global social contract to reduce maternal mortality
DESCRIPTION
Progress towards Millennium Development Goal 5a, reducing maternal deaths by 75% between 1990 and 2015, has been substantial; however, it has been too slow to hope for its achievement by 2015, particularly in sub-Saharan Africa, including Uganda. This suggests that both the Government of Uganda and the international community are failing to comply with their right-to-health-related obligations towards the people of Uganda. This country case study explores some of the key issues raised when assessing national and international right-to-health-related obligations. We argue that to comply with their shared obligations, national and international actors will have to take steps to move forward together. The Government of Uganda should not expect additional international assistance if it does not live up to its own obligations; at the same time, the international community must provide assistance that is more reliable in the long run to create the ‘fiscal space’ that the Government of Uganda needs to increase recurrent expenditure for health – which is crucial to addressing maternal mortality. We propose that the ‘Roadmap on Shared Responsibility and Global Solidarity for AIDS, TB and Malaria Response in Africa’, adopted by the African Union in July 2012, should be seen as an invitation to the international community to conclude a global social contract for health.TRANSCRIPT

ISSUES IN CURRENT POLICY
A global social contract to reduce maternal mortality: the humanrights arguments and the case of Uganda
Gorik Ooms,a Moses Mulumba,b Rachel Hammonds,c Laila Abdul Latif,d
Attiya Waris,e Lisa Formanf
a Researcher, Department of Public Health, Institute of Tropical Medicine; Researcher, Law and Development ResearchGroup, University of Antwerp, Antwerp, Belgium. Correspondence: [email protected]
b Executive Director, Center for Health, Human Rights and Development, Kampala, Uganda
c Researcher, Department of Public Health, Institute of Tropical Medicine; Researcher, Law and Development ResearchGroup, University of Antwerp, Antwerp, Belgium
d Researcher, Go4Health Project, University of Nairobi, Nairobi, Kenya; Advocate, Rachier & Amollo Advocates,Nairobi, Kenya
e Senior Lecturer, Commercial Law Department, University of Nairobi, Nairobi, Kenya
f Assistant Professor, Dalla Lana School of Public Health, University of Toronto, Toronto, Canada
Abstract: Progress towards Millennium Development Goal 5a, reducing maternal deaths by 75% between1990 and 2015, has been substantial; however, it has been too slow to hope for its achievement by2015, particularly in sub-Saharan Africa, including Uganda. This suggests that both the Government ofUganda and the international community are failing to comply with their right-to-health-related obligationstowards the people of Uganda. This country case study explores some of the key issues raised whenassessing national and international right-to-health-related obligations. We argue that to comply with theirshared obligations, national and international actors will have to take steps to move forward together.The Government of Uganda should not expect additional international assistance if it does not live up to itsown obligations; at the same time, the international community must provide assistance that is morereliable in the long run to create the ‘fiscal space’ that the Government of Uganda needs to increaserecurrent expenditure for health – which is crucial to addressing maternal mortality. We propose that the‘Roadmap on Shared Responsibility and Global Solidarity for AIDS, TB and Malaria Response in Africa’,adopted by the African Union in July 2012, should be seen as an invitation to the international communityto conclude a global social contract for health. © 2013 Reproductive Health Matters
Keywords: human rights, right to health, reproductive rights, maternal mortality, fiscal space,displacement, Uganda
Reducing maternal deaths by 75% between 1990and 2015 is one of the main goals of MillenniumDevelopment Goal (MDG) 5 (goal 5a). While prog-ress towards this goal has been substantial, ithas been too slow to hope for its achievementby 2015, particularly in sub-Saharan Africa.1 Forexample, according to the WHO World HealthStatistics 2013 report, in 2010 the maternal mor-tality ratio (MMR) in Uganda was 310 maternaldeaths per 100,000 live births, whereas a decadeearlier it had been 530.2 This is progress, butthere is no room for complacency.
