration in the outcome
• Motor learning theory?• Mass practice
• Dosage, intensity, progressive resistance + (other increments)
• Task specificity• Neural adaptation
127
Diagnostic methods
• High speed MRI imaging
• Still crude
• Patient must be supine
• Screening• Accelerometry and acoustics
128
Hype & enthusiasm
129
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 44
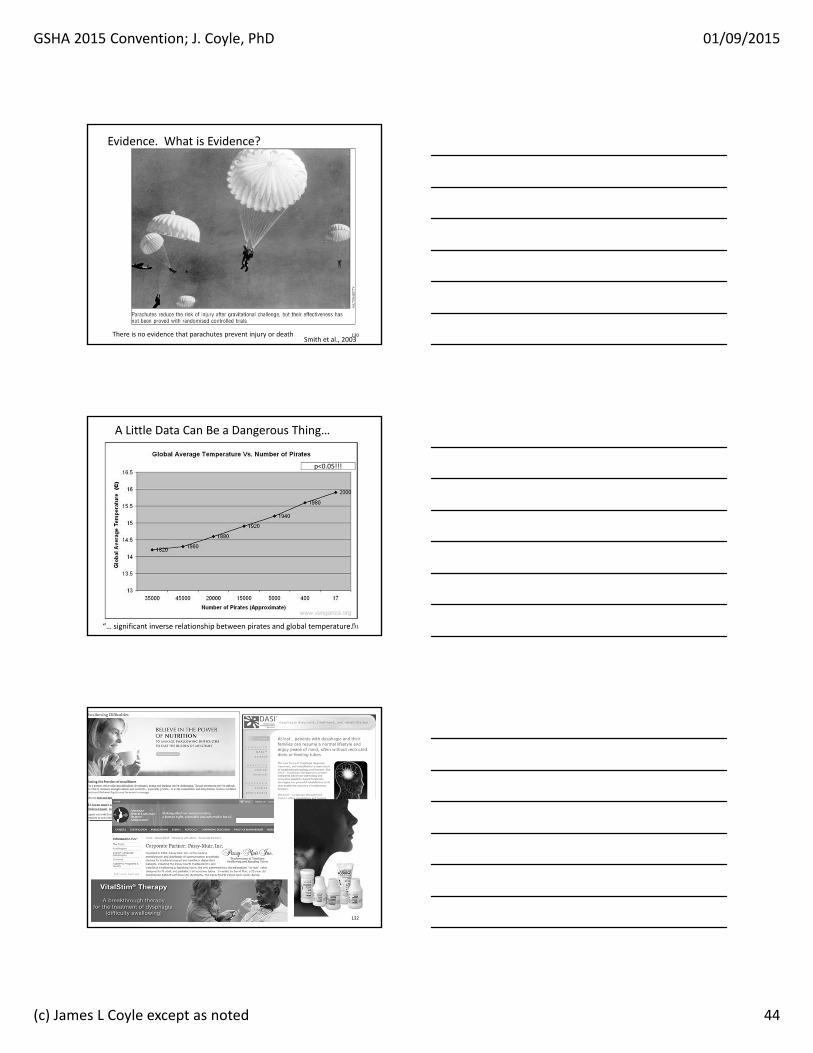
Evidence. What is Evidence?
Smith et al., 2003130There is no evidence that parachutes prevent injury or death
“… significant inverse relationship between pirates and global temperature.”
p<0.05!!!
