git f bs
TRANSCRIPT
Upper Gastrointestinal Foreign Bodies
Dr. Mohammad Shaikhani.

Case history:
13 years girl presented to the endoscopy unit with H/O ingesting a pin during trial to hold a pin between her teeth before 24 hours.
No previous H/O FB ingestion. No H/O psychiatric diseases.
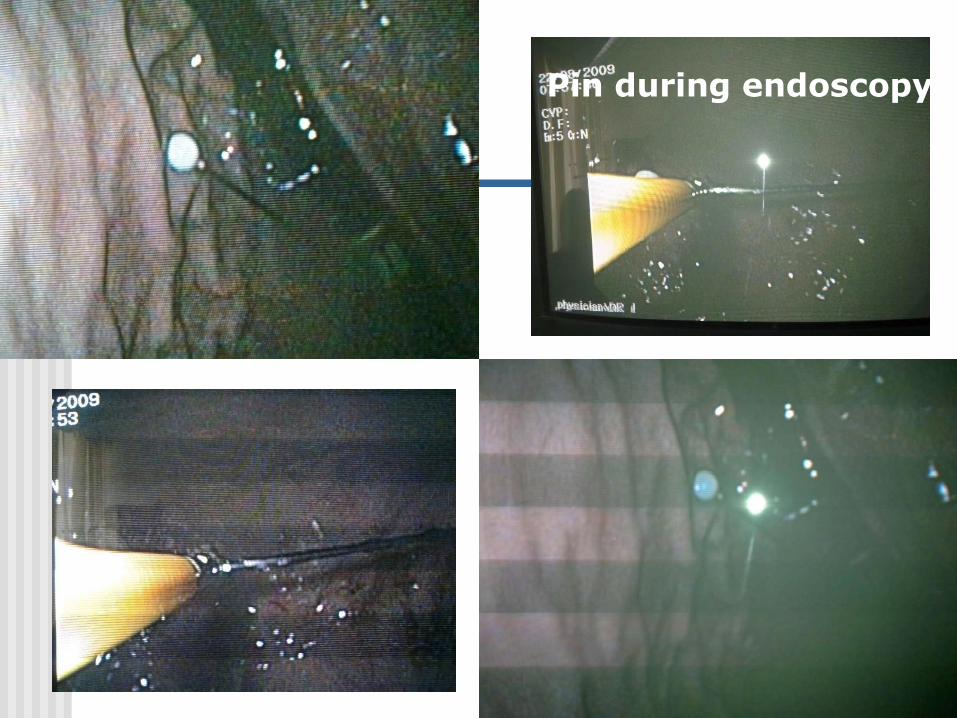
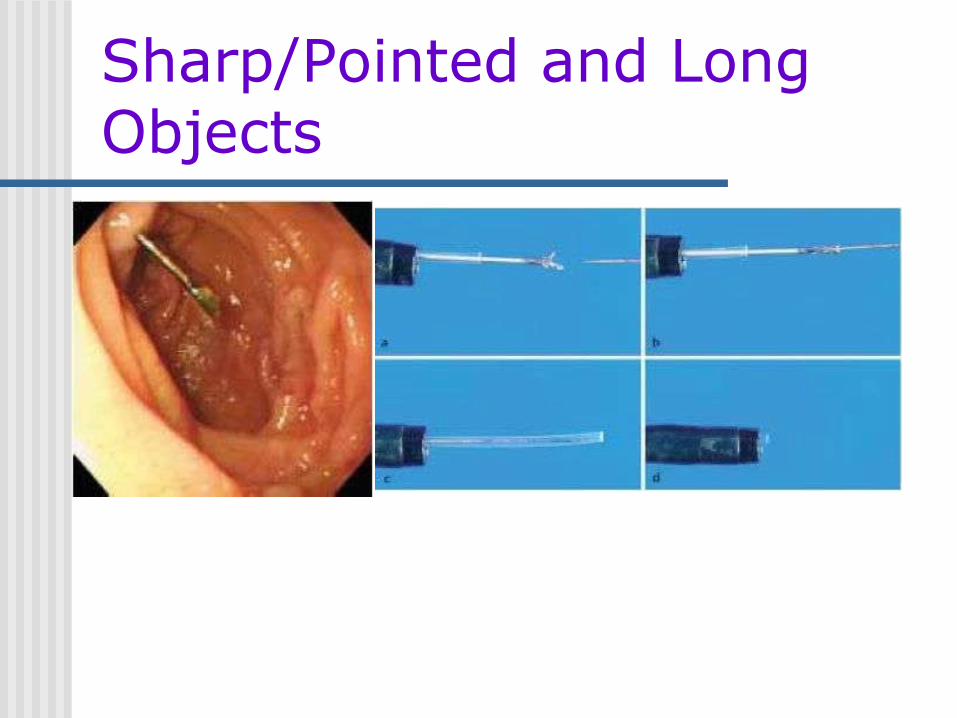
Pin during endoscopy:

