general method for analysing dentist-patient interaction
TRANSCRIPT

General method for analysingdentist-patient interaction
i-lans Verheij\ Guusje ter l-lorst\Pier Prins^ and Jaap Veerkamp^'Department of Social Dentistry, ACTA,^Department of Clinical Psychology. Universityof Amsterdam, 'Department of Pedodonties,ACTA, Amsterdam
Verheij JGC, Horst G ter, Prins PJM, Veerkamp J: General method for analysingdentist-patient interaction. Cotnmunity Dent Oral Epidetniol 1989; 17: 173-6.
Abstract - The interaction between dentist and patient during dental treatment mayinfluence the frequency of dental visits in the future because this interaction mayincrease the dental fear of the patient. To find the characteristics of the dentist'sbehavior that increase or decrease dental fear a statistical analysis of the interactionmay be used. Data of such interactions are known as time series. Because it is highlyprobable that the behavior of an individual at two different points in time isautocorrclated a correct statistical analysis of the ititcraction between dentist andpatient tnust take this possibility into account. A general statistical tnethod isproposed that can take autocorrelations into account. The method is compared witha simpler method that may not deal adequately with autocorrelations.
Key words: behaviorai dental science:loglinear models: Markov chains
J. G. C. Verheij, Department of Social Dentistry,ACTA, Louwesweg 1, 1066 EA Amsterdam, TheNetherlands
Accepted for publication 22 November 1988
What patients experience during theirvisits to the dentist tnay detertnine thefrequency of their dental visits in the fu-ture. One of the factors that influence thefrequency of dental visits is dental fear(1). This fear may have several originsand one of these could be the patient'sexperience during previous dental treat-ments (2-8). If it is assumed that dentalfear is something that is learned duringdental treatment then it is necessary toknow which characteristics of the dentaltreatment lead to dental fear. One of thepossibilities is the behavior of the dentist(9). Moreover, when dental fear is some-thing that is acquired during dental treat-ment, the dental treattnent of childrenshould be structured in a way that avoidsthe learning of dental fear. If this learningeffect is avoided, children will visit thedentist tnore regularly when they havegrown up.
Little is known about the direct infiu-ence of the dendst's behavior duringtreatment on either the facilitation or re-duction of the patient's fear. A few stud-ies have, however, been conducted but ageneral method for analysing data fromthis type of research has been lacking. Ashas been shown (10) the conclusions maydepend on the method chosen to an-alyse the observations. Different conclu-sions may be reached when autocorrela-tions are present in the behavior of thedentist and the patient. These autocorre-lations can be taken into account in tnore
than one way and this leads to differentmethods to analyse the observations ofan investigation.
Observations of the interaction be-tween dentist and patient have as a gene-ral characteristic that they are recordedsequentially in time. Such observationsare known as time series in statisticalanalysis and several tnethods are avail-able to analyse these observations in acoherent tnanner. These statistical tech-niques can be divided into two groups.This division depends on the level oftneasuretnent of the variables in the in-vestigation. When the variables are tnea-sured on an interval scale or a higherscale the methods described in (for exam-ple) Box & jENKtNS (11) can be used.When, as in our study, the variables aretneasured on a lower scale other tech-niques are necessary. A description of thetechnique for this type of observationscan be found in BISHOP et al. (12). In thispaper a general description of the lattermethod will be given and it will be shownhow autocorrelations in both the beha-vior of the dentist and the patient can behandled within this framework. Also themethod proposed will he compared withthe method of WEINSTEIN et al. (14) andit will be shown that the method ofWEINSTHIN et al. (14) is a simpler versionof the general method that is proposedin this paper. The method proposed willbe illustrated with a simple example andfrom this example it can be seen that the
conclusions of an investigation dependon the way autocorrelations in both thebehavior of the dentist and the patientare handled. The data used in this exam-ple are frotn PRINS el al. (13) and thisreference must also be consulted for adetailed description of the design andprocedure of the exatnpie. Because of theobjectives stated above this paper alsorenders an account of the statistical anal-ysis that was used in (10) and (13).
iUateriai and methods
In the example that is used to illustratethe statistical technique the observationsare the repeated recordings of dentist andchild behavior during dental treatment.The treatment consisted of giving thechild a local anesthesia, preparitig a cavi-ty and restoring it without the use ofa rubber datn. Both dentist and childbehavior were scored using a modifiedversion of the coding scheme ofWEINSTEIN el al. (14). Behavior of dentistand child was scored in several behavior-al dimensions and each ditnension con-sisted of several types of behavior. Thebehavior of the child will be coded asfear related and noti fear related and onlyone ditnension of the dentist behaviorwill be used to illustrate the statisticaltechnique. Also the illustration will berestricted to 2 points in titne; i.e. timeT and time T-1. Thus only the relationbetween the behavior of the dentist and

174 VERHEI] ET AL.
child at points T and T-1 will be studied.These restrictions do not change the logicof the statistical tnethod.
