growth in children after bone marrow transplantation for advanced neuroblastoma compared with growth...
TRANSCRIPT

Growth in children after bone marrow transplantation for advanced neuroblastoma compared with growth after transplantation for leukemia or aplastic anemia
Steven M. Willi, MD, Kenneth Cooke , MD, Joel Go ldwe in , MD, Charles S. August , MD, Jerrold S. Olshan, MD, and Thomas Moshang, Jr., MD
From the Divisions of Endocrinology and Oncology, Children's Hospital of Philadelphia and De- partment of Pediatrics, University of Pennsylvania School of Medicine, and the Department of Radiation Oncology, Hospital of the University of Pennsylvania and Department of Medicine, University of Pennsylvania School of Medicine, Philadelphia
The l inear growth of 26 children with progressive and advanced neuroblastoma treated with high-dose chemotherapy, total body irradiation, and bone marrow transplantat ion between 1978 and 1988 at the Children's Hospital of Philadelphia was compared with the growth of 33 chi ldren who had transplants for leukemia and of 12 who had transplants for aplast ic anemia. The mean growth veloci ty, expressed as a standard deviat ion score, for the chi ldren who underwent bone marrow transplantat ion for neuroblastoma was -2.83. This was signif icantly (p <0.005) less than the standard deviat ion scores for chi ldren with transplants for acute lymphoblast ic leukemia, acute nonlymphocyt ic leukemia, and aplast ic anemia, which were -0.98, -0.07, and -1.05, respectively. A 6-year fol low-up study of 32 long-term survivors of cancer revealed that the 11 patients with neu- roblastoma cont inued to grow poorly, whereas a comparison group of 21 survi- vors of bone marrow transplantation for leukemia had essentially normal growth 2 years after the procedure. Major therapeut ic di f ferences between the two groups inc luded the doses of local radiotherapy and the type and number of cy totox ic agents used. In comparison with the relat ively mild growth-inhibit ing effects of preparat ive regimens for leukemia and aplast ic anemia, the very in- tensive preparat ive regimens used in patients with neuroblastoma have signif- icant negat ive effects on growth. (J PEDIATR 1992;120:726-32)
Supported by U.S. Public Health Service grant RR 00240, from the General Clinical Research Center Program of the Division of Re- search Resources, National Institutes of Health, Bethesda, Mary- land, and by the Tomorrow Fund of the Children's Hospital of Philadelphia. Presented in part at the 59th Annual Meeting of the Society for Pediatric Research, Washington, D.C., May 2, 1989.
Submitted for publication Aug. 7, 1991; accepted Nov. 14, 1991.
Reprint requests: Thomas Noshang, Jr., MD, Division of Endocri- nology/Diabetes, Child~:en'~ Hospital of Philadelphia, 34th St. and Civic Center Blvd., Philadelphia, PA 19104. 9/2o/3so54
Since the advent of bone marrow transplantation as a treatment for various neoplastic, hematologic, immuno- logic, and metabolic disorders, many children who would have died are now surviving for long periods. Preparative treatment for BMT involves the administration of suprale- thai doses of both chemotherapeutic agents and radiation. Although curing the underlying disease is the primary goal of BMT, the short- and long-term effects of these treatments are also important. One important issue in the assessment of treatment outc6me in pediatric patients is linear growth. Previous studies of growth after BMT 13 have examined
726

Volume 120 Growth after bone marrow transplantation 727 Number 5
I ALL Acute lymphoblastic leukemia ANLL Acute nonlymphocytic leukemia BMT Bone marrow transplantation GVHD Graft-versus-host disease SDS Standard deviation score TBI Total body irradiation
height rather than growth velocity, and the patients re- ported on had transplants for aplastic anemia or acute leu- kemia. Preconditioning for BMT is more intensive for chil- dren with neuroblastoma than for patients with leukemia or aplastic anemia. Although growth is moderately attenuated in patients with leukemia after BMT, the effect of BMT on growth in those with neuroblastoma has not been evaluated. Our study focused on a group of children who survived au- tologous and allogeneic BMT for neuroblastoma and com- pared their growth with that of children who had BMT for aplastic anemia or leukemia.
