geneva midwifery dialogue_23 feb15 - by jim campbell
TRANSCRIPT
The midwifery workforce: challenges and solutionsGeneva Dialogue: How many midwives does the world need?
A consultation to inform the UN Secretary-General’s Global Strategy on Women’s, Children’s and Adolescents’ Health
Palais de Nations, Geneva. 23rd February, 2015
Jim CampbellDirector, Health Workforce, WHO
Executive Director, Global Health Workforce Alliance

The challenges….some context
SDGs UHC GS2.0
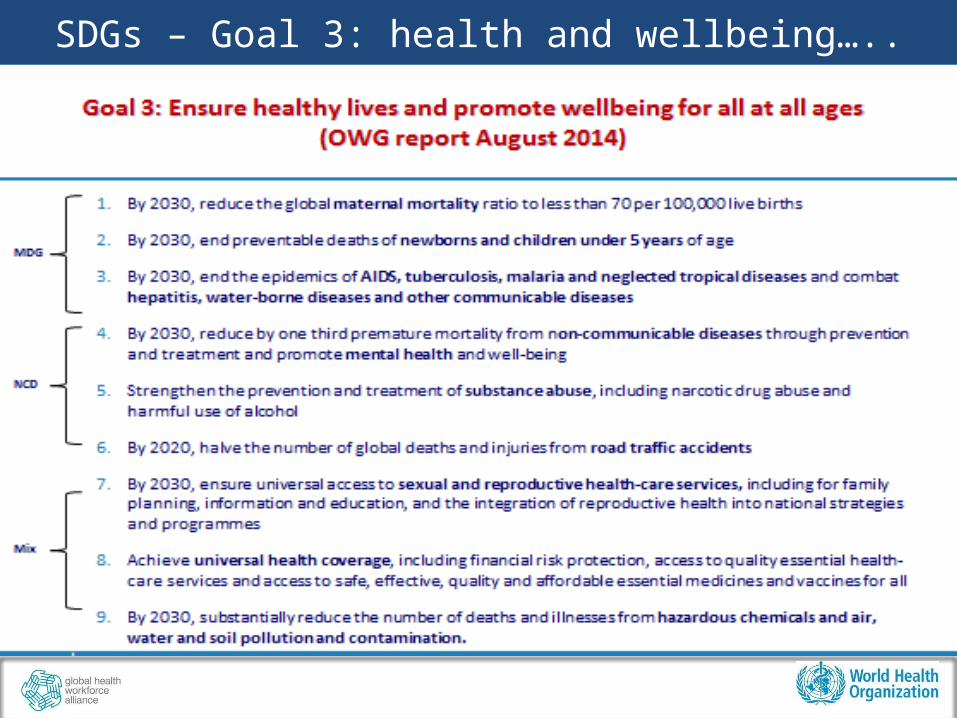
SDGs – Goal 3: health and wellbeing…..
SDGs – Goal 3: health and wellbeing…..
SDGs: Goal 3c: increase substantially …..the recruitment, development and training and retention of the health workforce……
“increase” -> requires a baseline and progress over time -> increase numbers (but not density/pop)
-> increase numbers (but more of the same)-> increase density (but not equity)-> increase density (but not effective coverage)
“substantially” -> vs. population/women’s need? -> vs. capacity to educate and retain (supply)?-> vs. financial resources to employ (demand)?