A Little Data Can Be a Dangerous Thing…
131
132
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 45
133
134
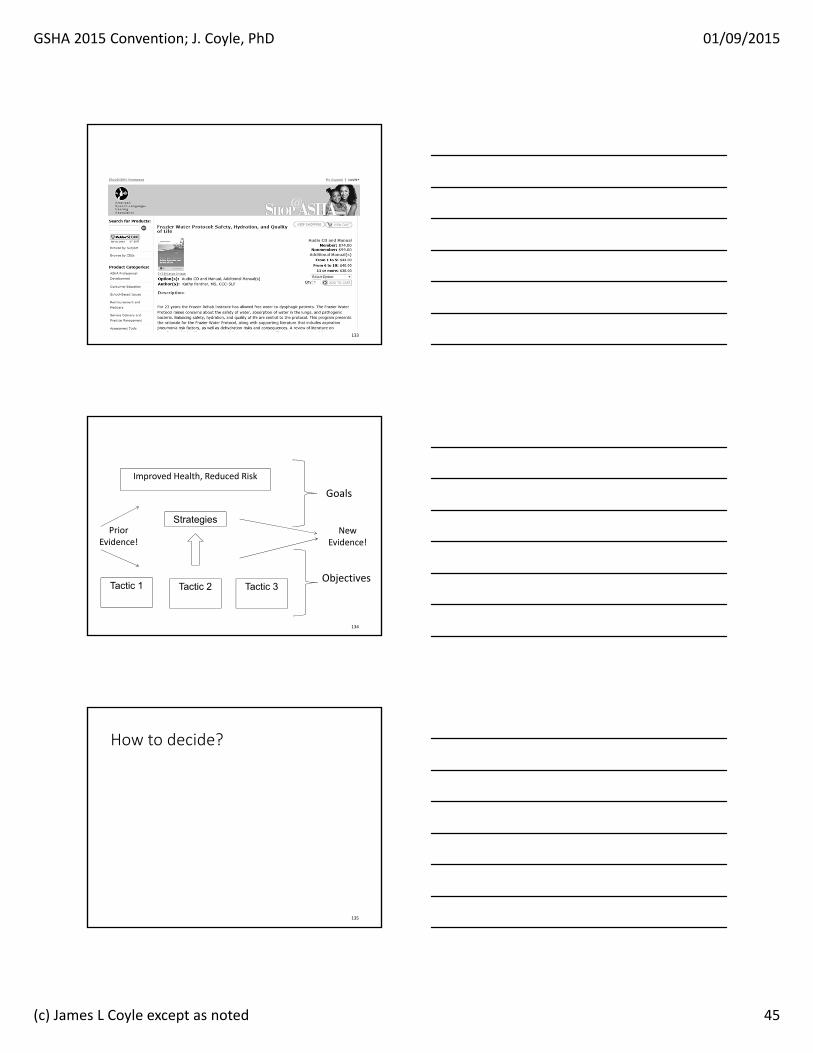
Tactic 1 Tactic 2 Tactic 3
Strategies
Objectives
Improved Health, Reduced Risk
Goals
NewEvidence!
PriorEvidence!
How to decide?
135
GSHA 2015 Convention; J. Coyle, PhD 01/09/2015
(c) James L Coyle except as noted 46
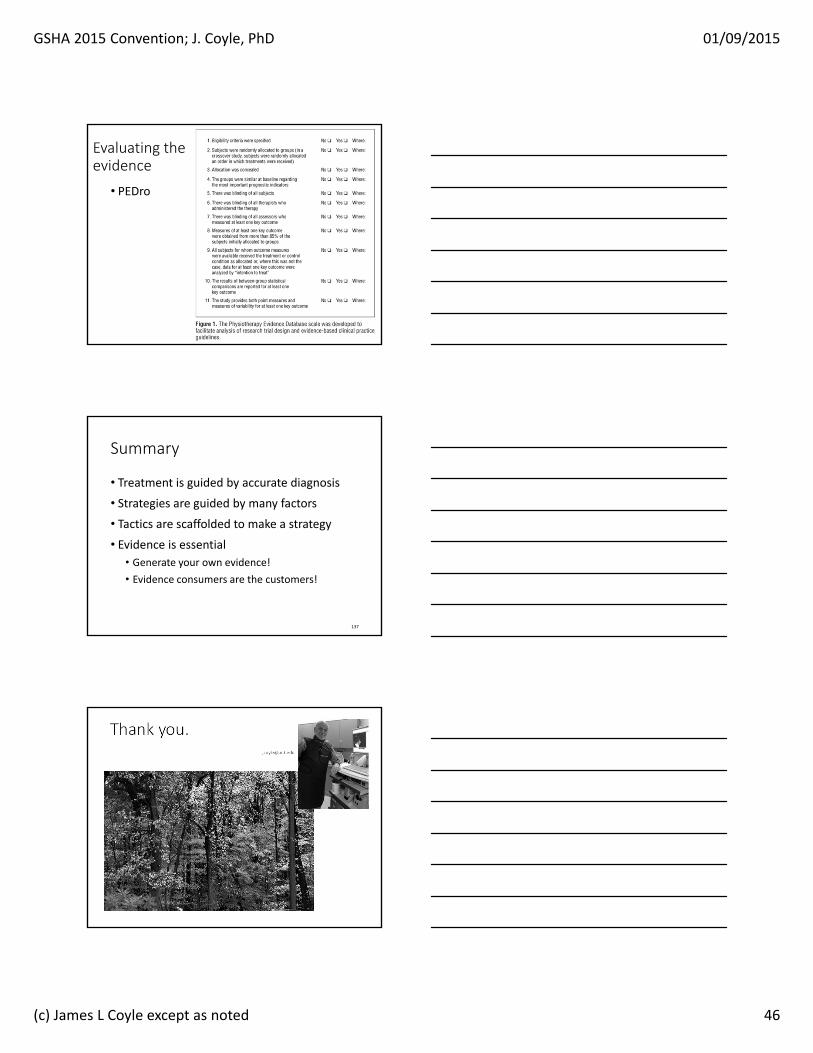
Evaluating the evidence
• PEDro
136
Summary
• Treatment is guided by accurate diagnosis
• Strategies are guided by many factors
• Tactics are scaffolded to make a strategy
• Evidence is essential• Generate your own evidence!
• Evidence consumers are the customers!
137
Thank [email protected]

Acheson, D. E. (2003). FDA Public Health Advisory: Reports of blue discoloration and death in patients receiving enteral feedings tinted with the dye, FD&C blue No. 1. http://www.cfsan.fda.gov/~dms/col-ltr2.html.
Aitken, M. E., & Hammond, D. C. M. (2002). Double-muscle flap repair of the tethered tracheostomy scar. Annals of Plastic Surgery, 49(3), 328-332.