M E T H O D S
Patients. Between September 1978 and January 1988, a total of 41 children underwent BMT for advanced neuro- blastoma at the Children's Hospital of Philadelphia. Of these, 26 patients (14 boys) survived for more than 6 months and could be studied. Twenty patients had stage IV disease and six had progressive stage III disease. The median age at transplant was 4.8 years (range 2.2 to 13.3 years). For- ty-five patients (30 boys) who survived 6 months after BMT for aplastic anemia or leukemia were similarly studied. These patients included 12 with aplastic anemia, 16 with acute lymphoblastic leukemia, and 17 with acute nonlym- phocytic leukemia. Their median age was 10.1 years (range 2.2 to 18.0 years).
The long-term effect of BMT on longitudinal growth in patients with cancer was evaluated in children surviving at least 2 years after BMT; none of these patients incurred re- lapse of their primary disease. This long-term study of sur- vivors compares, for a 6-year period after BMT, the annual growth rates of 11 children (6 boys) with neuroblastoma (median age 4.6 years, range 2.2 to 9.4 years) with those of 22 children (13 boys) with leukemia (median age 8.3 years, range 2.2 to 15.0 years).
Treatment protocols. Patients with neuroblastoma were treated with chemotherapy, surgery, and local x-ray ther- apy to the tumor bed immediately before BMT; 17 had ad- ditional local radiotherapy to distant sites of active disease as part of their pretransplant Conditioning regimen. Of these patients, 10 had local irradiation to the cranium in doses between 400 and 1000 cGy. in preparation for BMT, patients received melphalan, 210 mg/m 2, and conventional doses of other agents, including doxorubicin, 45 mg/m z
given twice, teniposide, 180 mg/m 2 given twice, and cis- platin, 100 mg/m 2. They also received 999 or 1200 cGy to- tal body riradiation, as either 333 cGy for 3 days or 200 cGy twice a day for 3 days. Seven patients received marrow from human leukocyte antigen-matched siblings, and 19 re- ceived frozen, thawed, autologous marrow. 4, 5
Patients with ALL had transplants during the second or subsequent remission and therefore had received prolonged antileukemia therapy (including corticosteroids) before consideration for BMT. Of the 16 patients with ALL, 13 had cranial irradiation in doses from 600 to 2400 cGy (mean dosage 1851 eGy). Children with ANLL had transplants during the first remission and had no cranial irradiation be- fore BMT. Preparative regimen s for BMT in patients with leukemia evolved during a period of years from protocols employing cyclophosphamide, 120 mg/kg (total dosage), and TBI in doses ranging from 800 cGy (single fraction) to 333 cGy given three times (total dosage 999 cGy), and from 160 cGy given eight times (total dosage 1280 cGy) to 200 cGy give n six times (total dosage 1200 eGy). 6 Since 1985, all children with acute leukemia, whose growth is reported herein, have been treated with cytarabine, 36 gm/m 2, and 1200 cGy fractionated TBI. 7 Seventeen patients with leu- kemia were exposed to one of the two TBI regimens used to treat neuroblastoma; 10 patients were given a single frac- tion of 800 cGy. The third fractionation regimen (160 cGy twice a day for 4 days) was used in the treatment of the re- maining six patients.
The i2 children with aplastic anemia were prepared for BMT either with cyclophosphamide, 200 mg/kg (total dos- age) (three patients), or with cyclophosphamide (same dose) and 300 cGy TBI (nine patients). 8 The patients with aplastic anemia were excluded from the analysis of long- term effects of BMT on growth because they received little or no TBI. All of the children who had BMT for leukemia and aplastic anemia received marrow from family members with identical human leukocyte antigens.
All children receiving allogeneic transplants were given methotrexate at regular intervals for 100 days after BMT in an attempt to prevent graft-versus-host disease. 9 During the study period, acute GVHD was treated with intrave- nously administered methylprednisolone t~ and anti-thymo- cyte globulin and with orally administered prednisone. Chronic GVHD was treated with prednisone given daily or every other day.
