genomic and epigenomic profiles of gastrointestinal cancers · syed muhammad fahmy alkaff tony kiat...
TRANSCRIPT

Patrick Tan, MD PhD
Professor, Duke-NUS Medical School
Deputy Executive Director, Biomedical Research Council,
Agency for Science, Technology and Research (A*STAR)
30th European Congress of Pathology
Bilbao, Sept 2018
Genomic and Epigenomic Profiles of
Gastrointestinal Cancers

Enterprise | Interest
Patents related to cancer epigenomics

Tay et al., Cancer Research (2003)
Molecular and Clinical Heterogeneity in
Gastric Cancer
Tay et al., (2003) Cancer Research

Today’s Topics
1) What are the regulators of the cancer transcriptional
landscape?
- Epigenomics and Cancer Immunity
2) What are the Key Determinants for Development of
Gastric Cancer?
- Pre-Malignant Condition (Intestinal Metaplasia)

Cancer Gene Expression is Controlled by
Epigenomic Changes
Padmanabhan, Ushijima and Tan (2017)
Nature Reviews Gastro Hepat

Regulatory Elements can be Identified by
Histone Modifications
Modification Regulatory Elements
H3K4Me1 Enhancers
H3K4Me3H3K4Me2H2A.Z
Promoters
H3K27Ac Active Enhancers/ Promoters
H3K27Me3 Inactive Enhancers/ Promoters
H3K36Me3 Transcribed Regions
H3K9Me3 Constitutively Repressed Genes
Example
H3K4Me3
Active Promoter
PoisedPromoter
InactivePromoter
H3K27Me3

Gene Promoters : Critical Integrators of
Regulatory Inputs
Valen and Sandelin (2011) Trends in Genetics

>50% of Human Genes have Multiple Promoters
Davuluri et al (2008) Trends in Genetics

Epigenomic Promoter Profiling Localizes Somatic Promoters
19 N/T pairs + 12 cell lines (H3K4me3, H3K27ac, H3K4me1)
23,000 Promoter Elements (H3K4me3 High, H3K4me1 Low)
UnalteredTumor-Specific Gain
(Somatic Gain)Tumor-Specific Loss
(Somatic Loss)

Somatic Promoters are Correlated with H3K27ac Activity
and Frequently Map to Multi-Isoform Genes

18% of GC Somatic Promoters Comprise
Alternative Promoters

MET – Altered Signaling Shown by N-terminal
Promoter Variants
Muratani et al., 2014 Nat Comm
TCGA (Papillary RCC) 2016 NEJM
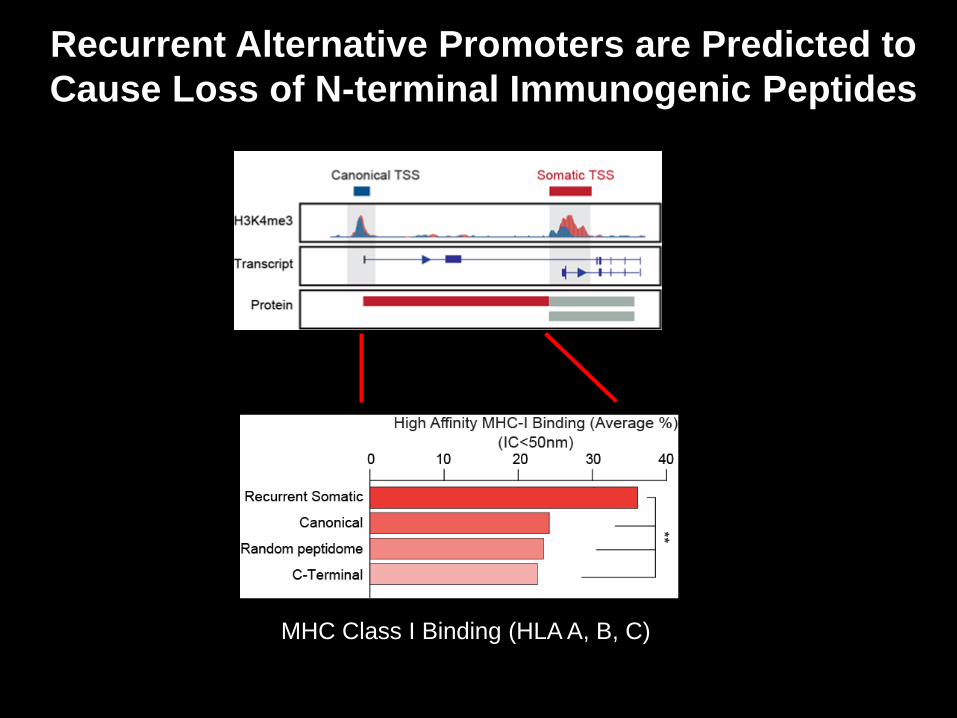
Recurrent Alternative Promoters are Predicted to
Cause Loss of N-terminal Immunogenic Peptides
MHC Class I Binding (HLA A, B, C)

