glaucoma workup review: from a to oct dr. nathan rains eye center of northern colorado
TRANSCRIPT
Glaucoma Workup Review: from A to OCT
Dr. Nathan Rains
Eye Center of Northern Colorado

What is Glaucoma?
3 million Americans have glaucoma
One of the leading causes of adult blindness
No symptoms until extensive peripheral vision loss (for most types of glaucoma)
“sneak thief of sight”
Chronic condition, no cure, just control
Control is lower eye pressures by
Eye drops, laser surgeries, or medical surgeries

What is Glaucoma?Prevalence
http://www.nei.nih.gov/eyedata/glaucoma.asp#1

What is Glaucoma? Definition
... optic neuropathy with associated visual function loss, with intraocular pressure (IOP) being one of the primary risk factors...
American Academy of Ophthalmology
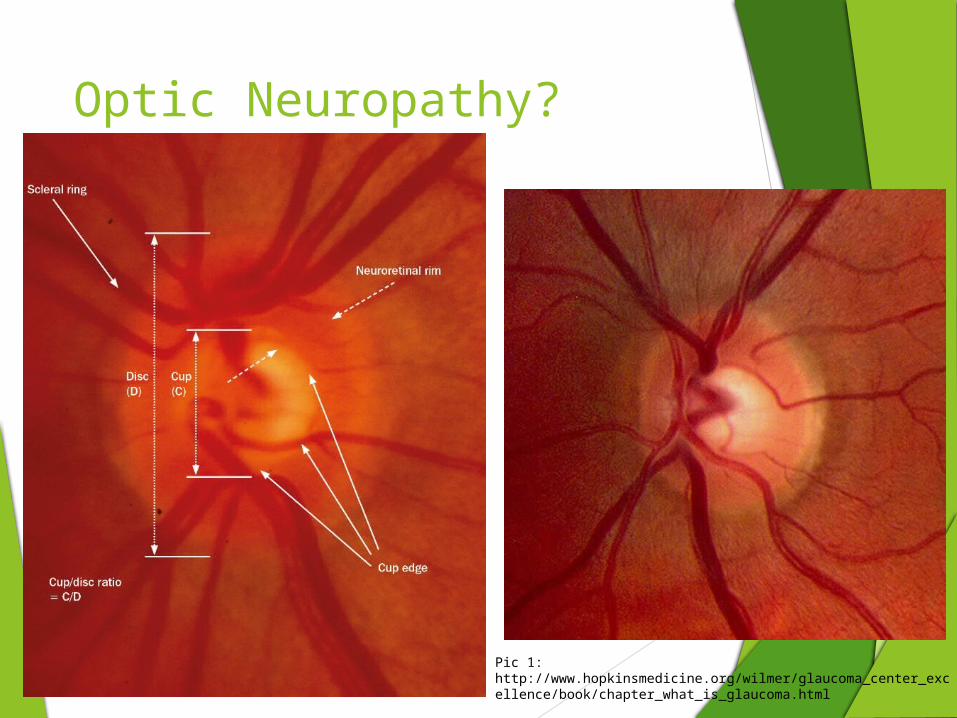
Optic Neuropathy?
Pic 1: http://www.hopkinsmedicine.org/wilmer/glaucoma_center_excellence/book/chapter_what_is_glaucoma.html
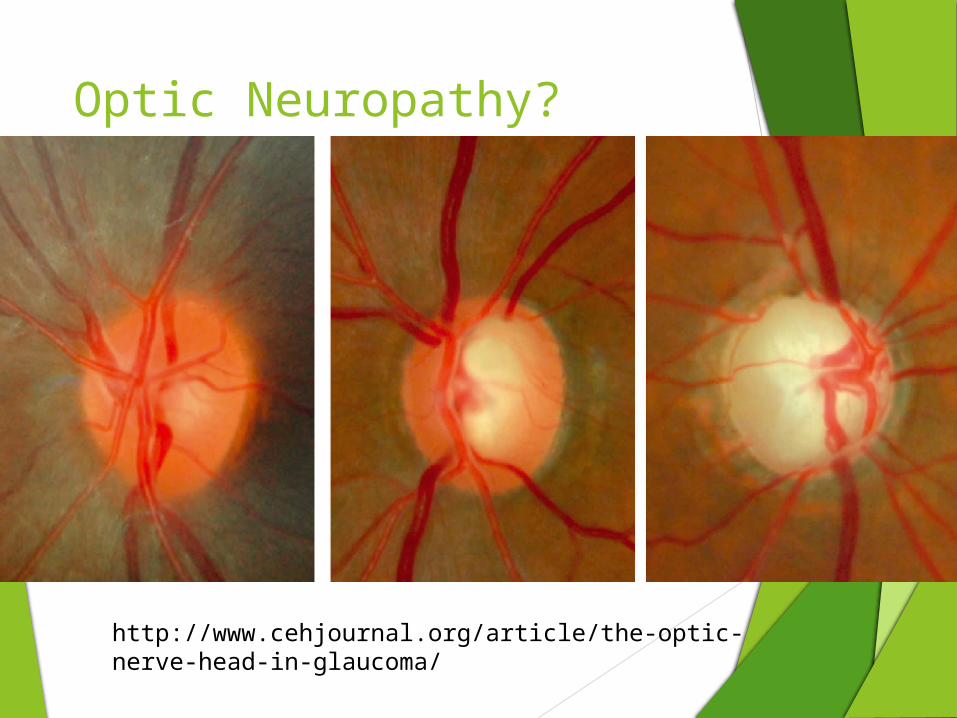
Optic Neuropathy?
http://www.cehjournal.org/article/the-optic-nerve-head-in-glaucoma/
Goals of Glaucoma Testing
The ultimate goal of glaucoma testing is three fold: To Diagnose Glaucoma (probably the hardest step)
Is the test RELIABLE
Is the test REPEATABLE
To Determine its Severity
Suspect, mild, moderate, severe
Initiate treatment, set appropriate target pressures, etc.
To Monitor Progression