Ajemian, M. S., Nirmul, G. B., Anderson, M. T., Zirlen, D. M., & Kwasnik, E. M. (2001). Routine fiberoptic endoscopic evaluation of swallowing following prolonged intubation: implications for management. Archives of Surgery., 136(4), 434-437.
Alia, I., & Esteban, A. (1999). Protocol-guided weaning:a key issue in reducing the duration of mechanical ventilation. Intensivmed, 36(5), 429-435.
Alkhuja, S. (1998). Dysphagia in the patient with a tracheostomy: six cases of inappropriate cuff deflation or removal. Heart & Lung: Journal of Acute & Critical Care., 27(1), 74.
Barker, J., Martino, R., Reichardt, B., Hickey, E. J., & Ralph-Edwards, A. (2009). Incidence and impact of dysphagia in patients receiving prolonged endotracheal intubation after cardiac surgery. Canadian Journal of Surgery, 52(2), 119-124.
Barquist, E., Brown, M., Cohn, S., Lundy, D., & Jackowski, J. (2001). Postextubation fiberoptic endoscopic evaluation of swallowing after prolonged endotracheal intubation: a randomized, prospective trial. Critical Care Medicine, 29(9), 1710-1713.
Belafsky, P. C., Blumenfeld, L., LePage, A., & Nahrstedt, K. (2003). The accuracy of the modified Evan's blue dye test in predicting aspiration. Laryngoscope., 113(11), 1969-1972.