Recurrent N-terminal Peptides Stimulate Immune
Responses in Experimental Systems (1)
EpiMAX Immune Profiling (Healthy Donors)

Recurrent N-terminal Peptides Stimulate Immune
Responses in Experimental Systems (2)

GCs with High Alternative Promoter Usage Exhibit
Decreased T-Cell Cytolytic Activity (GZMA, PRF1)*
TCGA – Nature 2014
(RNA-seq)
ACRG – Nat Med 2015
(Nanostring)
* Adjusted for mutation count and
tumor purity
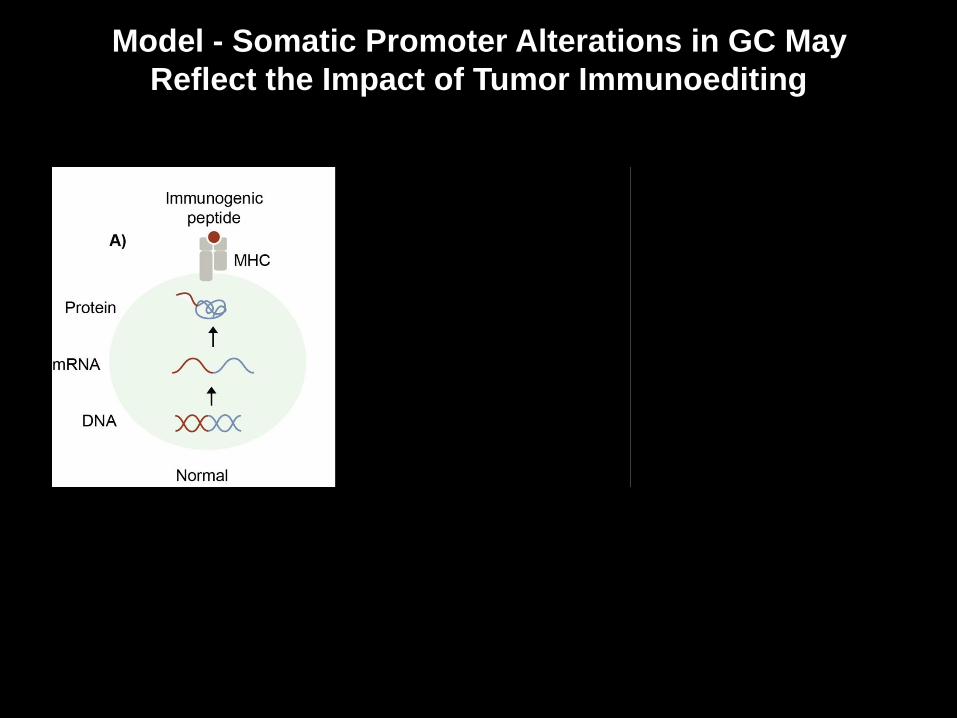
Model - Somatic Promoter Alterations in GC May
Reflect the Impact of Tumor Immunoediting

