global, regional, and thailand movements on universal ... dr suwit... · global, regional, and...
TRANSCRIPT

Global, Regional, and Thailand
Movements on Universal Health
Coverage and the Important of
Quality Health Services
Dr. Suwit Wibulpolprasert, Senior Adviser on Disease Control, MoPH.
Presented at the CAP UHC Workshop on UHC and HA
November 25th 2013, Narai Hotel, Silom, Bangkok, Thailand.

The Universal Health Coverage
• Universal access to quality comprehensive
(promotion, prevention, treatment,
rehabilitation and palliative care) essential
health services and technologies, without
financial barriers
• Free but low quality health services is not UHC
• Three dimensions to target on Who, What and
How much to cover in the UHC in each
country?
Suwit Wibulpolprasert, MoPH, Thailand

Thai UC – three dimensions of UC cube
• X axis: Who is covered?– Universal (100%) Coverage by
3 public schemes
• Y axis: Proportion of the costs covered?– Total health cost– Low incidence of catastrophic
health expenditure and medical impoverishment
• Z axis: Which services are covered?– Essential comprehensive
services and drugs– High cost services are
covered e.g. Renal Replacement Therapy, chemotherapy, ARVs
UHC is feasible and sustainable
• UHC can be started and achieved at low level
of income – don’t wait until you are rich
• UHC is effective for poverty reduction
• Fiscal spaces and innovative financing are
possible for additional resources mobilization
• Mechanisms are there to ensure quality, value
for money, sustainable financing and meeting
the emerging challenges
Suwit Wibulpolprasert, MoPH, Thailand

UHC can be started and achieved at low level of income –
Economic Crisis is an opportunity not a threat
390
710
760
1490
2,700
1,900
0
1,000
2,000
3,000
4,000
1970
1972
1974
1976
1978
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
US $
1997: Asian
financial crisis
1990 SHI
introduced
1980 CSMBS
introduced
1983 CBHI
introduced
1975 Low Income
scheme introduced
2002 Universal
Coverage for entire
population achieved
2001: 29% of
population are
uninsured
year
GD
P/ca
pit
a
29%
42%
53%
The children n elderly 71%
100%
Suwit Wibulpolprasert, MoPH, Thailand
6
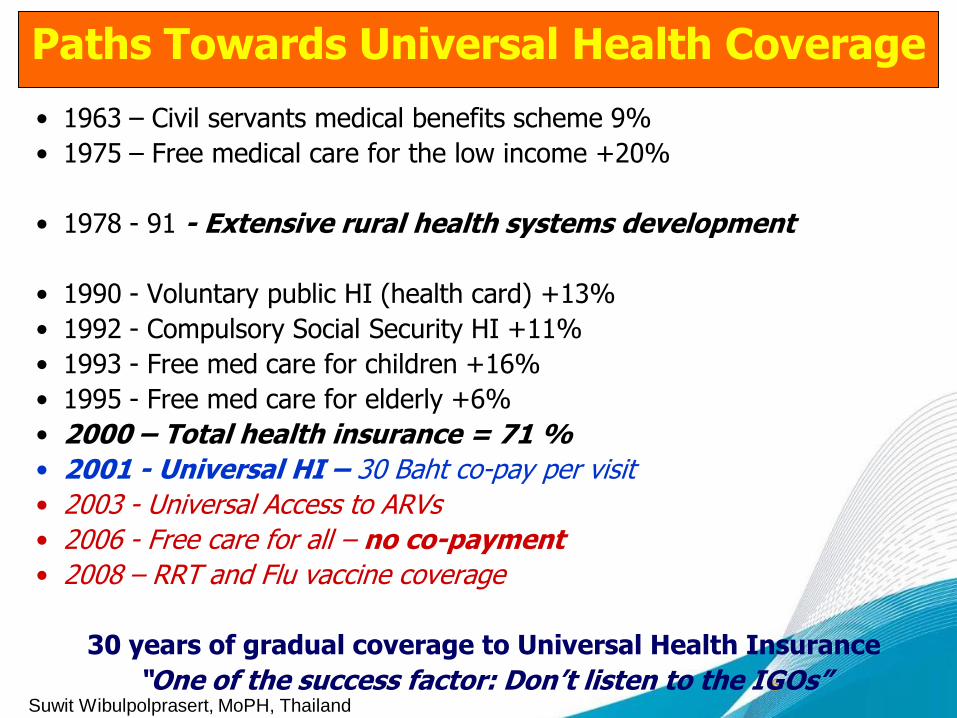
Paths Towards Universal Health Coverage
• 1963 – Civil servants medical benefits scheme 9%
• 1975 – Free medical care for the low income +20%
• 1978 - 91 - Extensive rural health systems development
• 1990 - Voluntary public HI (health card) +13%
• 1992 - Compulsory Social Security HI +11%
• 1993 - Free med care for children +16%
• 1995 - Free med care for elderly +6%
• 2000 – Total health insurance = 71 %
• 2001 - Universal HI – 30 Baht co-pay per visit
• 2003 - Universal Access to ARVs
• 2006 - Free care for all – no co-payment
• 2008 – RRT and Flu vaccine coverage
30 years of gradual coverage to Universal Health Insurance
“One of the success factor: Don’t listen to the IGOs” Suwit Wibulpolprasert, MoPH, Thailand