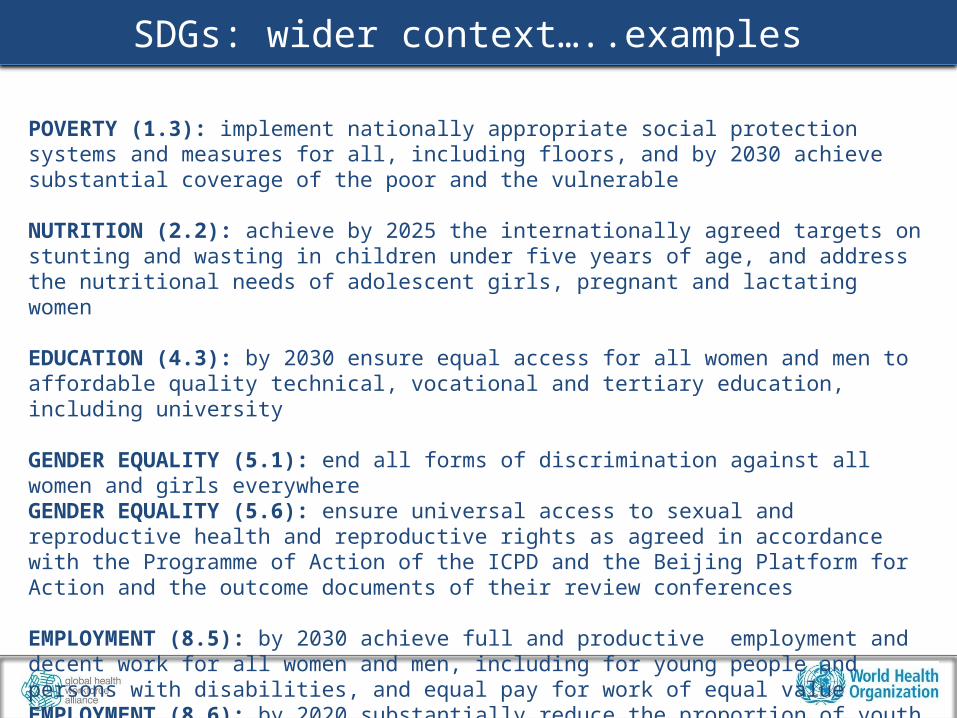
SDGs: wider context…..examples
POVERTY (1.3): implement nationally appropriate social protection systems and measures for all, including floors, and by 2030 achieve substantial coverage of the poor and the vulnerable
NUTRITION (2.2): achieve by 2025 the internationally agreed targets on stunting and wasting in children under five years of age, and address the nutritional needs of adolescent girls, pregnant and lactating women
EDUCATION (4.3): by 2030 ensure equal access for all women and men to affordable quality technical, vocational and tertiary education, including university
GENDER EQUALITY (5.1): end all forms of discrimination against all women and girls everywhere GENDER EQUALITY (5.6): ensure universal access to sexual and reproductive health and reproductive rights as agreed in accordance with the Programme of Action of the ICPD and the Beijing Platform for Action and the outcome documents of their review conferences
EMPLOYMENT (8.5): by 2030 achieve full and productive employment and decent work for all women and men, including for young people and persons with disabilities, and equal pay for work of equal valueEMPLOYMENT (8.6): by 2020 substantially reduce the proportion of youth not in employment, education or training
Source: OWG on SDGs (2014).

Universal Health Coverage…..
UHC
Source: WHO, World Bank (2014). Monitoring progress towards UHC at country and global levels: Framework, measures and targets.