Glaucoma Testing
Tonometry Pachymetry Gonioscopy Tomography Perimetry *Biomicroscopy *Photography *Corneal Hysteresis *Ganglion Cell Complex


What is Tonometry?
The measurement of intraocular pressure (IOP) recorded in mmHg
Normal IOP – 10-20 mmHg (avg ~ 16mmHg)
Ocular hypertension - >20-22mmHg
Diurnal fluctuations – 4-6 mmHg
Pressure is highest at night, in the supine position (3 am)
Difference between eyes – 2-3 mmHg
>4-6 is suspicious
Only treatable measure of glaucoma
All medicine and surgery is geared to this one task, lower IOP
Tested at every examination and followup care
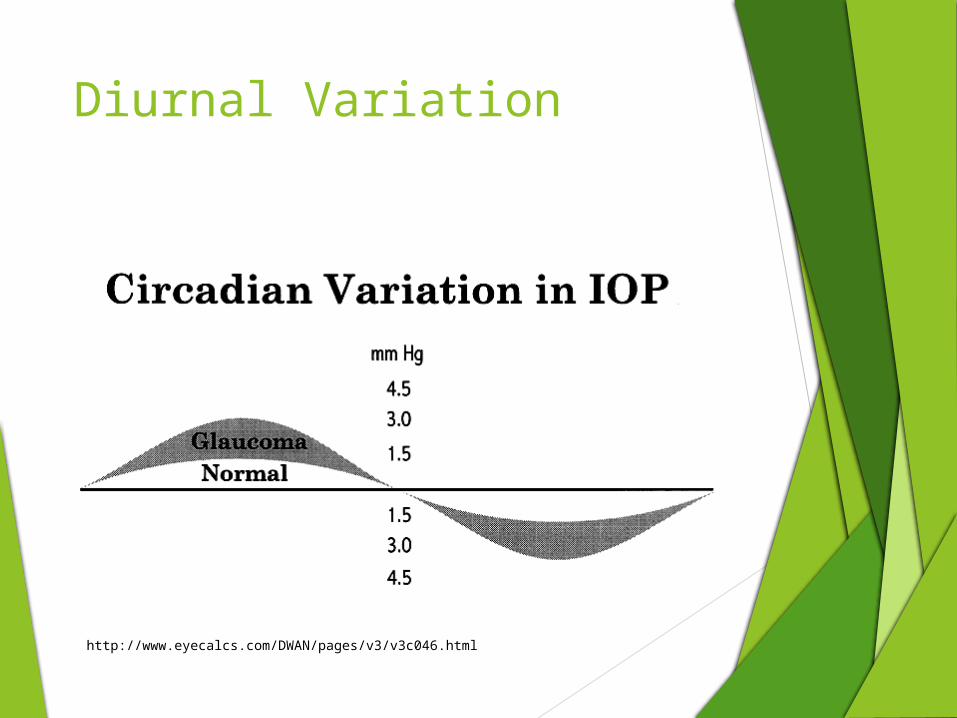
Diurnal Variation
http://www.eyecalcs.com/DWAN/pages/v3/v3c046.html
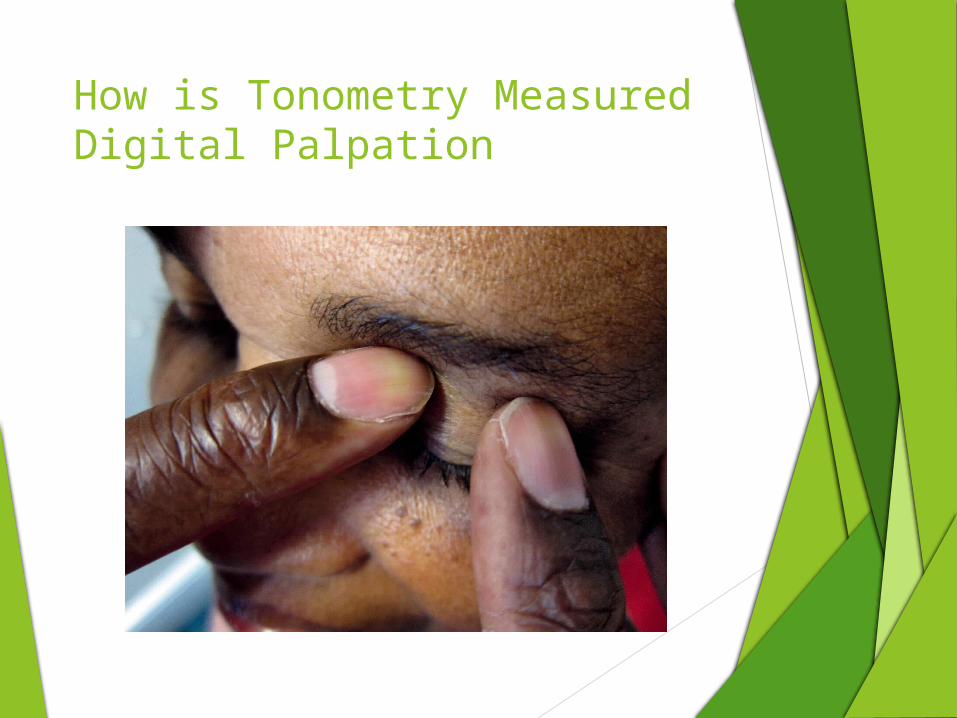
How is Tonometry MeasuredDigital Palpation