In a ground-breaking resolution adopted in2009, the United Nation Human Rights Council
Contents online: www.rhm-elsevier.com
recognized that preventable maternal mortalityis a human rights violation, proclaiming that“most instances of maternal mortality and mor-bidity are preventable, and that preventablematernal mortality and morbidity is a health,development and human rights challenge thatalso requires the effective promotion and pro-tection of the human rights of women and girls”(Article 2).3
While there is no human right to be healthy,the human right to “the highest attainable stan-dard of health” (the right to health) means boththat every human being has entitlements to publicefforts to improve or preserve her or his health,
Doi: 10.1016/S0968-8080(13)42736-2 129

G Ooms et al. Reproductive Health Matters 2013;21(42):129–138
and to enjoy freedom from interference that wouldbe detrimental to their health.4 For the people ofeach State, the duty-bearer is, first and foremost,their Government, followed by the internationalcommunity as the second line duty-bearer, andspecifically “States in a position to assist”.4
In this paper, we argue that both the Govern-ment of Uganda and the international communityare failing to comply with their right-to-health-related obligations towards the people of Uganda,and that in order to comply, they will have totake steps forward together. The Government ofUganda should not expect additional interna-tional assistance if it does not live up to its ownobligations, but at the same time, the interna-tional community must provide assistance that ismore reliable in the long run to create the ‘fiscalspace’ that the Government of Uganda needs toincrease recurrent expenditure for health – whichis crucial to addressing maternal mortality.
To clarify the multiple issues raised when assess-ing national and international right-to-health-related obligations, we adopted a county case studyapproach, as it allows for a more in-depth detailedanalysis. We chose to focus on maternal mortality inUganda because the scope of the Government ofUganda’s right-to-health-related obligations is thesubject of a petition filed in the ConstitutionalCourt, which testifies to the growing realisation ofthe importance of clarifying this issue.5
Our analysis will focus on four points:
• that mobilising resources matters; while it isnot the only factor in reducing maternal mor-tality, it is an important one;
• that many states are failing to comply withtheir obligation to mobilise maximum avail-able resources, both domestically and in termsof international assistance;
• that health aid has to become more reliable toenable the effective use of additional domesticresources; and
• that the ‘Roadmap on Shared Responsibilityand Global Solidarity for AIDS, TB and MalariaResponse in Africa’, adopted by the AfricanUnion in July 2012, should be seen as an invi-tation to the international community to con-clude a global social contract for health.6
Mobilising resources mattersSeveral reasons have been put forward to explainthe failure to achieve MDG 5a in sub-Saharan Africa,
130
including a shortage of financial resources, lack ofpolitical will, vague legislation and policy that donot pinpoint responsibility, cultural beliefs, gender-based discrimination, education and literacy chal-lenges, health system weaknesses (including lack ofhealth professionals with adequate skills and train-ing) and a range of infrastructural deficiencies.7
The International Covenant on Economic, Socialand Cultural Rights indicates that the rights itdescribes impose corresponding obligations: “totake steps, individually and through internationalassistance and co-operation, especially economicand technical, to the maximum of its availableresources, with a view to achieving progressivelythe full realization of the rights recognized inthe present Covenant” (emphasis added).8 Is theCovenant’s focus on maximum available resourceswarranted and what does it mean?
It is difficult to track government health expen-diture for maternal health in particular. Further-more, in line with Freedman and colleagues, weargue that instead of focusing on “the fine pointsof precisely which effective [maternal health]interventions theoretically fit best into genericpackages, we now need to address the healthsystem that must deliver them.”9 Therefore, weexamined the recent evolution of governmenthealth expenditure (GHE) – that is, for the entirehealth system.
