ghit14_ppt_emerging accountable care_sprice
TRANSCRIPT
Emerging Accountable Care Models: Paradigm Shift from Volume to ValueShelley Price, MS, FHIMSSDirector, Payer and Life Sciences, HIMSS
DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not necessarily represent official policy or position of HIMSS.
@SPriceHIMSS | #GovHIT
Learning Objectives
• Understand trends and drivers in healthcare reform from a volume-based system to a value-based system in both the private and public sectors
• Recognize and connect the common themes, issues and challenges between Population Health, new Payment Models, and Accountable Care Organizations
• Learn about new partnerships and efforts toward collaborative, accountable care
• Gain knowledge of the role of data and health IT in driving toward transformation through population health and new payment and delivery models
Agenda
• Healthcare Reform: Why and How
– Driving toward transformation through population health and new payment and delivery models
• Themes, Issues and Challenges
– Population Health
– Payment Models
– Accountable Care Organizations
• Case Studies
• Data and HIT
• HIMSS Resources
• Take-aways
• Questions
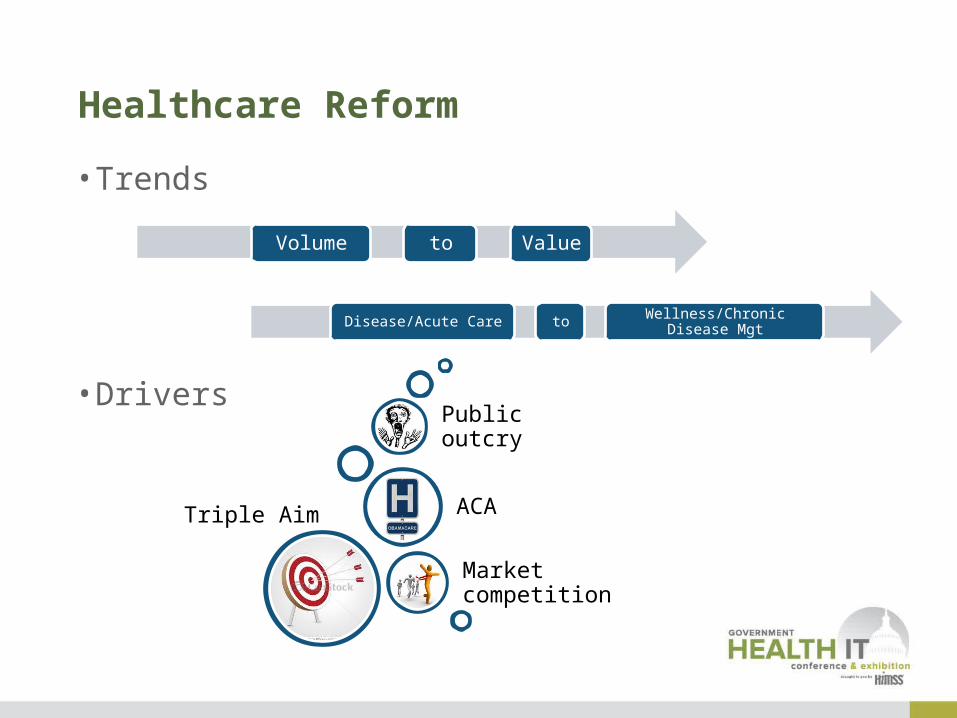
Healthcare Reform
Volume to Value
Disease/Acute Care to Wellness/Chronic Disease Mgt
• Trends
• Drivers
Triple Aim
Market competition
ACA
Public outcry
How Do We Get There?
Population Health
Enabler: New Payment and
Delivery Models
Sample Vehicle: ACOs
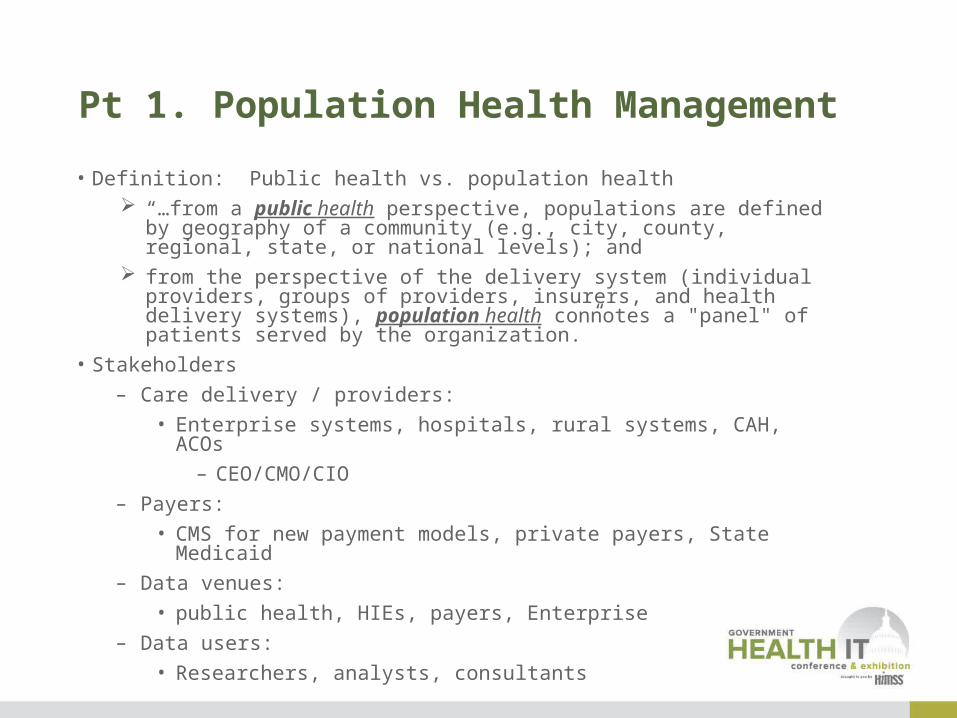
Pt 1. Population Health Management
• Definition: Public health vs. population health “…from a public health perspective, populations are defined by
geography of a community (e.g., city, county, regional, state, or national levels); and
from the perspective of the delivery system (individual providers, groups of providers, insurers, and health delivery systems), population health connotes a "panel" of patients served by the organization.”
• Stakeholders
– Care delivery / providers:
• Enterprise systems, hospitals, rural systems, CAH, ACOs
– CEO/CMO/CIO
– Payers:
• CMS for new payment models, private payers, State Medicaid
– Data venues:
• public health, HIEs, payers, Enterprise
– Data users:
• Researchers, analysts, consultants

PHM: Issues – Needs & Challenges
• Starting up
– C-Suite: How do I begin? Where do I begin? Sure it’s the way of the future…but I am overwhelmed with (go-live, ICD-10, reporting, et al); how can I start in on this?
• Lack of a business plan
• Project management problem
• Available technology ‘toolkits’
– Many ‘solutions’
– Is it right for me? How do I use it?
• Data
– Access
– Architecture
– Timeliness
• Funding
– Initial investment cost; maintenance for activities; limited alternative payment models
• Staffing
– New skills needed (e.g. PHIM, analytics)
– Staffing shortages
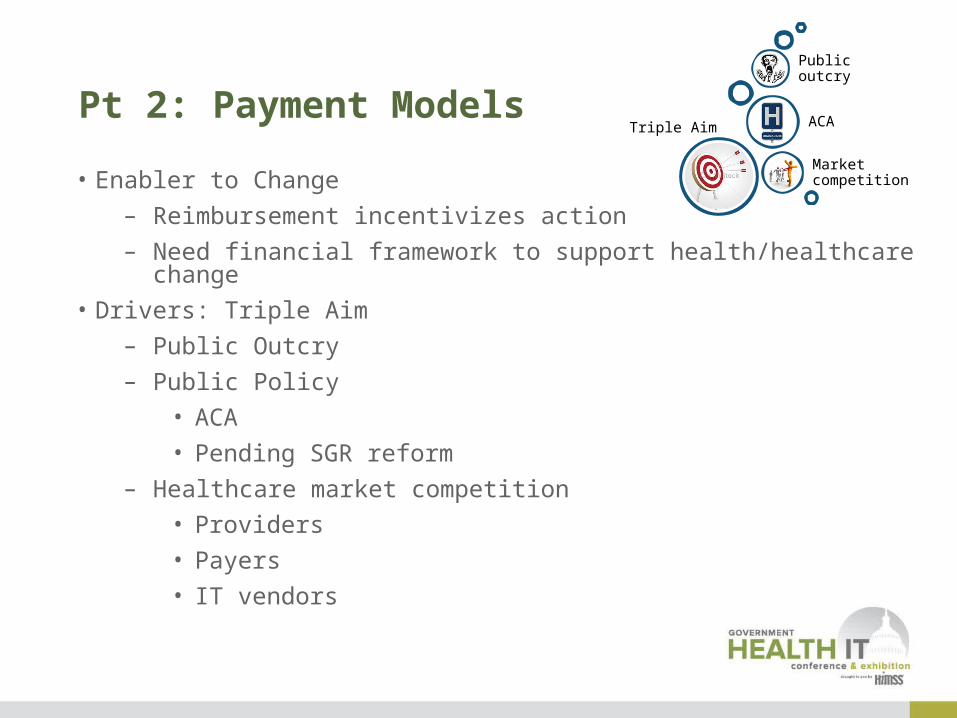
Pt 2: Payment Models
• Enabler to Change
– Reimbursement incentivizes action
– Need financial framework to support health/healthcare change
• Drivers: Triple Aim
– Public Outcry
– Public Policy
• ACA
• Pending SGR reform
– Healthcare market competition
• Providers
• Payers
• IT vendors
Triple Aim
Market competition
ACA
Public outcry
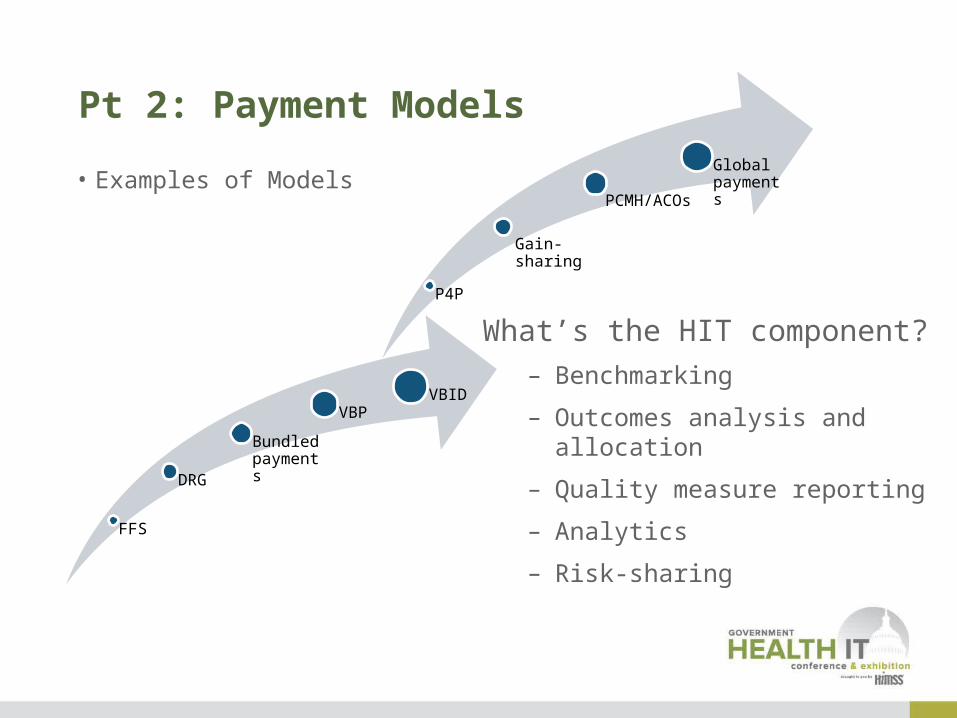
Pt 2: Payment Models
• Examples of Models
FFS
DRG
Bundled payments
VBPVBID
P4P
Gain-sharing
PCMH/ACOs
Global payments
What’s the HIT component?
– Benchmarking
– Outcomes analysis and allocation
– Quality measure reporting
– Analytics
– Risk-sharing

Pt 3: Accountable Care OrganizationsYou’ve Seen One, Then You’ve Seen One
• What | Who | How?
– In general……
• What / Definition / Purpose:
– A group of defined providers working collaboratively, connectively, within a risk-baring structure to improve quality, heath outcomes, and costs of a defined patient population
• Who / Stakeholders:
– Primary: Large hospital systems, large group practices, small-group practices, primary care providers, payers (public and private), IT solution vendors
– Secondary: Consultants, HIEs, regulators…patients????
• How?
– That’s the secret sauce…
Federal ACOs
Background
• 2010 Affordable Care Act: Encourage development of ACOs• Mirrors the Triple-Aim • Several programs driving to ‘value” by linking payment and
outcomes, measured by quality
• CMS Medicare Shared Savings (MSSP) Program intent:• Promote accountability for a population of Medicare
beneficiaries• Improve the coordination of FFS items and services• Encourage investment in infrastructure and redesigned
care processes• Incent higher value care
ACO Eligibility Requirements
• An ACO must provide documentation in its application describing plans to:
– Promote evidence-based medicine– Promote beneficiary engagement– Report internally on quality and cost metrics– Coordinate care
ACO Models: ‘Risk’
• Track One or One-Sided Model
– Shared saving-only option
– “On-ramp” with less risk
– Potential of earning 50% shared savings
• Track Two or Two-Sided Model
– Shared savings/losses model
– Performance based risk in exchange for higher reward
– Potential of earning 60% shared savings
• Two Track Approach for First Agreement Period Only
• All ACOs must participate in the two sided model in subsequent agreement periods

Quality Reporting and Performance
• 33 measures selected combining– Process measures; easier to calculate based on administrative
data, such as claims– Outcome measures including patient experience of care
provide a more complete picture of quality of care improvement but rely on both claims and clinical quality data
– Risk adjustment is included for a number of proposed measures
– Of the 33 measures: • 7 are collected via the patient survey,
• 3 are calculated via claims data,
• 1 is derived from the EHR Incentive Program, and
• 22 are collected via the GPRO web interface
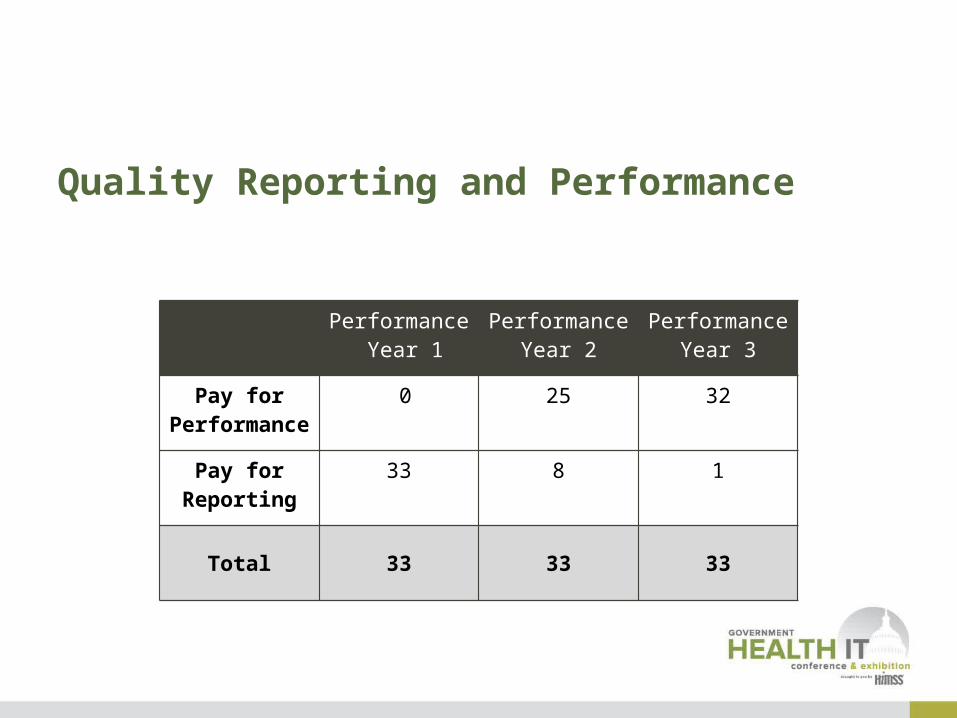
Quality Reporting and Performance
Performance Year 1
Performance Year 2
Performance Year 3
Pay for Performanc
e
0 25 32
Pay for Reporting
33 8 1
Total 33 33 33
ACOs: By the Numbers – CBO Estimates
17
• Estimated Participation– ACOs: 50-270– Beneficiaries: 1.0-5.0M
• Costs and Savings (3 years)– Total savings: $470M (Federal) – Bonuses to ACOs: $1.31B – Penalties from ACOs: $20M– Average ACO startup cost incl 1st yr operating: $.58M

Federal Programs Today (MSSP)
1. April 10, 2012: 27 selected
– Est. 375,000 beneficiaries, 10,000 physicians, 10 hospitals, 13-smaller physician-driven
organizations in 18 States
2. July 9, 2012: 89 selected
– Est. 1.2 million beneficiaries in 40 States and Washington, D.C.
3. Jan 10, 2013: 106 selected
– 47 States, PR, and DC are now served
– Increasing trend toward physician-led practices (approx half of new group)
• serving <10,000 beneficiaries each; approx 20 percent CHCs, rural health clinics and
CAH
4. Dec 23, 2013: 123 selected
– Est. 1.5 million additional beneficiaries
– Focus on underserved: 1 in 5 ACOs include CHCs, rural health clinics, and CAH that serve
low-income and rural communities

©2013 LEAVITT PARTNERS
Geo Dispersion: Medicare Shared Savings ACOs
Source: Center for Medicare & Medicaid Innovation
3rd Round
2nd Round
1st Round
Federal Programs Today
• Other Programs
– Pioneer Model ACOs
• December 2011: 32 organizations
– Advanced Payment ACOs
• January 2013: 15 organizations
– Physician Group Practice Transition Demonstration
• January 2012: 6 organizations
• All Told: more than 5.3 million beneficiaries through nearly 400 organizations in all states except Delaware are receiving care from providers participating in CMS initiatives

4 million Medicare beneficiaries having care coordinated by 220 MSSP and 32 Pioneers ACOs(Geographic Distribution of ACO Population)
21Source: Centers for Medicare & Medicaid

But What is Really Going on?
• MSSP ACOs
– Jan 2013 reporting of 1st cohort (27):
• Track 1 – Successfully reported quality measures: 25 (incl. 4 out of 5 Advanced Payment)
• Track 2 – Generated Losses: 2
• Track 2 – Generated Savings: 2
• Pioneer Model ACOs
– 32 Original Pioneer ACOs caring for 669,000 Medicare patients and all met the quality criteria. Of those,
• 18 lowered the average Medicare cost below the benchmark
– 13 saved enough to share a total of $76M with Medicare
– 5 with savings not sufficient enough to share with Medicare
• 14 increased average Medicare costs

Commercial ACOs
©2013 LEAVITT PARTNERS
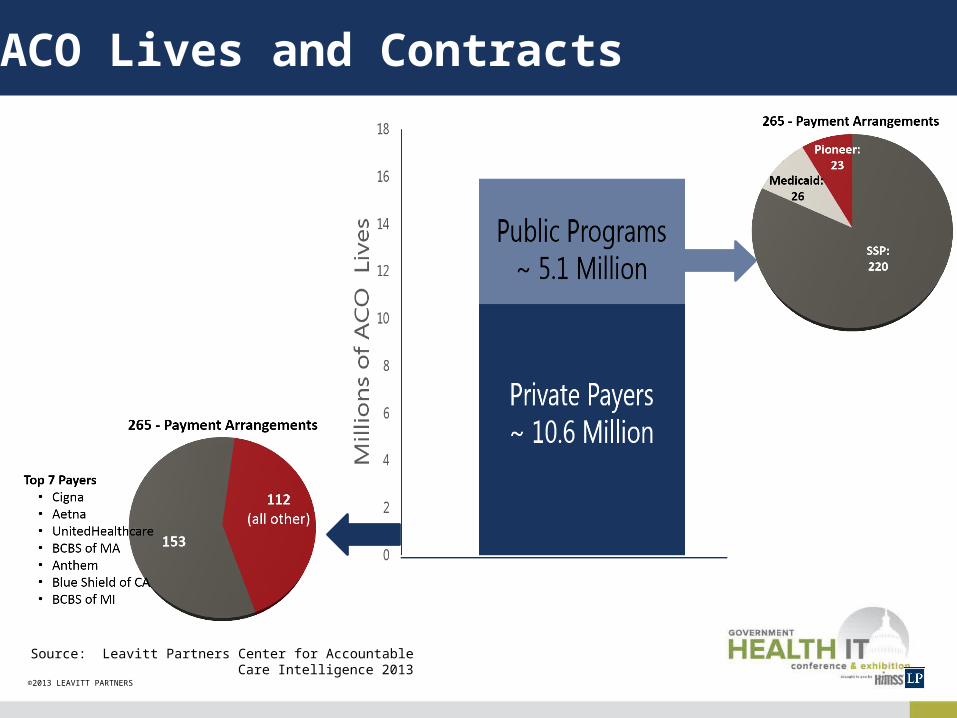
ACO Lives and Contracts
Source: Leavitt Partners Center for Accountable Care Intelligence 2013
©2013 LEAVITT PARTNERS
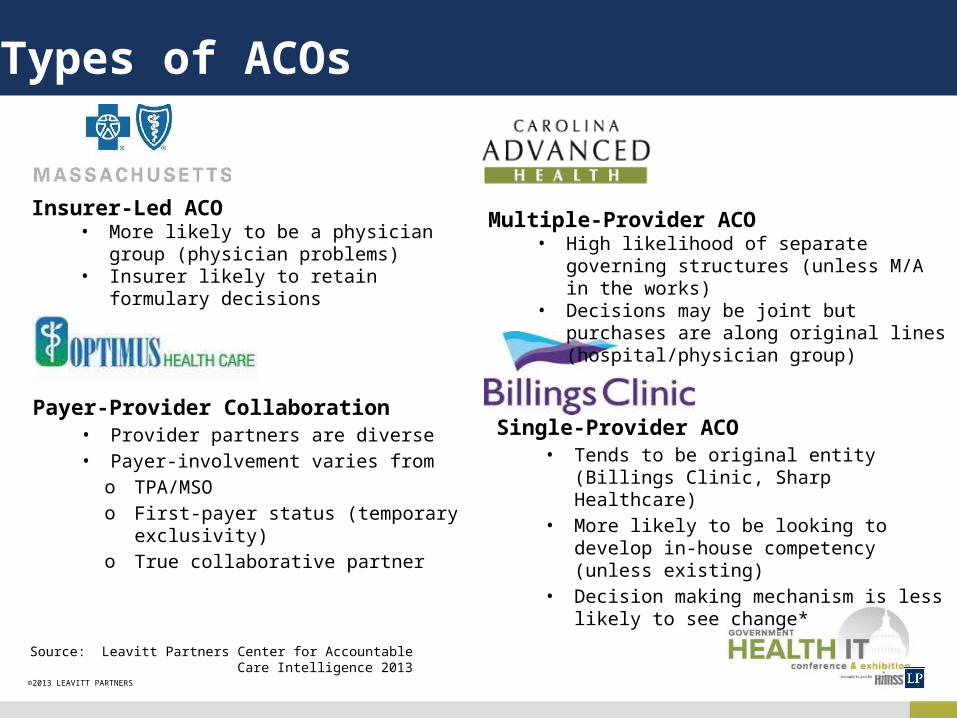
Types of ACOs
Payer-Provider Collaboration• Provider partners are diverse• Payer-involvement varies from
o TPA/MSOo First-payer status (temporary
exclusivity)o True collaborative partner
Single-Provider ACO• Tends to be original entity (Billings
Clinic, Sharp Healthcare)• More likely to be looking to develop in-
house competency (unless existing)• Decision making mechanism is less
likely to see change*
Insurer-Led ACO• More likely to be a physician group
(physician problems)• Insurer likely to retain formulary decisions
Multiple-Provider ACO• High likelihood of separate governing
structures (unless M/A in the works)• Decisions may be joint but purchases are
along original lines (hospital/physician group)
Source: Leavitt Partners Center for Accountable Care Intelligence 2013
Innovation in the Commercial Marketplace
• Commercial Health Plans are engaging with Providers toward Accountable Care. Examples:
– Aetna
• Facilitating the clinical, financial, technological and cultural changes ; Aiding in implementing technology to unlock the power of evidence-based medicine and preventive care
– Example of results: 45% reduction in hospital admissions; 50% fewer patient hospital days; $600 annual savings per patient
– Cigna
• Strong focus on care coordinators and case managers
• 89 ‘collaboratives’ in 27 states
– covering 910,000 lives and
– through 36,000 providers
HIMSS Perspective

Pediatric ACOs
HIMSS TOWN HALL: Understanding the Particular Characteristics of Pediatric Populations and How They Could Impact Accountable Care Organizations
Presentation by Deb Wells, CHOP for the HIMSS ACO Task Force
April 4, 2014
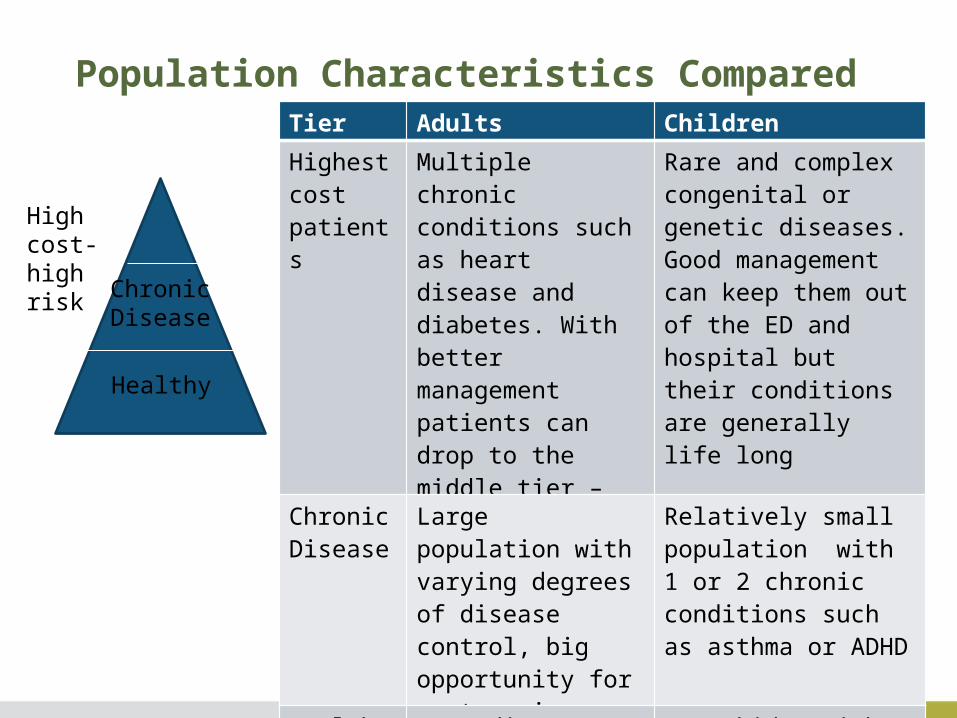
Population Characteristics Compared
Healthy
Chronic Disease
High cost-high risk
Tier Adults Children
Highest cost patients
Multiple chronic conditions such as heart disease and diabetes. With better management patients can drop to the middle tier – often elderly
Rare and complex congenital or genetic diseases. Good management can keep them out of the ED and hospital but their conditions are generally life long
Chronic Disease
Large population with varying degrees of disease control, big opportunity for cost savings
Relatively small population with 1 or 2 chronic conditions such as asthma or ADHD
Healthy patients
Depending on who you ask 60-75% of patients
Most kids, with focus on prevention, growth & development
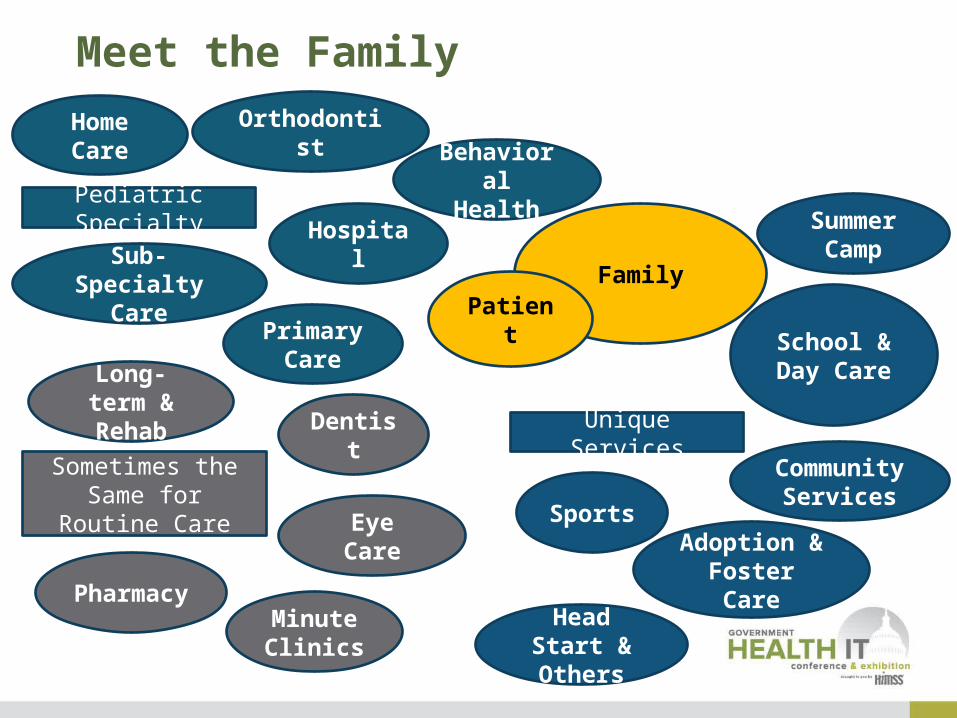
Meet the Family
School & Day Care
Community
Services
Dentist
Behavioral Health
Adoption & Foster
Care
Sports
Primary Care
Sub-Specialty
Care
Pharmacy Head
Start & Others
Long-term & Rehab
Home Care
Hospital
Minute Clinics
Pediatric Specialty
Unique ServicesSometimes the
Same for Routine Care Eye
Care
Summer Camp
Orthodontist
FamilyPatien
t
Key Issues• Kid’s unique medical needs and social environment necessitate care from
pediatric-trained physicians and child-specific community resources such as schools
• It is essential to select performance metrics that are meaningful to pediatrics and that accurately measure the quality of pediatric care
• Population characteristics and scarce sub-specialists require a regional vs local provider base
• Technology needs to include functionality to support pediatric care
• Children with medical complexity usually have many subspecialists and rely on community resources and will need special care throughout their lives
• The family is generally responsible for a child’s health care, rather than the patient him- or herself
• Federal leadership provided by Medicare is lacking in Medicaid, but states have begun working with providers to form Medicaid ACOs
• A largely healthy population means that a larger number of patients is needed to show significant cost savings

Influencing Quality and the Payer Relationship with C&BI
CASE STUDY by the C&BI Value Task ForceApril 4, 2014
Key Issues• Current coding and FFS program not
sufficient nor indicative of quality in complex obstetrics cases
• Hawaii Pacific Health and Hawaii Medical Service Association (BCBS) partnered on obstetrics program
• Contract tying reimbursement to outcomes synchronously achieved patient outcomes and fiscal objectives