Tonometry InstrumentsIndentation – iCare & Tonopen
http://www.icaretonometer.com/rebound-technology/Good 38 sec video

Tonometry InstrumentsNon-Contact Tonometry
Advantages
No anesthesia
*No contact
Ease of use
Quick
Disadvantages
Patients 'love' to hate this test
Accuracy?

Tonometry Instruments Goldmann Applanation Tonometry
Gold standard
Accurate
Inexpensive
easy to use
Disadvantages
Anesthesia
still dependent on corneal properties
Tonometry Instruments
Take homes
Digital
basic, only detects extremely high pressures
Indentation
portable, cheap, supine
Non-contact tonometry
expensive machine, touchless, quick, patient discomfort
Applanation
gold standard, inexpensive, easy to use, less variability
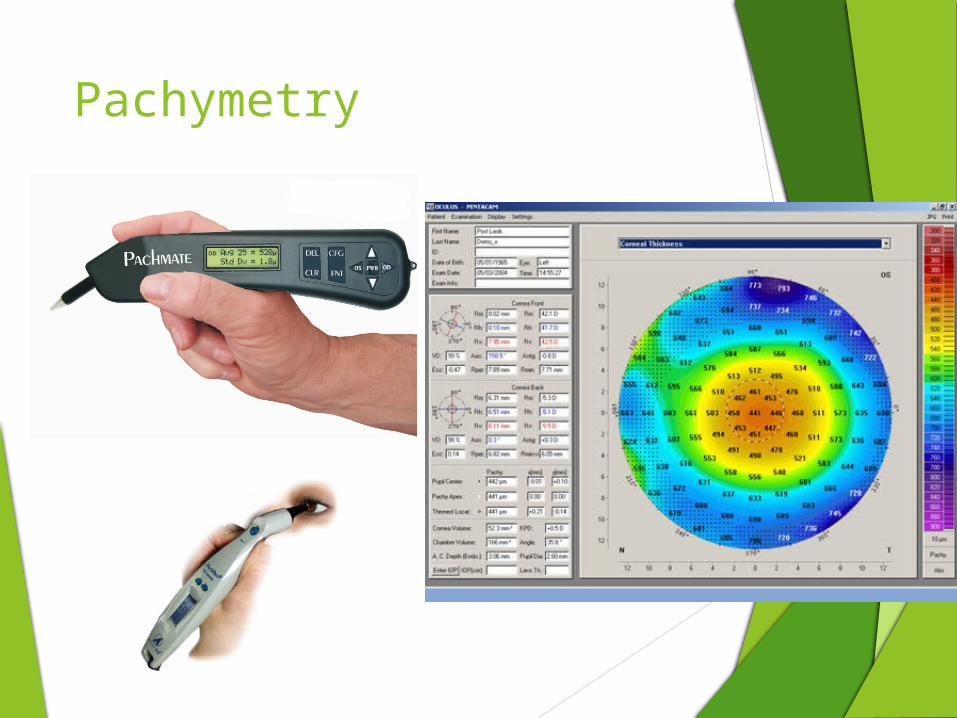
Pachymetry

What is Pachymetry?
The measurement of corneal thickness, in microns (um)
Average CENTRAL corneal thickness ~ 555 um
In glaucoma, used as a risk factor in the development of glaucoma Ocular Hypertensive Treatment Study (OHTS)
CCT <555, high risk
CCT 555-585 no increased risk
CCT >585 low risk

Pachymetry and IOP correction table?
Theory
The thicker the cornea, the artificially high reading
The thinner the cornea, the artificially low reading
IOP correction table? 1975 study
Every 100um adjust by 7mmHg
17 other studies, all different IOP per 100um adjustment… no consensus
Reason Thickness of cornea is only one part of it:
Corneal properties (steep/flat, hysteresis (stiffness), etc.)

