general abdominal radiography tony pease, dvm, ms assistant professor of radiology north carolina...
TRANSCRIPT

General Abdominal Radiography
Tony Pease, DVM, MSAssistant Professor of Radiology
North Carolina State University

Objectives
• Acquisition of radiographs
• Abdominal radiographic anatomy
• Radiographic patterns of abdominal disease
• Determine normal compared to abnormal
• Determine further evaluations needed

Reading
• Chapter 38– Pages 483-493

Abdominal Radiography
• Generally being replaced with ultrasound– Ultrasound does not give a global picture
• Radiographs are a snapshot of disease– 1/120th of a second picture
• Ultrasound is real time

Abdominal Anatomy
• A lot of organs in a small space
• Rely on location

Acquiring radiographs
• Relatively high kVp (70)– Moderate image contrast– Some of shades of grey– More than bone less than thorax
• Moderate mAs– Minimizes motion artifact– Maximizes contrast
• Enemas and fasting are helpful

Positioning
• Include caudal thorax
• Try to include greater trochanter of femur
• Center beam just caudal to the last rib



Large patients
• May need two films per view– Four films per study
– Make sure to overlap images

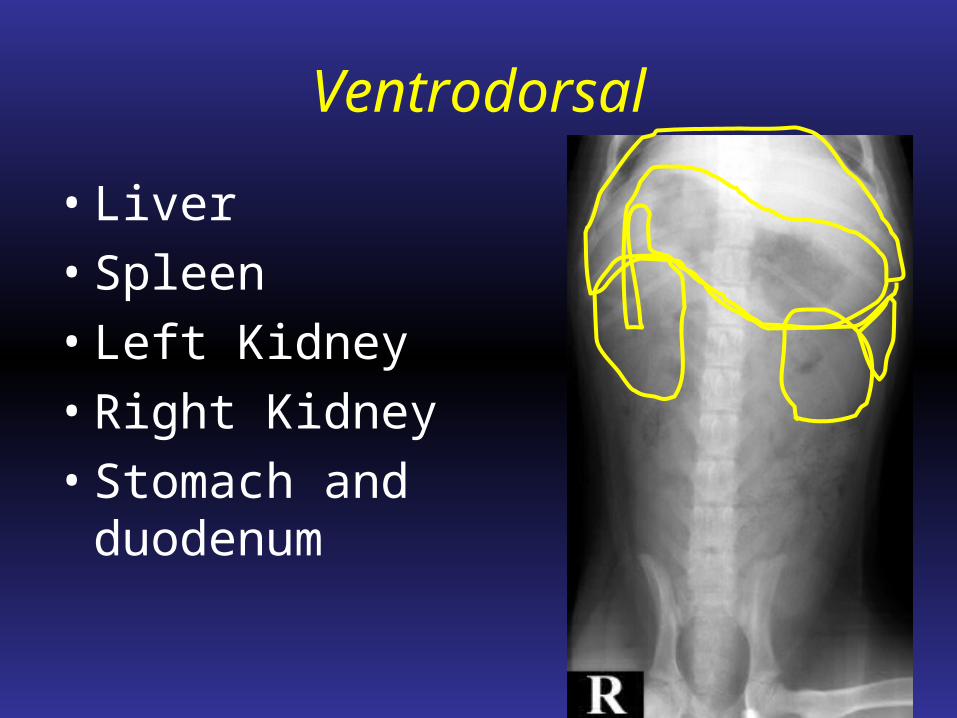
Ventrodorsal
• Liver
• Spleen
• Left Kidney
• Right Kidney
• Stomach and duodenum


Left lateral
• Esophagus• Pylorus• Duodenum• Liver• Spleen• Left kidney• Right kidney• Urinary bladder


Right lateral
• Fundus• Liver• Spleen• Left kidney• Right kidney• Urinary
bladder

Normal cat abdomen

Deep circumflex iliac artery
Sometimes confused for medial iliac lymph nodes or ureteral calculi

Positional radiographs
• Remember gas rises
• Can manipulate the animal

Can you see the gas?


Lateral horizontal beam

Horizontal beam
• Place the animal in left lateral– Puts the fundus of the stomach down
– Smaller pylorus is high
• Gas accumulates near the diaphragm

Some incidential findings
• Lucency on the ventral aspect of L3-4
• Cholesterol granulomas
• Spondylosis deformans

Lack of ventral aspect of L4
• It is where the diaphragm attaches

Cholesterol granuloma
• Generally in cats

Smooth bridging bone

Spaces of the abdomen
• Retroperitoneal– Dorsal to the colon
– Contains kidneys, adrenal glands, lymph nodes
– Continuous with mediastinum
• Peritoneal– Surrounds visceral organs
– Generally a potential space

Can compare spaces
Retroperitoneal space
Good detail
Peritoneal space
Poor detail
Loss of serosal detail
• Poor radiographic technique
• Fat content of a puppy or kitten
• Peritoneal fluid (many types)
• Carcinomatosis
• Lack of fat
• Peritonitis

Peritoneal fluid
• Soft tissue and fluid are similar opacity
• Therefore lose detail in the abdomen
• Ultrasound superior for peritoneal fluid
• Emaciation and fluid cause similar appearance, except for overall size of abdomen

Peritoneal fluid
• Multiple causes– Increased hydrostatic pressure– Decreased plasma colloid oncotic pressure– Capillary permeability
• Radiographs very insensitive for detecting• Cannot tell fluid type from radiographs