Essentially the observations used tostudy the interaction between a dentistand a child consist of two time series.One for the dentist and one for the child.The research question would be: can thetitne series representing the behavior ofthe dentist be used to increase the pre-dictability of the behavior of the child.Stated differently, is there a relation be-tween the behavior of the dentist andthe child. Because two titne series areavailable, both can be used to predict theother. In the present example the timeseries representing the behavior of thedentist will be used to predict the beha-vior of the child. A probletn with thistype of observation is that there may bea relation between the behavior of thedentist at time T and time T-1. A relationmay also exist between the behavior ofthe child at time T and time T-1. Thisproblem is known as autocorrelation instatistical analysis. Because correlationsonly have meaning when variables aremeasured on an interval scale or higherthe tertn autodependence will be used inthe present context. Thus the behavior ofboth the dentist and the child may beautodependent.
Within the method proposed it is pos-sible to check the presence of autodepen-dence in the behavior of the dentist andthe child. Also the method can be usedwhether or not autodependence is pres-ent. The method is an application ofMarkov chain theory and uses loglinearmodel theory to test the presence of cer-tain effects. The method can be usedwhen all observations are included in theanalyses and when only behavioralchanges are irtcluded in the analysis. Theobservations are recorded in a multidi-mensional frequency table. In the presentexample the table has 16 entries becausethere are 4 variables with 2 categorieseach. These 4 variables are behavior ofthe dentist at time T, behavior of thedentist at time T-1, behavior of the childat time T, and behavior of the child attime T-1. Each variable has 2 eategories.The ftrst category represents absence ofthe behavior and the second categorypresence of the behavior. When all obser-vations are included in the analysis theduration of the behavior is taken intoaccount because in each tirjie interval abehavior is recorded. The corresponding
frequency table can have observations inall cells. In the second case only behav-ioral changes are recorded and thus theduration of the behavior is not taken intoaccount. The frequency table is the sameas in the ftrst case but has structural ze-roes. These zeroes represent cotnbina-tions of behavior that cannot occur with-in this recording scheme; i.e. the behaviorat time T is the same as the behavior attime T-1. These cotnbinatiotis are denot-ed by the technical term self-transitionsand the corresponding cells are excludedfrotn the analysis. Thus the satne fre-quency table can be used with both re-cording schetnes.
From a practical point of view includ-ing all observations in the analysis is thepreferred option. In this case the totalnumber of observations is larger andconsequently sotne effects can be estitnat-ed tnore accurately. If self-transitionsare excluded frotn the analysis the be-havior of the dentist and the child mustbe coded in at least 3 categories. Whenthere are fewer categories it is not pos-sible to test the presence of autodepen-dence. Furthermore the frequency tablebecotnes large very quickly and this de-pends on the number of categories usedto code the behavior. When self-transi-tions are included in the analysis the be-havior can be coded as present and notpresent. Now only 2 categories are need-ed per behavior and thus the frequencytable becomes as small as possible. Afurther point concerning the exclusion ofself-transitions is related to the commonnotion of causality. This notion statesthat the cause must precede the effect.When self-transitions are excluded fromthe analysis it is not known whether achange in behavior of the dentist oc-curred before or after a change in beha-vior of the child. Consequently it is notpossible to state that a change in beha-vior of the dentist caused a change inbehavior of the child. Thus both frotn apractical and theoretical point of view allobservations should be iticluded in theanalysis.
In the present exatnple variables 2 and3 are of interest. These variables repre-sent behavior of the dentist at time T-1and behavior of the child at time T.When there is a relation between these 2variables the behavior of the dentist af-fects of the child. This effect willbe written as [23] as is done by BISHOP etcd. (12). To test the presence of this rela-
tion WEINSTEIN et al. (14) use a statisticaltest that compares the conditional prob-ability of fear related behavior of thechild against the unconditional prob-ability of fear related behavior. The con-ditional probability is the probabilitythat the child will show fear related be-havior at time T given the behavior of thedentist at time T-1. The unconditionalprobability is the probability that thechild will show fear related behavior attime T without taking the behavior ofthe dentist into account. This testing pro-cedure can be translated to the presentfratnework. Within our approach thefour-ditnensional frequency table wouldbe summed over the variables 1 (behaviorof the dentist at time T) and 4 (behaviorof the child at time T-1). This resultsin a 2x2 frequency table with entriesbehavior of the dentist at time T-1 andbehavior of the child at titne T. Now thechi-square statistic for testing the relationbetween the behavior of the detitist attitne T-1 and the behavior of the childat titne T can be computed. Althoughdifferent in appearance the testing proce-dure of WEINSTEIN et al. (14) and thetesting procedure given above lead to ex-actly the satne results.