Center of cornea
Compare symmetry (>30, repeat)
LASIK/PRK?
Diseased Corneas?
Fuchs, keratoconus?
Used as a RISK factor
No universal agreement on IOP correction table to use
So, we do NOT adjust IOP measurement
Pachymetry Pearls
Goals of Glaucoma Testing
The ultimate goal of glaucoma testing is three fold: To Diagnose Glaucoma (probably the hardest step)
Is the test RELIABLE
Is the test REPEATABLE
To Determine its Severity
Suspect, mild, moderate, severe
Initiate treatment, set appropriate target pressures, etc.
To Monitor Progression
What is Glaucoma?By Type
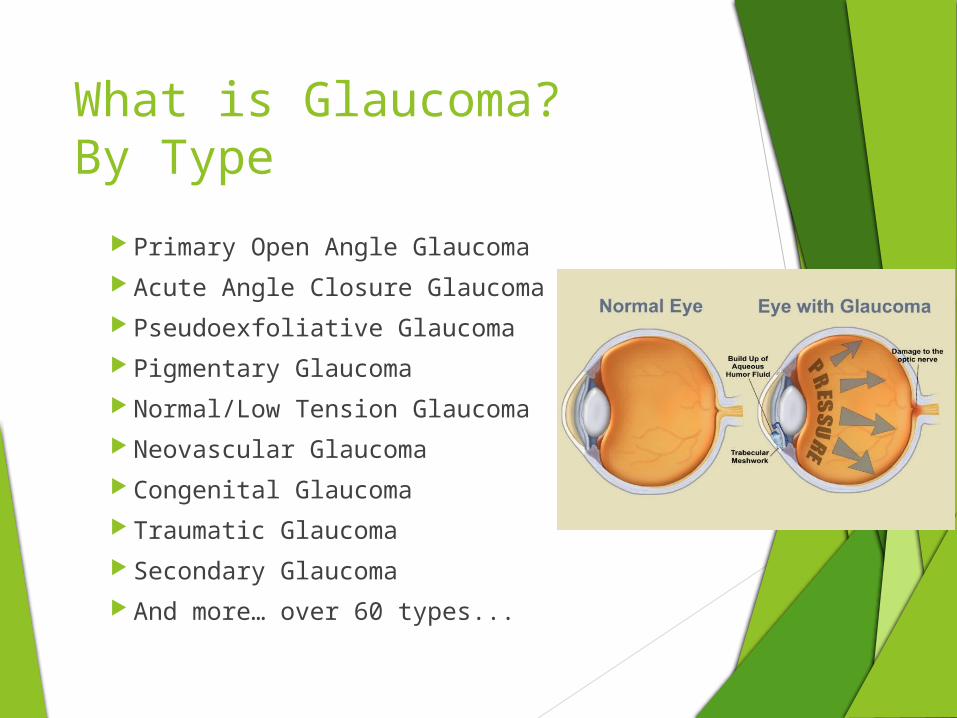
Primary Open Angle Glaucoma Acute Angle Closure Glaucoma Pseudoexfoliative Glaucoma Pigmentary Glaucoma Normal/Low Tension Glaucoma Neovascular Glaucoma Congenital Glaucoma Traumatic Glaucoma Secondary Glaucoma And more… over 60 types...
Gonioscopy
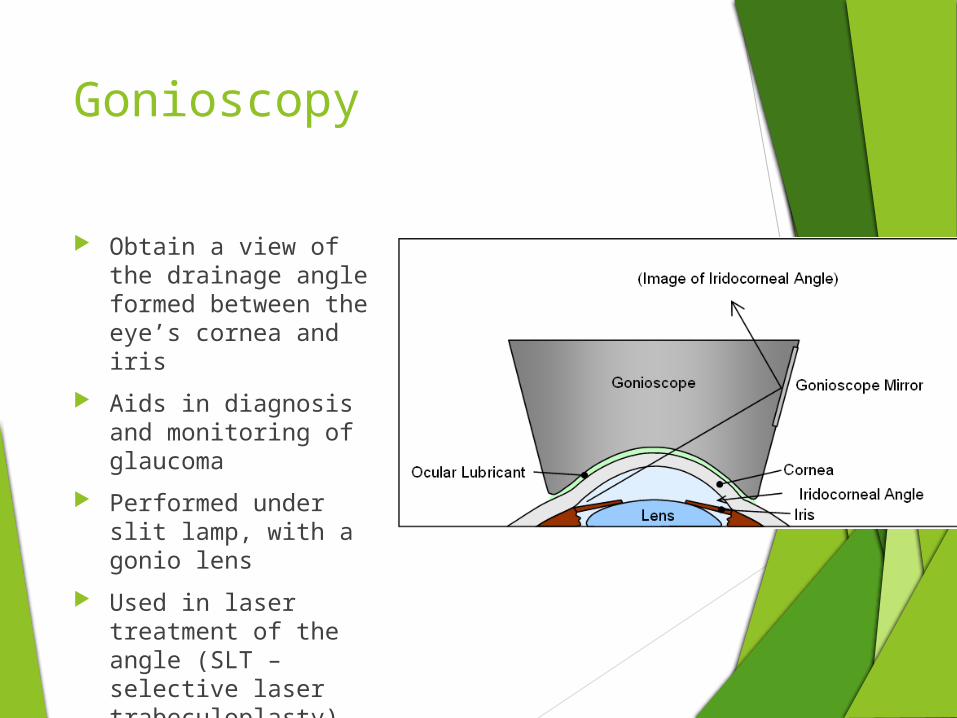
Obtain a view of the drainage angle formed between the eye’s cornea and iris
Aids in diagnosis and monitoring of glaucoma
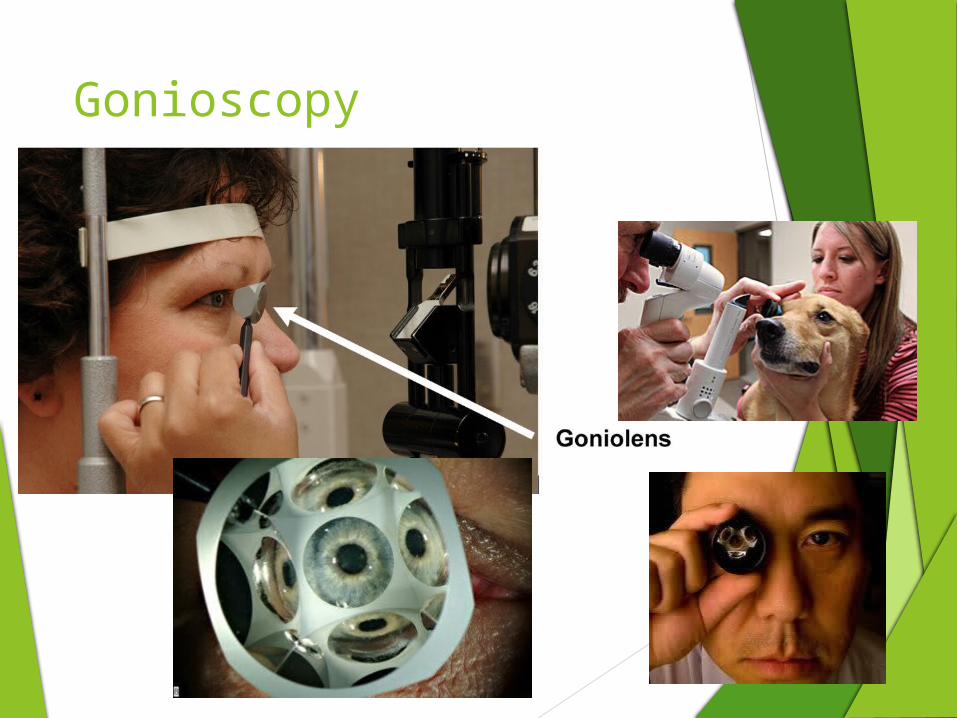
Performed under slit lamp, with a gonio lens
Used in laser treatment of the angle (SLT – selective laser trabeculoplasty)
Gonioscopy