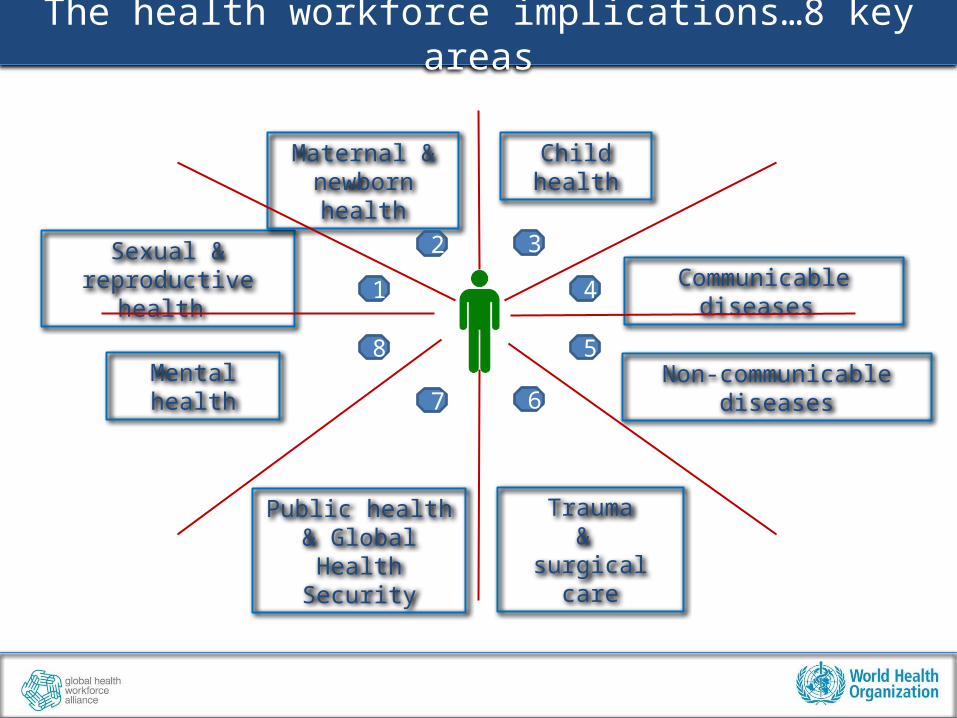
The health workforce implications…8 key areas
Sexual & reproductive health
Maternal & newborn health
Child health
Communicable diseases
Non-communicable diseasesMental health
Trauma&
surgical care
Public health & Global Health
Security
1
2
4
3
8
7
5
6
Health Workforce 2030………
Q: What are the health workforce implications of the SDGs, UHC and
GS2.0?
Q. What evidence can we draw upon?
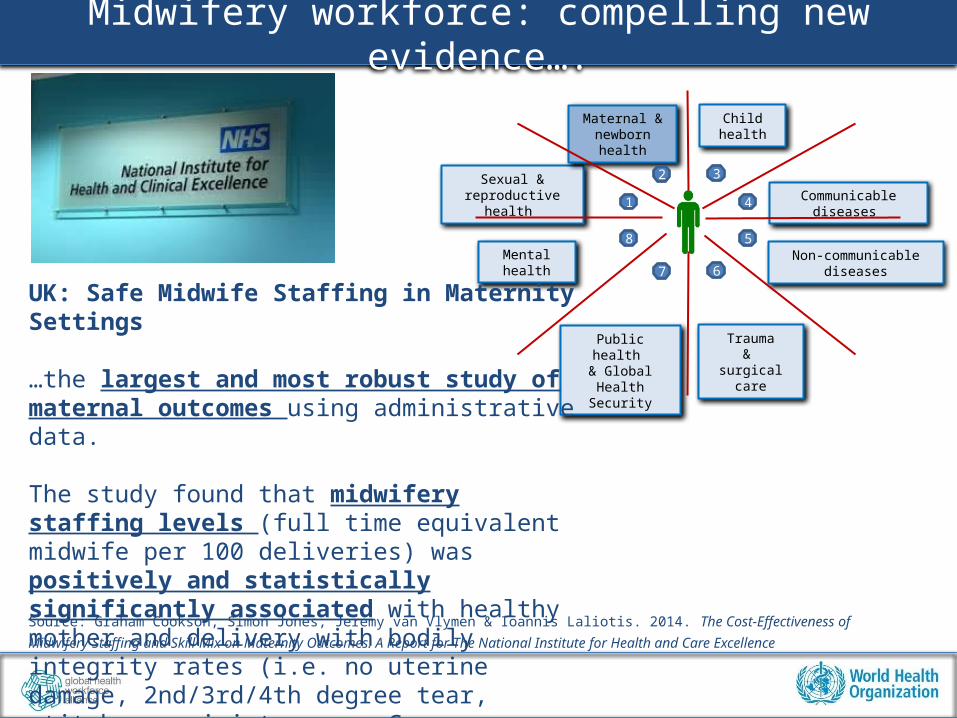
Midwifery workforce: compelling new evidence….