Within the present framework it be-comes clear what assumptions are neces-sary for the testing procedure ofWEINSTEIN et al. (14). As is well known,testing the association between variables2 and 3 (the association between the be-havior of the dentist at titne T-1 and thebehavior of the child at time T) with thetnethod described above is only possiblewhen there is no association betweenvariable 1 on one hand and variables 2and 3 on the other. The behavior of thedentist at time T must not be related tobehavior of the dentist at time T-1 norto the behavior of the child at titne T.Also there must be no association be-tween variable 4 and variable 2 or 3,which tneans that there tnust be no rela-tion between the behavior of the child attitne T atid the behavior of the child attitne T-1 nor to the behavior of the den-tist at titne T-1. In the present study thiswould mean that there must be no auto-dependence in the behavior of the dentistand the behavior of the child. Further-more at time T and T-1 there is no rela-tion between the behavior of the dentistand the behavior of the child. In ournotation this would itnply that the effects[12], [13], [24] and [34] would be zero.
Analvsis of dentist-patient interaetion 175
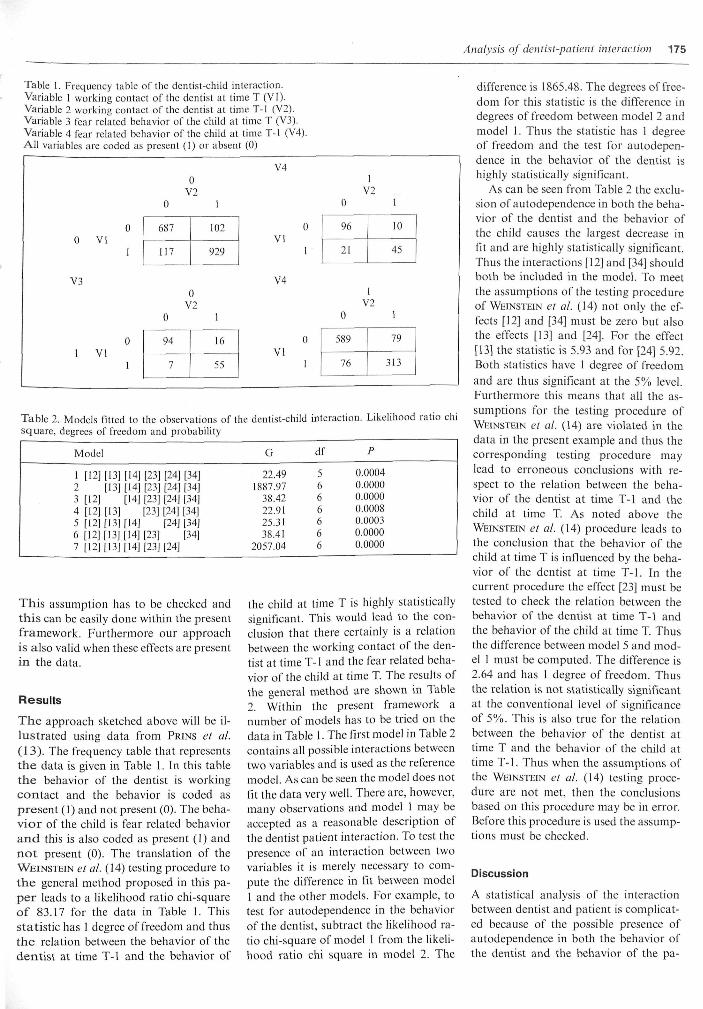
Table 1. Frequency table of the dentist-child interaction.Variable 1 working contact of the dentist at titne T (VI).Variable 2 working eontact of the dentist at time T-1 (V2).Variable 3 fear related behavior of the child at time T (V3).Variable 4 fear related behavior of the child at time T-I (V4).AH variables are coded as present (1) or absent (0)
Table 2. Models fttted to the observations of the dentist-child interaction. Likelihood ratio chisquare, degrees of freedom and probability
Model
1 [12][13]2 [13]3 [12]4 [12] [13]5 [12] [13]6 [12] [13]7 [12] [13]
[14][I4[[14]
[14][14]114]
[23][23][23][23]
[23][23]
[24[|24][24][241[24]
[24]
[34][34][34][34][34][34]
G
22.491887.97
38.4222.9125.3138.41
2057.04
df
5666666
P
0.0004
0.00000.00000.00080.00030.00000.0000
This assumption has to be checked andthis ean be easily done within the presentframework. Furthermore our approachis also valid when these effects are presentin the data.