7
Three schemes for Universal Health Insurance
2012
NHS Act CSMBS decree SS Act Contribution
2001
National Health
Security Office Comptroller Dept
Social
Security Office
Capitation 100 $US/y
“Fee for service”380 $US/y
Capitation 75 $US/y
Designated Public /
Private Providers
47.8 mil. 5.5 mil. 9.5 mil.
Private roomnon- ED
The population
TAX1991
Service
s
1963
Rest of Pop Civil servants Formal employees

8
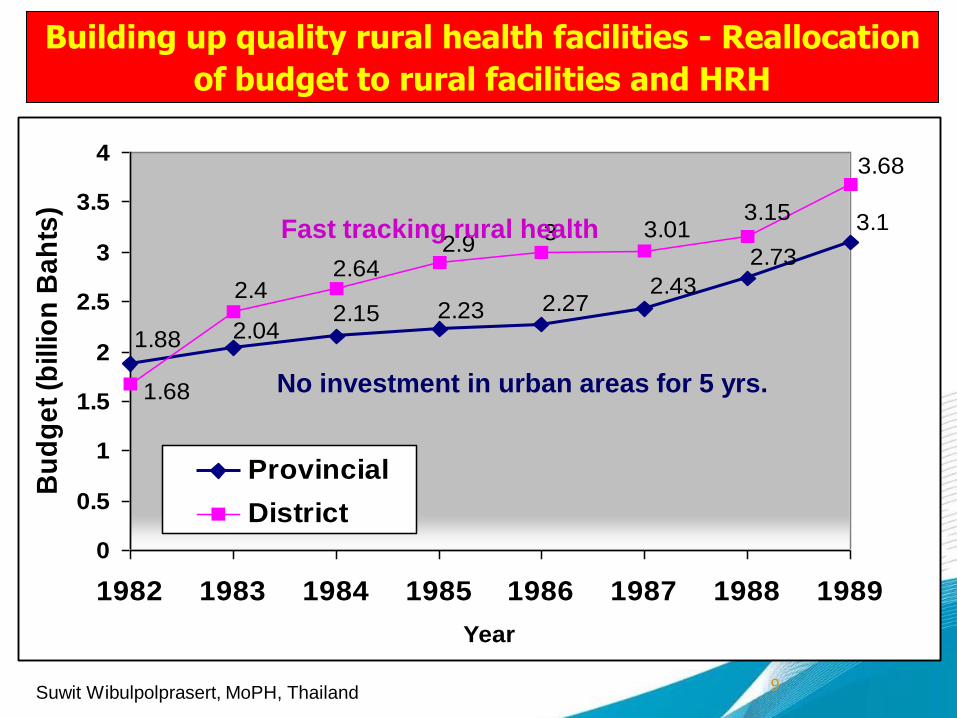
• Extensive expansion of rural health services in
early 80s – in spite of economic crisis
• How? – Budget shifting - Freeze new capital
investment in urban health facilities for 5 years and
reallocate to rural health facilities.
• Extensive production of motivated Rural Health
Workers with compulsory public services and
incentives
• Establishment of Hospital Accreditation Institute
Ensuring availability
of quality health services
Suwit Wibulpolprasert, MoPH, Thailand
9
Building up quality rural health facilities - Reallocation
of budget to rural facilities and HRH
3.1
2.73
2.432.272.232.15
2.041.88
3.68
3.153.013
2.92.64
2.4
1.68
0
0.5
1
1.5
2
2.5
3
3.5
4
1982 1983 1984 1985 1986 1987 1988 1989
Year
Bu
dg
et
(billio
n B
ah
ts)
Provincial
District
Fast tracking rural health
No investment in urban areas for 5 yrs.
Suwit Wibulpolprasert, MoPH, Thailand