Bennett, J., Van Lieshout, P., Pelletier, C., & Steele, C. (2009). Sip-sizing behaviors in natural drinking conditions compared to instructed experimental conditions. Dysphagia, 24(2), 152-158.
Bernhard, W., Yost, L., Joynes, D., Cothalis, S., & Turndorf, H. (1985). Intracuff pressures in endotracheal and tracheostomy tubes. Related cuff physical characteristics. Chest, 87, 720 - 725.
Bordon, A., Bokhari, R., Sperry, J., Testa, D. t., Feinstein, A., & Ghaemmaghami, V. (2011). Swallowing dysfunction after prolonged intubation: analysis of risk factors in trauma patients. American Journal of Surgery, 202(6), 679-682. doi: http://dx.doi.org/10.1016/j.amjsurg.2011.06.030
Borzelleca, J. F., Depukat, K., & Hallagan, J. B. (1990). Lifetime toxicity/carcinogenicity studies of FD & C Blue No. 1 (brilliant blue FCF) in rats and mice. Food Chem Toxicol, 28(4), 221-234.
Brookes, J. T., Seikaly, H., Diamond, C., Mechor, B., & Harris, J. R. Prospective randomized trial comparing the effect of early suturing of tracheostomy sites on postoperative patient swallowing and rehabilitation. Journal of Otolaryngology, 35(2), 77-82.
Burns, H. P., Dayal, V. S., Scott, A., van Nostrand, A. W., & Bryce, D. P. (1979). Laryngotracheal trauma: observations on its pathogenesis and its prevention following prolonged orotracheal intubation in the adult. Laryngoscope, 89(8), 1316-1325.
Cameron, J. L., Reynolds, J., & Zuidema, G. D. (1973). Aspiration in patients with tracheotomies. Surgical Gynecology and Obstetrics, 136, 68-70.
Carnaby-Mann, G. D., & Crary, M. A. (2010). McNeill dysphagia therapy program: a case-control study. Archives of Physical Medicine & Rehabilitation, 91(5), 743-749. doi: http://dx.doi.org/10.1016/j.apmr.2010.01.013
Chastre, J., & Fagon, J.-Y. (2002). Ventilator-associated pneumonia. American Journal of Respiratory and Critical Care Medicine, 165(7), 867-903. doi: 10.1164/ajrccm.165.7.2105078
Chin, R. Y., & Ellul, S. (2009). Dysphagia after emergency intubation: case report and literature review. Dysphagia, 24(1), 105-108. doi: http://dx.doi.org/10.1007/s00455-008-9154-3
Colton-House, J., Noordzij, J. P., Murgia, B., & Langmore, S. (2011). Laryngeal injury from prolonged intubation: a prospective analysis of contributing factors. Laryngoscope, 121(3), 596-600. doi: http://dx.doi.org/10.1002/lary.21403
Crary, M. A., Carnaby, G. D., LaGorio, L. A., & Carvajal, P. J. (2012). Functional and physiological outcomes from an exercise-based dysphagia therapy: a pilot investigation of the McNeill Dysphagia Therapy Program. Archives of Physical Medicine & Rehabilitation, 93(7), 1173-1178. doi: http://dx.doi.org/10.1016/j.apmr.2011.11.008
Curiel Garcia, J., Guerrero-Romero, F., & Rodriguez-Moran, M. (2001). [Cuff pressure in endotracheal intubation: should it be routinely measured?]. Gac Med Mex, 137, 179 - 182.
Czop, M., & Herr, D. L. M. (2002). Green skin discoloration associated with multiple organ failure. Critical Care Medicine, 30(3), 598-601.
Dettelbach, M. A., Gross, R. D., Mahlmann, J., & Eibling, D. E. (1995). Effect of the Passy-Muir Valve on aspiration in patients with tracheostomy. Head & Neck, 17(4), 297-302.
