giving sbar report
TRANSCRIPT

Giving SBAR
ReportSituation
Background
Assessment
Recommendation

What is SBAR?
SBAR is an acronym for a standardized
method of giving report between
healthcare providers
S: Situation
B: Background
A: Assessment
R: Recommendation

Why SBAR? Improving Safety
The Institute of Medicine report To Err is Human (1999) challenged healthcare workers to examine several preventable errors that lead to poor patient outcomes
Communication failure was listed as one of the errors that can be prevented
SBAR standardizes the way patient information is communicated between healthcare providers, decreasing the likelihood that important information is missed during transitions of care

Why SBAR?
Improving Communication
Joint Commission National Patient Safety
Goal 2: Improve the effectiveness of
communication among caregivers
The Joint Commission’s Transition of Care
(2012) report revealed communication
breakdowns to be one of the root causes of
ineffective patient transitions and poor
patient outcomes

Barriers to Effective
Communication
Caregivers have differing expectations of
what to expect in report
Organizational cultures that do not
promote successful handoffs
Inadequate amount of time to give a
detailed handoff report
Lack of standardization of handoff reports
Why SBAR? Improving Collaboration
The ANA Code of Ethics calls nurses to collaborate with all members of the healthcare team
Collaboration requires “mutual trust, recognition and respect…shared decision making…and open dialogue…”(Provision 2.3) among all members of the healthcare team
The use of SBAR reporting standardizes communication allowing the healthcare team to focus their efforts on developing a multidisciplinary plan of care instead of gaps in communication

Breaking it DownWhat it all means…
S: Situation
What is going on?
What is the patient’s name?
Why is the patient coming for treatment?
How did they obtain the wound?
How long have they had the wound?
How is the patient currently treating their
wound?
Example #1: Mr. P. Mr. P., 27yo, is here for a periorbital laceration that he
sustained in a fight 10 days ago He was originally admitted to the hospital for treatment
and was discharged with instructions to follow up with his PCP or Patient First to have the stitches removed
When he went to Patient First two days ago, the physician there refused to remove the stitches because he suspected infection
The Patient First physician prescribed Bactrim and told him to make an appointment with the wound center.
He is currently treating the wounds with antibiotic ointment and gauze
He changes his dressings once a day

B: Background What is the pertinent history?
Include only relevant information
Patient’s PCP, brief social background
Lives alone, nursing home, home care, homeless, etc.
Patient’s medical/surgical history
Diabetes, PVD, PAD, malignancies, obesity, DVT, etc.
Allergies
Especially to medications/products that are commonly used to treat wounds
Sulfa, PCN, silver, iodine, etc.
Medications that may effect the patient’s ability to heal or the way the physician can treat the patient
Steroids, chemotherapy, anticoagulants, illicit drug use, smoking, ETOH, etc.
Recent labs, wound cultures, biopsies, radiology reports, vascular testing, etc.
Be as specific as possible; include dates, actions taken
Example #1: Mr. P. Mr. P. does not have a PCP He has a history of methamphetamine and IV heroin abuse
He states that it has been 47 days since he last used either drug
He reports that he recently completed a stay in rehab and regularly attends NA meetings
He has no other medical history
Mr. P. is on his 3rd day of Bactrim He is also taking Tramadol for pain
He takes no other medications
A hospital x-ray of Mr. P’s face was negative for any fractures
No wound culture was taken at the Patient First before he was prescribed his antibiotic
A: Assessment
What are your assessment findings?
How many wounds are there?
What are their sizes?
May generalize if multiple wounds
Are there any causes for concern?
s/s infection, dehiscence, pain, malodor, etc.
Example #1: Mr. P. Mr. P.’s wound is on his L lower periorbital region
It measures 3.2 cm x 0.4 cm x 0.3 cm
The sutures are intact at the distal portion of the wound The wound has started to dehisce at the proximal portion
The wound is mostly yellow slough with a small amount of red granulation tissue
The wound has a moderate amount of non-purulent serosanguinous drainage
There is no odor but there is erythema, increased warmth and edema of the periwound
The patient also c/o 8/10 wound pain Constant wound pain of 4-5/10
Mr. P. is not running a fever and he is not complaining of chills or body aches

R: Recommendation
What do you think the next course of action should be?
Are any diagnostic tests or labs needed?
Does the wound need to be debrided?
Will the patient need home care to help with management of the wound?
What kind of dressing do you anticipate the patient needing?
What are the educational needs of the patient/caregiver?