Research protocol. All patients who underwent BMT at this institution were thereafter admitted at regular intervals to the clinical research center under a research protocol. Patients were admitted immediately before BMT, at 6 months and 1 year after BMT, and at yearly intervals thereafter. Patients underwent physical examination and routine blood testing for the presence of disease, including
7 2 8 Willi et al. The Journal of Pediatrics May 1992
qJ ~
ro o .
o x_
qJ ..s
E -a
z
1 0 -
8
6 -
4 -
2 -
0
1 6 -
1 2 -
8 -
4 -
-8 -7 -6 -5 -4
A
I I T I I I I I
-3 -2 -1 0 1 2 3 4 5 6
-6 -5 -4 -3 -2
B
! I I I l I l [ I
-8 -7 -1 0 1 2 3 4 5 6
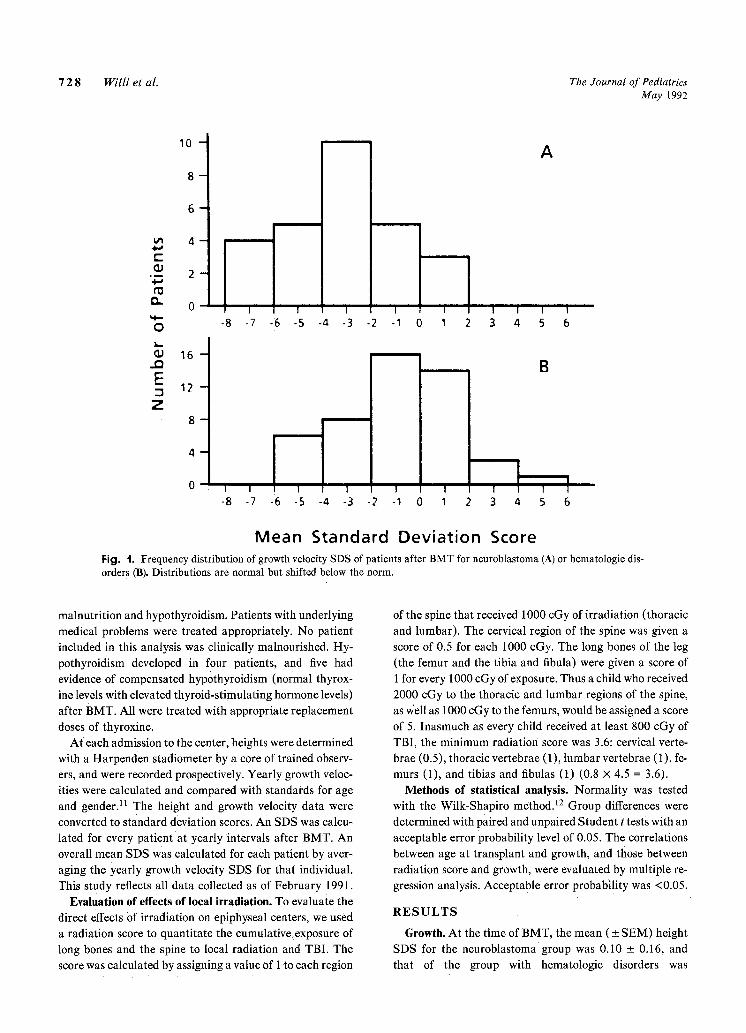
Mean Standard Deviation Score Fig. 1. Frequency distribution of growth velocity SDS of patients after BMT for ncuroblastoma (A) or hematologic dis- orders (B). Distributions are normal but shifted below the norm.
malnutrition and hypothyroidism. Patients with underlying medical problems were treated appropriately. No patient included in this analysis was clinically malnourished. Hy- pothyroidism developed in four patients, and five had evidence of compensated hypothyroidism (normal thyrox- ine levels with elevated thyroid-stimulating hormone levels) after BMT. All were treated with appropriate replacement
doses of thyroxine. At each admission to the center, heights were determined
with a Harpenden stadiometer by a core of trained observ- ers, and were recorded prospectively. Yearly growth veloc- ities were calculated and compared with standards for age and gender) 1 The height and growth velocity data were converted to standard deviation scores. An SDS was calcu- lated for every pat ientat yearly intervals after BMT. An overall mean SDS was calculated for each patient by aver- aging the yearly growth velocity SDS for that individual. This study reflects all data collected as of February 1991.