DeVita, M. A., & Spierer-Rundback, L. (1990). Swallowing disorders in patients with prolonged orotracheal intubation or tracheostomy tubes. Critical Care Medicine, 18(12), 1328-1330.
Dikeman, K., & Kasandjian, M. (2003). Communication and swallowing management of tracheostomized and ventilator-dependent adults. Clifton Park, N.J.: Thomson Delmar Learning.
El Solh, A., Okada, M., Bhat, A., & Pietrantoni, C. (2003). Swallowing disorders post orotracheal intubation in the elderly. Intensive Care Medicine, 29(9), 1451-1455.
Eliachar, I. (2000). Unaided Speech in Long-Term Tube-Free Tracheostomy. Laryngoscope, 110(5), 749-760.
Engoren, M., Arslanian-Engoren, C., & Fenn-Buderer, N. (2004). Hospital and long-term outcome after tracheostomy for respiratory failure. Chest, 125(1), 220-227.
File, T. M., Tan, J. S., Thomson, R. B., Stephens, C., & Thompson, P. (1995). An outbreak of Pseudomonas aeruginosa ventilator-associated respiratory infections due to contaminated food coloring dye--further evidence of the significance of gastric colonization preceding nosocomial pneumonia. Infection Control & Hospital Epidemiology, 16(7), 417-418.
Freeman, B. D., & Morris, P. E. (2012). Tracheostomy practice in adults with acute respiratory failure. Critical Care Medicine, 40(10), 2890-2896.
Gaynor, E. B., & Greenberg, S. B. (1985). Untoward sequelae of prolonged intubation. Laryngoscope, 95(12), 1461-1467.
Gilbey, P. (2012). Fatal complications of percutaneous dilatational tracheostomy. American Journal of Otolaryngology, 33(6), 770-773. doi: http://dx.doi.org/10.1016/j.amjoto.2012.07.001
Gottschalk, A., Burmeister, M., Blanc, I., Schulz, F., & Standl, T. (2003). [Rupture of the trachea after emergency endotracheal intubation]. Anasthesiol Intensivmed Notfallmed Schmerzther, 38, 59 - 61.
Griffiths, J., Barber, V. S., Morgan, L., & Young, J. D. (2005). Systematic review and meta-analysis of studies of the timing of tracheostomy in adult patients undergoing artificial ventilation. from http://www.bmj.com/cgi/content/abstract/bmj.38467.485671.E0v1
doi:10.1136/bmj.38467.485671.E0 (published 18 May 2005) Gross, R. D., Mahlmann, J., & Grayhack, J. P. (2003). Physiologic effects of open and closed tracheostomy
tubes on the pharyngeal swallow. Annals of Otology, Rhinology & Laryngology., 112(2), 143-152. Hamdy, S., Jilani, S., Price, V., Parker, C., Hall, N., & Power, M. (2003). Modulation of human swallowing
behaviour by thermal and chemical stimulation in health and after brain injury. Neurogastroenterology & Motility, 15(1), 69-77.
Hamer, P. W., McGeachie, J. M., Davies, M. J., & Grounds, M. D. (2001). Evans Blue Dye as an in vivo marker of myofibre damage: optimising parameters for detecting initial myofibre membrane permeability. Journal of Anatomy, 200(1), 69-79.
Hara, K., Tohara, H., Wada, S., Iida, T., Ueda, K., & Ansai, T. (2013). Jaw-opening force test to screen for dysphagia: Preliminary results. Arch Phys Med Rehabil. doi: 10.1016/j.apmr.2013.09.005

Hart, T., Tsaousides, T., Zanca, J. M., Whyte, J., Packel, A., Ferraro, M., & Dijkers, M. P. (2014). Toward a theory-driven classification of rehabilitation treatments. Archives of Physical Medicine & Rehabilitation, 95(1 Suppl), S33-44.e32. doi: http://dx.doi.org/10.1016/j.apmr.2013.05.032
Heffner, J. E., & Zamora, C. A. (1990). Clinical predictors of prolonged translaryngeal intubation in patients with the adult respiratory distress syndrome. Chest, 97(2), 447-452.
