gold clasification antonio anzueto md professor medicine university of texas
TRANSCRIPT

GOLD
Clasification
Antonio Anzueto MDProfessor MedicineUniversity of Texas

Faculty Disclosures
Non-commercial, non-governmental interests relevant to my presentation :Member of the ATS/ERS Task force on COPD and COPD Exacerbations, Current
Member of Scientific Committee of GOLD, Current
Personal financial interests in commercial entities that are relevant to my presentation:
Boehringer Ingelheim: consultant: advisory board, CurrentGlaxoSmithKline: consultant, advisory board, Research Grant to the
University, CurrentChiesi: consultant, advisory board, Past
Bayer-Schering Pharma: consultant, advisory board, CurrentDey Pharma: consultant, advisory board, Current
Forest laboratories: consultant, advisory board, Current

2000- Staging of COPD: GOLD Guidelines
I: Mild
II: Moderate
III: Severe
IV: Very Severe
•FEV1 80%• With or without
symptoms
•FEV1 50 - 79%• With or without
symptoms
•FEV1 30 - 49%• With or without
symptoms
•FEV1 <30%
• Or presence of chronic
respiratory failure or right heart
failure
Active reduction of risk factor(s); Influenza vaccinationAdd short-acting bronchodilator (when needed)
Add regular treatment with one or more long-acting bronchodilators (when needed); Add rehabilitation
Add ICS if repeated exacerbations
Add long-term oxygen if CRFConsider surgical treatments

Agusti A et al. Respiratory Research 11 (1):122-136, 2010

GOLD - Goal of COPD Management
Overall COPD Control
Current Control Future Risk
Symptoms
Activity
QoL
Lung function
Exacerbations
Progressionof the disease
Mortality
Medication adverse effects
achieving reducing
defined by defined by
GOLD 2011 www.goldcopd.org
Time for change
Preventative: Tackle the root cause
Approach: Fundamentally shift the
way we treat COPD
1
2

GOLD Assessment
Sev
erit
y o
f A
irfl
ow
O
bst
ruct
ion
Worse obstruction
More severe
Exa
cerb
atio
ns
Frequent exacerbations
DSevere ObstructionSevere Symptoms++ Exacerbations
High
High
High
Risk
Risk
Risk
Symptoms
CSevere ObstructionMinimal Symptoms++ Exacerbations
AMild-Mod
ObstructionMinimal SymptomsFew Exacerbations
BMild-Mod Obstruction
Severe SymptomsFew Exacerbations
GOLD Website. http://www.goldcopd.com. Updated December 2012

Do these groups
exist ?
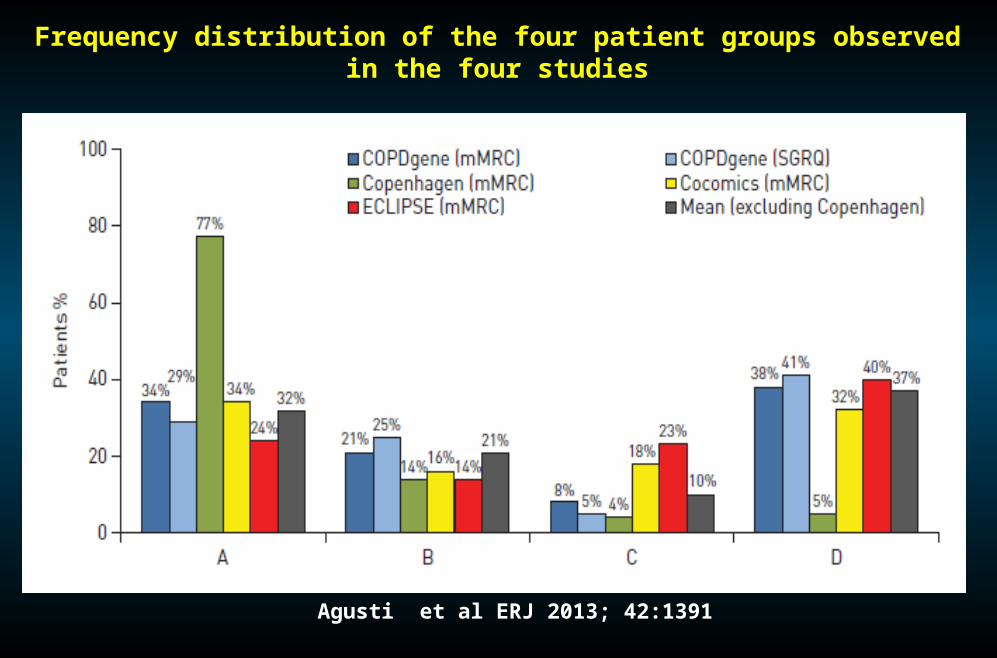
Frequency distribution of the four patient groups observed in the four studies
Agusti et al ERJ 2013; 42:1391