Resuits
T h e approach sketched above will be il-lustrated using data frotn PRINS et al.(13). The frequency table that representsthe data is given in Table 1. In this tablethe behavior of the dentist is workingcontact and the behavior is coded aspresent (1) and not present (0). The beha-vior of the child is fear related behaviora n d this is also coded as present (1) andno t present (0). The translation of theWEINSTEIN et al. (14) testing procedure to
the general method proposed in this pa-pe r leads to a likelihood ratio chi-squareof 83.17 for the data in Table 1. Thisstatistic has 1 degree of freedotn and thusthe relation between the behavior of thedentist at time T-1 and the behavior of
the child at time T is highly statisticallysigniftcant. This would lead to the con-clusion that there certainly is a relationbetween the working contact of the den-tist at time T-1 and the fear related beha-vior of the child at time T. The results ofthe general method are shown in Table2. Within the present framework atiutnber of tnodels has to be tried on thedata in Table 1. The first model in Table 2contains all possible interactions betweentwo variables and is used as the referencemodel. As can be seen the model does notftt the data very well. There are, however,tnany observations and model 1 may beaccepted as a reasonable description ofthe dentist patient interaction. To test thepresence of an interaction between twovariables it is tnerely necessary to cotn-pute the difference in fit between model1 and the other models. For example, totest for autodependence in the behaviorof the dentist, subtract the likelihood ra-tio chi-square of tnodel 1 from the likeli-hood ratio chi square in model 2. The
difference is 1865.48. The degrees of free-dotn for this statistic is the difference indegrees of freedom between model 2 andmodel 1. Thus the statistic has 1 degreeof freedom and the test for autodepen-dence in the behavior of the dentist ishighly statistically significant.
As can be seen frotn Table 2 the exclu-sion of autodependence in both the beha-vior of the dentist and the behavior ofthe child causes the largest decrease itifit and are highly statistically significant.Thus the interactions [12] and [34] shouldboth be included in the model. To meetthe assumptions of the testing procedureof WEINSTEIN et al. (14) not only the ef-
fects [12] and [34] must be zero but alsothe effects [13] and [24]. For the effect[13] the statistic is 5.93 and for [24] 5.92.Both statistics have 1 degree of freedomand are thus significant at the 5% level.Furthermore this means that all the as-sumptions for the testing procedure ofWEINSTEIN et al. (14) are violated in the
data in the present example and thus thecorresponding testing procedure maylead to erroneous conclusions with re-spect to the relation between the beha-vior of the dentist at titne T-1 and thechild at time T. As noted above theWEINSTEIN et al. (IA) procedure leads to
the conclusion that the behavior of thechild at time T is influenced by the beha-vior of the dentist at time T-1. In thecurrent procedure the effeet [23] must betested to check the relation between thebehavior of the dentist at time T-1 andthe behavior of the child at time T. Thusthe difference between model 5 and mod-el 1 must be cotnputed. The difference is2.64 and has 1 degree of freedotn. Thusthe relation is not statistically significantat the conventional level of significanceof 5%. This is also true for the relationbetween the behavior of the dentist attime T and the behavior of the child attitne T-1. Thus when the assumptions ofthe WEINSTEIN et al. (14) testing proce-
dure are not met, then the conclusionsbased on this procedure may be in error.Before this procedure is used the assump-tions must be checked.
Discussion
A statistical analysis of the interactionbetween dentist and patient is complicat-ed because of the possible presence ofautodependence in both the behavior ofthe dentist and the behavior of the pa-

176 VERHEIJ ET AL.
tient. When autodependence is presentin the behavior of the dentist and thebehavior of the patient ignoring this au-todependence may lead to erroneousconclusions. In general it seems that toooften the conclusion is reached that thebehavior of the patient is influenced bythe behavior of the dentist when autode-pendence is ignored. At least when thepurpose of the investigation is to predictthe behavior of the patient. As has beenshown it is possible to do a correct statis-tical analysis and take autodependenceinto account. The same technique can heextended to as many time lags as arenecessary. In practice, however, the fre-quency table becomes large very quicklyand many cells of the table may containa small number of observations. For ex-ample in the present study the time lagswere 5 seconds apart. To investigate theinfluence of the last minute of behaviorof the dentist on the behavior of the child12 time lags are needed and this wouldrequire a frequency table of 4096*4096,which is about 16 million cells. Thusthere are practical limits to method pro-posed. The main value of the presentmethod may be that it makes clear whichassumptions are necessary to do a sim-pler statistical analysis of the interactionbetween dentist and patient. When theseassumptions are known it becomes pos-sible to judge the reasonableness of theassumptions.