10
Rural health centers with 3-6 nurses n CHWs cover 2,000-5,000 population
Adequate and appropriately manned rural health facilitieis
Rural community hospital with 2-8
doctors cover 30-100,000 population
Extensive production
of appropriate cadres
and motivated health
personnel with
mandatory public
works and adequate
support are essential.
Suwit Wibulpolprasert, MoPH, Thailand

1111
From reverse to upright triangle: PHC utilization (OP visits)
Suwit Wibulpolprasert, MoPH, Thailand

UHC achieved
UHC is effective for poverty reduction
UHC achieved
Source: Viroj Tangcharoensathien
Suwit Wibulpolprasert, MioPH, Thailand

13
Fiscal Space to health from peace and economic growth
Per
cen
tage
Year
Source: Bureau of BudgetSuwit Wibulpolprasert, MoPH, Thailand

Mechanism to ensure Better Value for Money and
Cost Control for Sustainable Financing
• 20% of UC budget to P&P & community H fund
• Health Intervention and Technology Assessment to
ensure ‘value for money”
• Strategic purchasing – Central purchasing w VMI and
TRIPs flexibilities – internal fiscal space
• Close end capitation budget with mixed payment
mechanisms and PC gate keeper
• Improve quality of health services – HA+++Suwit Wibulpolprasert, MoPH, Thailand

Central purchasing and bargaining of drug and instrument
Items
Unit cost (Baht)
Saving (Baht)Before After Number (unit)
1.Instrument
Folding lens 4,000 2,800 64,100 76,920,000
Unfolding lens 4,000 700 7,197 23,750,1o0
Balloon stent 20,000 10,000 26,655 266,550,000
Coronary stent 30,000 5,000 10,575 264,375,000
Drug elutent stent 85,000 17,000 33,794 2,297,992,000
DES Alloy stent 55,000 25,000 343 10,290,000
2. Drug (sample)
ARV (AZT 300 mg caps.) 1201.22 891.23 47,000 14,569,530
ARV (EFV 600 mg tabs.) 304.89 149.51 400,000 62,152,000
ARV (LPV/RTV 200/50 mg (CL) 2139.82 1481.91 170,000 111,844,700
Botulinum toxin type A 100 IU 10,750.00 7977.74 946 2,622,557.96
Docetaxel 80 mg inj 25654.32 4716.26 2,700 56,532,747.31
IVIG 5% 100 ml 9,649.62 5,479 19,200 80,075,904
Peg-interferon alpha 11,000 3,150 77,000 604,450,000
Influenza vaccine 200 150.28 643,319 31,985,820
Erythropoietin 671 229 1,634,239 722,333,638
CAPD fluid 200 105 19,095,657 1,814,087,415
Saving 6,440,531,412.27
From: NHSO 2012Suwit Wibulpolprasert, MoPH, Thailand