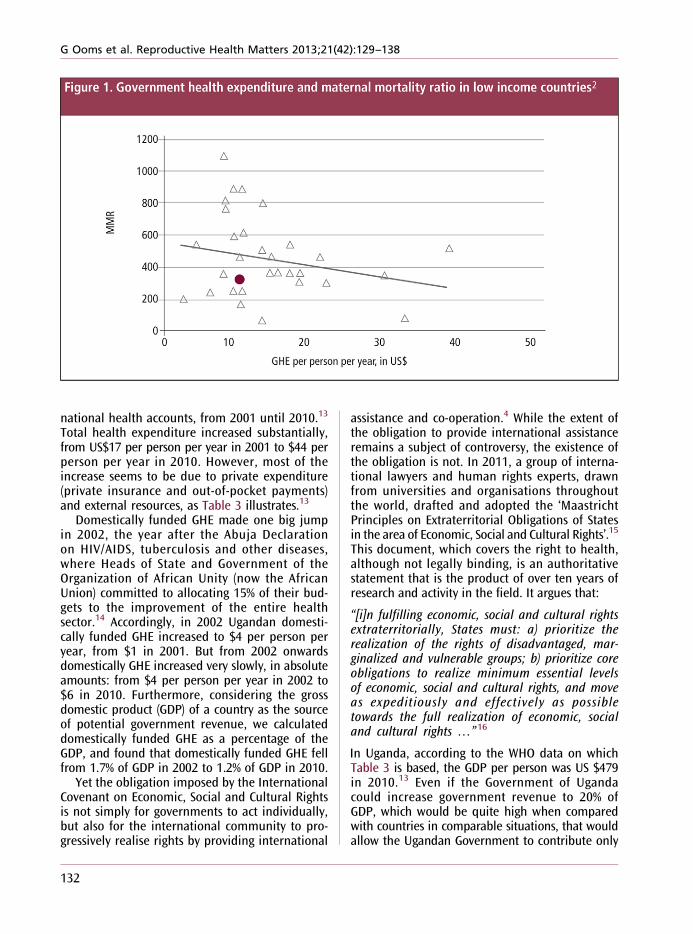
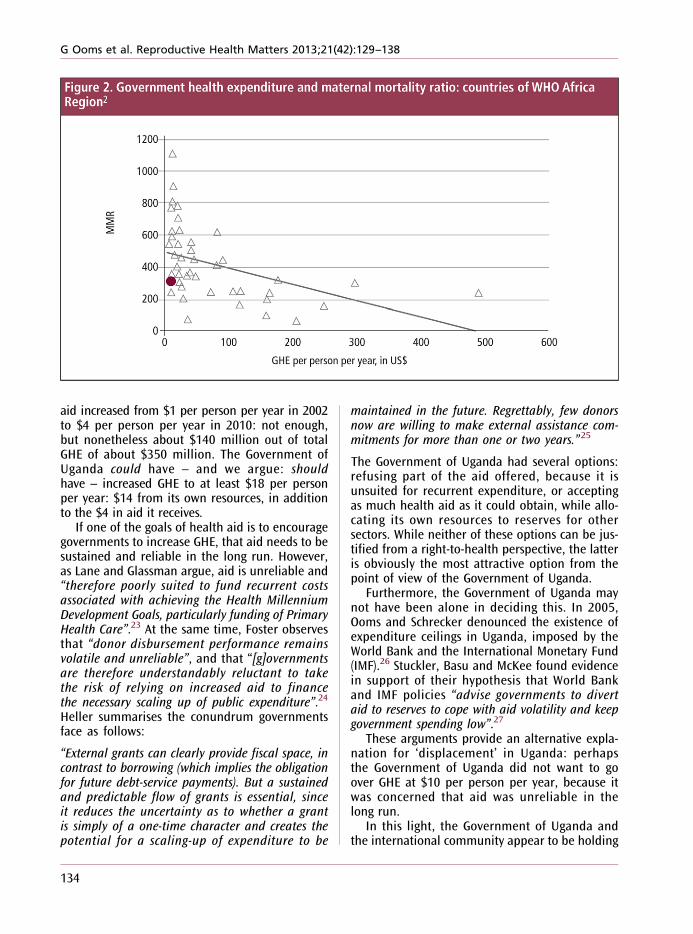
Table 1 and Figure 1 below illustrate the rela-tionship between GHE (in US$ per person per year)and the MMR in low-income countries. Table 2and Figure 2 illustrate the relationship betweenGHE and MMR in all countries of the WHO Africaregion. The distances between the dots and thetrend lines illustrate that how financial resourcesare spent is as important as how much resourcesare allocated. In Chad, for example, where GHEstands at $8 (per person per year), the MMR is1,100 per 100,000 live births, while in Madagascarthe MMR is only 240, with GHE at $9. Scholarshave examined several hypotheses to explain thisirregular correlation. Unger and colleagues arguethat disease control programmes have negativelyaffected health systems and consequently mater-nal health care.10 Penn-Kekana and colleaguesnote that “there are also frequent examples offailure to render strategies effective or to deliverthem to intended groups despite the availabilityof inputs and appropriately trained staff in theright place at the right time.”11
The purpose of our analysis, however, is not toexamine why additional financial resources may

G Ooms et al. Reproductive Health Matters 2013;21(42):129–138
not always produce the desired effect of strongerhealth systems and decreasing maternal mortality,but to analyse why it is difficult to increase thefinancial resources. The question at this point isnot whether government health expenditure isthe only factor; the question is whether it is animportant factor. Or to put it another way, cancountries like Uganda lower their maternal mor-tality ratios without increasing their financialresources for health?