Sexual & reproductive health
Maternal & newborn health
Child health
Communicable diseases
Non-communicable diseasesMental health
Trauma&
surgical care
Public health & Global Health
Security
1
2
4
3
8
7
5
6
UK: Safe Midwife Staffing in Maternity Settings
…the largest and most robust study of maternal outcomes using administrative data.
The study found that midwifery staffing levels (full time equivalent midwife per 100 deliveries) was positively and statistically significantly associated with healthy mother and delivery with bodily integrity rates (i.e. no uterine damage, 2nd/3rd/4th degree tear, stitches, episiotomy, or Caesarean-section)
Source: Graham Cookson, Simon Jones, Jeremy van Vlymen & Ioannis Laliotis. 2014. The Cost-Effectiveness of Midwifery Staffing and Skill Mix on Maternity
Outcomes. A Report for The National Institute for Health and Care Excellence

Midwifery workforce: more compelling evidence….
Sexual & reproductive health
Maternal & newborn health
Child health
Communicable diseases
Non-communicable diseasesMental health
Trauma&
surgical care
Public health & Global Health
Security
1
2
4
3
8
7
5
6
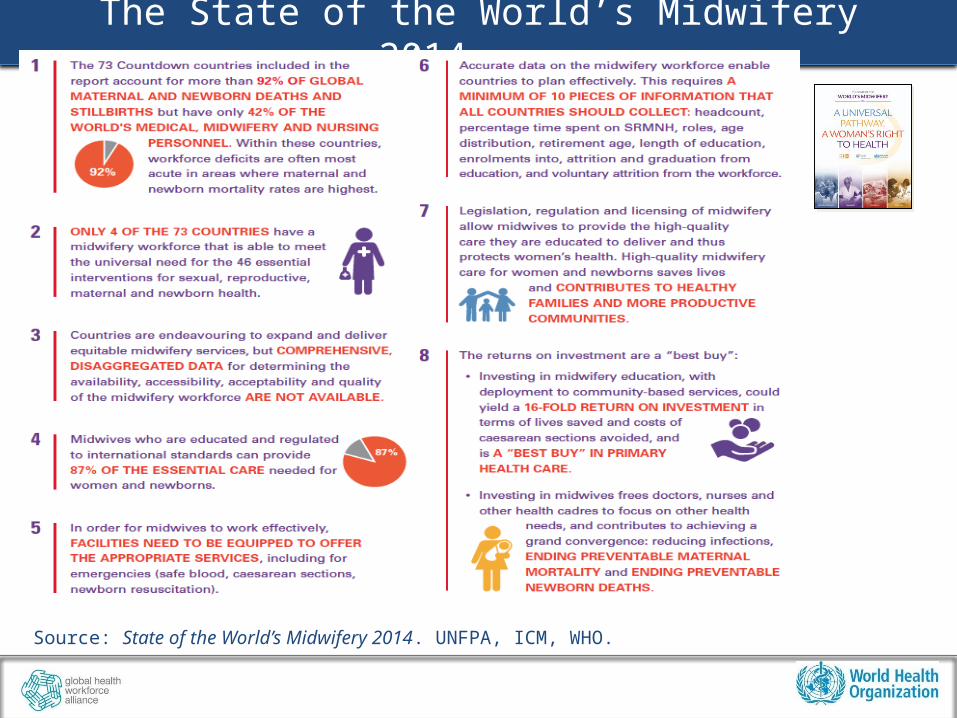
The State of the World’s Midwifery 2014....
“Midwifery workforce”
The health professionals whose primary function includes health services provided to women during pregnancy, labour and birth, as well as post-partum care for mothers and newborns. This includes midwives and others competent in the practice of midwifery, such as nurse-midwives and doctors with relevant competence (and in certain countries, auxiliary nurse midwives). These professionals are also referred to as skilled birth attendants [11].
Source: State of the World’s Midwifery 2014. p.206. UNFPA, ICM, WHO. adapted from ICM, UNFPA, WHO (2006) Midwifery in the Community: Lessons Learned.