Gonioscopy.org Video Clip
Can’t See That Stupid Line
Normal angle
Pigmented Angle
http://www.academy.org.uk/tutorials/gongrade.jpg
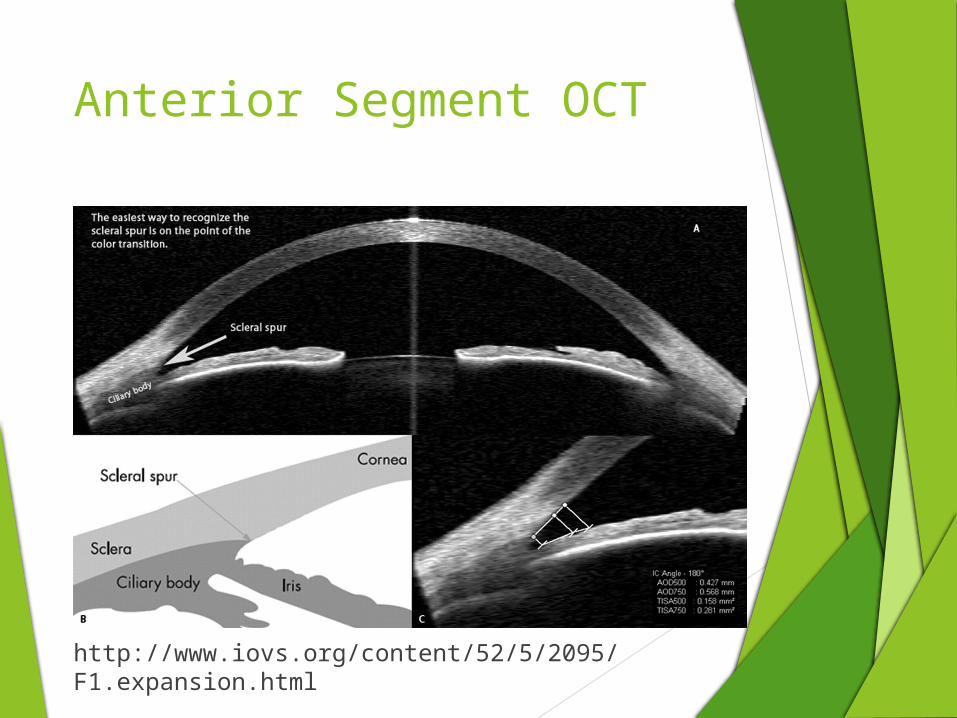
Anterior Segment OCT
http://www.iovs.org/content/52/5/2095/F1.expansion.html
GonioscopyTake home
Helps diagnose and determine type of glaucoma
Check out gonioscopy.org
Glaucoma Testing
Tonometry Pachymetry Gonioscopy Tomography Perimetry *Biomicroscopy *Photography *Corneal Hysteresis *Ganglion Cell Complex