Evaluation of effects of local irradiation. To evaluate the direct effects Of irradiation on epiphyseal centers, we used a radiation score to quantitate the cumulative exposure of long bones and the spine to local radiation and TBI. The score was calculated by assigning a Value of 1 to each region
of the spine that received 1000 cGy of irradiation (thoracic and lumbar). The cervical region of the spine was given a
score of 0.5 for each 1000 cGy. The long bones of the leg (the femur and the tibia and fibula) were given a score of 1 for every 1000 cGy of exposure. Thus a child who received 2000 cGy to the thoracic and lumbar regions of the spine, as v~ell as 1000 cGy to the femurs, would be assigned a score of 5. Inasmuch as every child received at least 800 cGy of TBI, the minimum radiation score was 3.6: cervical verte- brae (0.5), thoracic vertebrae (1), lumbar vertebrae (1), fe- murs (1), and tibias and fibulas (1) (0.8 x 4.5 = 3.6)i
Methods of statistical analysis. Normality was tested with the Wilk-Shapiro method. 12 Group differences were
determined with paired and unpaired Student t tests with an acceptable error probability level of 0.05. The Correlations between age at transplant and growth, and those between radiation score and growth, were evaluated by multiple re- gression analysis. Acceptable error probability was <0.05.
R E S U L T S
Growth. At the time of BMT, the mean ( _+ SEM) height SDS for the neuroblastoma group was 0.10 + 0.16, and that of the group with hematologic disorders was

Volume 120 Growth after bone marrow transplantation 729 Number 5
tu 3 rr" O (J 2
c5 1
0
O O -1 i i i
- 2 "1-
0
~ - 4 0
0
LEUKE v M ~ 2 2 • *
3 2 2 ~ / ~ 11 ~ 7 6 ~
NEUROBLASTOMA ~- I I I I ! I
1 2 3 4 5 6
YEARS AFTER TRANSPLANTATION Fig. 2. Average growth velocity SDS by years since BMT. Long-term survivors with neuroblastoma (0) are compared with patients with hematologic disorders (11). Numbers correspond to number of patients measured at each interval. (As- terisk: p <0.05.)
0.34 + 0.20. After BMT, however, growth velocity was profoundly affected in the patients with neuroblastoma. A frequency analysis (Fig. 1, A) of overall SDSs for growth velocity in these 26 patients approximated a normal distri- bution (Wilk-Shapiro test statistic = 0.9789). However, this distribution was shifted nearly 3 SD below the normal mean. The comparison group of 45 patients with hemato- logic disorders also demonstrated a frequency of SDSs with a normal distribution, but the downward shift in distribu- tion was only 1 SD (Fig. 1, B).
The mean (+ SEM) growth velocity SDS for the neuro- blastoma group was -2.83 + 0.43, significantly less than that of each of the others: aplastic anemia -1.05 + 0.86, ANLL -0.07 _+ 0.48, and ALL -0.98 + 0.58. When growth velocities for the three subgroups with hematologic disorders were analyzed, they did not differ significantly from one another or from the statistical norm. The overall mean growth velocity SDS for the group of patients with hematologic disorders was -0.66, significantly better than the growth velocity SDS for the patients with neuroblas- toma (p <0.005).
Eleven patients with neuroblastoma had disease-free survival times ranging from 2 to 10 years after BMT. No patient had a relapse occurring more than 20 months after BMT, so these patients were considered to have been "cured" of their disease. A similar group of 22 patients with leukemia were available for comparison. Figure 2 demon-
strates that growth velocity in the long-term survivors of neuroblastoma remained poor, even several years after BMT. In contrast, the annual growth velocities of th e long- term survivors of ALL and ANLL improved in each successive year after BMT and, in years 4 through 6, were greater than the normal mean. This finding suggests that some "catch-up" growth occurred in these patientsr Older, postpubertal children normally have low growth velocities, and there is a tendency for SDS to become normal with ad- vancing age. The pattern Of growth in long-term survivors of both neuroblastoma and the hematologic disorders was unchanged, however, even when measurements in patients older than 14 years of age were excluded (data analysis not shown).