Rate of use of Lopinavir/Ritonavir (200/50mg)
bottles CL
0
5,000
10,000
15,000
20,000
25,000
UC Scheme
CL
Suwit Wibulpolprasert, MoPH, Thailand
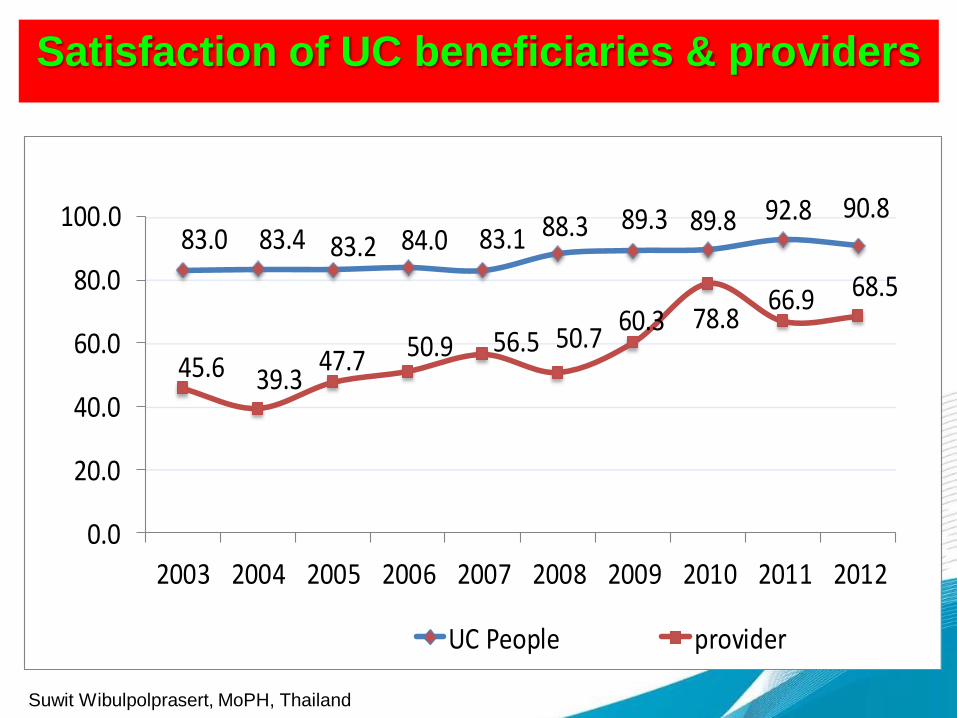
Satisfaction of UC beneficiaries & providers
Percent
Expand financial incentives to Health personnel
83.0 83.4 83.2 84.0 83.1 88.3 89.3 89.8 92.8 90.8
45.6 39.347.7 50.9 56.5 50.7
60.3 78.866.9 68.5
0.0
20.0
40.0
60.0
80.0
100.0
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012
UC People provider
Suwit Wibulpolprasert, MoPH, Thailand

The regional and global movements on UHC
• Countries with UHC - Brunei, China, Japan, Korea,
Malaysia, Singapore, Sri Lanka, Thailand, Brazil,
Mexico, Costa Rica, Chile, Cuba
• Asian countries committed - India, Indonesia, Laos
PDR, Maldives, Philippines, Vietnam, South Africa
• Joint Statement ASEAN plus three HMM – July 12
• UNGA resolution on UHC - December 2012
• UHC in the post 2015 and SDGs and ECOSOC 13
Suwit Wibulpolprasert, MoPH, Thailand

The UNGA resolution on UHC
• Include UHC in the discussion on the post 2015
development agenda
• ECOSOC consider UHC as part of its 2013 work
programs with WHO n WB – July 3rd 2013
• Continue consultation on UHC and possibility of a
HLM in UNGA – indicators and targets of UHC
developed by WHO and WB in September 2013
• UNSG and UN agencies to give high priority to UHC
Suwit Wibulpolprasert, MoPH, Thailand

The Role of Countries to move UHC
• Target UHC and move concretely and actively to
achieve it thru both HSS and HI development
• Global advocacy movement – to put UHC as the
post 2015 and the Sustainable Development Goals
• Capacity building (INNE) thru Knowledge
management – the Japan-WB trust fund on UHC,
the Joint Learning Network (JLN), the ASEAN plus
three UHC networks, the AAAH, the HTAsiaLink,
and the Thai CAP UHC program
Suwit Wibulpolprasert, MoPH, Thailand