Pin retrieved by endoscopy:
International j of clinical practice 2006
GIT FBs represent a significant clinical problem in the Emergency Department, causing a high degree of financial burden, morbidity and mortality. A large variety of foreign bodies are accidentally ingested or inserted into the GIT in different age groups.
This a retrospective review of 38 patients presented to ERT with GIT FBs between January 2001 and December 2004.
30 males/ eight females (M: F ratio of 3.75:1) with an age range of 10 months to 87 years (median age 25.5 years), accidental in 14 , deliberate in 11, for anal erotism in 11 &assault in two cases. The median time before presentation was 12 h, mean length of hospital stay was 1.7 days.
Treatment was conservative in 15 patients; five patients had gastroscopic retrieval; 15 patients underwent examination under anaesthetic, retrieval and proctosigmoidoscopy and three patients underwent laparotomy for impacted foreign bodies. GIT foreign body ingestion or insertion is common; however, majority of cases can be successfully managed conservatively.

Common >100 000 /year, 80% in children, with a peak incidence between 6 months-3 years.
The type/frequency varies in different geographical regions& by the medical specialty reporting the ingestion. Majority of ingestions are accidental in children, often
witnessed by an adult caregiver. Ingestions in adults are more often intentional associated
with psychiatric disturbance, alcohol consumption& incarcerated adults seeking the relative comforts of medical facilities.
Most blunt ingested objects pass through the GIT without incident, but sharp objects, 5–30% of swallowed objects, pose a more serious threat of perforation.
In Asia, where the ingestion of fish is more common, fish bones may become lodged as they pass& account for a greater fraction of reported ingestions in adults &children.
The most common reported ingestion in children in US/Europe is coins, 80% In adults, meat impaction is the most common cause of accidental ingestion,
usually associated with underlying pathology such as esophageal stricture or eosinophilic esophagitis.
Other causes of accidental ingestions in adults include tooth brushes, used to induce vomiting in patients with eating disorders.
Sharp &multiple objects are typically swallowed intentionally. Recent adolescent gang activity includes the practice of the ingestion of a
foreign body as part of an initiation ritual.

80–90% pass spontaneously, 10–20% require endoscopic removal, <1% require surgical intervention.
Sharp objects have a much higher perforation rate, ranging from 15 to 35%. Some objects require special attention, including small magnets, which have become popular building materials in children’s toys& the ingestion of button batteries.
One of the most serious intentional ingestions is small packets of drugs, which are usually swallowed to transport the illegal substances from one location to another.
Once in the stomach, most foreign bodies pass without incident. Some large objects will predictably fail to pass the pylorus, and others will fail
to negotiate the duodenal sweep. In these patients early endoscopic intervention is indicated to avoid later
surgery.

The routine management of coin ingestion if it is passed into the stomach is to wait 2–3 weeks and repeat an abdominal radiograph if the coin has not been observed in the stool .
Alternatively, metal detectors have been used to avoid radiation exposure and monitor the passage of coins.
If the child remains asymptomatic, some physicians will wait an additional 2–3 weeks before removing the coins.
Ovoid objects >2cm by 5cm in adult-sized individuals have difficulty passing through the pylorus&are typically removed when discovered.
if an object is greater than 1cm by 3cm in a child we recommend removal. If watchful waiting does not lead to passage within 2–3 weeks in the stomach,
endoscopic removal is typically recommended. If patients are symptomatic, regardless of the size of the object in the stomach,
they should be retrieved.

Long objects have difficulty negotiating the duodenal sweep& should also be removed.
In adult patients, objects greater than 10 cm in length are routinely removed from the stomach rather than allow them to pass the pylorus&risk becoming lodged in the duodenum.
Ingested batteries are serious because they can alkaline caustic material causing mucosal ulceration,mercury poisoning, lithium absorption.
In symptomatic patients batteries should be removed regardless of battery size or the age of the patient.