Gender distribution and growth. The gender distribution of patients in the neuroblastoma group (14 male, 12 female) differed from that of the hematologic group (30 male, 15 female), mostly because a higher proportion of boys with ALL underwent BMT after relapse. The SDS did not dif- fer significantly between boys and girls.
Age distribution and growth. The patients with neuro- blastoma were significantly younger than those who under- went BMT for hematologic malignancies (p <0.001 by un- matched t test). In a regression analysis of our long-term survivors (Fig. 3), a statistically significant increase in growth velocity was noted with increasing age at the time of BMT. This finding indicates that age at time of BMT in-

7 3 0 Wil l i et al. The Journal o f Pediatrics May 1992
4 R = 0 . 4 7 �9
p < 0.02 �9 2
A �9 �9 O �9 �9 �9
�9 �9 � 9 1 4 9 �9
a - 2 � 9 �9
- 4 �9 �9 �9
- 6 �9
1 | ~ 1 1- [ I i
2 4 6 8 10 12 14 16
l
18
AGE AT TRANSPLANTATION Fig. 3. Linear regression analysis of growth after BMT versus age at time of procedure. Each individual long-term sur- vivor is represented by dark triangle. Regression is statistically significant (p = 0.002), but R 2 value (0.22) suggests rel- atively weak correlation.
fluenced subsequent growth. However, the low R 2 value (0.22) in this regression analysis indicates that this influ- ence was relatively weak.
To examine this relationship more fully, we performed an age-matched analysis of the patient groups by excluding children more than 6 years of age at the time of BMT. This exclusion was chosen because it yielded two populations of patients who had similar age distributions. The median ages at BMT in the resulting neuroblastoma (n = 16) and non- neuroblastoma (n = 7) patient groups were similar at 3.7 and 3.5 years, respectively. The mean ages at BMT in the two groups were identical (3.9 years), as were the ranges in age (2.2 to 6.0 years). The mean SDS for the patients with neuroblastoma (-2:76) was significantly lower (p <0.01) than for the nonneuroblastoma group (-0.65). The differ- ence between growth velocities found in patients with neu- roblastoma versus those with hematologic malignancies was nearly as great in age-matched samples as they were in the groups overall.
Irradiation and growth. In light of the potential negative effects of irradiation on growth, cumulative doses of radi- ation exposure to the cranium and epiphyseal centers were examined as they related to growth attenuation. All patients included in the analysis (i.e., not those with aplastic anemia) were treated with between 800 and 1280 cGy of TBI. Very few of our patients, with the exception of those with ALL, received cumulative doses of cranial radiation previously suggested (>2400 cGy) 13 to cause growth hormone deft-
ciency in a large percentage of patients. Moreover, a signif- icant number of patients within our neuroblastoma group who received relatively low cumulative doses of cranial ra- diation (1200 cGy or less) grew poorly. Although growth hormone function needs to be evaluated in the BMT patients, we could not identify a threshold value (for cumu- lative cranial irradiation) above which a statistically signif- icant adverse effect on growth velocity could be established.
The relationship between irradiation of epiphyseal growth plates (based on the radiation score described above) and growth in the long-term survivors of cancer is illustrated in Fig. 4. Analysis of the data from survivors of neuroblastoma and leukemia together demonstrated this relationship to be statistically significant (p <0.01). However, there was no correlation between epiphyseal irradiation and subsequent growth in the neuroblastoma group, perhaps because the growth failure in these patients was so uniformly profound. A multiple regression analysis, including the age of patients at BMT, did not alter these results. Thus the more severe growth disturbance found in the patients with neuroblas- toma cannot be attributed to greater exposure of growth plates to radiation alone.