Distribution of COPD types
Johannessen et al. AJRCCM 2013; 188:51-59

GOLD Group Distribution
A B C D0
5
10
15
20
25
30
35
40
COPD CohortPrimary Care
% o
f S
ub
ject
s
GOLD Groups Agusti et al ERJ 2013; 42:1391Haughney et al ERJ 2014; 43:993

Jones et al. ERJ 2013; 42: 647-654
Comparison of CAT and MRC

Assess risk of
exacerbations
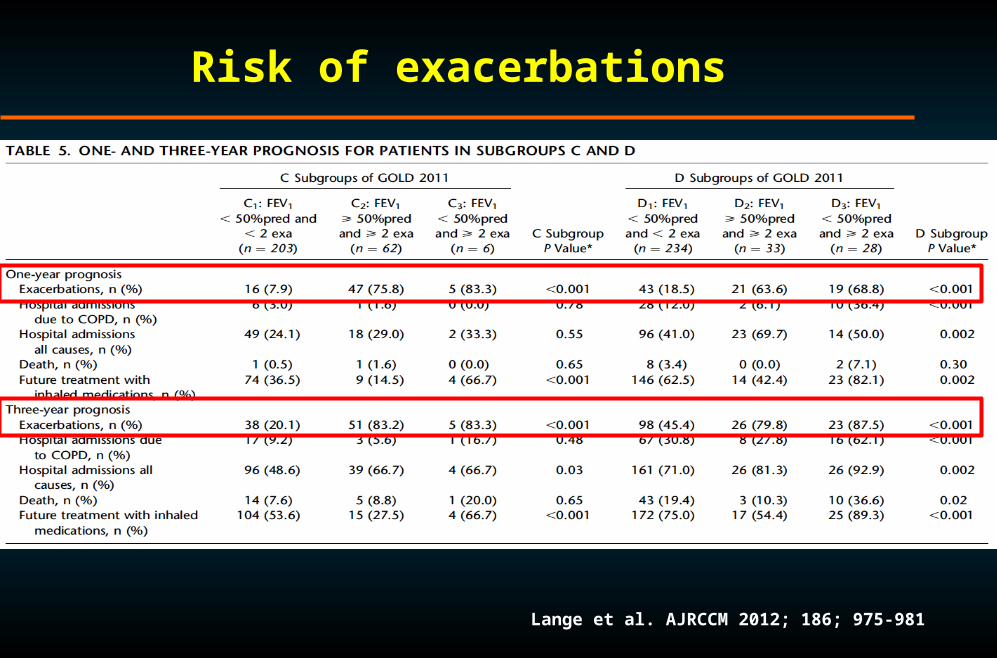
Risk of exacerbations
Lange et al. AJRCCM 2012; 186; 975-981