In Uganda (the round dot in the figures), GHEstands at $10, and the MMR at 310. Among 23 low-income countries with comparable levels of GHE($15 or less), only seven have a lower MMR (and arearguably allocating GHE more efficiently when itcomes to reducing theMMR): Bangladesh, Cambodia,Eritrea, Madagascar, Myanmar, Nepal and Tajikistan.The other 15 countries have a higher MMR. Among14 countries in the WHO Africa region where theMMR is lower than in Uganda, only two have simi-lar or lower GHE: Eritrea and Madagascar. So thereprobably is some room to further reduce the MMRin Uganda without increasing GHE, but not much.
We therefore argue that the conclusion of Borghiand colleagues of 2006 is still valid today:
“Current investment in maternal health is insuffi-cient to meet MDG 5, and substantial additionalresources will need to be mobilised to strengthenthe health system to scale up coverage of maternalhealth services and to create demand for these ser-vices through appropriate financing initiatives.”12
Both the Government of Uganda and theinternational community are failing tocomply with their obligations towardsthe people of UgandaTo comply with its right-to-health-related obli-gations under the International Covenant on Eco-nomic, Social and Cultural Rights, the Governmentof Uganda is obliged to take steps to progressivelyrealise the right to health, to the maximum ofavailable resources.8 The International Covenanton Economic, Social and Cultural Rights, and Gen-eral Comment 14, clarify that when a governmentis unable to respect, protect and fulfil its right-to-health-related obligations, the internationalcommunity – notably other countries in a positionto assist – are obliged to provide assistance.4
To assess whether the Government of Ugandais spending the maximum of available resources,we looked at the WHO estimates for Uganda’s
131
G Ooms et al. Reproductive Health Matters 2013;21(42):129–138
national health accounts, from 2001 until 2010.13
Total health expenditure increased substantially,from US$17 per person per year in 2001 to $44 perperson per year in 2010. However, most of theincrease seems to be due to private expenditure(private insurance and out-of-pocket payments)and external resources, as Table 3 illustrates.13
Domestically funded GHE made one big jumpin 2002, the year after the Abuja Declarationon HIV/AIDS, tuberculosis and other diseases,where Heads of State and Government of theOrganization of African Unity (now the AfricanUnion) committed to allocating 15% of their bud-gets to the improvement of the entire healthsector.14 Accordingly, in 2002 Ugandan domesti-cally funded GHE increased to $4 per person peryear, from $1 in 2001. But from 2002 onwardsdomestically GHE increased very slowly, in absoluteamounts: from $4 per person per year in 2002 to$6 in 2010. Furthermore, considering the grossdomestic product (GDP) of a country as the sourceof potential government revenue, we calculateddomestically funded GHE as a percentage of theGDP, and found that domestically funded GHE fellfrom 1.7% of GDP in 2002 to 1.2% of GDP in 2010.
Yet the obligation imposed by the InternationalCovenant on Economic, Social and Cultural Rightsis not simply for governments to act individually,but also for the international community to pro-gressively realise rights by providing international
132
assistance and co-operation.4 While the extent ofthe obligation to provide international assistanceremains a subject of controversy, the existence ofthe obligation is not. In 2011, a group of interna-tional lawyers and human rights experts, drawnfrom universities and organisations throughoutthe world, drafted and adopted the ‘MaastrichtPrinciples on Extraterritorial Obligations of Statesin the area of Economic, Social and Cultural Rights’.15
This document, which covers the right to health,although not legally binding, is an authoritativestatement that is the product of over ten years ofresearch and activity in the field. It argues that:
“[i]n fulfilling economic, social and cultural rightsextraterritorially, States must: a) prioritize therealization of the rights of disadvantaged, mar-ginalized and vulnerable groups; b) prioritize coreobligations to realize minimum essential levelsof economic, social and cultural rights, and moveas expeditiously and effectively as possibletowards the full realization of economic, socialand cultural rights …”16
In Uganda, according to the WHO data on whichTable 3 is based, the GDP per person was US $479in 2010.13 Even if the Government of Ugandacould increase government revenue to 20% ofGDP, which would be quite high when comparedwith countries in comparable situations, that wouldallow the Ugandan Government to contribute only

G Ooms et al. Reproductive Health Matters 2013;21(42):129–138