Hewitt, A., Hind, J. A., Kays, S. A., Nicosia, M. A., Doyle, J., Tompkins, W., . . . Robbins, J. A. (2008). Standardized instrument for lingual pressure measurement. Dysphagia, 23(1), 16-25.
Higgins, D. M. (1997). Dysphagia in the patient with tracheostomy: Six cases of inappropriate cuff deflation or removal. Heart & Lung: Journal of Acute & Critical Care, 26(3), 215-220.
Holevar, M., Dunham, M., Clancy, T. V., Como, J. J., Ebert, J. B., Griffen, M. M., . . . Tisherman, S. A. (2008, 8/10/28/). Practice management guidelines for the timing of tracheostomy. from http://www.east.org/Portal/Default.aspx?tabid=57
http://www.east.org/tpg/trachtiming.pdf Hwang, C. H., Choi, K. H., Ko, Y. S., & Leem, C. M. (2007). Pre-emptive swallowing stimulation in long-
term intubated patients. Clinical Rehabilitation, 21(1), 41-46. Jayasekeran, V., Rothwell, J., & Hamdy, S. (2011). Non-invasive magnetic stimulation of the human
cerebellum facilitates cortico-bulbar projections in the swallowing motor system. Neurogastroenterol Motil, 23(9), 831-e341. doi: 10.1111/j.1365-2982.2011.01747.x
Jayasekeran, V., Singh, S., Tyrrell, P., Michou, E., Jefferson, S., Mistry, S., . . . Hamdy, S. (2010). Adjunctive functional pharyngeal electrical stimulation reverses swallowing disability after brain lesions. Gastroenterology, 138(5), 1737-1746. doi: 10.1053/j.gastro.2010.01.052
Kang, J. Y., Choi, K. H., Yun, G. J., Kim, M. Y., & Ryu, J. S. Does removal of tracheostomy affect dysphagia? A kinematic analysis. Dysphagia, 27(4), 498-503.
Kays, S., & Robbins, J. (2006). Effects of sensorimotor exercise on swallowing outcomes relative to age and age-related disease. Seminars in Speech & Language, 27(4), 245-259.
Lan, Y., Ohkubo, M., Berretin-Felix, G., Sia, I., Carnaby-Mann, G. D., & Crary, M. A. (2012). Normalization of temporal aspects of swallowing physiology after the McNeill dysphagia therapy program. Annals of Otology, Rhinology & Laryngology, 121(8), 525-532.
Leslie, P., Drinnan, M. J., Ford, G. A., & Wilson, J. A. (2002). Resting respiration in dysphagic patients following acute stroke. Dysphagia, 17(3), 208-213.
Leslie, P., Drinnan, M. J., Ford, G. A., & Wilson, J. A. (2005). Swallow respiratory patterns and aging: presbyphagia or dysphagia? Journals of Gerontology Series A-Biological Sciences & Medical Sciences, 60(3), 391-395.
LoCicero, J. (1984). Tracheo-carotid artery erosion following endotracheal intubation. J Trauma, 24, 907 - 909.
Logemann, J. A., Pauloski, B. R., & Colangelo, L. (1998). Light digital occlusion of the tracheostomy tube: a pilot study of effects on aspiration and biomechanics of the swallow. Head & Neck., 20(1), 52-57.
Lucarelli, M. R., Shirk, M. B., Julian, M. W., & Crouser, E. D. (2004). Toxicity of food drug and cosmetic blue no. 1 dye in critically ill patients. Chest, 125(2), 793-795.