Hurst et al. NEJM 2010; 363: 1128-38
Risk of exacerbations

Han et al. Lancet Infect Dis 2013; 1: 43-50
GOLD classification

GOLD Risk Categories using SGRQ
Han et al Lancet Respiratory 2012

CT Scan Correlated: Emphysema
COPD gene database
A
D
B
C
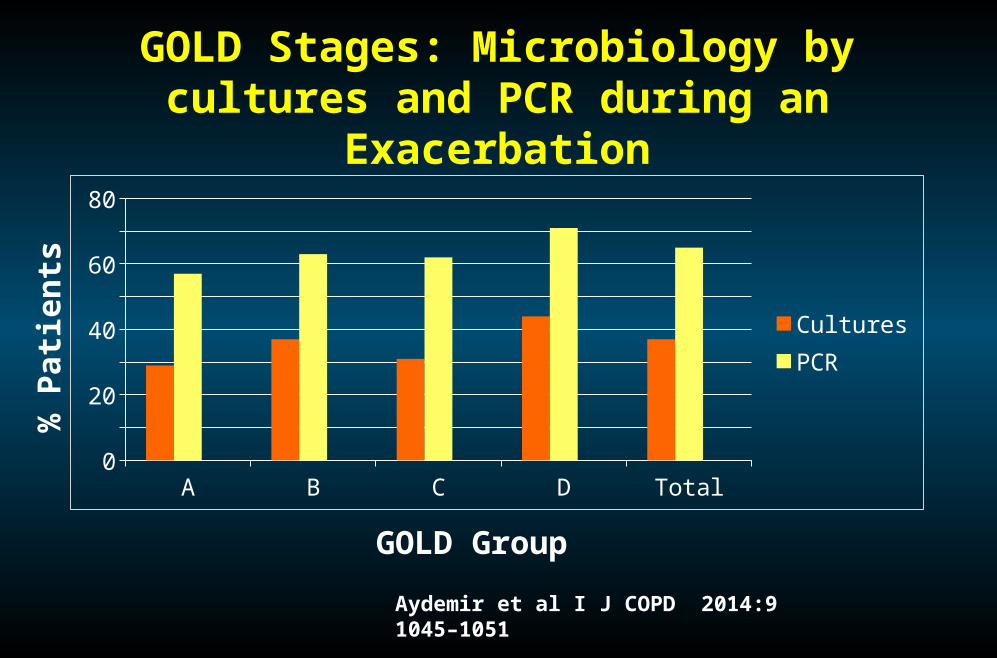
GOLD Stages: Microbiology by cultures and PCR during an Exacerbation
A B C D Total0
10
20
30
40
50
60
70
80
CulturesPCR
% P
atie
nts
GOLD Group
Aydemir et al I J COPD 2014:9 1045–1051

Prognostic
value
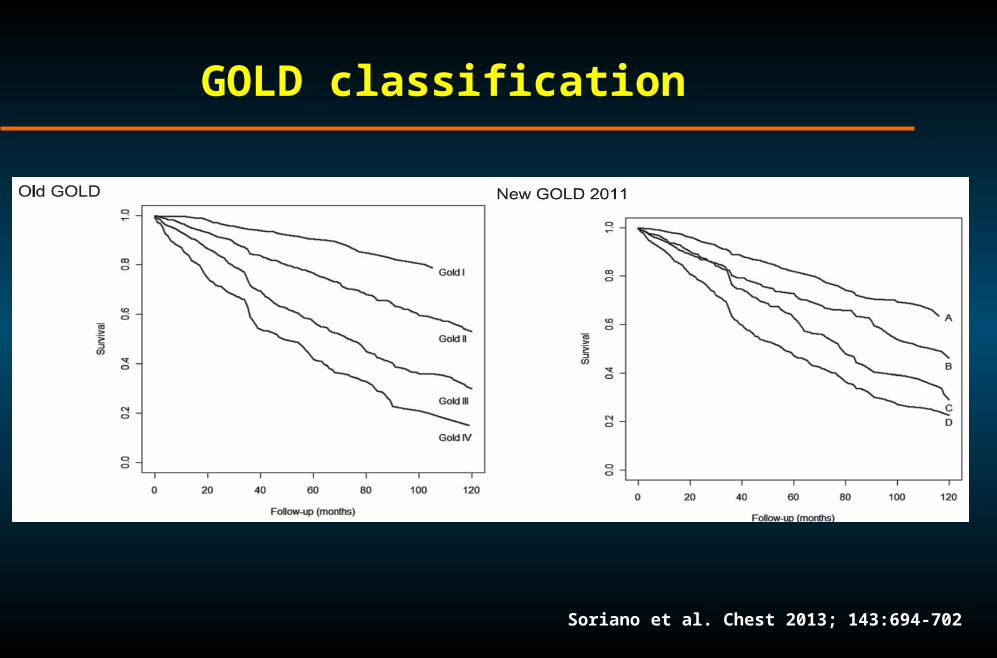
GOLD classification
Soriano et al. Chest 2013; 143:694-702
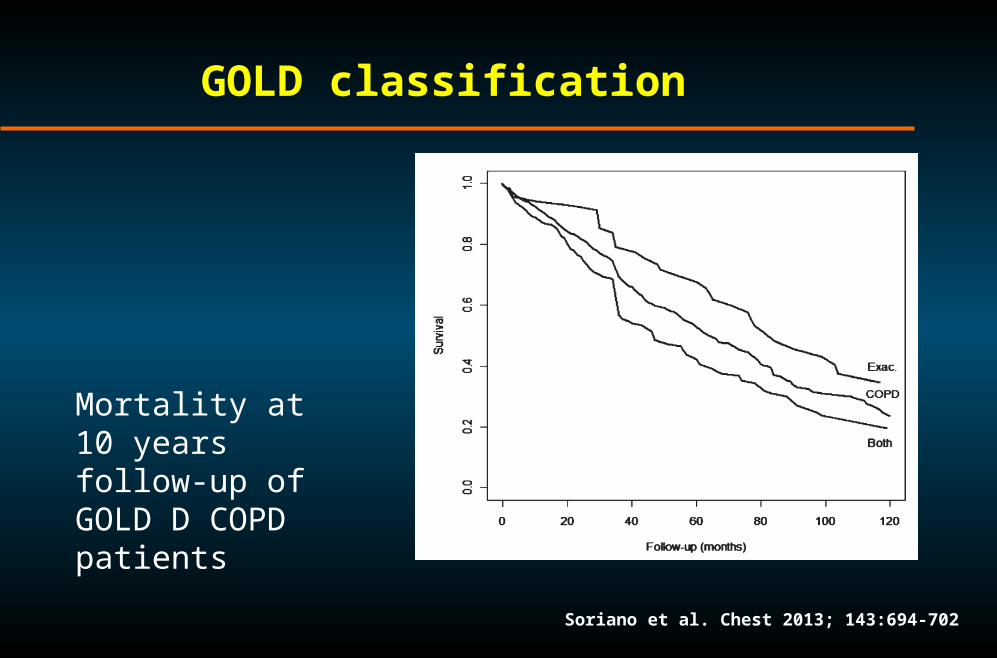
GOLD classification
Soriano et al. Chest 2013; 143:694-702
Mortality at 10 years follow-up of GOLD D COPD patients