$96 per person per year in domestic funding toits entire budget.17 If the Government of Ugandawould then spend 15% of that budget on health,as promised in the Abuja Declaration, the domes-tically funded GHE would increase to $14 perperson per year – as compared to the 2010 levelof $6 per person.13
The High-Level Taskforce on Innovative Inter-national Financing for Health Systems found that,in low-income countries, the annual costs of achiev-ing the current health sector MDGs would be about$50-55 per person per year.18 Even if we take pri-vate expenditure out of the equation – accordingto the World Health Report of 2010, it is “onlywhen direct payments fall to 15–20% of totalhealth expenditures that the incidence of finan-cial catastrophe and impoverishment falls to negli-gible levels”– GHE should still be at least $45 perperson per year.19 The gap between $45 per personper year and $14 (what domestically funded GHEcould be) is $31, and that is what the internationalcommunity must provide, at the least, to enable theGovernment of Uganda to comply with the healthsector part of its core right-to-health-related obliga-tions: “basic arithmetic”, according to Sachs.20 Atpresent, however, aid to Uganda is about $10 perperson per year, or a third of the $31 gap. Further-more, it should be noted that the $10 per personper year in aid covers all external resources, includ-ing the resources that are spent outside of thegovernment budget. If total GHE is $10 per personper year in 2010, and domestically funded GHE is$6, then ‘on budget aid’ is merely $4 per person peryear – while it should be $31.
The Government of Uganda and theinternational community have to takesteps forward togetherTable 3 suggests that Uganda is a textbook exampleof ‘displacement’: when international assistance fora given programme increases, domestically fundedpublic expenditure for the same programme tendsto decrease.21,22 In Uganda, between 2002 and2010, there was no decrease of domestically fundedGHE in absolute amounts, but there was a seriousdecrease when measured as a percentage of GDP,as Table 3 illustrates.
But what were the Government of Uganda’soptions? While domestically funded GHE increasedfrom $4 per person per year in 2002 to $6 in 2010,total GHE increased from $5 per person per year2002 to $10 in 2010. This indicates how ‘on budget’
133
G Ooms et al. Reproductive Health Matters 2013;21(42):129–138
aid increased from $1 per person per year in 2002to $4 per person per year in 2010: not enough,but nonetheless about $140 million out of totalGHE of about $350 million. The Government ofUganda could have – and we argue: shouldhave – increased GHE to at least $18 per personper year: $14 from its own resources, in additionto the $4 in aid it receives.
If one of the goals of health aid is to encouragegovernments to increase GHE, that aid needs to besustained and reliable in the long run. However,as Lane and Glassman argue, aid is unreliable and“therefore poorly suited to fund recurrent costsassociated with achieving the Health MillenniumDevelopment Goals, particularly funding of PrimaryHealth Care”.23 At the same time, Foster observesthat “donor disbursement performance remainsvolatile and unreliable”, and that “[g]overnmentsare therefore understandably reluctant to takethe risk of relying on increased aid to financethe necessary scaling up of public expenditure”.24
Heller summarises the conundrum governmentsface as follows:
“External grants can clearly provide fiscal space, incontrast to borrowing (which implies the obligationfor future debt-service payments). But a sustainedand predictable flow of grants is essential, sinceit reduces the uncertainty as to whether a grantis simply of a one-time character and creates thepotential for a scaling-up of expenditure to be
134
maintained in the future. Regrettably, few donorsnow are willing to make external assistance com-mitments for more than one or two years.”25
The Government of Uganda had several options:refusing part of the aid offered, because it isunsuited for recurrent expenditure, or acceptingas much health aid as it could obtain, while allo-cating its own resources to reserves for othersectors. While neither of these options can be jus-tified from a right-to-health perspective, the latteris obviously the most attractive option from thepoint of view of the Government of Uganda.
Furthermore, the Government of Uganda maynot have been alone in deciding this. In 2005,Ooms and Schrecker denounced the existence ofexpenditure ceilings in Uganda, imposed by theWorld Bank and the International Monetary Fund(IMF).26 Stuckler, Basu and McKee found evidencein support of their hypothesis that World Bankand IMF policies “advise governments to divertaid to reserves to cope with aid volatility and keepgovernment spending low”.27
These arguments provide an alternative expla-nation for ‘displacement’ in Uganda: perhapsthe Government of Uganda did not want to goover GHE at $10 per person per year, because itwas concerned that aid was unreliable in thelong run.