Example #1: Mr. P. The wound looks like it should probably be debrided
I also think that we should take a culture of the wound since one has never been done and the wound does not appear to be responding to the Bactrim
Since the wound appears infected and is producing a moderate amount of drainage Aquacel Ag may be a good choice for a dressing since it is absorptive and antimicrobial
Mr. S. can be taught how to perform his dressing changes and is physically able to do so I do not anticipate him needing any skilled nursing care

Your TurnHow would you give an SBAR report on a patient?
SBAR Assignment Imagine that Mr. S. has come to the wound
center as a new patient for treatment of his wounds
The information on the next few slides is what you learned about him during your initial assessment
Use the Wound Healing Center SBAR Report Sheet to help you organize your report
Bring completed SBAR Report Sheet to your one-on-one meeting with Ore
Mr. S.: Patient Profile Mr. S., 43yo police officer
injured in the line of duty
After being nearly paralyzed
he is now unable to walk
without assistance
Height: 5’7”
Weight: 215 lbs
Spends majority of his day in
bed or sitting in his
wheelchair
PCP: Dr. Saul Goodman
Pharmacy: Boetticher
Pharmaceuticals
History:
Obesity, high blood pressure, high cholesterol, diabetes, PTSD, cholecystectomy 10 yrs. ago, L leg DVT w/ IVC filter placement 2 mos. ago
Recent diagnostics:
HbA1c 10.3
AM finger stick 279
INR 2.6
Current medications:
Metoprolol, Janumet, Lipitor, Lantus, Percocet, Colace, MVT, Coumadin