Optic Neuropathy?
http://www.cehjournal.org/article/the-optic-nerve-head-in-glaucoma/
Optical Coherence Tomography
Non-invasive, high resolution, imaging technology
Time Domain vs Spectral Domain
TD – 400 scans per sec, 10um
SD – 20,000-40,000 per sec, 3um
3-D reconstructions
AWESOME!
Scan types
Retinal (macular)
Optic Disc
http://www.docvadis.fr/aobeffroi/page/l_oeil_et_les_examens/les_machines_utilisees_par_l_ophtalmologiste/oct_ou_tomographie_en_coherence_optique.html
OCT Optic Disc
Scans the optic disc using a 6mm cube
Obtains Retinal Nerve Fiber Layer Thickness
Color codes a thickness map
‘hour glass’ appearance
Red (350um), to blue (0um)
Normative table
RNFL thickness
Symmetry
C/D ratio
Etc.
RNFL TSNIT Map
Quadrant and Clock Hour RNFL thickness chart
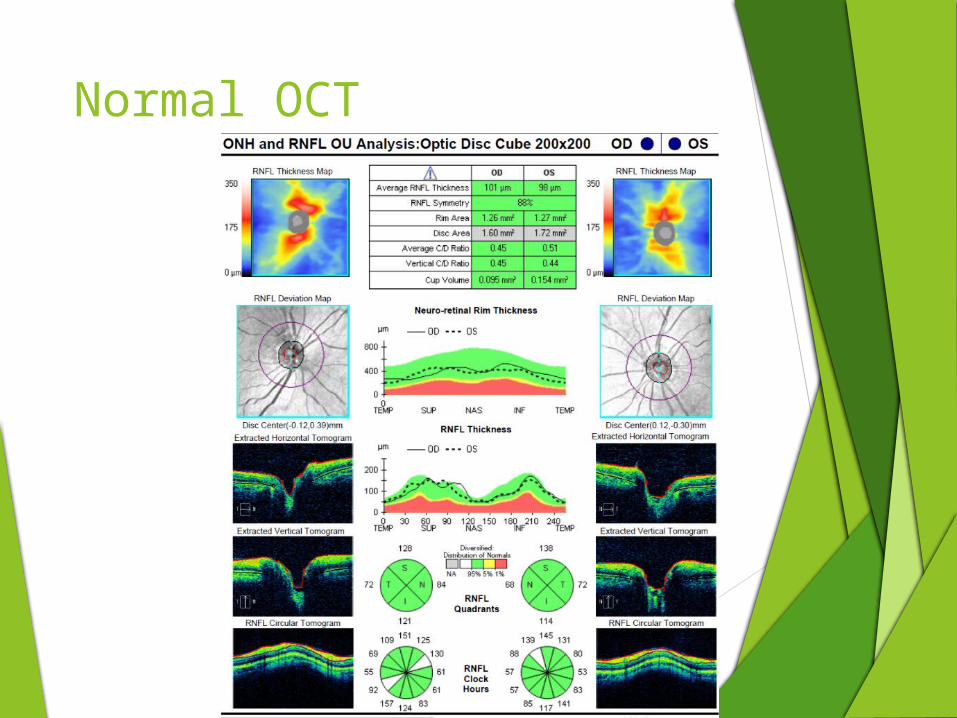
Normal OCT
OCT Optic DiscDiagnosing Glaucoma
Average RNFL
Symmetry
>20um difference is statistically significant
Quadrant RNFL layout
Inferior and Superior are the greatest indicators
Clock Hour RNFL layout
Inferior temp and/or superior temp thin
Lastly – does it correlate with the visual field
***structural loss precedes VF loss***

