gene expression based categorization of transplant pancreas biopsies fu l. luan m.d....
Post on 19-Dec-2015
217 views
TRANSCRIPT
Gene Expression Based Categorization of
Transplant Pancreas Biopsies
Fu L. Luan M.D.
University of Michigan

No disclosure to declare

Background
• Pancreas transplantation is an effective treatment for patients
with type 1 diabetes mellitus;
• Successful pancreas transplant establishes long-term
normoglycemia with no risk of hypoglycemia;
• Potential benefit on improvement of diabetic related end-
organ damage and cardiovascular risk factors;
• Potential benefit on extending patient survival;

Value of Pancreas Allograft on Patient Survival
P. Salvalaggio et al. Diabetes Care 32(4): 600-602; 2009

Effects of Pancreas Allograft on CVD Risks
Blood Pressure Total cholesterol
F. L. Luan, et al. Transplantation 84:541-544; 2007

Pancreas Transplants, by Transplant Type,1998-2007
1998 1999 2000 2001 2002 2003 2004 2005 2006 20070
400
800
1200
1600All Pancreas SPK PAK PTA
Nu
mb
er
of
Tra
nsp
lan
ts

1-Year 3-Year 5-Year 10-Year0%
20%
40%
60%
80%
100% SPK PTA PAK
Un
ad
just
ed
Gra
ft S
urv
iva
l (%
)
Unadjusted 1-Year, 3-Year, 5-Year, and 10-Year Pancreas Graft Survival

The Challenges to Maintain a Functioning Pancreas Allograft
• Complication related to graft and vascular
thrombosis accounts for about 20% of early graft
failure;
• Acute rejection as cause of graft failure within the
first year was reported at around 20%;
• Chronic rejection as cause of graft failure within the
first year was reported at around 19%;

• Pancreas allograft biopsy is the gold standard;
• Clinical indication remains subtle;
• Maryland classification, and lately Banff
classification provide guidance for clinicians;
• Response to the treatment varies;

Molecular Mechanisms Involved in Allograft Rejection and/or Failure
• Large amount of information available on molecular
mechanisms involved in kidney allograft rejection and/or
failure;
• Microarray technology has allowed better correlation of
sets of gene expression with transplant renal outcome;
• Little is known about molecular mechanisms involved in
pancreas allograft rejection or failure;

Hypothesis
• Pancreas allograft displays similar molecular
mechanisms in acute and chronic rejection, and/or
allograft failure;
• Pancreas allograft exhibits unique molecular markers
inherent to it’s organ specificity;
• The pattern of molecular expression in pancreas
allograft may correlates with the allograft outcome;

Materials and Methods
• 26 pancreas transplant biopsy and 4 human
pancreas specimens (unaffected area of tumor
pancreatectomies);
• All specimens were processed with fixation in
formaldehyde and paraffin-embedding ;
• Maryland classification for histological diagnosis;
• Patient management was individualized;

Technical Consideration (I)
• The formaldehyde-fixed, paraffin-embedded tissue samples
were cut in 5 µm sections;
• De-paraffinization was performed and followed by
rehydration;
• The sections (5 slides for each sample) were scraped off the
slides and harvested in appropriated lysis buffer;
• The total RNA was extracted using the phenol chloroform
protocol and reverse-transcribed into cDNA;

• TaqMan® Low Density arrays (TLDA) technique was employed
for parallel analysis of different mRNAs in samples;
• The cDNA expression value of each sample was compared
with other samples following the delta CT technique and the
expression of target genes was normalized to a calibrator;
• Real time RT-PCR expression values were analyzed with DChip
using 2D hierachical clustering for samples as well as for
genes;
Technical Consideration (II)

Unordered values, coded from low (green) to high (red)
?Can we group these patients and/or genesbased on the expression?
Consider the expression profiles for the samples and define a similarity, e.g correlation
S2
S1
S3
S3
1) Assess similarity between all combinations
2) Merge the two with the highest similarity
3) Repeat 1) and 2) until nothing left to merge
S3
S2
S1
S1
S2

?How meaningful are those groupings?
1) Initiate a perturbation by randomly removing one sample
2) Re-cluster3) Compare the
sample composition of the resulting clusters
If there is a clear structure (long branches) we probably capture some effect
Non-random data should be robust to perturbations