Lange et al. AJRCCM 2012; 186: 975-981
GOLD classification
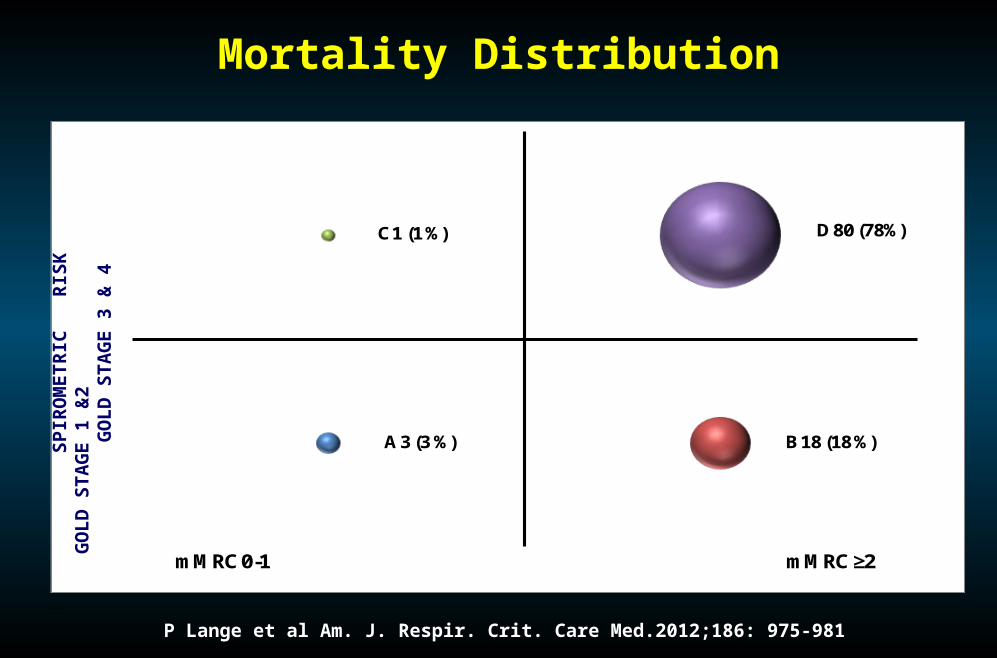
mMRC 0-1 mMRC ≥2
A 3 (3 %) B 18 (18 %)
C 1 (1 %) D 80 (78%)
Mortality DistributionS
PIR
OM
ET
RIC
R
ISK
GO
LD
STA
GE
1 &
2
GO
LD
STA
GE
3
& 4
P Lange et al Am. J. Respir. Crit. Care Med.2012;186: 975-981