Malandraki, G. A., Johnson, S., & Robbins, J. (2011). Functional MRI of swallowing: From neurophysiology to neuroplasticity. Head & Neck, 33(S1), S14-S20. doi: 10.1002/hed.21903
Maloney, J. P., Halbower, A. C., Fouty, B. F., Fagan, K. A., Balasubramaniam, V., Pike, A. W., . . . Moss, M. (2000). Systemic absorption of food dye in patients with sepsis. New England Journal of Medicine, 343(14), 1047-1048.
Mandoe, H., Nikolajsen, L., Lintrup, U., Jepsen, D., & Molgaard, J. (1992). Sore throat after endotracheal intubation. Anesth Analg, 74, 897 - 900.
Muz, J., Mathog, R. H., Nelson, R., & Jones, L. A., Jr. (1989). Aspiration in patients with head and neck cancer and tracheostomy. American Journal of Otolaryngology, 10(4), 282-286.
Myers, E. M. M. D. (1982). Hypopharyngeal perforation: a complication of endotracheal intubation. Laryngoscope, 92(5), 583-585.
Nordin, U., Lindholm, C., & Wolgast, M. (1977). Blood flow in the rabbit tracheal mucosa under normal conditions and under the influence of tracheal intubation. Acta Anaesthesiol Scand, 21, 81 - 94.
Nseir, S., Di Pompeo, C., Jozefowicz, E., Cavestri, B., Brisson, H., Nyunga, M., . . . Durocher, A. (2007). Relationship between tracheotomy and ventilator-associated pneumonia: a case control study. European Respiratory Journal, 30(2), 314-320.
O'Neil-Pirozzi, T. M., Lisiecki, D. J., Momose, K. J., Connors, J. J., & Milliner, M. P. (2003). Simultaneous modified barium swallow and blue dye tests: A determination of the accuracy of blue dye test aspiration findings. Dysphagia, 18(1), 32-38.
Oberwaldner, B., & Eber, E. (2006). Tracheostomy care in the home. Paediatric Respiratory Reviews, 7(3), 185-190.
Pelletier, C. A., & Lawless, H. T. (2003). Effect of citric acid and citric acid-sucrose mixtures on swallowing in neurogenic oropharyngeal dysphagia. Dysphagia, 18(4), 231-241.
Power, M. L., Fraser, C. H., Hobson, A., Singh, S., Tyrrell, P., Nicholson, D. A., . . . Hamdy, S. (2006). Evaluating oral stimulation as a treatment for dysphagia after stroke. Dysphagia, 21(1), 49-55.
Randestad, A. M. D., Lindholm, C.-E. M. D. P., & Fabian, P. M. D. (2000). Dimensions of the cricoid cartilage and the trachea. Laryngoscope, 110(11), 1957-1961.
Robbins, J., Gangnon, R. E., Theis, S. M., Kays, S. A., Hewitt, A. L., & Hind, J. A. (2005). The effects of lingual exercise on swallowing in older adults. Journal of the American Geriatrics Society, 53(9), 1483-1489.
Robbins, J., Kays, S. A., Gangnon, R. E., Hind, J. A., Hewitt, A. L., Gentry, L. R., & Taylor, A. J. (2007). The effects of lingual exercise in stroke patients with dysphagia. Archives of Physical Medicine & Rehabilitation, 88(2), 150.
Sandhu, R. S., Pasquale, M. D., Miller, K., & Wasser, T. E. (2000). Measurement of endotracheal tube cuff leak to predict postextubation stridor and need for reintubation. Journal of the American College of Surgeons., 190(6), 682-687.
Santos, P. M., Afrassiabi, A., & Weymuller, E. A., Jr. (1994). Risk factors associated with prolonged intubation and laryngeal injury. Otolaryngology - Head & Neck Surgery, 111(4), 453-459.
Sapienza, C. M., Troche, M., Pitts, T., & Davenport, P. W. (2011). Respiratory strength training: concept and intervention outcomes. Seminars in Speech & Language, 32(1), 21-30.