Sharp foreign bodies are more likely to be associated with complications. Perforation may occur anywhere in GIT, but is more common in areas of
angulation, including the C loop of the duodenum&ileocecal valve. Areas of congenital malformation or previous surgery are also more likely to
be associated with bowel perforation after ingestion. The risk of perforation rises with the number of objects ingested. The ingestion of any single magnet piece presents little risk, but two or more
magnets may pose a problem as they may attract across several layers of bowel leading to pressure necrosis, fistula formation, free perforation or obstruction.

Foreign bodies intentionally or unintentionally
inserted or ingested objects inadvertently ingested animal and
fish bones food bolus impactions
Epidemiology
children 80 percent of cases - pediatric population
a peak incidence : 6 months - 3 years
coins, keys, buttons, small toys, nails, pins,
thumbtacks, and disc batteries
Epidemiology
Adults patients with psychiatric disorders and
those seeking some secondary gain
the very elderly, the demented, the
intoxicated. with dentures and dental
bridgework

Pathophysiology
Complications
Bowel perforation and obstruction
bleeding, respiratory compromise,
fistulization, and abscess formation
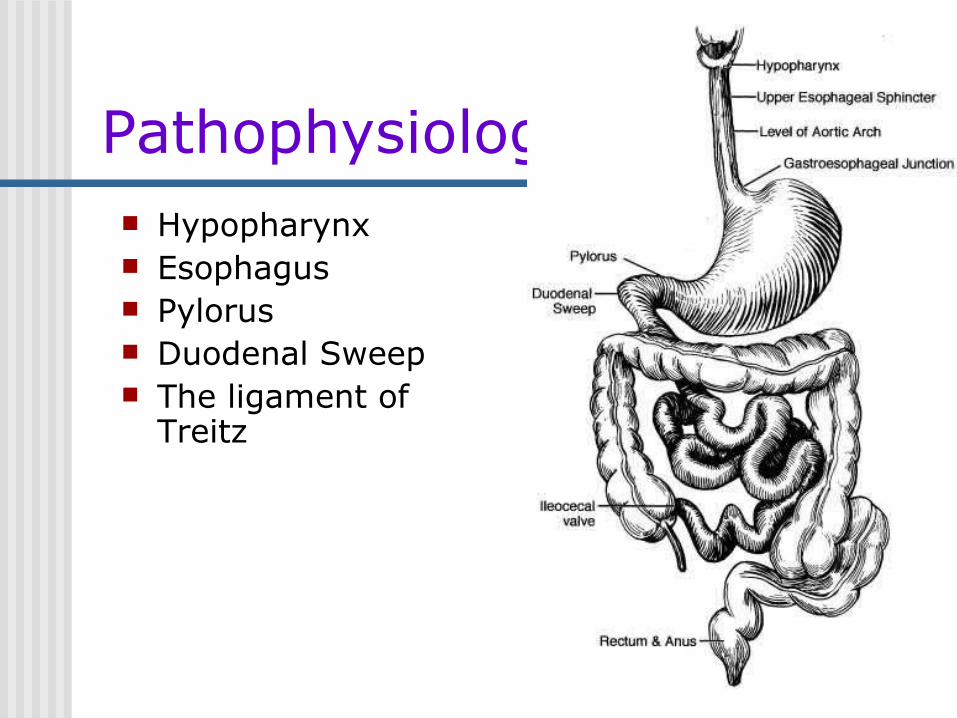
Pathophysiology Hypopharynx Esophagus Pylorus Duodenal Sweep The ligament of
Treitz

Diagnosis
History and Physical Examination Radiographic Studies Endoscopy
History and Physical Examination history of ingestion
onset of symptoms
physical examination unremarkable or nonspecific
recognize complications
Radiographic Studies The plain film of the chest and
abdomen
help determine the presence, type, and
location of the foreign body.
identifying possible complications

Radiographic Studies
Coin in esophagus

Radiographic Studies
The diagnostic capabilities of plain film are limited not all ingested objects are radiopaque False-negative rates 47% To children, hand-held metal detectors

Radiographic Studies
The role of contrast studies - limited(Barium esophagrams)
suspicion of perforation
complete esophageal obstruction