The State of the World’s Midwifery 2014....
Source: State of the World’s Midwifery 2014. UNFPA, ICM, WHO.
Solutions: The message from Ban Ki-moon.....
Source: State of the World’s Midwifery 2014. UNFPA, ICM, WHO.
The midwifery workforce, within a supportive health system, can support women and girls to prevent unwanted pregnancies, provide assistance throughout pregnancy and childbirth, and save the lives of babies born too early.
I fully support the Midwifery 2030 vision articulated in this report. This vision is within reach of all countries, at all stages of economic and demographic transition.
Solutions: The evidence from Tim Evans.....
Source: State of the World’s Midwifery 2014. UNFPA, ICM, WHO.
Educating midwives results in good value for money. A targeted intervention for a community-based midwifery workforce ranks positively for economy, efficiency and effectiveness.
It has an impact comparable to that of child immunization, and could yield a 16-fold return on investment.
It is a “best buy” in primary health care.
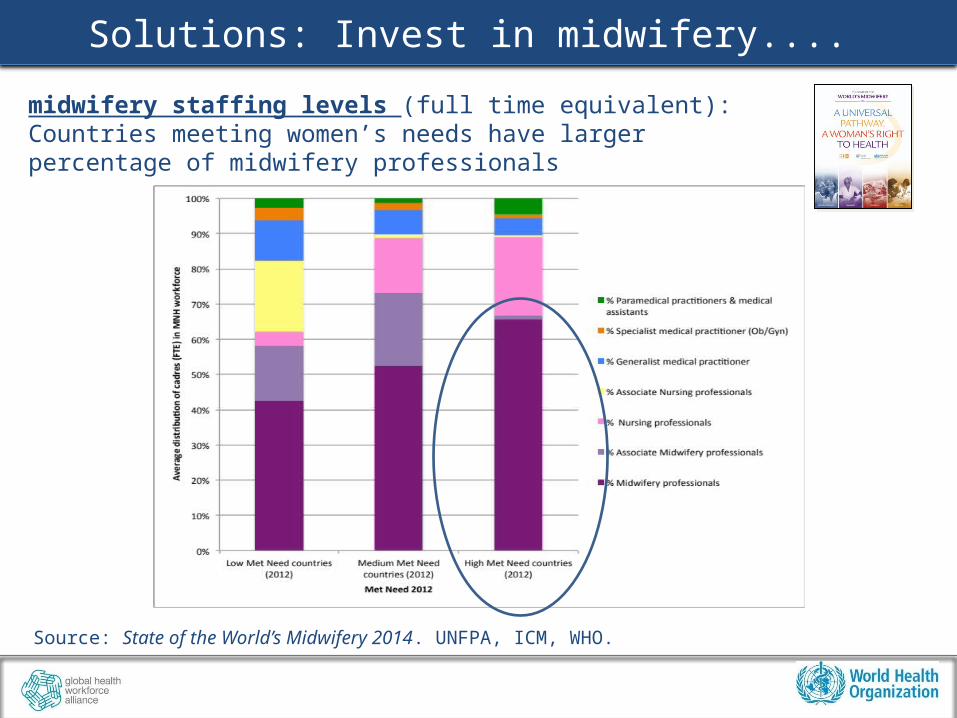
Solutions: Invest in midwifery....
Source: State of the World’s Midwifery 2014. UNFPA, ICM, WHO.
midwifery staffing levels (full time equivalent): Countries meeting women’s needs have larger percentage of midwifery professionals

Solutions: We must understand women’s needs
Examples from sub-Saharan Africa

Solutions: We must look where need is rising
Example: West & Central AfricaBetween 2012-2030, the health workforce in francophone West and Central Africa will need to respond to:• 1.1 billion antenatal visits• 0.2 billion births• 0.8 billion postnatal visits
Countries
Met need 2012
Met need 2030
Direction
Burkina Faso 37% 31% Decline
Cameroon 11% 18% Increase
Central African Republic 18% 17% Decline
Chad 8% 15% Increase
Congo 40% 21% Decline
DRC 53% 14% HIGH RISK: Decline
Gabon 99% 67% HIGH RISK: Decline
Guinea 30% 45% Increase
Mali 30% 27% Decline
Source: State of the World’s Midwifery 2014. UNFPA, ICM, WHO. Additional analysis by Maria Guerra-Arias, ICS Integrare
HOWEVER: Projections indicate not all countries will have a workforce that is able to meet women’s needs for the essential SRMNH services.