D I S C U S S I O N
The first detailed study of growth attenuation in patients treated for neoplastic disorders was reported in 1975.14 In that same year, Shalet et al. 13 demonstrated a high inci- dence of growth hormone deficiency and growth failure

Volume 120 Growth after bone marrow transplantat ion 731 Number 5
UJ 4
0
O0 2
Z 0
0
LLI a - 2 r~ r
a - 4 Z
I -- r - 6
�9 ~ �9 �9 "l,-,,... L m
U ~ �9 �9
�9 ,o
I I I I I
3 4 5 6 7
R A D I A T I O N S C O R E
Fig. 4. Growth related to radiation in long-term survivors. Each patient with neuroblastoma is represented by dark cir- cle; each patient with leukemia is represented by dark square. Combination analysis of all children with cancer yielded statistically significant regression (p <0.005). This relationship is shown by dashed line (r = -0.53). However, regression analysis of only patients with neuroblastoma, represented by solid line, showed no significant difference (r = -0.33; p = 0.27).
among patients treated with high doses of cranial irradia- tion. Much effort has been directed toward finding dosage regimens that are curative without sacrificing growth or hormonal function. Diminished growth hormone secretion occurs in the majority of patients treated with cranial irra- diation in the range of 2500 to 3000 cGy 15 and has been
demonstrated in patients treated with as little as 1800 to 2400 cGy. 16 Previous studies in patients after BMT have
demonstrated subnormal growth in those treated with lower cumulative doses of cranial irradiation. 13 Our findings
confirm these reports in a group of patients given radio- therapy for neuroblastoma, with total doses between 999 and 2200 cGy (mean = 1396 cGy). In fact, their growth velocities were shifted almost 3 SD below the norm, but with a normal distribution curve. We found a similar but less se- vere effect on the patients treated for hematologic malig- nancies or aplastic anemia. There was no correlation with gender distribution, and the correlation with age was rela- tively minor. Closer analysis of the effect of age showed that patients with neuroblastoma grew significantly slower than did age-matched patients with leukemia or aplastic anemia.
There was a significant correlation between epiphyseal irradiation and growth velocity when all survivors of BMT for cancer were included in the analysis. This finding con- firms a previous report that relates loss of adult stature to the dose and location of radiotherapy received by patients with cancer. 17 However, the growth attenuation was so
uniformly profound in survivors of BMT who had had neu- roblastoma that no relationship between growth and cranial or epiphyseal plate irradiation could be established.
There is no convincing evidence that cytotoxic drugs alone impair anterior pituitary function 18 or long-term
growth. However, the number of reports of deleterious ef- fects of cytotoxic drugs on growth, in combination with ra- diation, is increasing. 19-21 One striking difference between
our two groups, in addition to local radiation doses, was the number and dosage of chemotherapeutic agents employed in preconditioning. The strong possibility exists, therefore, that the multiple agents employed in close temporal prox- imity to TBI combined to disturb growth in the children who
had transplants for neuroblastoma. Chronic GVHD has been reported to contribute to poor
growth in patients who have undergone BMT.1, 3 This trend
was found in our patients with hematologic disorders as well, and perhaps accounts for the relatively low growth- velocity SDS in patients with aplastic anemia. Chronic GVHD cannot be implicated as a cause of the severe growth disturbance found in the patients with neuroblastoma because chronic GVHD developed in only one of seven pa- tients who received allogeneic marrow. Most patients with neuroblastoma received autologous marrow.
The incidence of thyroid dysfunction in this study (23.8%) agrees with findings previously reported with BMT.1 The highest incidence of thyroid abnormalities was

7 3 2 Willi et al. The Journal of Pediatrics May 1992
found among patients with neuroblastoma who had received
local radiation to the head or neck or both.
We conclude that in patients with neuroblastoma who
have survived BMT, growth is severely impaired. Their
young age at diagnosis and the substantial exposure of
growth plates to radiation no doubt contribute to the growth
disturbance found in these patients. However, in age-
matched samples, the growth of patients with neuroblas-
toma was significantly slower than that of children with he-
matologic malignancies. Furthermore, the lack of correla-
tion between radiation dosage and growth velocity in the
patients with neuroblastoma suggests that their severe
growth failure must be attributed to other, more significant
factors. The use of multiple chemotherapeutic agents, and
perhaps especially melphalan, in combination with radio-
therapy during preconditioning for B M T must be consid-
ered as one of these factors. An important and encouraging
finding is that the survivors of B M T for ALL, A N L L , and
aplastic anemia grow fairly well, appear to have "catch-up"
growth by the third posttransplant year, and subsequently
have normal growth velocities.