Summary
• Largest catalogue of epigenome-guided promoter
elements in gastric cancer
• Tumor-specific promoter alterations are widespread
and frequently map to multi-isoform genes
• Alternative promoters can drive expression of novel
pro-oncogenic isoforms (eg RASA3, MET)
• Alternative promoter usage may decrease
tumor antigenicity
• Somatic usage of alternative promoters
may facilitate immune evasion
Qamra et al., (2017) Cancer Discovery

Today’s Topics
1) What are the regulators of the cancer transcriptional
landscape?
- Epigenomics and Cancer Immunity
2) What are the Key Determinants for Development of
Gastric Cancer?
- Pre-Malignant Condition (Intestinal Metaplasia)

Compound Mechanism of action Treatment setting Reference
Cetuximab Anti-EGFR mAB 1st-line metastatic Lordick et al. 2013
Panitumumab Anti-EGFR mAB 1st-line metastatic Waddell et al. 2013
Gefitinib Anti-EGFR TKI 2nd-line metastatic Petty et al. 2017
Trastuzumab Anti-HER2 mAB 2nd-line metastatic Makiyama et al. 2018
Pertuzumab Anti-HER2 mAB 1st-line metastatic Tabernero et al. 2017
Lapatinib Anti-EGFR/HER2 TKI 2nd-line metastatic Satoh et al. 2014
Rilotumumab Anti-HGF mAB 1st-line metastatic Catenacci et al. 2017
Onartuzumab Anti-MET mAB 1st-line metastatic Shah et al. 2017
Napabucasin Anti-STAT3 2nd-line metastatic Shah et al. 2018
Bevacizumab Anti-VEGF mAB Perioperative Cunningham et al. 2017
Bevacizumab Anti-VEGF mAB 1st-line metastatic Ohtsu et al. 2011
Ramucirumab Anti-VEGFR-2 mAB 1st-line metastatic Fuchs et al. 2018
Olaparib PARP inhibitor 2nd-line metastatic Bang et al. 2017
Pembrolizumab PD-1-directed mAB 2nd-line metastatic Shitara et al. Lancet
2018
Advanced GC is Replete with Many Unsuccessful Phase III Trials
Lordick F (in press)

Gastric Cancer and Intra-Patient Heterogeneity
Sundar and Tan (2018) Cancer Discovery

Most Gastric Cancers* Follow a Multi-step
Carcinogenesis Sequence
Yeoh and Tan (2015) Gastroenterology
*Diffuse-type GC does not involve metaplasia

Gastric Cancer Epidemiology Program(GCEP)
Four Singapore Hospitals : NUH, SGH, TTSH, CGH
Funded by National Medical Research Council

GCEP Translational Study (“TransGCEP”)
Selection of High-Risk IM Patients (n=148)
56% moderate/marked IM
All Chinese
All positive for Hp serology
(Previous Infection)
Normal Mucosa
Mild IM (<30%)
IM (≥30% cellularity)
p value (IM vs Normal)
n=43 n=22 n=83
Age (year), mean ±SD
62±7 60±7 62±7 0.17
Race
Chinese 43 (100) 22 (100) 83 (100) --
Gender (%)
Male 22 (51) 12 (55) 42 (51) 1
Female 21 (49) 10 (45) 41 (49)
Smoking (%) 0.048
Current/ Ex-Smoker
9 (21) 4 (18) 32 (39)
Non-smoker 34 (79) 18 (82) 51 (61)
Alcohol consumption (%)
5 (12) 5 (23) 20 (24) 0.1
Family history of GC
in first-degree relative (%)
7 (16) 3 (14) 13 (16) 1
Hp serology positivity (%)
43 (100) 22 (100) 83 (100) --
Chronic gastritis (%) 38 (88) 22 (100) 83 (100) 0.004
Atrophic gastritis (%) 0 (0) 0 (0) 67 (81) --
Low Grade Dysplasia (%)
0 (0) 0 (0) 2 (2) --
EGN (%) 0 (0) 0 (0) 4 (5) --
Endoscopy
surveillance (months), mean ±SD
56±12 58±8 49±18 0.04