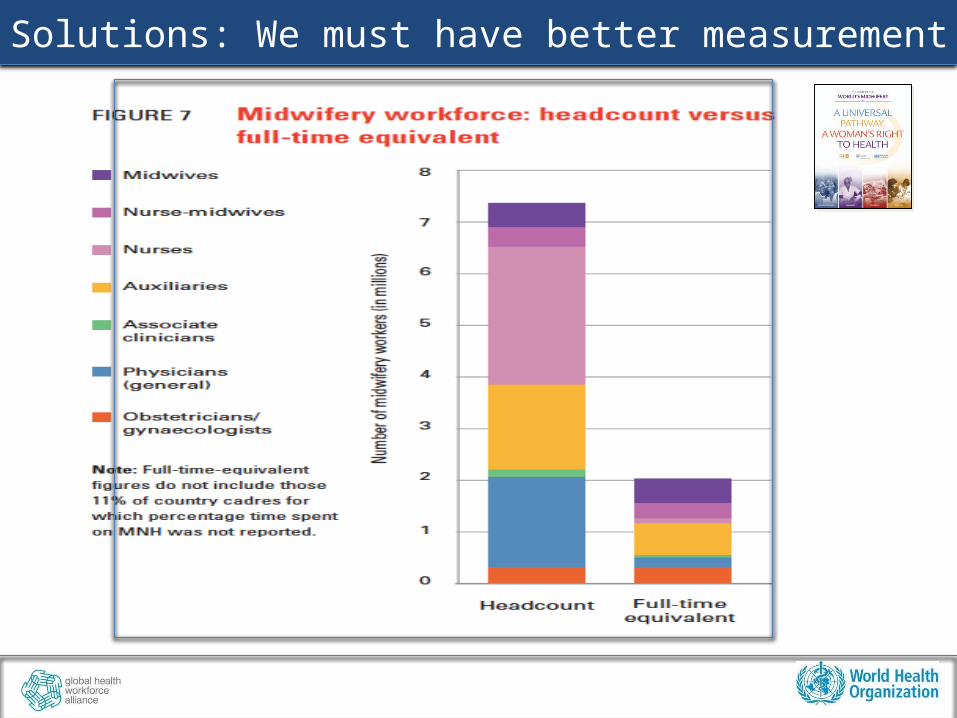
Solutions: We must have better measurement
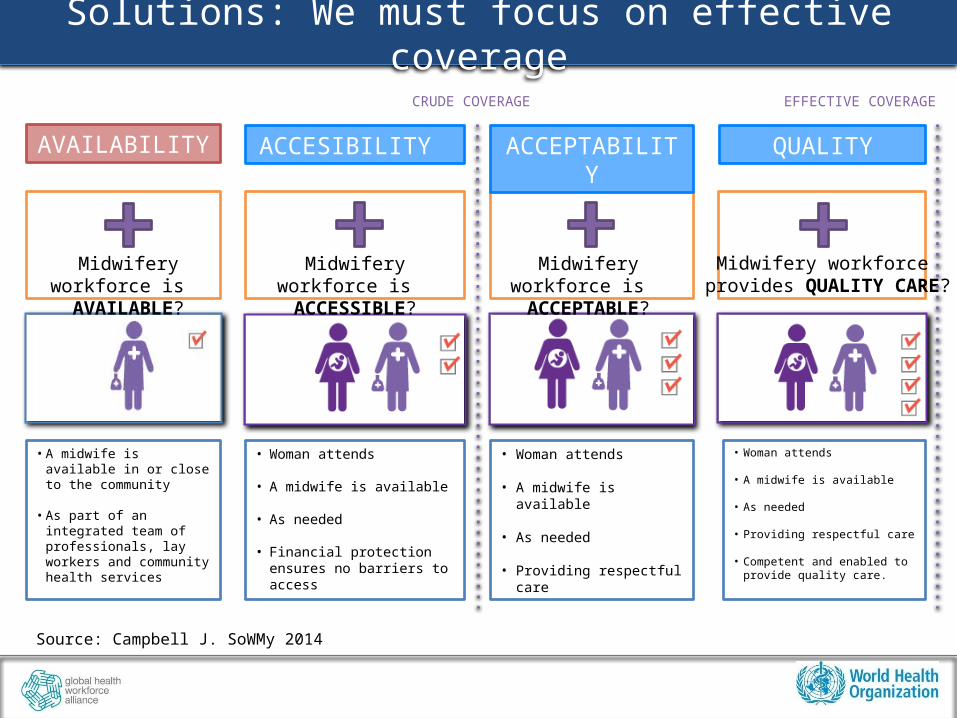
Solutions: We must focus on effective coverage
Midwifery workforce is AVAILABLE?
Midwifery workforce is ACCESSIBLE?
Midwifery workforce is ACCEPTABLE?
Midwifery workforce provides QUALITY CARE?
AVAILABILITY ACCESIBILITY ACCEPTABILITY QUALITY
• A midwife is available in or close to the community
• As part of an integrated team of professionals, lay workers and community health services