Agusti et al. ERJ 2013; 42: 636-646
Outcomes according to GOLD
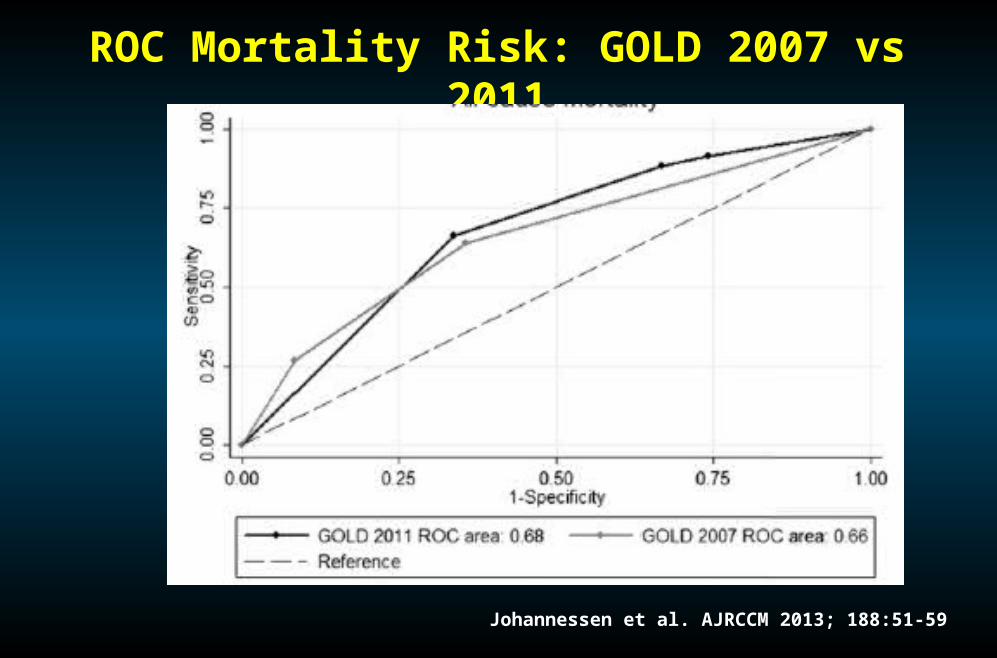
ROC Mortality Risk: GOLD 2007 vs 2011
Johannessen et al. AJRCCM 2013; 188:51-59

Treatment

Agusti et al. ERJ 2013; 42: 636-646
Treatment according to GOLD
Add ICS if exacerbations
1st choice:ICS+LABA or LAMA
C: 70% FEV1<50%D: 63% FEV1<50%
GOLD D and B: HR Exacerbation Reduction ICS+ LABA vs LABA
Anzueto et al ATS 2014

GOLD D Subgroups: HR Exacerbation Reduction ICS+ LABA vs LABA
Anzueto et al ATS 2014

What do we know of the new GOLD classification
Prevalence of the four groups varied between populations.
Groups A and D – more stable over time
Hospitalization and Mortality lowest in A, highest D, similar B and C
Comorbidities – more prevalent and symptomatic in B and D
Exacerbations increases from A to D


GOLD is a dynamic process that
Evolves with th
e disease

GOLD 2014:Antocholinergics
2013 2014
http://www.goldcopd.org/. Document 2014 Revision, Page 23

GOLD 2014:Anticholinergics – Adverse Events2013 2014
2013 Tiospir study – clarify adverse eventos of Spiriva Respimat
http://www.goldcopd.org/. Document 2014 Revision, Page 23

What we need next GOLD classification:
Phenotypes
Co-morbid conditions
Progression of disease – changes from one group to another
De-escalation of therapy

Different Look of COPD!
Agusti A et al. Am J Respir Crit Care Med. 2011;184:(5):507-513.