In this light, the Government of Uganda andthe international community appear to be holding

G Ooms et al. Reproductive Health Matters 2013;21(42):129–138
each other hostage. The international communitywould be reluctant to increase health aid toUganda further: it financed most of the increasein GHE between 2002 and 2010, and althoughthe GDP of Uganda doubled in size, the Govern-ment allocated the additional revenue elsewhere.But if the international community does not makelong-term aid commitments, then the Govern-ment of Uganda in turn could be reluctant toincrease GHE, because it does not want to createexpectations that it may not be able to meet inthe longer term.28
The ‘African Union Roadmap on SharedResponsibility and Global Solidarity forAIDS, TB and Malaria Response in Africa’provides a way forwardHow can this deadlock be broken? Governmentslike the Government of Uganda should be encour-aged to increase domestically funded GHE without
running the risk of seeing wealthier states reducetheir health aid; and the international communityshould be encouraged to increase health aid toUganda without running the risk of seeing theGovernment of Uganda decrease domestic fund-ing for health. States needing assistance and statesproviding assistance should aim for a global socialcontract for health, based on the right to health,under which they make reciprocal commitmentsand under which they can hold each other account-able for agreed increases in both domesticallyfunded GHE and health aid.
A first major step towards such a global socialcontract has been taken already. In July 2012, theAfrican Union adopted a ‘Roadmap on SharedResponsibility and Global Solidarity for AIDS,TB and Malaria Response in Africa’ (Roadmap),which calls on African governments and on theinternational community to fill the funding gapstogether.6 Although the title of the Roadmap refersto AIDS, tuberculosis and malaria only, it contains
135

G Ooms et al. Reproductive Health Matters 2013;21(42):129–138
proposals about financial responsibility for healthin general, and about reciprocal responsibility.Section 39 of the Roadmap states:
“Protecting development assistance, however, willrequire more visible southern leadership and com-mitment to increased domestic and diversified fund-ing and effective and efficient use of resources.”6
The Roadmap suggests that African Union mem-bers are willing to be held accountable for theirefforts in relation to the commitments they havemade, but expect in return longer-term predictablehealth aid. Now it is time for the international com-munity to acknowledge the offer, and to prepare ananswer, in line with its own existing commitments.
Although the suggestions in the Roadmap arenot precise enough to serve as the basis for abinding treaty, they can be considered as anopening bid: increased domestic funding inreturn for increased and more reliable aid, andvice versa. A Framework Convention on GlobalHealth could formalise the principles of such aglobal social contract for health, while a protocolon financing could set targets, to be revised regu-
136
larly, until all preventable maternal mortality isindeed effectively prevented.29
Within the context of the post-2015 agenda,we consider the Roadmap as a bid worth consider-ing. While we think it remains important that thepost-2015 health agenda keeps a focus on priorityhealth issues, including maternal mortality andsexual and reproductive health and rights, specificneeds have to be addressed within the context ofhealth systems as a whole. In order to ensure thatincreased domestic funding for health does notdisplace health aid, or vice versa, and that GHEfrom all sources combined increases, we believea global social contract for health is required.
AcknowledgmentsThis study is part of the Go4Health research project,funded by the European Union’s Seventh FrameworkProgramme, grant HEALTH-F1-2012-305240, bythe Australian Government’s NH&MRC-EuropeanUnion Collaborative Research Grants, grant 1055138,and by the Canadian Institutes of Health ResearchOperating Grant, Ethics grant 131587.
References
1. United Nations. Millennium Development Goals 7. Karlsen S, Say L, Souza J, et al. The relationship
Report 2011. 2012. http://www.un.org/millenniumgoals/11_MDG%20Report_EN.pdf.2. World Health Organization. World Health Statistics2013. 2013. http://www.who.int/gho/publications/world_health_statistics/2013/en/.
3. United Nations Human Rights Council. Preventablematernal mortality and morbidity and human rights.Resolution 11/8 U.N. Doc. A/HRC/RES/11/8. 2009.http://ap.ohchr.org/documents/E/HRC/resolutions/A_HRC_RES_11_8.pdf.
4. Committee on Economic, Social and Cultural Rights.General Comment 14, The right to the highestattainable standard of health. U.N. Doc. E/C.12/2000/4.2000. http://www1.umn.edu/humanrts/gencomm/escgencom14.htm.