DNA Mutations – Point Mutations and Indels
(MAF>4%)
TP53 and ARID1A
Clonal Mutations are Rare
(TP53 – 2%; ARID1A – 3%)
Laser Capture Microdissection
Confirms Mutations in IM Cells
IMs Exhibit Low
Mutation Burdens
Compared to GC
NL
IM
GC

Copy Number Alterations and Telomere Erosion
MYC
NL IM
10% of IMs have sCNAs
Most sCNAs target Chr 8q
IMs have significantly shorter
Telomeres (Genome Instability)

Sequencing Detects More Hp-Infected IMs Compared
to Histology
All 15 have Hp DNA
(100%)33 cases have Hp DNA
(27%)

Genomic Sequencing Can Detect Active
Low-Level Hp Infection
Histology-confirmed HP cases
Show no Hp reads after eradication
(ie Hp DNA is transient)
Giemsa staining confirms Hp infection in
Sequencing positive cases

IMs Exhibit Global DNA Methylation Alterations
and a Subgroup is Hypermethylated
IMs Exhibit Increased
DNA Methylation
Normal Intestinal Metaplasia

IM Hypermethylation is Associated with Genes related
to Cell Fate Commitment and EZH2 Binding
EZH2 Chip-Seq
at IM Regions
Compared to Advanced GC
(CIN, EBV, MSI Subtypes)

IMs do *not* exhibit Intragenic DNA Hypomethyation
Signatures of Advanced GC
Globally, most cancers are
hypomethylated compared to normal tissues
(eg Berman et al 2012 Nat Genet)
Cancer hypomethylation occurs at repetitive and intragenic
regions, contributing to genomic instability
(Sheaffer et al 2016 Cancer Prev Res; Ehlich et al. 2009 Epigenomics)
DNA Hypomethylation is
Exclusively Seen in Advanced GC

Integration with Clinical Outcome
(Regression, Persistence, Progression)
TransGCEP
Samples
LGD/HGD
/EGC
Regression criteria based on Rugge et al (2003)
Progression includes both LGD and HGD, as both have higher GC risk than IM

Factors influencing IM regression and progression
Mutation Burden Telomere Length
DNA Methylation Copy Number Alterations
Regression

Summary Slide: What our Data Supports
Genomic profiling reveals that IMs exhibit low mutational
burdens compared with GCs
In general, TP53 and ARID1A mutations are rare in IM
Some IMs have FBXW7 mutations, chromosome 8q
amplifications, or shortened telomeres
Sequencing detects more IM patients with active H. pylori
infection than histology
(Epi)genomic alterations in IM predict
subsequent disesae progression or
regression
Huang et al., 2018 Cancer Cell

Acknowledgements
Chang Xu
Angie Lay Keng Tan
Minghui Lee
Suting Tay
Kakoli Das
Manjie Xing
Aliya Fatehullah
Syed Muhammad
Fahmy Alkaff
Tony Kiat Hon Lim
Jonathan Lee
Khek Yu Ho
Steven George Rozen
Bin Tean Teh
Nick Barker
Chung King Chia
Christopher Khor
Choon-Jin Ooi
Kwong Ming Fock
Jimmy So
Wee Chian Lim
Khoon Lin Ling
Tiing Leong Ang
Andrew Wong
Khay Guan YeohMing Teh
Kie Kyon Huang
Kalpana Ramnarayanan
Feng Zhu
Supriya Srivastava
Aditi Qamra
Manjie XingNisha Padmanabhan
Jeffrey Kwok
Shenli Zhang
Chang Xu
Yan Shan Leong
Lee-Lim Ai Ping
Qianqao Tang
John Connolly
Kyoung Mee-Kim
Jeeyun Lee
Dennis Kappei
Khay Guan Yeoh