Selection of Gene Markers for the Study
• Molecules involved in rejection processes, both acute and
chronic, were obtained from the various literatures in kidney
transplantation;
• Molecules specific to pancreas, down-regulated during
disease processes and up-regulated during regeneration
processes, were obtained by searching publically available
dataset at http://www.ncbi.nlm.nih.gov/geo and
http://www.betacell.org;
• Molecules considered “house keeping genes” were chosen;
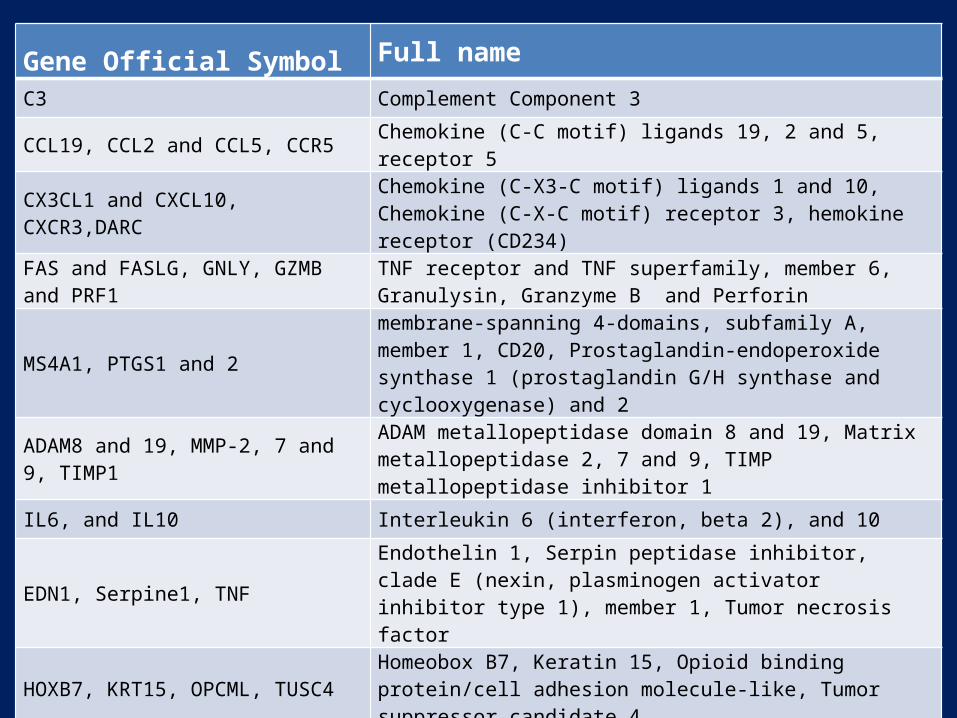
Gene Official Symbol Full name
C3 Complement Component 3
CCL19, CCL2 and CCL5, CCR5 Chemokine (C-C motif) ligands 19, 2 and 5, receptor 5
CX3CL1 and CXCL10, CXCR3,DARC Chemokine (C-X3-C motif) ligands 1 and 10, Chemokine (C-X-C motif) receptor 3, hemokine receptor (CD234)
FAS and FASLG, GNLY, GZMB and PRF1
TNF receptor and TNF superfamily, member 6, Granulysin, Granzyme B and Perforin
MS4A1, PTGS1 and 2membrane-spanning 4-domains, subfamily A, member 1, CD20, Prostaglandin-endoperoxide synthase 1 (prostaglandin G/H synthase and cyclooxygenase) and 2
ADAM8 and 19, MMP-2, 7 and 9, TIMP1 ADAM metallopeptidase domain 8 and 19, Matrix metallopeptidase 2, 7 and 9, TIMP metallopeptidase inhibitor 1
IL6, and IL10 Interleukin 6 (interferon, beta 2), and 10
EDN1, Serpine1, TNF Endothelin 1, Serpin peptidase inhibitor, clade E (nexin, plasminogen activator inhibitor type 1), member 1, Tumor necrosis factor
HOXB7, KRT15, OPCML, TUSC4 Homeobox B7, Keratin 15, Opioid binding protein/cell adhesion molecule-like, Tumor suppressor candidate 4
INS, GCG, SST, AMY1A,CCKAR, ELA2A
Insulin, Glucagon, Somatostatin, Amylase, alpha 1A, Cholecystokinin A receptor, Elastase 2A
PDX1, MAF, MAFB, NEUROD1Pancreatic and duodenal homeobox 1(Ipf1), V-maf musculoaponeurotic fibrosarcoma oncogene homolog and B, Neurogenic differentiation 1
POLR2A, PPIA, UBC, 18s rRNA and GAPDH
Polymerase (RNA) II (DNA directed) polypeptide A, Peptidylprolyl isomerase A, Ubiquitin C, 18s ribosomal RNA, Glyceraldehyde-3-phosphate dehydrogenase