Endoscopy
diagnostic accuracy safe and effective therapy Endoscopy indication
when the history suggests a GIFB,
irrespective of a negative radiograph
Endoscopy
Emergent endoscopy is indicated
high-grade esophageal obstruction
esophageal foreign object or food bolus
impaction
suspected ingestion of sharp and pointed
objects.
Endoscopy
Endoscopy contraindicated
bowel perforation or small bowel
obstruction beyond the ligament
of Treitz
Treatment Indications and Timing for Therapy
Endoscopic Management
Surgery
Indications and Timing for Therapy symptomatic patients---
therapeutic intervention
asymptomatic patients--- location
and characteristics

Indications and Timing for Therapy
All GIFBs lodged in the esophagus -
an urgent basis ( longer than 24
hours )
Once an object has reached the
stomach - management can be
individualized

Indications and Timing for Therapy
In most cases of gastric foreign
body - conservative management Endoscopic retrieval is indicated
objects that fail to progress
Large objects (>2 cm in diameter)
long objects (>5 cm in length)
Sharp objects because their risk of
perforation (15 - 35%)
Indications and Timing for Therapy Surgery is indicated
evidence of perforation, hemorrhage, fistula
formation, obstruction secondary to a GIFB.
GIFBs fail to progress and/or cannot be
retrieved endoscopically.
Endoscopic Management
General Considerations success rates ranging from 90-100% Endoscopic extraction failures - the
number and type of object(s).
Endoscopic Management General Considerations
lodged at the hypopharynx -
laryngoscope
Rigid esophagoscopy
Extracorporral practice
Overtube or hood

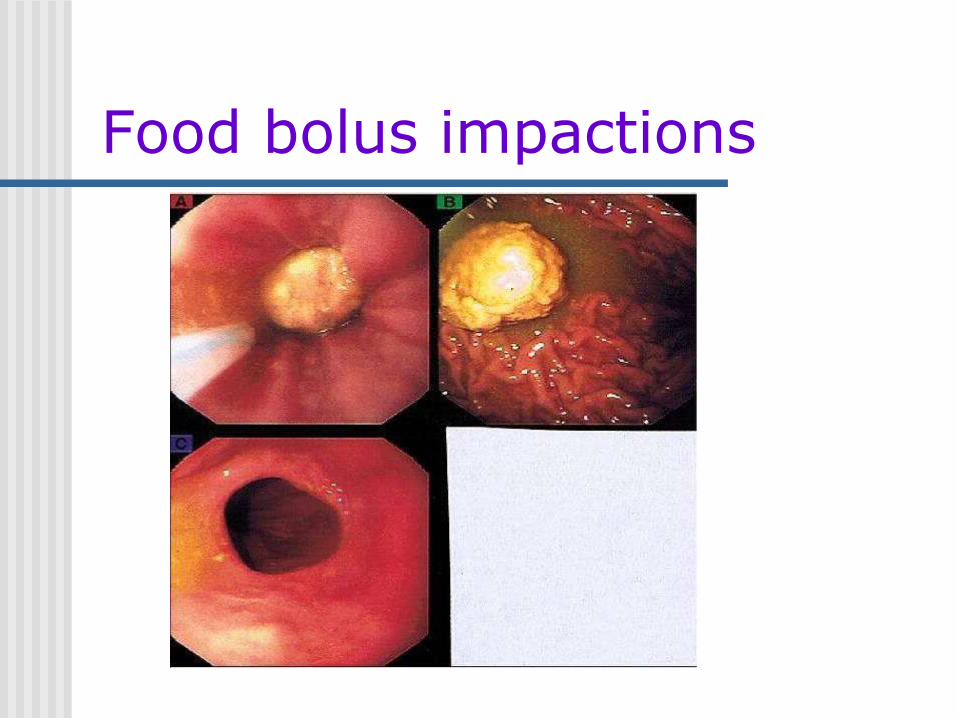
Food bolus impactions
Food bolus impactions can produce obstruction.
Urgent management: severe distress excessively salivating
12 - 24 hours

Food bolus impactions
Many food boluses - a gentle nudge
(sedation and air-insufflation)
- be disrupted and debulked using a
forceps
Using grasping forceps (rat-toothed, or
alligator type)
Food bolus impactions
Food bolus impactions cannot be removed with flexible
endoscopy, options include
repeated attempt by a second endoscopist
rigid esophagoscopy
laparotomy/thoracotomy

Coins and Other Small, Blunt Objects
Blunt objects
esophagus gastric pass gastric ( urgent) (3-4w) (>1w) endoscopy surgery
Sharp/Pointed and Long Objects the most dangerous GIFBs and the
most challenging objects to remove
15- 35% of ingested sharp/pointed
objects cause a gastrointestinal
perforation if untreated.
Sharp/Pointed and Long Objects
Sharp/pointed and long objects in the esophagus merit urgent attention

In esophagus
Sharp/Pointed and Long Objects
Long objects (particularly >10 cm) in the
stomach -- remove endoscopically
Sharp/Pointed and Long Objects
Sharp/Pointed and Long Objects
Sharp objects that cannot be removed by endoscope - followed with daily radiographs
surgical intervention should be considered the object has failed to progress over 3
consecutive days. acute onset of abdominal pain, fever,
evidence of obstruction, and bleeding.