• Woman attends
• A midwife is available
• As needed
• Financial protection ensures no barriers to access
• Woman attends
• A midwife is available
• As needed
• Providing respectful care
• Woman attends
• A midwife is available
• As needed
• Providing respectful care
• Competent and enabled to provide quality care.
CRUDE COVERAGE EFFECTIVE COVERAGE
Source: Campbell J. SoWMy 2014
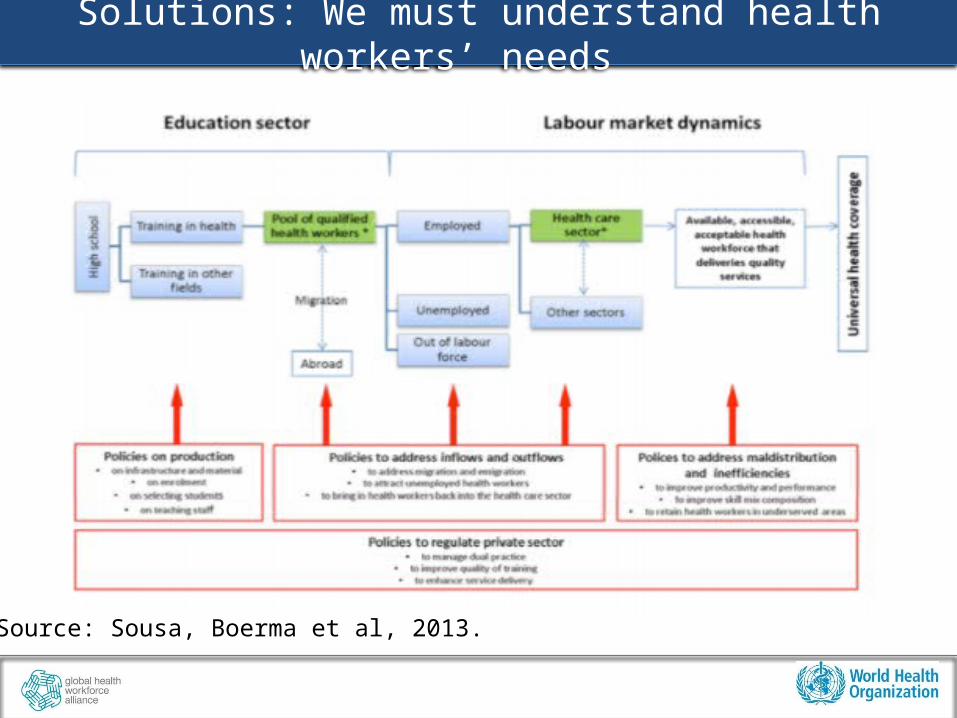
Solutions: We must understand health workers’ needs
Source: Sousa, Boerma et al, 2013.