Mr. S.: Patient Profile Social history
Occasional cigar smoker
Used to drink 1-2 beers after work since the accident now drinks up to a 6-pack/night
Recently began refusing to participate with his physical therapy
He is receiving physical therapy and skilled nursing care in his home
Living conditions Lives at home with his
wife, no children
Juan Tabo Home Health provides skilled nursing and PT
Hospital bed with a regular mattress
Wheelchair with a pillow in the seat for padding
Rolling walker
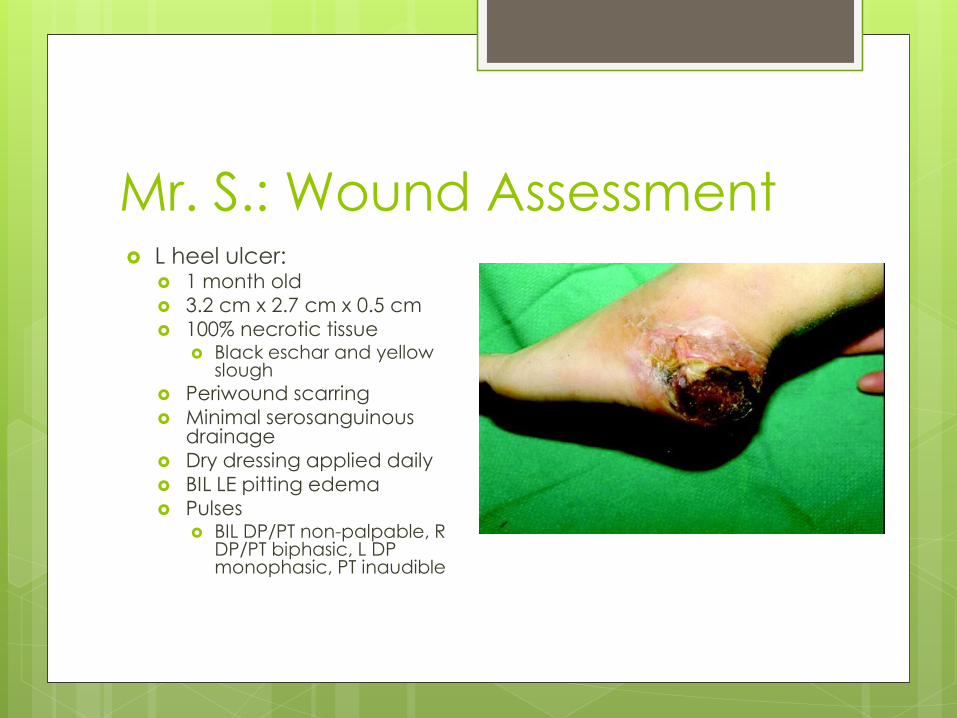
Mr. S.: Wound Assessment L heel ulcer:
1 month old
3.2 cm x 2.7 cm x 0.5 cm
100% necrotic tissue Black eschar and yellow
slough
Periwound scarring
Minimal serosanguinousdrainage
Dry dressing applied daily
BIL LE pitting edema
Pulses BIL DP/PT non-palpable, R
DP/PT biphasic, L DP monophasic, PT inaudible
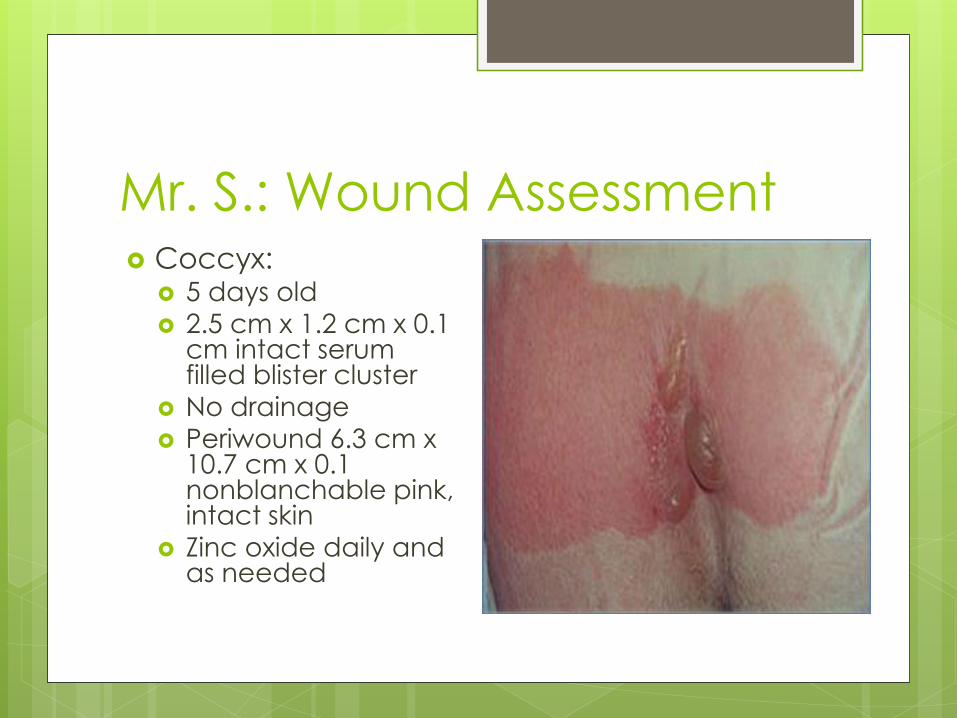
Mr. S.: Wound Assessment Coccyx:
5 days old
2.5 cm x 1.2 cm x 0.1 cm intact serum filled blister cluster
No drainage
Periwound 6.3 cm x 10.7 cm x 0.1 nonblanchable pink, intact skin
Zinc oxide daily and as needed
References American Nurses Association. (2001). Code of ethics for nurses with
interpretive statements. Retrieved from http://www.nursingworld.org/MainMenuCategories/EthicsStandards/CodeofEthicsforNurses/Code-of-Ethics.pdf
Institute of Medicine. (1999). To err is human: Building a safer health system.Retrieved from https://www.iom.edu/~/media/Files/Report%20Files/1999/To-Err-is-Human/To%20Err%20is%20Human%201999%20%20report%20brief.pdf
The Joint Commission. (2012). Transitions of care: The need for a more effective approach to continuing patient care. Retrieved from http://www.jointcommission.org/assets/1/18/hot_topics_transitions_of_care.pdf
Kaiser Permanente. (n.d.). Guidelines for communicating with physicians using the SBAR process. Retrieved from file:///C:/Documents%20and%20Settings/oreezi/My%20Documents/Downloads/SBAR%20Guidelines%20Kaiser%20Permanente%20(2).pdf
Narayan, M.C. (2013). Using SBAR communications in efforts to prevent patient rehospitalizations. Home Healthcare Nurse,31(9), 504-515 doi: 10.1097/NHH.0b013e3182a87711