Overtube

Latex hood
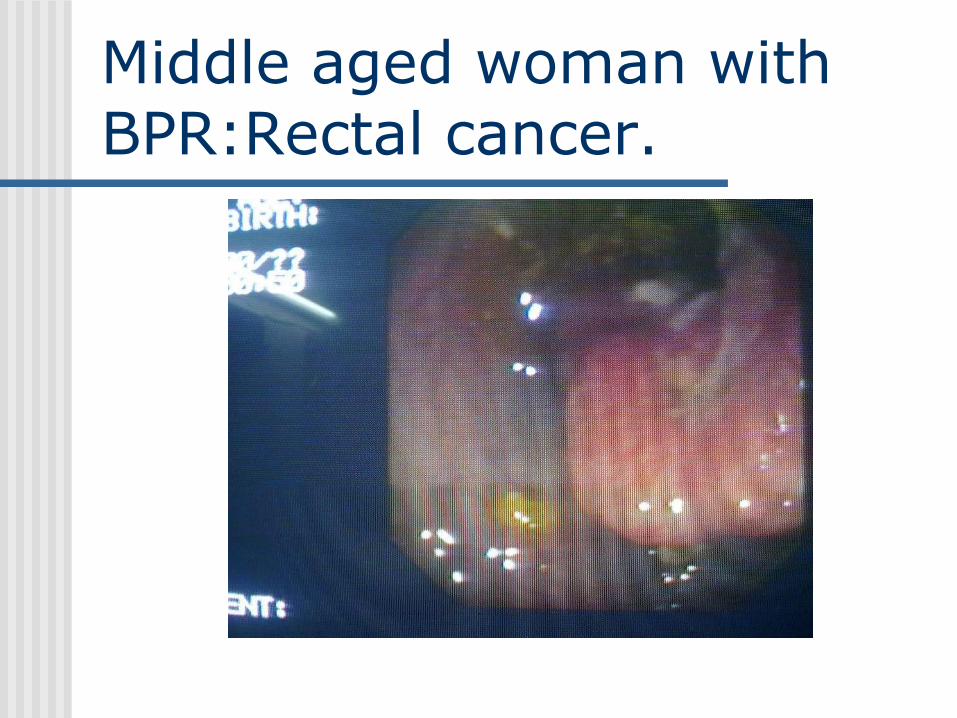
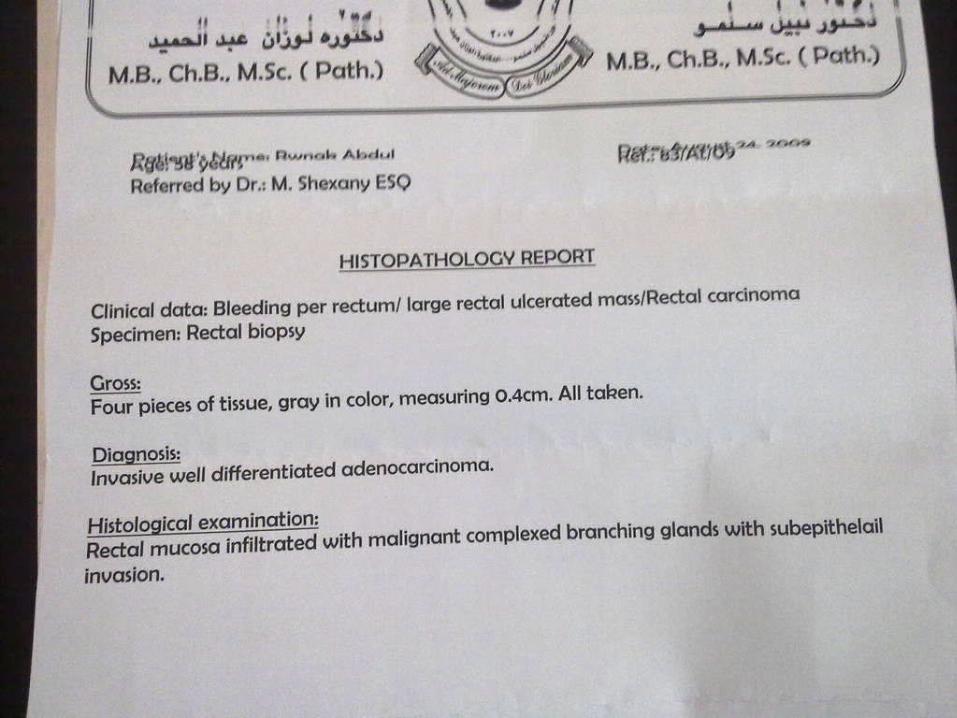
Middle aged woman with BPR:Rectal cancer.