• Results:
– State-of-the-art obstetrical service line
– Decrease in C-Section in low-risk deliveries
– Value-based payments: Increase to 15% of payments
– New contract: moving to 50% of payment value-based
Data and HIT

• Data warehousing• Healthcare data integration• Enterprise analytics• Predictive analytics• Population health
Financial Data
Clinical Data
Operational Data
Hope & promise….
and the challenge
Clinical & Business Intelligence – Turn Data into Action
“Defensive” Risk Management• Readmissions Management • Chronic Disease Detection • Inpatient Length of Stay Management • At Risk Population Detection • Hospital Acquired Condition Prevention
“Offensive” Risk Management• Chronic Care Management • Tailored Benefit Design • Wellness Program Management • Disease Detection & Early Intervention
PHM and ACO Common ChallengesSome common clinical analytics:
Some common financial analytics:• Revenue Cycle• Clinical Quality & Outcomes• Physician Performance & Outcomes Analysis• Patient/Customer Satisfaction• Market (to assess ROI)• Labor Management
HIMSS Resources
• Population Health and Accountable Care
– Resources
• C&BI Task Force: 10 Steps to Build a PHM Program, definitions for clinicians, CEO/CMO interviews, Using your ED for PHM
• Accountable Care Task Force: Various resources including ACO Core IT Capabilities; ACO and mobile case studies
• ACO Federal Programs resource page
• State HIT ACO Dashboard
– Education
• HIMSS14: 24 sessions (Pop Health)
• HIMSS14: 12 sessions (ACOs), ACO symposium; virtual education
• Congressional Seminar Series
• Communities
• www.himss.org/ProviderPayerCommunity
• www.himss.org/ClinBusIntelCommunity

Take-Aways
• Transitioning healthcare system to fee-for-value is hard
• The accountable care / fee-for-value concept is here to stay
• You've seen one, you’ve seen one
• Technology is both the key and a challenge
Questions?
Thank you!
Shelley Price, MS, FHIMSSDirector, Payer & Life Sciences, HIMSS
Phone: 703-562-8846Mobile: 703-967-4425Email: [email protected]
@SPriceHIMSS | #GovHIT