5. Centre for Health, Human Rights and Development,Advocating for the Right to Reproductive Health Carein Uganda, The Import of Constitutional PetitionNo. 16 of 2011. 2012. http://www.cehurd.org/wp-content/uploads/downloads/2012/01/Petition-16-Study.pdf.
6. African Union. Roadmap on Shared Responsibility andGlobal Solidarity for AIDS, TB and Malaria Response inAfrica. 2012. http://www.au.int/en/sites/default/files/Shared_Res_Roadmap_Rev_F%5b1%5d.pdf.
between maternal education and mortality amongwomen giving birth in health care institutions: analysisof the cross-sectional WHO Global Survey onMaternal and Perinatal Health. BMC Public Health2011;11:606. http://www.biomedcentral.com/1471-2458/11/606.
8. International Covenant on Economic, Social andCultural Rights, G.A. res. 2200A (XXI), 21 U.N.GAORSupp. (No. 16) at 49, U.N. Doc. A/6316 (1966),993 U.N.T.S. 3, entered into force Jan. 3, 1976.http://www1.umn.edu/humanrts/instree/b2esc.htm.
9. Freedman LP, Graham WJ, Brazier E, et al. Practicallessons from global safe motherhood initiatives: timefor a new focus on implementation. Lancet2007;370(9595):1383–91.
10. Unger J-P, Van Dessel P, Sen K, De Paepe P. Internationalhealth policy and stagnating maternal mortality: isthere a causal link? Reproductive Health Matters2009;17(33):91–104.
11. Penn-Kekana L, McPake B, Parkhurst J. Improvingmaternal health; getting what works to happen.Reproductive Health Matters 2007;15(30):28–37.
12. Borghi J, Ensor T, Somanathan A, et al. on behalf ofLancet Maternal Survival Series steering group.
G Ooms et al. Reproductive Health Matters 2013;21(42):129–138
Mobilising financial resources for maternal health.Lancet 2006;368(9545):1457–65.
13. World Health Organization. National Health Accounts;Uganda; WHO estimates for country NHA data.http://www.who.int/nha/country/uga/en/.
14. Organisation of African Unity. Abuja Declaration onHIV/AIDS, Tuberculosis, and Other Related InfectiousDiseases. 2001. http://www.un.org/ga/aids/pdf/abuja_declaration.pdf.
15. De Schutter O, Eide A, Khalfan A, et al. Commentaryto the Maastricht Principles on Extraterritorial Obligationsof States in the area of Economic, Social and CulturalRights, 28 September 2011. Human Rights Quarterly2012;34:1084–69. http://www.lse.ac.uk/humanRights/articlesAndTranscripts/2012/HRQMaastricht.pdf.
16. The Maastricht Principles on Extraterritorial Obligations ofStates in the area of Economic, Social and Cultural Rights,28 September 2011. http://www.maastrichtuniversity.nl/web/Institutes/MaastrichtCentreForHumanRights/MaastrichtETOPrinciples.htm.
17. International Monetary Fund. Regional economic outlook.Sub-Saharan Africa: April 2012. http://www.imf.org/external/pubs/ft/reo/2012/afr/eng/sreo0412.pdf.
18. Taskforce on Innovative International Financing forHealth Systems. More Money for Health, and MoreHealth for the Money. 2009. http://www.internationalhealthpartnership.net/fileadmin/uploads/ihp/Documents/Results___Evidence/HAE__results___lessons/Taskforce_report_EN.2009.pdf.
19. World Health Organization. World Health Report 2010.Health Systems Financing: The Path to UniversalCoverage. Geneva: WHO, 2010. http://whqlibdoc.who.int/whr/2010/9789241564021_eng.pdf.
20. Sachs J. Achieving universal health coverage inlow-income settings. Lancet 2012;380(9845):944–47.
RésuméLes progrès vers l’OMD 5a, une réduction de 75%des décès maternels entre 1990 et 2015, ont étésubstantiels, mais néanmoins trop lents pourespérer le réaliser cet objectif d’ici à 2015, enparticulier en Afrique subsaharienne, y comprisen Ouganda. Cela laisse entendre que ni leGouvernement ougandais ni la communautéinternationale ne respectent leurs obligationsliées au droit à la santé envers la populationougandaise. Cette étude de cas de pays explorecertaines questions clés soulevées lors del’évaluation des obligations nationales etinternationales relatives au droit à la santé.Nous avançons que pour s’acquitter de leursobligations partagées, les acteurs nationaux et
21. Farag M, Nandakumar AK, Wallack SS, et al. Doesfunding from donors displace government spendingfor health in developing countries? Health Affairs2009;28(4):1045–55.