R E F E R E N C E S
1. Sanders JF, Pritchard S, Mahoney P, et al. Growth and devel- opment following bone marrow transplantation for leukemia. Blood 1986;68:1129-35.
2. Leiper AD, Stanhope R, Lau T, et al. The effect of total body irradiation and bone marrow transplantation during childhood and adolescence on growth and endocrine function. Br J Hae- matol 1987;67:419-26.
3. Bushhouse S, Ramsay N, Pescovitz OH, Kim T, Robinson LL. Growth in children following irradiation for bone marrow transplantation. Am J Pediatr Hematol/Oncol 1989;1 I:134- 40.
4. August CS, Serota FT, Koch PA, et al. Treatment of advanced neuroblastoma with supralethal chemotherapy, radiation and allogeneic or autologous marrow reconstitution. J Clin Oncol 1984;2:609-16.
5. August CS, Auble B. In: Dicke K, Spitzer G, Jagannath S, Evinger-Hodges M J, eds. Autologous bone marrow transplan- tation. Proceedings of the Fourth International Symposium, University of Texas-M.D. Anderson Cancer Center, 1989:567- 73.
6. Serota FT, Burkey ED, August CS, D'Angio GJ. Total body irradiation as preparation in the treatment of acute leukemia and aplastic anemia. Int J Radiat Oncol Biol Phys 1983; 9:1941-9.
7. Kamani N, Bayever E, August CS, Auble B, Goldwein JW, D'Angio GJ. Fractionated total body irradiation preceding high-dose cytosine arabinoside as a preparative regimen for bone marrow transplantation in children with acute leukemia: a pilot study from the Children's Hospital of Philadelphia [Abstract]. Blood 1990;7b:547a.
8. Bayever E, Champlin B, Ho W, et al. Comparison between bone marrow transplantation and antithymocyte globulin in treatment of young patients with severe aplastic anemia. J PE- D I A T R 1984;105:920-5.
9. Storb R, Thomas ED, Buckner CD, et al. Allogeneic marrow grafting for the treatment of aplastic anemia. Blood 1974; 43:157-80.
10. August C, Serota F, Koch P, Githens J. Treatment of acute graft-versus-host reactions with high dose methylprednisolone [Abstract]. Blood 1981;58(suppl):169a.
11. Tanner JM, Davies P. Clinical longitudinal standards for height and height velocity for North American children. J PE- OIATR 1985;107:317-29.
12. Shapiro SS, Wilk MB. An analysis of variance test for normality. Biometrica 1965;52(3&4):591-611.
13. Shalet S, Beardwell CG, Morris-Jones PH, et al. Pituitary function after treatment of intracranial tumors in children. Lancet 1975;2:104-7.
14. Onoyama Y, Abe M, Takahashi M, et al. Radiation therapy of brain tumors in children. Radiology 1975;115:687-93.
15. Shalet SM. Irradiation-induced growth failure. Clin Endo- crinol Metab 1986;15:591-606.
16. Costin G. Effects of low-dose cranial radiation on growth hor- mone secretory dynamics and hypothalamic-pituitary func- tion. Am J Dis Child 1988;142:847-52.
17. Silber J, Littman P, Meadows AT. Stature loss following skel- etal irradiation for childhood cancer. J Clin Onco11990;8:304- 12.
18. Shalet SM. Disorders of the endocrine system due to radiation and cytotoxic chemotherapy. Clin Endocrino11983;19:637-59.
19. Clayton PE, Shalet SM, Morris-Jones PH, Price DA. Growth in children treated for acute lymphoblastic leukemia. Lancet 1988;1:460-2.
20.. Kirk JA, Raghupathy P, Stevens MM, et al. Growth failure and growth hormone deficiency after treatment for acute lym- phoblastic leukemia. Lancet 1987;1:190-3.
21. Olshan JS, Gubernick J, Packer RJ, et al. The effects of ad- juvant chemotherapy on growth in children surviving medul- loblastoma. Cancer (in press).