Mild
Severe Severe
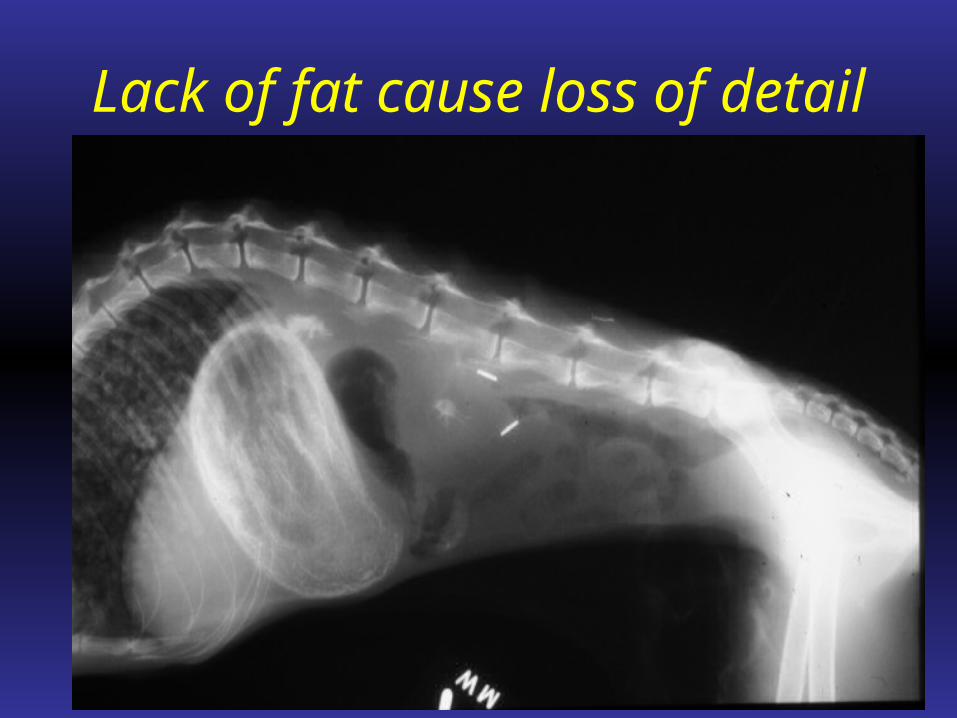
Lack of fat cause loss of detail

Is there peritoneal fluid?

Retroperitoneal space
• Only thing that is dorsal to the colon

Don’t forget that other view

Abdominal lymph nodes
• Many lymph nodes in abdomen
• Generally not seen radiographically– Even if large
• Medial iliac lymph nodes are the exception
• Ultrasound more useful for lymph nodes

Medial iliac lymph nodes

Don’t forget about goats
• Can help diagnose caseous lymphadenitis

Pneumoretropertioneum
• Retroperitoneum communicates with the mediastinum
• Therefore usually associated with:– Subcutaneous emphysema
– Pneumomediastinum
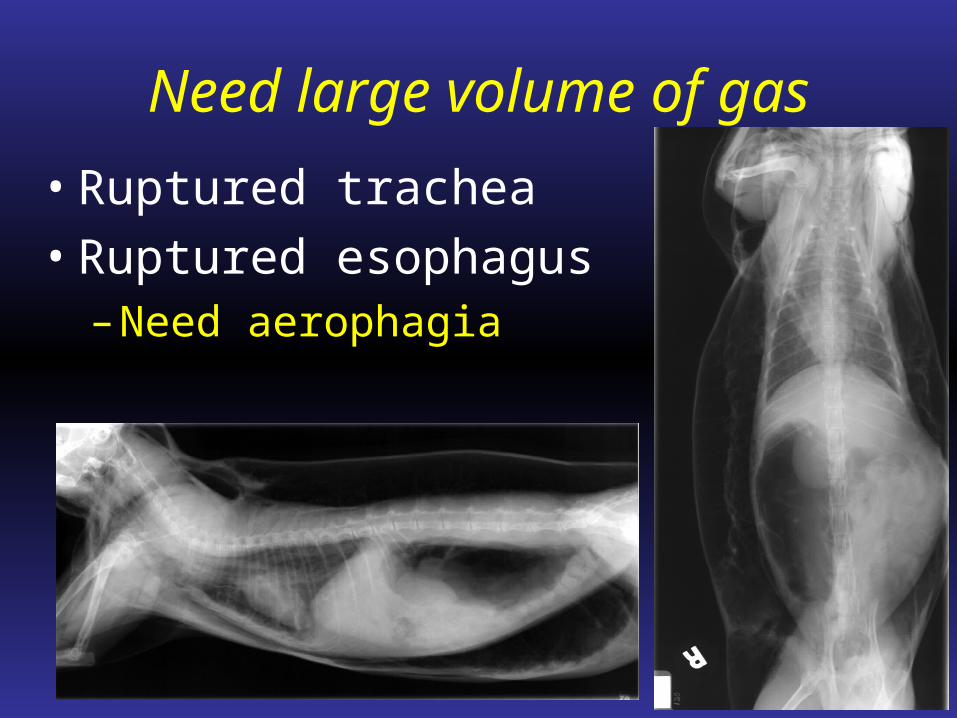
Need large volume of gas
• Ruptured trachea
• Ruptured esophagus– Need aerophagia

Pneumoretroperitoneum
• Not generally clinically important
• Just a sign of another disease

Even in the cow!

Pneumoperitoneum
• Can persist 10-14 days after surgery
• Rupture of a hollow viscus– Gastrointestinal perforation
– Surgical emergency!!
• External puncture wound

Several places to look

What about large animal?

Foals and calves
• Can image abdomen– Usually standing
– See fluid layers
• Can do barium enemas– Strictures or atresia ani

Ileus

Traumatic reticuloperitonitis

Traumatic reticuloperitonitis

All about the belly in 1 hour!
• Good general overview
• Over the next 3 weeks will be focused
• Radiographs are a good overview
• Helpful even if large animal
Questions?