Ch active DU/Severe deudenitis:

GERD:

Pre-pyloric ulcer:

Ch active DUs:

Young woman: severe nodular antral gastropathy & 2 ugly looking antral ulcers

Pregnant woman with ascites: Thickened diffusely infiltrated gastric body: linitis plastica.

Melena: ch active DU& Gastric polyp:

Antral gastropathy& Ch active DU:
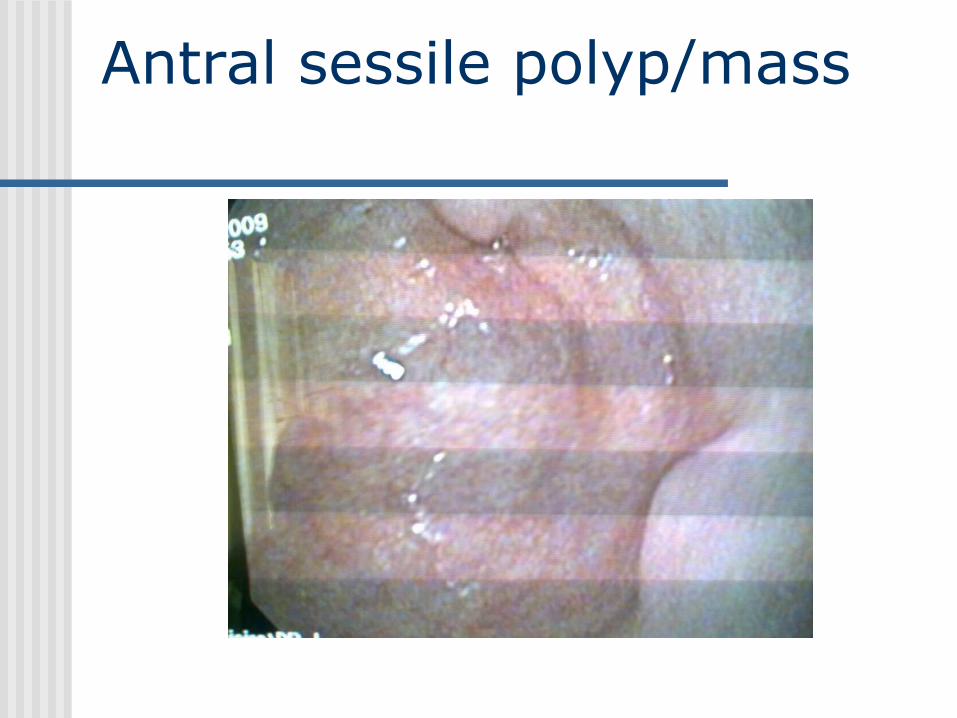
Antral sessile polyp/mass
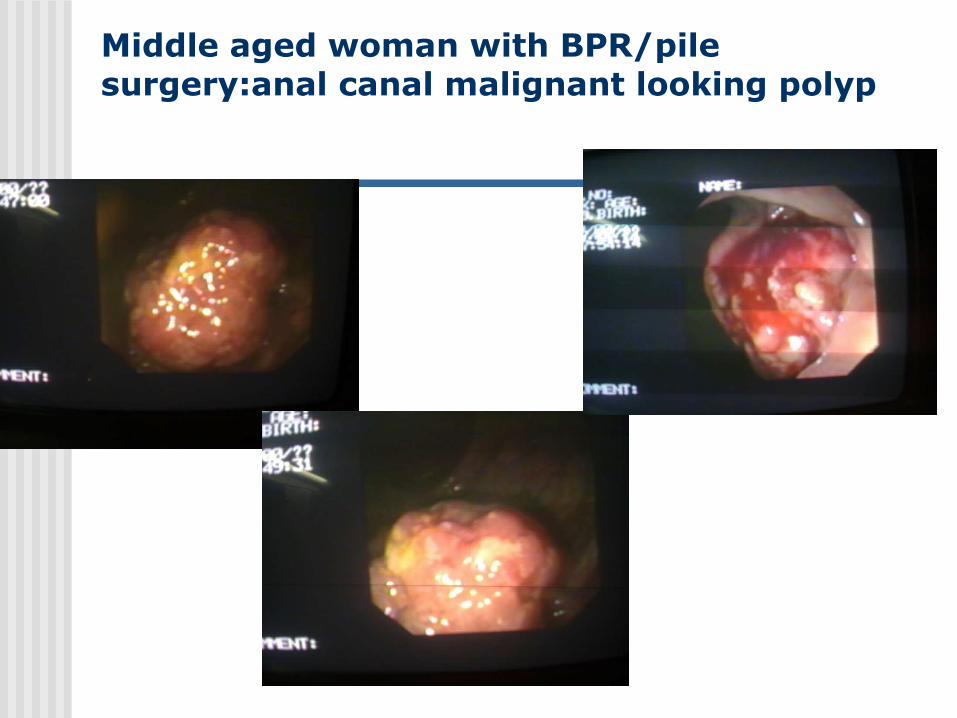
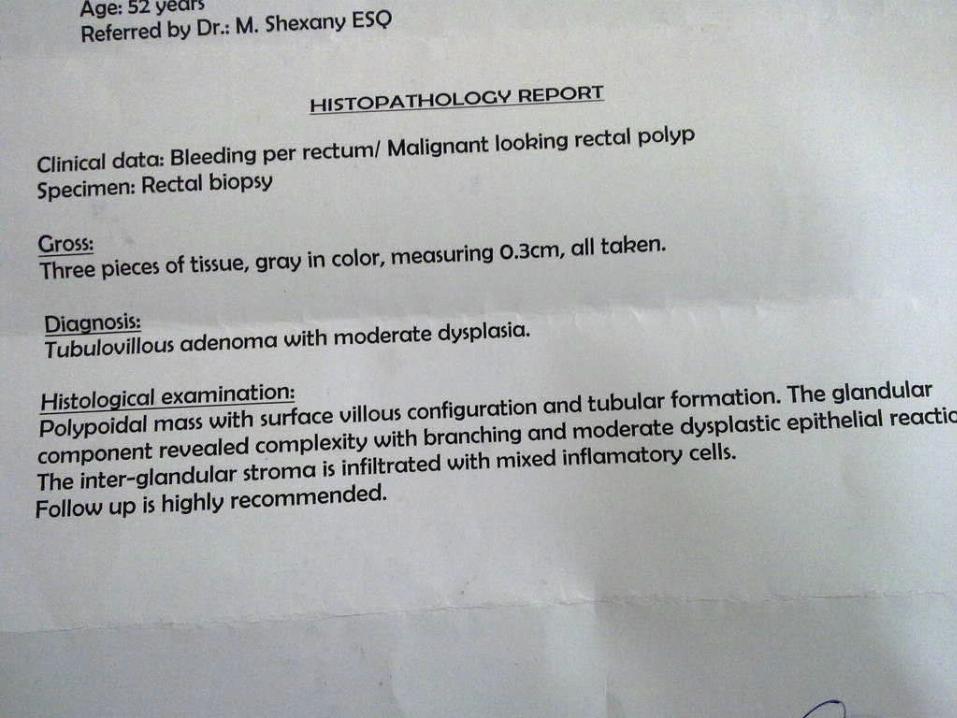
Middle aged woman with BPR/pile surgery:anal canal malignant looking polyp
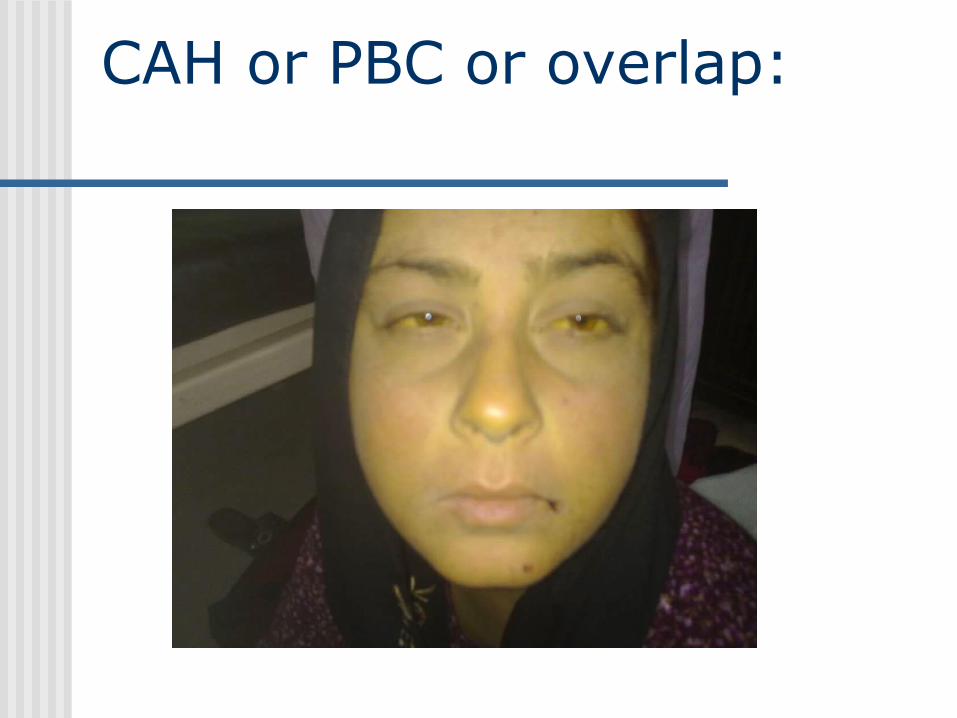
CAH or PBC or overlap:

Laurence moon bedl syndrome:

Necrotizing fascitis:

SLE:

RA deformed hands:

Psoriatic arthritis:

Young man with clubing from childhood & severe esophagitis:
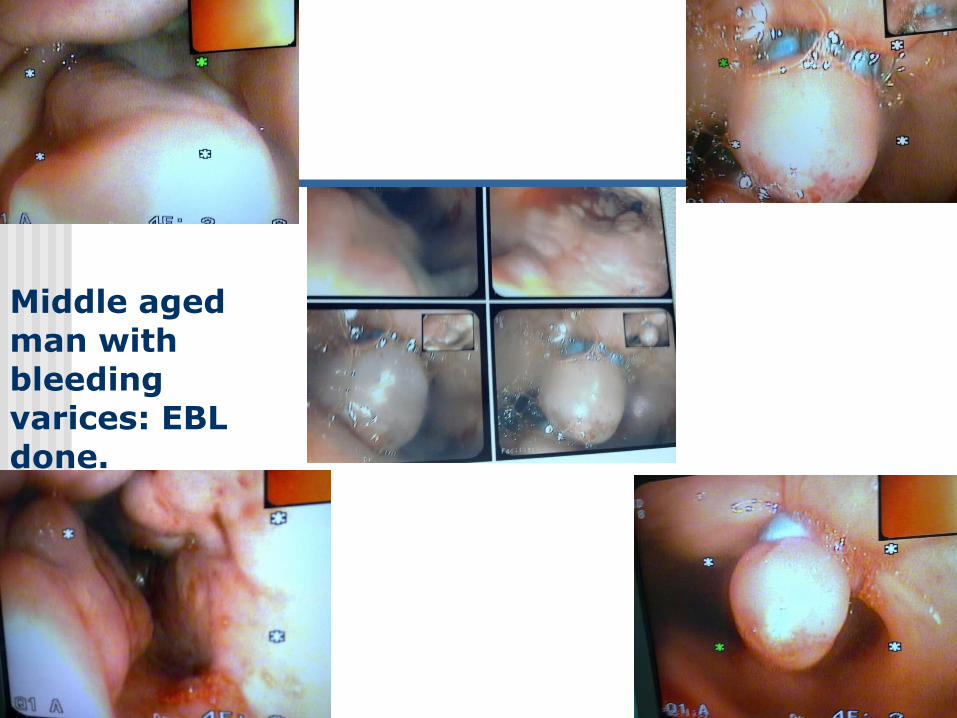
Middle aged man with bleeding varices: EBL done.

Young man with bleeding varices: white ball( bleeding varix) vs red ball (non- bleeding varix) appearance, after EBL.

Cardial varix after eso varices obliteration by EBL in a middle aged woman: