getting mothers with gestational diabetes to return for ... · getting mothers with gestational...
TRANSCRIPT
part of
33ISSN 1758-190710.2217/DMT.11.64 © 2012 Future Medicine Ltd Diabetes Manage. (2012) 2(1), 33–39
Summary The diagnosis of gestational diabetes is important for two reasons: to prevent adverse neonatal outcomes and identify women who are at high risk for developing diabetes in the future. The recommended screening test for diabetes postpartum in women with previous gestational diabetes is an oral glucose tolerance test. Screening rates postpartum using the recommended screening test remains disappointingly low in routine clinical practice. Simple reminders have been shown to increase screening rates but still result in a large proportion of women not being screened. This review will assess the rationale for screening postpartum and the barriers that have led to low screening rates.
Department of Medicine & Obstetrics/Gynecology at the University of Ottawa & Chief, Division of Endocrinology/Metabolism,
The Ottawa Hospital, ON, Canada
*Author for correspondence: Department of Medicine at the University of Ottawa & The Ottawa Hospital, Ottawa Health Research
Institute, Ottawa, ON, Canada; Tel.: +1 613 761 5164; Fax: +1 613 761 4036; [email protected]
� Gestational diabetes mellitus must be screened for in all pregnancies to prevent adverse pregnancy outcomes and to identify women for screening postpartum as there is an increased future risk of developing diabetes.
� Currently screening postpartum should be performed with an oral glucose tolerance test: fasting plasma glucose will miss 40% of women with dysglycemia postpartum, and it allows identification of women with impaired glucose tolerance who are at a higher risk of developing diabetes.
� Screening rates postpartum remain low due to a multitude of barriers. Simple reminders and nurse case managers have been shown to increase screening rates postpartum with an oral glucose tolerance test.
� Technologically advanced options (e.g. texting, SMS, e-mail and electronic health record reminders) need to be studied to evaluate if screening rates can be increased.
Prac
tice
Poi
nts
Getting mothers with gestational diabetes to return for postpartum testing: what works and what does not
management perspective
Heather D Clark* & Erin Keely
Gestational diabetes mellitus (GDM) is defined as carbohydrate intolerance of varying degree of severity with onset or first recognition in preg-nancy [1]. The incidence of GDM usually reflects the frequency of Type 2 diabetes (T2DM) in the underlying population as well as ethnicity and currently affects approximately 3–12% of the North American population [2]. There has been
a distinct increase in the prevalence of GDM over the past 20 years. In North America higher rates of immigration of high-risk populations owing to the adoption of a western lifestyle, higher birth rates in aboriginal populations, increasing rates of older maternal age at conception, and increasing obesity with a concomitant decrease in physical activity have all contributed to this increase [3].
Diabetes Manage. (2012) 2(1) future science group34
management PerSPective Clark & Keely
Rates of T2DM postpartum in women identified with gestational diabetes mellitus (GDM) range from 3% to over 70% in studies that examined women 6 weeks and up to 28 years postpartum [4]. A large population-based database in Ontario found the probability of developing T2DM in women who had GDM at 9 months postpartum of 3.7% and by 9 years a rate that was almost 20% compared with 2% in women who did not develop GDM [3]. Thus, women with GDM have a seven- to ten-fold increased risk of d eveloping T2DM within 10 years.
clinical practice guidelines for diagnosing gDm & postpartum screening � guidelines for diagnosis of gDm
The initial criteria for GDM diagnosis proposed by O’Sullivan and Mahan in 1964 were chosen to identify women at high risk of development of diabetes after pregnancy [5]. As the adverse effects of GDM on perinatal outcomes became increasingly recognized, the diagnosis of GDM was used to predict increased obstetrical risk [6,7]. However, the importance of postpartum screening to i dentify and prevent T2DM is still paramount.
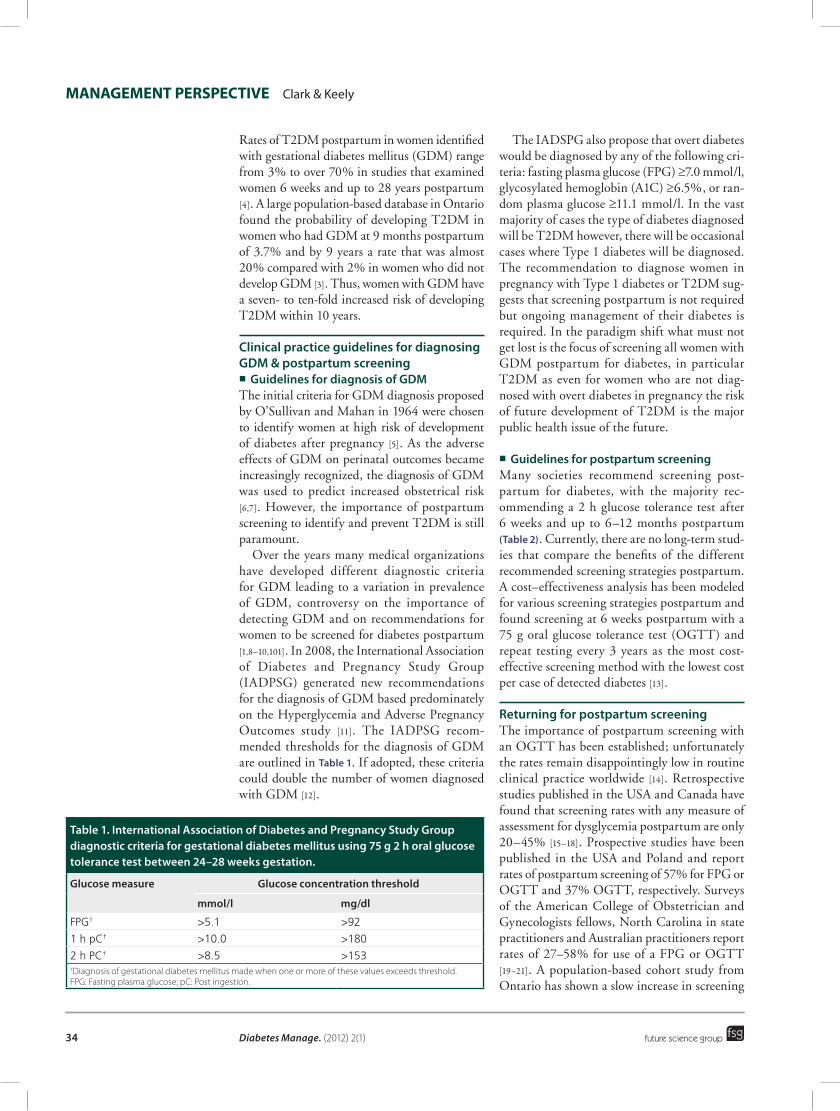
Over the years many medical organizations have developed different diagnostic criteria for GDM leading to a variation in prevalence of GDM, controversy on the importance of detecting GDM and on recommendations for women to be screened for diabetes postpartum [1,8–10,101]. In 2008, the International Association of Diabetes and Pregnancy Study Group (IADPSG) generated new recommendations for the diagnosis of GDM based predominately on the Hyperglycemia and Adverse Pregnancy Outcomes study [11]. The IADPSG recom-mended thresholds for the diagnosis of GDM are outlined in table 1. If adopted, these criteria could double the number of women diagnosed with GDM [12].
The IADSPG also propose that overt diabetes would be diagnosed by any of the following cri-teria: fasting plasma glucose (FPG) ≥7.0 mmol/l, glycosylated hemoglobin (A1C) ≥6.5%, or ran-dom plasma glucose ≥11.1 mmol/l. In the vast majority of cases the type of diabetes diagnosed will be T2DM however, there will be occasional cases where Type 1 diabetes will be diagnosed. The recommendation to diagnose women in pregnancy with Type 1 diabetes or T2DM sug-gests that screening postpartum is not required but ongoing management of their diabetes is required. In the paradigm shift what must not get lost is the focus of screening all women with GDM postpartum for diabetes, in particular T2DM as even for women who are not diag-nosed with overt diabetes in pregnancy the risk of future development of T2DM is the major public health issue of the future.
� guidelines for postpartum screeningMany societies recommend screening post-partum for diabetes, with the majority rec-ommending a 2 h glucose tolerance test after 6 weeks and up to 6–12 months postpartum (table 2). Currently, there are no long-term stud-ies that compare the benefits of the different recommended screening strategies postpartum. A cost–effectiveness analysis has been modeled for various screening strategies postpartum and found screening at 6 weeks postpartum with a 75 g oral glucose tolerance test (OGTT) and repeat testing every 3 years as the most cost-effective screening method with the lowest cost per case of detected diabetes [13].
returning for postpartum screeningThe importance of postpartum screening with an OGTT has been established; unfortunately the rates remain disappointingly low in routine clinical practice worldwide [14]. Retrospective studies published in the USA and Canada have found that screening rates with any measure of assessment for dysglycemia postpartum are only 20–45% [15–18]. Prospective studies have been published in the USA and Poland and report rates of postpartum screening of 57% for FPG or OGTT and 37% OGTT, respectively. Surveys of the American College of Obstetrician and Gynecologists fellows, North Carolina in state practitioners and Australian practitioners report rates of 27–58% for use of a FPG or OGTT [19–21]. A population-based cohort study from Ontario has shown a slow increase in screening
table 1. international association of Diabetes and pregnancy study group diagnostic criteria for gestational diabetes mellitus using 75 g 2 h oral glucose tolerance test between 24–28 weeks gestation.
glucose measure glucose concentration threshold
mmol/l mg/dl
FPG† >5.1 >92
1 h pC† >10.0 >180
2 h PC† >8.5 >153†Diagnosis of gestational diabetes mellitus made when one or more of these values exceeds threshold.FPG: Fasting plasma glucose; pC: Post ingestion.

Gestational diabetes & postpartum testing management PerSPective
future science group www.futuremedicine.com 35
rates over time, reaching a rate of 16% of women having an OGTT and 40% either a FPG or OGTT [22].
Barriers to screening postpartumBarriers to screening postpartum are most likely multifactorial; they may be related to knowledge and/or attitudes, accountability and fragmenta-tion of care and also may be related to logistical challenges and are outlined in Box 1.
� providersDiscrepancy in guideline recommendations for postpartum screening impact on postpartum screening rates and may affect providers’ opinion on the importance of postpartum screening. A clear and consistent message needs to be deliv-ered about the importance of postpartum test-ing [23]. Screening is important for the follow-ing reasons: early intervention in prediabetes has been shown to delay or prevent the diagnosis of diabetes [24–26]; identification of women at high risk for metabolic syndrome would determine ongoing surveillance and intervention which may decrease future cardiovascular risk [27,28]; and women who may conceive, identification of diabetes before the next pregnancy would reduce first trimester exposure to hyperglycemia diminishing the risk of congenital anomalies, m iscarriage or stillbirth [29,30].
Fragmentation of medical care from the pre-natal to postpartum period may contribute to lack of screening as these women are transitioned from obstetrical care and/or specialist care (endocrinology or internal medicine) during the pregnancy and returned to their primary-care provider (PCP) [31]. Internists/endocrinologists are more likely to order an OGTT postpar-tum and women who return for postpartum
ambulatory visits are also more likely to be screened [22,31]. When surveyed, 75% of fel-lows of the American College of Obstetrician and Gynecologists report routinely perform-ing a postpartum evaluation of glucose toler-ance reflecting the importance of screening [32]. However, in practice a retrospective chart review of women with GDM at a major academic hos-pital found only 30% of obstetricians were ordering any postpartum screening or explic-itly referring to the PCP for screening [15]. In Ontario from a population cohort study obstetri-cians ordered the fewest OGTTs in women with GDM postpartum [22]. The obstetrical provider takes responsibility for the postpartum visit but may not be perceived as being responsible for diabetes screening postpartum.
Lack of communication between obstetrical-care providers, internist/endocrinologist for GDM and the PCP also contributes to lack of screening postpartum. One study found that even when an electronic medical record is used and shared between care providers GDM was entered as a diagnostic code in only 30% of cases and approximately 45% had any documentation of GDM in the electronic medical record [21].
Other logistical challenges include lack of access to any postpartum care. If healthcare benefits end at 6 weeks postpartum in the USA some women may not be able to access care later for screening.
� Ogtt is a cumbersome testThe OGTT is a cumbersome test and is infre-quently carried out in routine practice. The logistics of arranging the test and ensuring women are fasting for the OGTT may con-tribute to the low postpartum screening rates [33]. The rationale for an OGTT postpartum
table 2. postpartum screening recommendations for women with gestational diabetes mellitus.
medical society (year) recommendation ref.
CDA (2008) 75 g OGTT 6 weeks–6 months postpartum and screening as per high-risk groups after that; prepregnancy screening for T2DM is also recommended
[8]
ADA (2008) 75 g OGTT or FPG with annual repeat testing if IFG/IGT is detected and every 3 years if glycemic levels are normal
[9]
5th International Workshop Group on GDM (2007)
Early postpartum with FPG or rPG, 75 g OGTT 6 weeks–1 year postpartum, annually FPG, triannually 75 g OGTT, planned prepregnancy 75 g OGTT
[1]
WHO (2006) 75 g OGTT >6 weeks postpartum [101]
SOGC (2002) 75 g OGTT 6 weeks–6 months postpartum [51]
ACOG (2001) 75 g OGTT or FPG 6–12 weeks postpartum [52]
ACOG: American College of Obstetrics and Gynecology; ADA: American Diabetes Association; CDA: Canadian Diabetes Association; FPG: Fasting plasma glucose; GDM: Gestational diabetes mellitus; IFG: Impaired fasting glucose; IGT: Impaired glucose tolerance; OGTT: Oral glucose tolerance test; rPG: Random plasma glucose; SOGC: Society of Obstetricians and Gynecologists of Canada; T2DM: Type 2 diabetes mellitus.

Diabetes Manage. (2012) 2(1) future science group36
management PerSPective Clark & Keely
as the recommended screening test is based on two principles. First, several studies have shown that a FPG alone has a low sensitivity for diag-nosing diabetes postpartum [34,35]. Second, only an OGTT allows diagnosis of impaired glucose tolerance (IGT), a FPG would miss up to 40% of women with IGT, an important predictor of future risk of T2DM and cardiovascular health. The benefits of accuracy of diagnosis and oppor-tunity to identify IGT with an OGTT must be weighed against the convenience, cost and poor reproducibility. Many clinical trials have demonstrated that T2DM may be delayed, if not prevented in high-risk patients (those with IGT) through lifestyle modifications and phar-macotherapy [24–26,36,37]. Although these studies did not specifically target women with GDM, The Diabetes Prevention Program did look at a subset of the patients who had a self-reported history of GDM and found a similar reduction in development of T2DM with lifestyle modi-fication as compared with the non-GDM group and an increased reduction in the development of T2DM with metformin than the non-GDM group, suggesting that pharmacological inter-vention for prevention of T2DM may be even more effective in women with a history of GDM compared with others [38]. GDM and a post-partum OGTT offers the opportunity for the medical system to identify women who need
to be followed more closely over time given the high probability of future development of T2DM and the evidence that lifestyle modifi-cation may change this outcome. It is incum-bent on us in the medical profession to offer s creening and ongoing management of these patients.
Alternative tests that are less-time inten-sive may need to be investigated to improve ease of screening. A FPG misses up to 40% of abnormal results, however, one could place an emphasis on impaired fasting glu-cose (IFG; 6.0–6.9 mmol/l) or even a lower target (5.6 mmol/l) as a threshold for ongo-ing follow-up and screening [34,35]. An A1C may be an alternative test for consideration for screening postpartum as fasting would not be required. Recently, an international expert committee appointed by the American Diabetes Association (ADA) endorsed the use of A1C for screening for T2DM outside of pregnancy. The assay has been standardized internationally and A1C values are relatively stable after collection [39]. The diagnostic threshold of A1C ≥6.5% has been proposed as it is at least as predictive as FPG and 2 h PG values for detecting dia-betes. Further studies to determine the opti-mal approach to postpartum screening and d iagnosis are required.
� patient factorsThe vast majority of women do not return for postpartum screening. There are many potential patient factors that may impact on post partum screening. Patient characteristics associated with increased screening have been reported in women who were married, older, had more education and a higher income although studies have been conflicting [14,17,31,40]. Women who would be perceived as at a clinically-higher risk of developing T2DM in the near future have been shown in studies as being less likely to return for screening [35,41]. Risk perception is an important motivator for compliance with testing and lifestyle intervention. However, several studies have shown that women with GDM do not perceive themselves as being at high risk for T2DM [35,42,43]. These studies suggest that there is a definite need to increase awareness among patients of the increased risk of d eveloping T2DM.
Postpartum surveys of women with previous GDM have identified several barriers to screen-ing. Perceived barriers include: lack of awareness
Box 1. Barriers to screening postpartum for diabetes.
provider � Variation in guidelines � Fragmentation of medical care � Lack of communication between care
providers � Lack of documentation in electronic medical
record � Primary responsibility for screening � Personal values
test characteristic � OGTT not performed routinely � OGTT requires fasting � OGTT requires a test 2 h later
patient � Perception of risk � Lack of time postpartum � Personal values � Deniability � Lack of access to medical care
OGTT: Oral glucose tolerance test.

Gestational diabetes & postpartum testing management PerSPective
future science group www.futuremedicine.com 37
of the need for the test, a perception of good health and not needing further care, afraid of being diagnosed with diabetes, negative expe-riences with care received during their preg-nancy, and time and logistics factors to attend an OGTT [44,45].
How can we increase screening rates?Despite the increasing realization of the poor compliance with postpartum screening for women with GDM there has been very little published about interventions to try to improve adherence with guidelines. Development of multifaceted interventions to increase screen-ing will be challenging as there is lack of com-plete understanding of the barriers physicians and patients face. A few prospective studies have looked at simple interventions to increase screening postpartum. One center reported on using a case manager nurse to follow GDM patients. The case manager focused on instruct-ing patients on the importance of follow-up testing and the life-long risk of diabetes and facilitated postpartum screening by providing laboratory requisitions, reminders and even vis-iting the woman at home to perform the test [35]. They reported any postpartum screening was completed in 57% of women with 72% of those completing a 2 h OGTT.
Reminders have been identified by patients and providers as a useful tool for improving postpartum testing rates [44,46]. Our group has performed a randomized controlled trial of reminders and found if the patient, the PCP or both received the reminder, screening rates increased fourfold from 14% for no reminder to approximately 60% [47]. With this result we implemented a reminder system in our routine clinical practice [48] and found rates of post-partum screening in routine clinical practice were lower than the randomized controlled trial (28 vs 60%); the higher rates in the interven-tion trial may reflect the added importance placed on screening postpartum by the health-care team as also demonstrated in previous studies [34,47–49]. Areas that might improve screening in routine clinical practice include electronic reminders to the women (text, SMS, e-mail) and the physician (electronic health reminders) although this has not been stud-ied. As part of the implementation strategy for the 2008 Canadian Diabetes Clinical Practice Guidelines, the Canadian Diabetes Association (CDA) has moved forward and produced
reminder tools for patients and providers [102]. Scheduled visits to healthcare providers post-
partum, either with an endocrinologist or inter-nist or during the 6-week routine follow-up visit with the obstetrician where the pregnancy-care provider ordered the test have been associated with higher rates of screening [31,50]. However, both patients and providers value the role of the PCP in postpartum testing [46]. Improved com-munication between providers and patients and between obstetrical and PCP is essential to facili-tate postpartum care. It is essential that the PCP be made aware of the diagnosis of GDM and rec-ommendations for screening for their patients. In addition, contributing to poor screening rates the women may not be returning to their PCP in a timely fashion and hopefully increased com-munication between healthcare providers would improve this [46].
Future perspectiveAs the recommendations from the IASDPG are incorporated by clinical societies there will be an increase in the number of women diagnosed with GDM and more importantly more women will be given a diagnosis of diabetes in preg-nancy (majority T2DM). Even with the early diagnosis of women with T2DM in pregnancy, screening postpartum will remain important for the prevention and early postpartum diagnosis of diabetes allowing the incorporation of inter-ventions to prevent complications of the disease. Pregnancy and the opportunity for screening of GDM and diabetes in general is a unique opportunity for future preventive healthcare in women. There are significant implications to the women’s health during the pregnancy and postpartum as well as significant effects for the baby also during the pregnancy and post-partum. The responsibility for coordinating postpartum screening must be made explicit so all providers know their role. Reminders and case management have been shown to increase screening rates for diabetes postpartum. These methods under rigorous study conditions still result in approximately 40% of women not being screened in a timely fashion. Scheduled visits with specialized-care providers have also been associated with increased screening. Although, further studies on interventions to improve screening rates are needed, we must act now and adopt some of the known methods that have increased screening rates. It is in the best interest of our patients and their future health.
Diabetes Manage. (2012) 2(1) future science group38
management PerSPective Clark & Keely
Financial & competing interests disclosureThe authors have no relevant affiliations or finan-cial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consul-tancies, honoraria, stock ownership or options, expert t estimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the p roduction of this manuscript.
referencesPapers of special note have been highlighted as:� of interest
1 Metzger BE, Buchanan TA, Coustan DR et al. Summary and recommendations of the Fifth International Workshop – Conference on Gestational Diabetes Mellitus. Diabetes Care 30(Suppl. 2), S251–S260 (2007).
2 Ferrara A. Increasing prevalence of gestational diabetes mellitus: a public health perspective. Diabetes Care 30(Suppl. 2), S141–S146 (2007).
3 Feig DS, Zinman B, Wang X, Hux JE. Risk of development of diabetes mellitus after diagnosis of gestational diabetes. CMAJ 179(3), 229–234 (2008).
� Reports the best estimate of the development of diabetes postpartum over time.
4 Kim C, Newton KM, Knopp RH, Kim C, Newton KM, Knopp RH. Gestational diabetes and the incidence of Type 2 diabetes: a systematic review. Diabetes Care 25(10), 1862–1868 (2002).
� Reviews the literature, to date, of the risk of developing of diabetes postpartum.
5 O’Sullivan JB, Mahan CM. Criteria for the oral glucose tolerance test in pregnancy. Diabetes 13, 278–285 (1964).
6 Crowther CA, Hiller JE, Moss JR et al. Effect of treatment of gestational diabetes mellitus on pregnancy outcomes. N. Engl. J. Med. 352(24), 2477–2486 (2005).
� Demonstrates that treatment of gestational diabetes mellitus (GDM) makes a difference.
7 Landon MB, Spong CY, Thom E et al. A multicenter, randomized trial of treatment for mild gestational diabetes. N. Engl. J. Med. 361(14), 1339–1348 (2009).
� Does not demonstrate that treatment of mild GDM makes a difference.
8 Canadian Diabetes Association. Canadian diabetes association 2008 clinical practice
guidelines for the prevention and management of diabetes in Canada. Can. J. Diabet. 32(Suppl. 1), S1–S201 (2008).
9 American Diabetes Association. Standards of medical care in diabetes – 2008. Diabetes Care 31(Suppl. 1), S12–S54 (2008).
10 Sacks DA, Sacks DA. Gestational diabetes – whom do we treat? N. Engl. J. Med. 361(14), 1396–1398 (2009).
11 International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 33(3), 676–682 (2010).
12 Moses RG. New consensus criteria for GDM: problem solved or a pandora’s box? Diabetes Care 33(3), 690–691 (2010).
13 Kim C, Herman WH, Vijan S, Kim C, Herman WH, Vijan S. Efficacy and cost of postpartum screening strategies for diabetes among women with histories of gestational diabetes mellitus. Diabetes Care 30(5), 1102–1106 (2007).
� The only study that evaluates the economics of screening.
14 Hunt KJ, Logan SL, Conway DL, Korte JE. Postpartum screening following GDM: how well are we doing? Curr. Diab. Rep. 10(3), 235–241 (2010).
15 Almario CV, Ecker T, Moroz LA et al. Obstetricians seldom provide postpartum diabetes screening for women with gestational diabetes. Am. J. Obstet. Gynecol. 198(5), 528 (2008).
� Assesses rates of postpartum screening.
16 Kim C, McEwen LN, Kerr EA et al. Preventive counseling among women with histories of gestational diabetes mellitus. Diabetes Care 30(10), 2489–2495 (2007).
� Evaluates whether preventive counseling increased screening postpartum.
17 Russell MA, Phipps MG, Olson CL et al. Rates of postpartum glucose testing after gestational diabetes mellitus. Obstet. Gynecol. 108(6), 1456–1462 (2006).
� Assesses rates of postpartum screening.
18 Smirnakis KV, Chasan-Taber L, Wolf M et al. Postpartum diabetes screening in women with a history of gestational diabetes. Obstet. Gynecol. 106(6), 1297–1303 (2005).
� Assesses rates of postpartum screening by obstetricians.
19 Baker AM, Brody SC, Salisbury K, Schectman R, Hartmann KE. Postpartum
glucose tolerance screening in women with gestational diabetes in the state of North Carolina. NC Med. J. 70(1), 14–19 (2009).
� Assesses rates of postpartum screening in North Carolina.
20 Morrison MK, Collins CE, Lowe JM. Postnatal testing for diabetes in Australian women following gestational diabetes mellitus. Aust. NZ J. Obstet. Gynaecol. 49(5), 494–498 (2009).
� Assesses rates of postpartum screening in Australia.
21 Stuebe A, Ecker J, Bates DW, Zera C, Bentley-Lewis R, Seely E. Barriers to follow-up for women with a history of gestational diabetes. Am. J. Perinatol. 27(9), 705–710 (2010).
� Evaluated barriers to screening postpartum.
22 Shah BR, Lipscombe LL, Feig DS, Lowe JM. Missed opportunities for Type 2 diabetes testing following gestational diabetes: a population-based cohort study. BJOG 118(12), 1484–1490 (2011).
� Evalauted rates of postpartum screening.
23 Agarwal MM, Dhatt GS, Punnose J et al. Gestational diabetes: dilemma caused by multiple international diagnostic criteria. Diabet. Med. 22(12), 1731–1736 (2005).
24 Knowler WC, Barrett-Connor E, Fowler SE et al. Reduction in the incidence of Type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 346(6), 393–403 (2002).
� Showed that treatment of people with impaired glucose tolerance (IGT) delayed the diagnosis of diabetes.
25 Pan XR, Li GW, Hu YH et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and diabetes study. Diabetes Care 20(4), 537–544 (1997).
� Showed that treatment of people with IGT delayed diagnosis of diabetes.
26 Tuomilehto J, Lindstrom J, Eriksson JG et al. Prevention of Type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 344(18), 1343–1350 (2001).
� Showed that treatment of people with IGT delayed the diagnosis of diabetes.
27 Albareda M, Caballero A, Badell G et al. Metabolic syndrome at follow-up in women with and without gestational diabetes mellitus in index pregnancy. Metabolism 54(8), 1115–1121 (2005).
future science group www.futuremedicine.com 39
Gestational diabetes & postpartum testing management PerSPective
28 Di CG, Ghio A, Resi V, Volpe L. Gestational diabetes mellitus: an opportunity to prevent Type 2 diabetes and cardiovascular disease in young women. Womens Health (Lond. Engl.) 6(1), 97–105 (2010).
� Review paper addressing the risk of metabolic syndrome and Type 2 diabetes on future cardiovascular risk in women with previous GDM.
29 Guerin A, Nisenbaum R, Ray JG, Guerin A, Nisenbaum R, Ray JG. Use of maternal GHb concentration to estimate the risk of congenital anomalies in the offspring of women with prepregnancy diabetes. Diabetes Care 30(7), 1920–1925 (2007).
� Determined the relationship between glycosylated hemoglobin and congenital anomalies.
30 Greene MF, Hare JW, Cloherty JP et al. First-trimester hemoglobin A1 and risk for major malformation and spontaneous abortion in diabetic pregnancy. Teratology 39(3), 225–231 (1989).
� Determined the relationship between glycosylated hemoglobin and congenital anomalies.
31 Kim C, Tabaei BP, Burke R et al. Missed opportunities for Type 2 diabetes mellitus screening among women with a history of gestational diabetes mellitus. Am. J. Public Health 96(9), 1643–1648 (2006).
� Evalauted rates of postpartum screening.
32 Gabbe SG, Gregory RP, Power ML et al. Management of diabetes mellitus by obstetrician-gynecologists. Obstet. Gynecol. 103(6), 1229–1234 (2004).
� Assesses rates of postpartum screening by obstetricians.
33 Ceccato NE, Ferris LE, Manuel D, Grimshaw JM. Adopting health behavior change theory throughout the clinical practice guideline process. J. Contin. Educ. Health Prof. 27(4), 201–207 (2007).
34 Reinblatt SL, Morin L, Meltzer SJ, Reinblatt SL, Morin L, Meltzer SJ. The importance of a postpartum 75 g oral glucose tolerance test in women with gestational diabetes. JOGC 28(8), 690–694 (2006).
� Evaluated the sensitivity of fasting plasma glucose versus oral glucose tolerance test for the diagnosis of diabetes postpartum.
35 Hunt KJ, Conway DL, Hunt KJ, Conway DL. Who returns for postpartum glucose screening following gestational diabetes mellitus? Am. J. Obstet. Gynecol. 198(4), 404–406 (2008).
� Looked at the prevalence of impaired glucose regulation postpartum on screening tests.
36 Xiang AH, Peters RK, Kjos SL et al. Effect of pioglitazone on pancreatic b-cell function and diabetes risk in Hispanic women with prior gestational diabetes. Diabetes 55(2), 517–522 (2006).
37 Gerstein HC, Yusuf S, Bosch J et al. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomised controlled trial. Lancet 368(9541), 1096–1105 (2006).
38 Ratner RE, Ratner RE. Prevention of Type 2 diabetes in women with previous gestational diabetes. Diabetes Care 30(Suppl. 2), S242–S245 (2007).
39 The international expert committee: international expert committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 32(7), 1327–1334 (2009).
40 Lawrence JM, Black MH, Hsu JW et al. Prevalence and timing of postpartum glucose testing and sustained glucose dysregulation after gestational diabetes mellitus. Diabetes Care 33(3), 569–576 (2010).
� Evalauted factors associated with screening postpartum.
41 Tan HH, Tan HK, Lim HS et al. Gestational diabetes mellitus: a call for systematic tracing. Ann. Acad. Med. Singapore 31(3), 281–284 (2002).
42 Kim C, McEwen LN, Piette JD et al. Risk perception for diabetes among women with histories of gestational diabetes mellitus. Diabetes Care 30(9), 2281–2286 (2007).
43 Morrison MK, Lowe JM, Collins CE. Perceived risk of Type 2 diabetes in Australian women with a recent history of gestational diabetes mellitus. Diabet. Med. 27(8), 882–886 (2010).
44 Sterne VL, Logan T, Palmer MA. Factors affecting attendance at postpartum diabetes screening in women with gestational diabetes mellitus. Practical Diabetes International 28(2), 64A–68A (2011).
� Evaluated barriers to screening postpartum.
45 Bennett WL, Ennen CS, Carrese JA et al. Barriers to and facilitators of postpartum follow-up care in women with recent gestational diabetes mellitus: a qualitative study. J Womens Health (Larchmt) 20, 239–245 (2011).
� Evaluated barriers and facilitators to screening postpartum.
46 Keely E, Clark H, Karovitch A, Graham I. Screening for Type 2 diabetes following gestational diabetes: family physician and patient perspectives. Can. Fam. Physician 56(6), 558–563 (2010).
� Evaluated barriers to screening postpartum.
47 Clark HD, Graham ID, Karovitch A et al. Do postal reminders increase postpartum screening of diabetes mellitus in women with gestational diabetes mellitus? A randomized controlled trial. Am. J. Obstet. Gynecol. 200(6), 634–637 (2009).
� Demonstrates that reminders increased screening postpartum.
48 Shea AK, Shah BR, Clark HD et al. The effectiveness of implementing a reminder system into routine clinical practice: does it increase postpartum screening in women with gestational diabetes? Chronic Dis. Can. 31(2), 58–64 (2011).
� Demonstrates that reminders increased screening postpartum.
49 Kaufmann RC, Schleyhahn FT, Huffman DG, Amankwah KS: Gestational diabetes diagnostic criteria: long-term maternal follow-up. Am. J. Obstet. Gynecol. 172(2 Pt 1), 621–625 (1995).
50 Ferrara A, Peng T, Kim C, Ferrara A, Peng T, Kim C: Trends in postpartum diabetes screening and subsequent diabetes and impaired fasting glucose among women with histories of gestational diabetes mellitus: a report from the Translating Research Into Action for Diabetes (TRIAD) Study. Diabetes Care 32(2), 269–274 (2009).
51 Berger H, Crane J, Farine D et al. Screening for gestational diabetes mellitus. J. Obstet.Gynaecol. Can. 24(11), 894–912 (2002).
52 Committee on Obstetric Practice. Committee on Obstetric Practice. ACOG Committee Opinion No. 435: postpartum screening for abnormal glucose tolerance in women who had gestational diabetes mellitus. Obstet. Gynecol, 113(6), 1419–1421 (2009).
� Websites101 WHO. Definition and diagnosis of diabetes
mellitus and intermediate hyperglycemia. http://whqlibdoc.who.int/publications/2006/9241594934_eng.pdf (Accessed 2 November 2011)
102 Canadian Diabetes Association. Make a difference: steps you can take to protect mothers and children. www.diabetes.ca/for-professionals/cpg/protecting-mothers-and-children (Accessed 2 November 2011)