OCT optic discExample

OCT Optic DiscMonitoring Glaucoma
Average NFL
Symmetry
Progression Analysis
http://www.healio.com/ophthalmology/journals/osli/2011-7-42-4-supplemental/%7Bde06c09a-2d95-42f4-b403-2fc1fa6a3550%7D/clinical-use-of-oct-in-assessing-glaucoma-progression
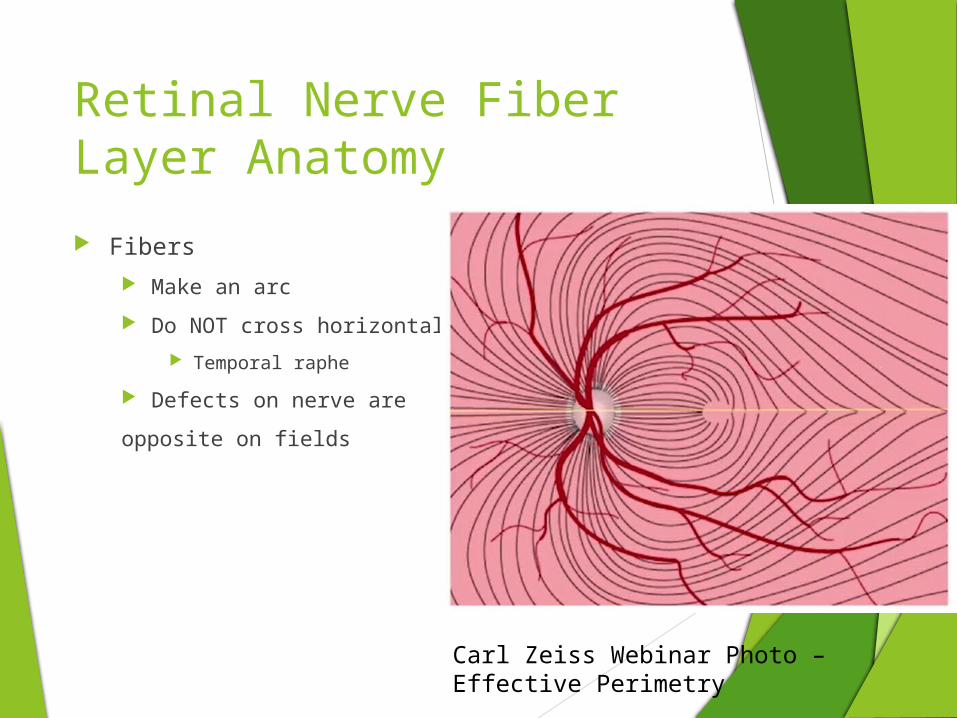
Retinal Nerve Fiber Layer Anatomy
Carl Zeiss Webinar Photo – Effective Perimetry
Fibers
Make an arc
Do NOT cross horizontal axis
Temporal raphe
Defects on nerve are
opposite on fields

PerimetryAutomated Visual Field
Automated Perimetry for Glaucoma
Types of tests used
30-2, 24-2, and 10-2
Strategies used
SITA Standard, SITA Fast

Visual Field
Types: 30-2, 24-2, 10-2 1st number refers to the degrees AROUND
fixation Ex: 10-2 – 10 degrees around the fovea (20 degrees total)
2nd number refers to the protocol Protocol 1 – points directly on the horiz and vert axis
Protocol 2 – points directly above and below axis
Easier to interpret and used exclusively now
Points tested 30-2 – 6 degrees apart, total points 76, ~8 min per eye
24-2 – 6 degrees apart, total points 54, ~5 min per eye
10-2 – 2 degrees apart, total points 54

30-2 vs 24-2?
24-2 advantagesFaster time (~5 min per eye)Less variableSimilar results
30-2 advantagesMore degrees of field tested
May help detect/monitor neurological defects, ie. Idiopathic intracranial hypertension
SITA Standard vs SITA Fast
SITA Standard
Best threshold test
Better for early detection in glaucoma
More reliable, more sensitive
SITA Fast
Fast(er)
Can be used for screening purposes
More Variable, less sensitive (underestimates) scotomas

When to use 10-2 in Glaucoma?
Previously, used exclusively in severe peripheral field loss
24-2 not providing enough information to monitor progression, so 10-2 replaces 24-2
Recently, published in the JAMA Ophthalmology, January 2014, 10-2 VF testing was found to detect early glaucomatous defects missed on 24-2
Of 22 eyes tested as normal on 24-2 testing, 22.7% were abnormal in 10-2 testing
May use 10-2 in addition to 24-2

