getting smart about developing individualized sequences of...
TRANSCRIPT

Getting SMART about DevelopingIndividualized Sequences of Health
Interventions
Daniel Almirall1,2 Linda M Collins2,3,5
Susan A Murphy1,2,4
1Institute for Social Research, University of Michigan2The Methodology Center, Penn State University
3Human Development and Family Studies, Pennsylvania State University4Department of Statistics, University of Michigan
5Department of Statistics, Pennsylvania State University
IMPACT Meeting - North Carolina - November 2, 2012Almirall, Collins, Murphy Building Adaptive Interventions 1 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
Outline
Adaptive InterventionsWhat? Why?
Evaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)What are SMARTs?
SMART Design PrinciplesKeep it SimpleChoosing Primary and Secondary Hypotheses
Discussion
Almirall, Collins, Murphy Building Adaptive Interventions 2 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
What? Why?
ADAPTIVE INTERVENTIONS
Almirall, Collins, Murphy Building Adaptive Interventions 3 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
What? Why?
Definition: An Adaptive Intervention is
I a sequence of individually tailored decision rulesI that specify whether, how, and/or whenI to alter the intensity, type, dosage, or delivery of treatmentI at critical decision points in the course of care.
Adaptive Interventions operationalize sequential decisionmaking with the aim of improving clinical practice.
Almirall, Collins, Murphy Building Adaptive Interventions 4 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
What? Why?
Concrete Example of an Adaptive InterventionPediatric Anxiety Example (SAD, GAD, SoP)
Maintain: CBT
CBT
Add Treatment: CBT + MED
Responder
s
Non-Responders
Tailoring Variable First-line Txt Second-line Txt
I Goal is to minimize the child’s symptom profile/trajectory.
Almirall, Collins, Murphy Building Adaptive Interventions 5 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
What? Why?
What makes up an Adaptive Intervention?1. Critical decisions: treatment options and more2. Tailoring variables: to decide how to adapt treatment3. Decision rules: inputs tailoring variable, outputs one or
more recommended treatments
Maintain: CBT
CBT
Add Treatment: CBT + MED
Responder
s
Non-Responders
Tailoring Variable First-line Txt Second-line Txt
Adaptive interventions AKA: dynamic treatment regimes, adaptive treatmentstrategies, treatment algorithms, structured treatment interruptions, practiceparameters, ASAM criteria...
Almirall, Collins, Murphy Building Adaptive Interventions 6 / 44

An Adaptive Intervention in Obesity
Maintain: GBI Refreshers
GBI Augment: GBI + Personal Health
Coach
Responder
Non‐Responder
Tailoring Variable: RESP if
4mo Wgt Change: >10% #Family Exprmts: avg>2/q Dietary intke: avg>3fv/wk
First‐line Txt:Months 0‐4
Second‐line Txt: Months 4‐12
Step Down: PHC‐lite (phone) GBI +
Personal Health Coach
Augment: GBI + Personal Health
Coach + Medication
Responder
Non‐Responder
Obesity: BMI ≤ 97%ile
Obesity: BMI > 97%ile
Tailoring Variable at Intake

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
What? Why?
Why Adaptive Interventions?Necessary because...
I Nature of chronic disorders (substance use, mental health,diabetes, cancer)
I Waxing and waning course (multiple relapse, recurrence)I Genetic and non-genetic factors influence courseI Co-occuring disorders may arise
I High patient heterogeneity in response to treatment
I Within person (over time) differential response to treatmentI Between person differential response to treatment
All require sequences of treatment decisions.
Almirall, Collins, Murphy Building Adaptive Interventions 8 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
GENERATING HYPOTHESES vs BUILDING vs EVALUATING
ADAPTIVE INTERVENTIONS?
Almirall, Collins, Murphy Building Adaptive Interventions 9 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
3 Different Research Questions/Aims= 3 Different Research Designs
I Aim 1: When generating hypotheses to build anAdaptive Intervention: e.g., Does augmenting txt (asobserved in a previous trial) for non-responders correlatewith better outcomes?
I Aim 2: When building an Adaptive Intervention: e.g, Whatare the best tailoring variables and/or decision rules?
I Aim 3: When evaluating a particular AdaptiveIntervention: e.g. Does the AI have a statisticallysignificant effect as compared to control intervention?
Almirall, Collins, Murphy Building Adaptive Interventions 10 / 44

3 Different Research Questions/Aims= 3 Different Research Designs
Ex. Q1: Does augmenting txt for non-responders (as observedin a previous trial) correlate with better outcomes?
Ex. Q2: What are the best tailoring variables or decision rules?
Ex. Q3: Does the Adaptive Intervention have a statisticallysignificant effect as compared to control intervention?
Observational ExperimentalStudies Studies
e.g., Analysis ofQuestion Aim Previous RCT SMART RCT
1 Hypothesis Gen. YES ≈ ∼2 Building ≈ YES ≈3 Evaluating ∼ ≈ YES

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
What are SMARTs?
SEQUENTIAL MULTIPLE ASSIGNMENTRANDOMIZED TRIALS (SMARTs)
Almirall, Collins, Murphy Building Adaptive Interventions 12 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
What are SMARTs?
What is a Sequential Multiple AssignmentRandomized Trial (SMART)?
I Multi-stage trials; same participants throughoutI Each stage corresponds to a critical decision pointI At each stage, subjects randomized to set of treatment
optionsI The goal of a SMART is to inform the development of
adaptive interventions.
I will give you an example SMART, but first...
Almirall, Collins, Murphy Building Adaptive Interventions 13 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
What are SMARTs?
Motivation for an Example SMARTChild-Adolescent Anxiety Multi-modal Study (CAMS)
I CAMS: acute-phase, efficacy, RCT for child anxiety
I CBT+MED > MED ≈ CBT > Placebo
I However, some families and clinicians remain concernedabout the use of MED in this population
I So an important next question for clinical practice is“Can we delay the use of MED?””If so, for whom?”
I Some children may do fine w/ CBT only and not need MED.
Almirall, Collins, Murphy Building Adaptive Interventions 14 / 44

Concrete Example of a SMART: Pediatric AnxietyCourtesy of Scott N Compton, Duke University Medical Center
Add Treatment: CBT + MED + FT Non-Responders
CBT + MED Maintain: CBT + MED
Step Down: CBT Only
R Maintain:
CBT
CBT Add Treatment: CBT + MED
Switch Treatment: MED
Responders R
Responders
Non-Responders R
O2 + Primary
Tailoring Variable First-line Txt Second-line Txt Y O1

One Adaptive Intervention Within the SMART
Add Treatment: CBT + MED + FT Non-Responders
CBT + MED Maintain: CBT + MED
Step Down: CBT Only R Maintain:
CBT
CBT Add Treatment: CBT + MED
Switch Treatment: MED
Responders R
Responders
Non-Responders R
O2 + Primary
Tailoring Variable First-line Txt Second-line Txt Y O1
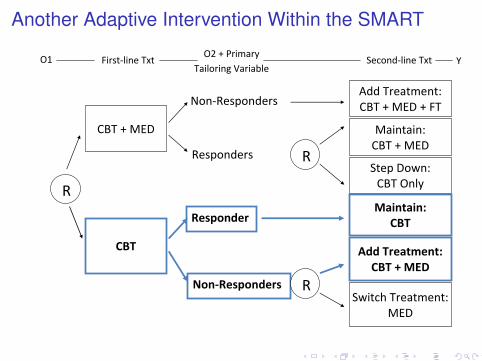
Another Adaptive Intervention Within the SMART
Add Treatment: CBT + MED + FT Non-Responders
CBT + MED Maintain: CBT + MED
Step Down: CBT Only
R Maintain:
CBT
CBT Add Treatment: CBT + MED
Switch Treatment: MED
Responders R
Responder
s
Non-Responders R
O2 + Primary
Tailoring Variable First-line Txt Second-line Txt Y O1

4 Embedded Adaptive Interventions in this SMART
Add Treatment:CBT + MED + FTNon‐Responders
CBT + MED Step Down:CBT Boost
Responders
Add Treatment:CBT + MED + FT Non‐Responders
CBT + MED Maintain:CBT + MED
Responders
Maintain:CBT BoostResponders
CBT Add Treatment:
CBT + MEDNon‐Responders
Maintain:CBT BoostResponders
CBT Switch Treatment:
MEDNon‐Responders
AI 1
AI 2
AI 3
AI 4

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
Keep it SimpleChoosing Primary and Secondary Hypotheses
SMART DESIGN PRINCIPLES
Almirall, Collins, Murphy Building Adaptive Interventions 19 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
Keep it SimpleChoosing Primary and Secondary Hypotheses
SMART Design Principles
I KISS Principle: Keep It Simple, Straightforward
I Power for simple important primary hypotheses
I Take Appropriate steps to develop a moredeeply-individualized Adaptive Intervention
Almirall, Collins, Murphy Building Adaptive Interventions 20 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
Keep it SimpleChoosing Primary and Secondary Hypotheses
Keep It Simple, StraightforwardOverarching Principle
At each stage, or critical decision point,...I Use low dimensional summary to restrict subsequent
treatmentsI Use binary responder statusI Should be easy to use in actual clinical practice
I Restrict class of treatment options only by ethical,feasibility, or strong scientific considerations
I Collect additional, auxiliary time-varying measuresI To develop a more deeply-tailored Adaptive InterventionI Think time-varying effect moderators
Almirall, Collins, Murphy Building Adaptive Interventions 21 / 44
Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
Keep it SimpleChoosing Primary and Secondary Hypotheses
SMART Design: Primary Aims
Choose a simple primary aim/question that aids developmentof an adaptive intervention.
Power the SMART to test this hypothesis.
Almirall, Collins, Murphy Building Adaptive Interventions 22 / 44

Primary Aim Example 1What is the main effect of initial CBT vs initial CBT+MED on longitudinal outcomes?
Add Treatment: CBT + MED + FT Non-Responders
CBT + MED Maintain: CBT + MED
Step Down: CBT Only R Maintain:
CBT
CBT Add Treatment: CBT + MED
Switch Treatmnt: MED
Responders R
Responders
Non-Responders R
O2 + Primary
Tailoring Variable First-line Txt Second-line Txt Y O1
PowerES N0.8 340.5 830.2 505ρ = 0.60α = 0.05β = 0.20

Primary Aim Example 2Is there a difference between two of the embedded adaptive interventions?
Add Treatment:CBT + MED + FTNon‐Responders
CBT + MED Step Down:CBT Boost
Responders
Add Treatment:CBT + MED + FT Non‐Responders
CBT + MED Maintain:CBT + MED
Responders
Maintain:CBT BoostResponders
CBT Add Treatment:
CBT + MEDNon‐Responders
Maintain:CBT BoostResponders
CBT Switch Treatment:
MEDNon‐Responders
AI 1
AI 2
AI 3
AI 4 Sample size calculators exist for this; see Oetting, Levy, Weiss,
and Murphy 2011.
Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
Keep it SimpleChoosing Primary and Secondary Hypotheses
SMART Design: Secondary Aims
Choose secondary aims/questions that further develop theAdaptive Intervention and take advantage of sequentialrandomization to eliminate confounding.
Almirall, Collins, Murphy Building Adaptive Interventions 25 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
Keep it SimpleChoosing Primary and Secondary Hypotheses
Secondary Aim Examples 1 and 2Best second-line treatment and second-line treatment tailoring aim.
O2 = CBT adherence, time to non-response, allegiance with therapist, changes in home environment
Add Treatment: CBT + MED
Switch Treatment: MED
Non-Responders R
O2 + Primary
Tailoring Variable First-line Txt Second-line Txt Y
CBT
Almirall, Collins, Murphy Building Adaptive Interventions 26 / 44

Secondary Aim Example 3Build a more deeply tailored adaptive intervention.
Add Treatment: CBT + MED + FT Non-Responders
CBT + MED Maintain: CBT + MED
Step Down: CBT Only
R Maintain:
CBT
CBT Add Treatment: CBT + MED
Switch Treatment: MED
Responders R
Responders
Non-Responders R
O2 + Primary
Tailoring Variable First-line Txt Second-line Txt Y O1
O1 = demographics, genetics, sub-diagnoses, co-morbidities, etc…
O2 = adherence, time to NR, changes at home, etc…

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
DISCUSSION
Almirall, Collins, Murphy Building Adaptive Interventions 28 / 44

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
Adaptive Interventions vs Adaptive ExperimentalDesigns?
I These ideas are not (necessarily) related. Confusing!
I Adaptive interventions are a type of intervention designI Adaptive experimental designs are particular type of
experimental designI SMARTs are not Adaptive Experimental DesignsI SMARTs do inform development of Adaptive Interventions
Almirall, Collins, Murphy Building Adaptive Interventions 29 / 44
Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
Take Home the FollowingI Adaptive Interventions individualize treatment up-front and
throughout
I Adaptive Interventions are guides for clinical practice
I SMARTs are used to build better Adaptive InterventionsI Next trial: SMART-optimized Adaptive Intervention vs.
state-of-the-art treatment
I SMARTs do not necessarily require larger sample sizes
I Existing RCTs can be used to begin to learn aboutadaptive interventions
I Observational study
Almirall, Collins, Murphy Building Adaptive Interventions 30 / 44

Interventions for Minimally Verbal Children with AutismPI: Kasari(UCLA), Kaiser(Vanderbilt), Smith(Rochester), Lord(Cornell), Almirall(Mich)
Non‐Responders (Parent training no feasible)
JASC (joint attention and
play) Re‐engage /continue JASC
JASC + Parent Training R
DTT (Discrete training)
Re‐engage /continue DTT
DTT + Parent Training
Responders(Blended txt unnecessary)
R
Non‐Responders(Parent training not feasible)
Responders(Blended txt unnecessary)
R
JASC+DTT
Re‐engage / continue JASC
R
JASC+DTT
Re‐engage /continue DTT
R

Adaptive InterventionsEvaluating versus Building an Adaptive Intervention?
Sequential Multiple Assignment Randomized Trial (SMART)SMART Design Principles
Discussion
Thank you! Questions?
Find papers on SMART:I http://www.lsa.stat.umich.edu/∼samurphy/ (Susan Murphy)I http://methcenter.psu.edu (Linda Collins)
These slides will be posted on my website:I http://www-personal.umich.edu/∼dalmiral/
Email me with questions about this presentation:I Daniel Almirall: [email protected]
Almirall, Collins, Murphy Building Adaptive Interventions 32 / 44

Adaptive Treatment for Children with ADHDPI: Pelham, Florida International University
Continue Medication Responders
Medication Increase Medication Dose
Add Behavioral Intervention
R Continue
Behavioral Intervention Behavioral
Intervention Increase Behavioral
Intervention
Add Medication
Non-Responders R
Responders
Non-Responders R

Treatment for Alcohol DependencePI: Oslin, University of Pennsylvania
Early Trigger for NR: 2+ HDD CBI
CBI + Naltrexone
R
Late Trigger for NR: 5+ HDD
CBI
CBI + Naltrexone
Non-Response R
Non-Response R
Naltrexone
TDM + Naltrexone
8 Week Response R
Naltrexone
TDM + Naltrexone
8 Week Response R
Extra Slides
Almirall, Collins, Murphy Building Adaptive Interventions 35 / 44

Hypothesis-generating Observational StudiesPost-hoc Analyses Useful for Building Adaptive Interventions
I Give examples of different observational study questionsthey can examine using data from a previous 2-arm RCT
I Standard observational study caveats apply:I No manipulation usually means lack of heterogeneity in txt
options (beyond what is controlled by experimentation inoriginal RCT)
I Some RCTs use samples that are too homogeneousI Confounding by observed baseline and time-varying factorsI Unobserved, unknown, unmeasured confounding by
baseline and time-varying factors
Almirall, Collins, Murphy Building Adaptive Interventions 36 / 44

Hypothesis-generating Observational StudiesPost-hoc Analyses Useful for Building Adaptive Interventions
I There exists a literature for examining the impact oftime-varying treatments in observational studies
I Marginal Structural Models (Robins, 1999; Bray, Almirall, etal., 2006) to examine the marginal impact of observedtime-varying sequences of treatment
I Structural Nested Mean Models (Robins, 1994; Almirall, etal., 2010, 2011) to examine time-varying moderators ofobserved time-varying sequences of treatment
I Marginal Mean Models (Murphy, et al., 2001): to examinethe impact of observed adaptive interventions
Almirall, Collins, Murphy Building Adaptive Interventions 37 / 44

Early precursors to SMART
I CATIE (2001) Treatment of Psychosis in Patients withAlzheimer’s
I CATIE (2001) Treatment of Psychosis in Patients withSchizophrenia
I STAR*D (2003) Treatment of Depression
Almirall, Collins, Murphy Building Adaptive Interventions 38 / 44
Other Alternatives
I Piecing Together Results from Multiple TrialsI Choose best first-line treatment on the basis of a two-arm
RCT; then choose best second-line treatment on the basisof another separate, two-arm RCT
I Concerns: delayed therapeutic effects, and cohort effects
I Observational (Non-experimental) Comparisons of AIsI Using data from longitudinal randomized trialsI May yield results that inform a SMART proposalI Understand current treatment sequencing practicesI Typical problems associated with observational studies
I Expert Opinion
Almirall, Collins, Murphy Building Adaptive Interventions 39 / 44

Why Not Use Multiple Trials to Construct an AIThree Concerns about Using Multiple Trials as an Alternative to a SMART
1. Concern 1: Delayed Therapeutic Effect
2. Concern 2: Diagnostic Effects
3. Concern 3: Cohort Effects
All three concerns emanate from the basic idea thatconstructing an adaptive intervention based on a myopic, local,study-to-study point of view may not be optimal.
Almirall, Collins, Murphy Building Adaptive Interventions 40 / 44

Why Not Use Multiple Trials to Construct an AIConcern 1: Delayed Therapeutic Effects, or Sequential Treatment Interactions
Positive Synergy Btwn First- and Second-line Treatments
Tapering off medication after 12 weeks of use may not appearbest initially, but may have enhanced long term effectivenesswhen followed by a particular augmentation, switch, ormaintenance strategy.
Tapering off medication after 12 weeks may set the child up forbetter success with any one of the second-line treatments.
Almirall, Collins, Murphy Building Adaptive Interventions 41 / 44

Why Not Use Multiple Trials to Construct an AIConcern 1: Delayed Therapeutic Effects, or Sequential Treatment Interactions
Negative Synergy Btwn First- and Second-line Treatments
Keeping the child on medication an additional 12 weeks mayproduce a higher proportion of responders at first, but may alsoresult in side effects that reduce the variety of subsequenttreatments available if s/he relapses.
The burden associated with continuing medication an additional12 weeks may be so high that non-responders will not adhereto second-line treatments.
Almirall, Collins, Murphy Building Adaptive Interventions 42 / 44

Why Not Use Multiple Trials to Construct an AIConcern 2: Diagnostic Effects
Tapering off medication after 12 weeks initial use may notproduce a higher proportion of responders at first, but may elicitsymptoms that allow you to better match subsequent treatmentto the child.
The improved matching (personalizing) on subsequenttreatments may result in a better response overall as comparedto any sequence of treatments that offered an additional 12weeks of medication after the initial 12 weeks.
Almirall, Collins, Murphy Building Adaptive Interventions 43 / 44
Why Not Use Multiple Trials to Construct an AIConcern 3: Cohort Effects
I Children enrolled in the initial and secondary trials may bedifferent.
I Children who remain in the trial(s) may be different.I Characteristics of adherent children may differ from study
to study.I Children that know they are undergoing adaptive
interventions may have different adherence patterns.
Bottom line: The population of children we are makinginferences about may simply be different from study-to-study.
Almirall, Collins, Murphy Building Adaptive Interventions 44 / 44