Demographics of Study PopulationCluster A
N=7Cluster B (I)
N=12Cluster B (II)
N=7Age (years, S.D.) 37.7 + 6.2 37.3 + 6.3 34.9 + 4.5Sex (male, %) 6 (85.7) 6 (50.0) 5 (71.4)Race (AA, %) 2 (28.6) 1 (8.3) 1 (14.3)Type of transplant SPK (%) PAK (%)
6 (85.7)1 (14.3)
6 (50.0)6 (50.0)
2 (28.6)5 (71.4)
Induction Thymo/OKT3 (%) Basiliximab (%)
4 (57.1)3 (42.9)
3 (25.0)9 (75.0)
1 (14.3)5 (71.4)
CNI CsA (%) Tac (%)
2 (28.6)5 (71.4)
2 (16.7)10 (75.0)
1 (14.3)6 (85.7)

Clinical Phenotypes and Clustering
Cluster AN=7
Cluster B N=19
In=12
II n=7
Pancreas allograft failure (%) 1 (14.8) 8 (66.7) 5 (71.4)
Acute rejection (Maryland) III or lower (%) IV and V (%)
7 (100)0 (0)
7 (58.3)4 (33.3)
5 (71.4)1 (14.3)
Chronic rejection (%) 0 (0) 1 (8.3) 2 (28.6)
Positive CD20 expression (%) 0 (0) 0 (0) 4 (57.1)

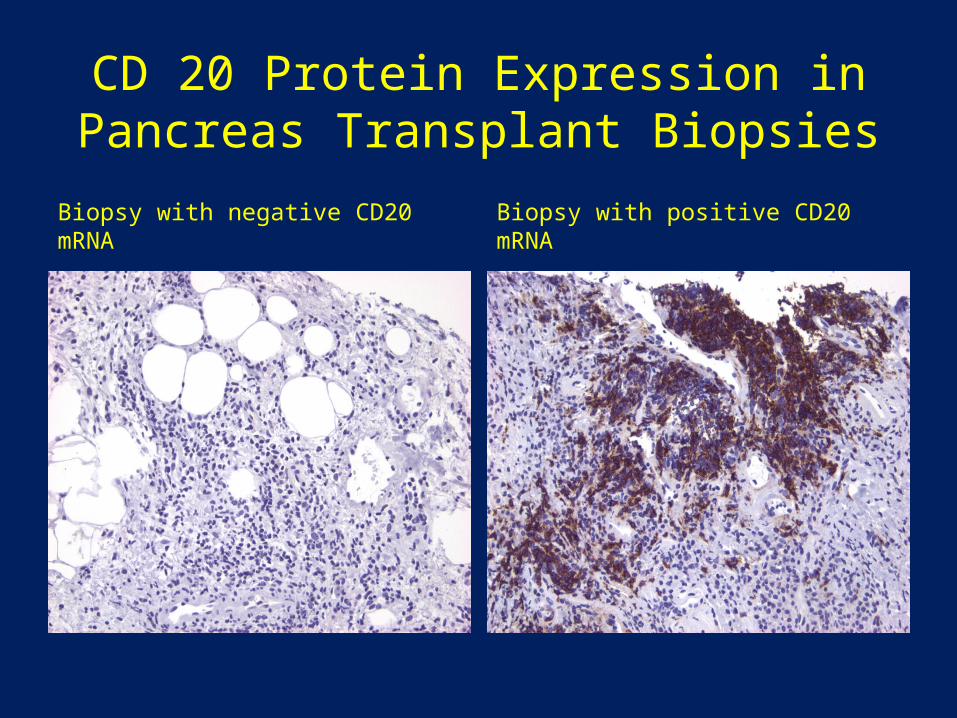
CD 20 Protein Expression in Pancreas Transplant Biopsies
Biopsy with negative CD20 mRNA Biopsy with positive CD20 mRNA

Expression of Some of Selected Molecular Markers

Expression of Some of Selected Molecular Markers

Summary
• The first study looking into molecular expression in transplant
pancreas specimen;
• Technique feasibility of obtaining RNA of good quality using
paraffin preserved pancreas biopsy specimen;
• Existence of variable up- and down-regulation of molecular
markers;
• Corresponding expression of protein in the biopsy specimens;
• Apparent correlation of expression pattern with observed
clinical outcome;

Future Direction and Potential Implication
• Need for a validation study involving large sample size;
• Need for definition of additional molecular markers;
• Need for more detailed correlation between expression
patterns and transplant outcome;
• Finally, prospective molecular study of pancreas allograft
using protocol biopsy;
• Potential guidance for target therapeutic intervention based
on variable molecular expression in the tissue;

Acknowledgement
Laboratory
• Matthias Kretzler, M.D.
• Fabian Trillsch, M.D.*
• Anna Henger,*
• Felix Eichinger,
Pathology• Henry Appelman, M.D.• Joel Greenson, M.D.
Transplant• Silas Norman, M.D.
* Currently in Germany