Returning to the SDGs – Goal 3: health and wellbeing…..
SDGs: Goal 3c: increase substantially …..the recruitment, development and training and retention of the health workforce…
…especially in low- and middle-income countries…..
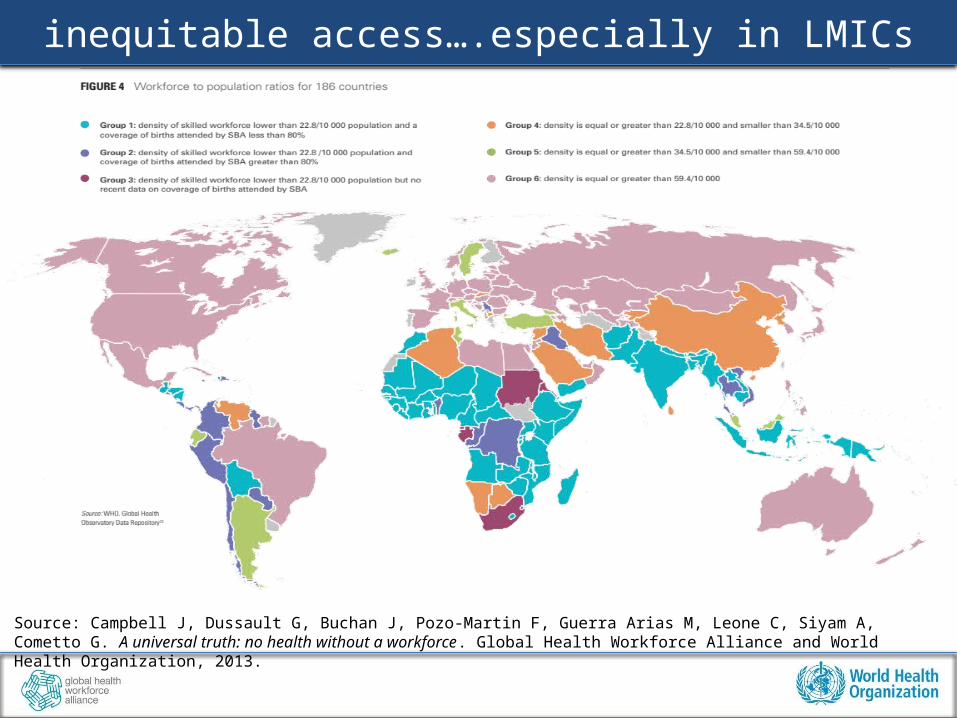
inequitable access….especially in LMICs
Source: Campbell J, Dussault G, Buchan J, Pozo-Martin F, Guerra Arias M, Leone C, Siyam A, Cometto G. A universal truth: no health without a workforce. Global Health Workforce Alliance and World Health Organization, 2013.

A message from Christine Lagarde.....
Source: Africa Rising—Building to the Future. Keynote Address by Christine Lagarde. Managing Director, International Monetary Fund. Maputo, May 29, 2014
Africa’s greatest potential is its people. They are the key for the region to fully capture the dividends from population growth. By some estimates, a one percentage point increase in the working age population can boost GDP growth by 0.5 percentage points. This is huge.
For this to happen, however, “good” jobs need to be created…..
My bottom line: invest in women. It has a great rate of return—economically and socially for the future.

Workforce 2030………
Q: What are the health workforce implications of the SDGs, UHC and
GS2.0?
A: Requires a new paradigm on future health employment
and economic growth.

THANK YOU!
- who.int/workforcealliance- @GHWAlliance #hrhstrategy- facebook.com/healthworkforce