Because Markov chain theory is usedto test the relation between the behaviorof the dentist and the behavior of thechild the assumptions that are necessaryfor such an analysis must also hechecked. It is assumed that the chain isstationary. This means that the prob-ability of changing from one type of be-havior to another is independent of thetime at which the behavioral change oc-curred. This assumption can only bechecked when there are observationsavailable for a number of dentist-patientinteractions. It is thus not possible to
check this assumption when observationsfor only one dentist-patient interactionare available. Furthermore in the presentexample it was assumed that the Markovchain is of order 1; i.e. the behavior attime T is only dependent on the be-havior at time T-1 and not dependent onthe behavior at time T-2, T-3, etc. Tocheck this assumption a frequency tablemust be created that is based on the as-sumption that the chain is of order 2.Now it can be checked whether the chainis of order 2 or order 1. The same proce-dure can be used to check whether thechain is of order 3, 4, etc. Thus in princi-ple both assumptions can be checked.Within the WEINSTEIN et al. (14) ap-proach the assumptions can not bechecked. Furthermore, within theWEINSTEIN et al. (14) procedure it is as-sumed that the Markov chain for both
the dentist and the patient is of order 0.A problem that is also related to the
size of the frequency table is caused bythe great number of dentist behaviors.The most desirable analysis would be toinclude all the behaviors of the dentist in1 frequency table and then one behaviorcan be tested taking into account all theother dentist behaviors. Because of prac-tical limitations this is, however, not pos-sible. The consequence of the separateanalysis of the dentist behaviors is thattoo tnany behaviors are related to thebehavior of the patient. This is causedby the fact that a nutnber of univariateanalyses are conducted and thus the ef-fects of the other dentist behaviors arenot taken into account when testing theeffect ofa particular behavior of the den-tist. This problem is also present in theprocedure of WEINSTEIN et al. (14).
References1. SCHUURS AHB. Factors associated with regutarity of dentat attendance. An experimental
psyehotogicat investigation. Thesis, University of Amsterdam, 1984.2. BERGGREN U , MEUNERT G . Dental fear and avoidance: eauses, symptotns and eonsequences.
JADA 1984; 109: 247-51.3. KLEINKNECHT RA, KLEPAC RK, ALnxANi:)ER LD. Origins and characteristics of fear of
dentistry. JADA 1973: S6: 842-8.4. LAUTCH H . Dental phobia. I3r J Psycliiatr 1971: 119: 151-8.5. MoLtN C, SEEMAN K. Disproportionate dental anxiety. Acta Odontot Scand 1970; 28:
197-212.6. SHOBEN EJ, BORLAND I. An empirical study of the etiology of dental fears. J Ctin Psyeh
1954; 10: 171-4.7. FORGIONE C, CLARK RE. Comments on an empirical study of the etiology of dental fears.
/ Dent Res 1974; Ji.- 496.8. GALE EN. Fears of the dental situation. J Dent Res 1972; 5/.' 964-6.9. KLEtNKNECHT RA. Fear of dentistry: its development, measurement and implication. In:
WEtNSTElN P, ed. Advances in behaviorat researeh in dentistry. Seattle: University of Washing-ton, 1978.
10. HORST G TER, PRINS PJM, VEERKAMP J, VERHEIJ JGC. Interactions between dentists andanxious child patients: a behavorial analysis. Community Dent Oral Epidemiol 1987: 15:249-52.
11. Box GEP, JENKINS GM. Time .series amdysis: forecasting and control. San Francisco: Holden-Day, 1976.
12. BISHOP Y M M , FIENBERG SE, HOLLAND PW. Discrete multivciriate analysis. Cambridge, MA:MIT-Press, 1975.
13. PRINS PJM, VEERKAMP J, HORST G TER, JONG A DE. TAN L. Behavior of dentists and childpatients during treatment. Community Dent Oral Epidemiol 1987; 15: 253-7.
14. WEINSTEIN P, GETZ T, RATENER P, DOMOTO P. The effect of dentist's behaviors on fear relatedbehaviors in ehildren. JADA 1982; 104: 32-8.