Automated PerimetryGlaucoma VF Types
Types
Nasal Step
Arcuate
Paracentral
Severity
Mild to Very Severe
http://www.medrounds.org/glaucoma-guide/2006/02/section-1-c-understanding-vision-loss.html
Visual FieldDiagnosing Glaucoma
Reliability Fixation losses, false positive, false negatives, etc.
Repeatability When there’s a defect, is it repeatable?
Three consecutive fields to reliably confirm glaucoma*
Global Indices GHT – glaucoma hemifield test
MD – Mean Deviation
PSD – Pattern Standard Deviation
VFI – Visual Field Index (percentage)
*Keltner et al. for the Ocular Hypertenstion Treatment Study Group, Arch Ophthalmol 123:1201 (2005)
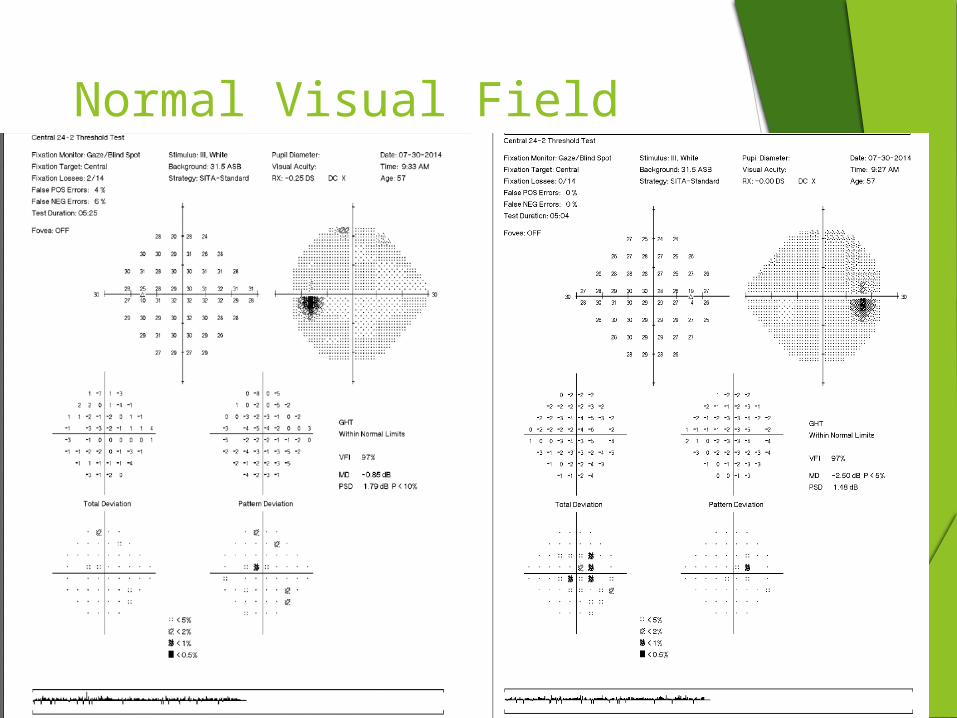
Normal Visual Field

Visual Field - Glaucoma
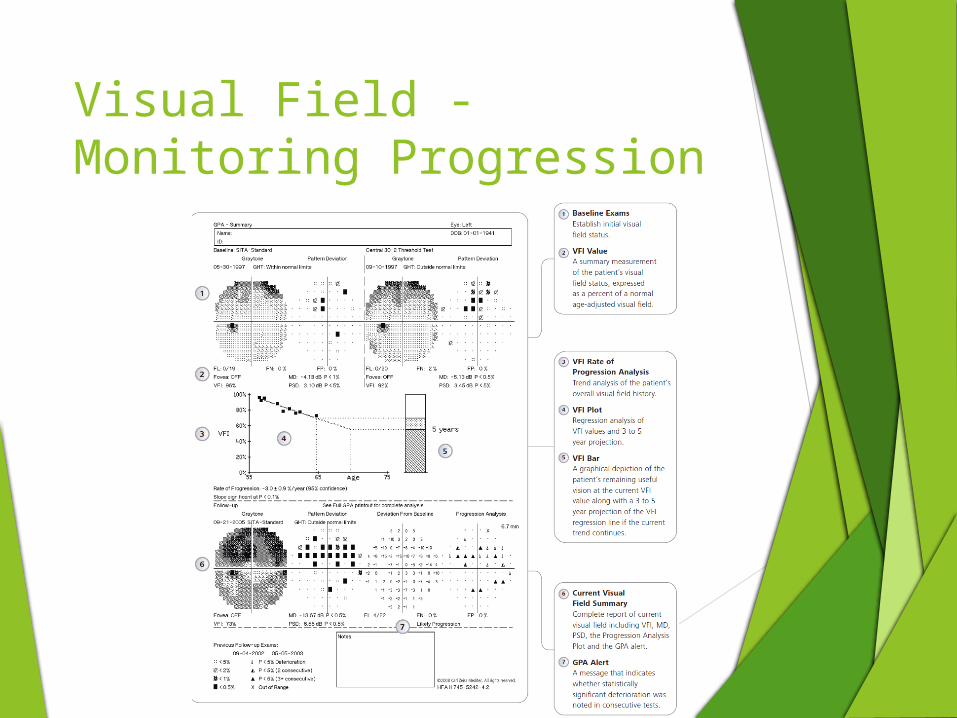
Visual Field - Monitoring Progression

Visual Field/OCT Integration

Visual Field/OCT Integration

Glaucoma Workup Review
The End! Questions?