22. Lu C, Schneider MT, Gubbins P, et al. Public financingof health in developing countries: a cross-nationalsystematic analysis. Lancet 2010;375(9723):1375–87.
23. Lane C, Glassman A. Smooth and predictable aid forhealth: a role for innovative financing? Washington, DC:Brookings Institution, 2008. http://www.brookings.edu/papers/2008/08_global_health_glassman.aspx.
24. Foster M. Fiscal space and sustainability: towards asolution for the health sector. In: High-Level Forum forthe Health MDGs, Selected papers 2003–2005. Geneva:WHO; Washington, DC: World Bank, 2005. p.67.http://www.who.int/hdp/publications/hlf_volume_en.pdf.
25. Heller P, Binding constraints on public funding:prospects for creating “fiscal space”. In: Preker A,Linder M, Chernichovsky D, et al, editors. Scaling UpAffordable Health Insurance: Staying the Course.Washington, DC: World Bank; 2013. p.93.
26. Ooms G, Schrecker T. Expenditure ceilings, multilateralfinancial institutions, and the health of poor populations.Lancet 2005;365(9473):1821–23.
27. Stuckler D, Basu S, McKee M. International MonetaryFund and aid displacement. International Journal ofHealth Services 2011;41(1):67–76.
28. Ooms G, Hill PS, Hammonds R, et al. Applying theprinciples of AIDS ‘exceptionality’ to global health:challenges for global health governance. GlobalHealth Governance 2010;4(1):1–9.
29. Gostin LO, Friedman EA, Ooms G, et al. The joint actionand learning initiative: towards a global agreementon national and global responsibilities for health.PLoS Med 2011;8(5):e1001031.
ResumenSe han logrado considerables avances hacia laconsecución del Objetivo 5a de Desarrollo delMilenio, reducir la mortalidad materna en un75% entre 1990 y 2015; sin embargo, estos hansido demasiado lentos para cumplir el objetivopara 2015, particularmente en África subsahariana,incluida Uganda. Esto indica que tanto el Gobiernode Uganda como la comunidad internacional noestán cumpliendo sus obligaciones para con elpueblo de Uganda respecto al derecho a la salud.Este estudio de caso de país explora algunos de losasuntos clave planteados al evaluar las obligacionesnacionales e internacionales relacionadas con elderecho a la salud. Argumentamos que paracumplir sus obligaciones compartidas, los actores
137

internationaux devront prendre des mesures pouravancer ensemble. Le Gouvernement ougandaisne doit pas attendre d’aide internationalesupplémentaire s’il n’honore pas ses propresobligations; en même temps, la communautéinternationale doit prodiguer une assistance plusfiable à long terme dans le but de créer « l’espacefiscal » dont le Gouvernement ougandais abesoin pour relever les dépenses de santérécurrentes, ce qui est essentiel pour luttercontre la mortalité maternelle. Nous proposonsque la « Feuille de route sur la responsabilitépartagée et la solidarité mondiale dans la riposteau SIDA, à la tuberculose et au paludisme enAfrique », adoptée par l’Union africaine en juillet2012, soit considérée comme une invitation lancéeà la communauté internationale en vue de conclure
nacionales e internacionales deberán tomarmedidas para seguir adelante de manera conjunta.El Gobierno de Uganda no debería esperarrecibir más ayuda internacional si no cumplesus obligaciones; asimismo, la comunidadinternacional debe brindar asistencia que seamás fiable a la larga para crear el ‘espacio fiscal’que el Gobierno de Uganda necesita para aumentarlos gastos recurrentes en salud, que es crucialpara tratar el problema de mortalidad materna.Proponemos que el ‘Mapa de responsabilidadcompartida y solidaridad mundial en respuestaal SIDA, la TB y la malaria en África’, adoptadopor la Unión Africana en julio de 2012, debeconsiderarse como una invitación a la comunidadinternacional para concluir un contrato socialmundial para la salud.
G Ooms et al. Reproductive Health Matters 2013;21(42):129–138
un contrat social mondial pour la santé.
138