Sapienza, C. M., & Wheeler, K. (2006). Respiratory muscle strength training: functional outcomes versus plasticity. Seminars in Speech & Language, 27(4), 236-244.
Scalabrino, N., Crespi, L., Bosco, M., Troisi, E., Vezzaro, G., Baravelli, M., . . . Anza, C. [Diagnosis and management of dysphagia in patients with tracheostomy tube after cardiac surgery: an early screening protocol]. Monaldi Archives for Chest Disease, 74(2), 70-75.
Shaker, R., Milbrath, M., Ren, J., Campbell, B., Toohill, R., & Hogan, W. (1995). Deglutitive aspiration in patients with tracheostomy: effect of tracheostomy on the duration of vocal cord closure. Gastroenterology, 108(5), 1357-1360.
Sharma, O. P., Oswanski, M. F., Singer, D., Buckley, B., Courtright, B., Raj, S. S., . . . Gandaio, A. (2007). Swallowing disorders in trauma patients: impact of tracheostomy. American Surgeon, 73(11), 1117-1121.
Skoretz, S. A., Flowers, H. L., & Martino, R. (2010). The incidence of dysphagia following endotracheal intubation: a systematic review. Chest, 137(3), 665-673.
Suiter, D. M., McCullough, G. H., & Powell, P. W. (2003). Effects of cuff deflation and one-way tracheostomy speaking valve placement on swallow physiology. Dysphagia., 18(4), 284-292.
Tadié, J.-M., Behm, E., Lecuyer, L., Benhmamed, R., Hans, S., Brasnu, D., . . . Guérot, E. (2010). Post-intubation laryngeal injuries and extubation failure: a fiberoptic endoscopic study. Intensive Care Medicine, 36(6), 991-998. doi: 10.1007/s00134-010-1847-z
Terzi, N., Prigent, H., Lejaille, M., Falaize, L., Annane, D., Orlikowski, D., & Lofaso, F. Impact of tracheostomy on swallowing performance in Duchenne muscular dystrophy. Neuromuscular Disorders, 20(8), 493-498.
Thompson-Henry, S., & Braddock, B. (1995). The modified Evan's blue dye procedure fails to detect aspiration in the tracheostomized patient: five case reports. Dysphagia, 10(3), 172-174.
Tobin, A. E., & Santamaria, J. D. (2008). An intensivist-led tracheostomy review team is associated with shorter decannulation time and length of stay: a prospective cohort study. Critical Care, 12(2), R48.
Wada, S., Tohara, H., Iida, T., Inoue, M., Sato, M., & Ueda, K. (2012). Jaw-opening exercise for insufficient opening of upper esophageal sphincter. Arch Phys Med Rehabil, 93(11), 1995-1999. doi: 10.1016/j.apmr.2012.04.025
Wagner, D. R., Elmore, M. F., & Knoll, D. M. (1994). Bacterial contamination of enteral feeding reservoirs. Journal of Parenteral & Enteral Nutrition, 18(6), 562-Dec.
Ward, J. J. (2013). High-flow oxygen administration by nasal cannula for adult and perinatal patients. Respiratory Care, 58, 98+.
Weymuller, E. A. (1988). Laryngeal injury from prolonged endotracheal intubation. Laryngoscope, 98(8)(Supplement), 14.
Whyte, J., Dijkers, M. P., Hart, T., Zanca, J. M., Packel, A., Ferraro, M., & Tsaousides, T. (2014). Development of a theory-driven rehabilitation treatment taxonomy: conceptual issues. Archives of Physical Medicine & Rehabilitation, 95(1 Suppl), S24-32.e22. doi: http://dx.doi.org/10.1016/j.apmr.2013.05.034
Winklmaier, U., Wust, K., Schiller, S., & Wallner, F. (2006). Leakage of fluid in different types of tracheal tubes. Dysphagia, 21(4), 237-242.