gender mainstreaming in health collaboration plan
TRANSCRIPT

Gender Mainstreaming in Health
Collaboration Plan 2011-2013
4/28/2011
Sohodra Rampersaud Cathy Cuellar
Health Promotion Advisor Gender Mainstreaming Advisor for LAC PAHO/WHO Guyana PAHO/WHO
GUYANA

Guyana: Gender Mainstreaming Plan of Action
1/14
Introduction
The Pan-American Health Organization/World Health Organization’s (PAHO/WHO’s) Gender, Cultural Diversity and Human Rights
program (GDR) is promoting and supporting the development of collaboration plans to mainstream gender in health in various
countries, including Guyana. This exercise is projected to facilitate the technical cooperation with countries in relation to the
commitment to implement the PAHO Gender Equality Policy in health. This collaboration plan aims to integrate the cross-cutting
priorities (CCP) of the Organization in the Guyana (GUY) technical cooperation program.
The strategy to implement the PAHO Gender Equality Policy is to support the process to develop and evaluate the Biennial Work
Plan (BWP) and provide close technical support to priority countries in the region to achieve gender equality in health. In Guyana,
there are concrete initiatives to advance gender mainstreaming in health. Both the PAHO/WHO Country Cooperation Strategy (CCS)
2010-2015 for Guyana and the Ministry of Health’s (MOH’s) National Health Sector Strategy (NHSS) 2008-2012, have identified
mechanisms and objectives to give priority to gender equity in health. These reference documents are the framework for the
collaboration plan for Guyana.
About Guyana
Guyana, with a population of 751,223 and 214,970 sq. km land mass, extends along the north-eastern coast of South America and
shares borders with Venezuela, Brazil, and Suriname. It is the only English-speaking country in the South American continent, being
a former British territory, which gained independence in 1966. Guyana is thereby a part of the English-speaking Caribbean and a
member of the Caribbean Community (CARICOM). The country is a democratic republic functioning under a Westminster system of
government.

Guyana: Gender Mainstreaming Plan of Action
2/14
The economy is based on its abundant natural resources (bauxite, gold and diamonds, fertile and productive soil, water resources
caused by many rivers, and a continental shelf off the Atlantic coast). The traditional agricultural sector remains a significant
contributor to the country’s revenue, with the non-traditional sector rapidly climbing. Guyana is home to a vast rainforest and in
response to climate change and related issues the government formulated a Low Carbon Development Strategy (LCDS).
Settlement patterns have resulted in an interior and coastland for Guyana and the country is further divided into 10 administrative
regions. Georgetown, the capital, comprises 20.7% of the total population and lies below sea level, which makes it prone to flooding.
The local government structure consists of 10 Regional Democratic Councils, 65 Neighbourhood Democratic Councils, six
municipalities and 76 Amerindian Village Councils.
The country has a multi-racial population, with Indo-Guyanese representing 43.45 %, Afro-Guyanese 30.20% and Amerindians
9.16%. People of “mixed heritage’ represent 16.73 % of the population. There are nine Amerindian tribes; most Amerindians live in
the interior and largely maintain their culture. There are three main religions: Christianity, Islam, and Hinduism.
Situation Analysis
The difficult terrain of the interior sometimes makes access to key services difficult for persons living in the hinterland and the
indigenous population is believed to be among the poorest in the country, as measured by traditional income indicators. However,
they are entitled to tribal lands and engage in farming. Amerindians exhibit some of the lowest health indicators. About 60% of all
malaria cases occur in the interior among the Amerindian population, and Amerindian women are at higher risk of poor maternal
health outcomes due to issues with timely access to quality emergency obstetric care. Promotion of the right to the highest attainable
standard of health (the right to health), support for its progressive realization, with a human rights and gender-based approach to

Guyana: Gender Mainstreaming Plan of Action
3/14
developing, implementing, and assessing health policies, plans, and programs will be critical for reducing health inequities in
Guyana.
The 2007 Household Income and Expenditure Survey (HIES) found 13% of the population living in extreme poverty. A 2002
household survey showed that 22% of the general male working-age population is not engaged in any type of income-
generating activity, as opposed to 66% of females. Education is a legal requirement for children aged 5 years 9 months to
14 years and access to secondary education has increased from 54.5 % in 1991 to 65 percent in 20021.
The government has advanced programs with a strong focus on social and human development, as reflected in the National
Development Strategy (201-2010), the Poverty Reduction Strategy (2002-2005), and the LCDS (2009). Among the mechanisms in
place to address social justice and inequality are the Sexual Offences Act (2010), the Domestic Violence Act (1996), a National
Policy on Domestic Violence (2008-2013), a Unit to implement the policy, the Women’s Affairs Bureau, the Men’s Affairs Bureau,
Constitutional Commissions on Indigenous People, Rights of the Child, Ethnic Relations, and Women and Gender Equity. The
Constitutional Commission on Human Rights comprises the heads of those already mentioned.
In addition, Guyana is signatory to the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW), the
Convention on the Rights of the Child (CRC) the Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or
Punishment, the Abolition of Forced Labour Convention, United Nations Convention against Transnational Organized Crime Protocol
to Prevent, Suppress and Punish Trafficking in Persons, especially Women and Children, the Optional Protocol to the International
Covenant on Civil and Political Rights and the Millennium Development Goals (MDGs). Guyana has a growing political
representation of women, with at least one third of the National Assembly and Cabinet being women. However, the country has a
1 Millennium Development Goals Progress Report (2008)

Guyana: Gender Mainstreaming Plan of Action
4/14
large population of women who are single parents; many of these women have low-end jobs. The government has provided training
for the job market, but progress continues to be challenged by high rates of gender-based violence, including femicide and ineffective
or slow implementation of related policies and programs.
In the health sector, the public sector needs more incentives to deliver high quality, consumer-oriented services; while the shortage
of health care professionals, migration, inadequate integration of strategic health information through a comprehensive health
information system, and strategic use of the information, remain major challenges. Non-communicable diseases (NCDs) and their
risk factors constitute the main causes of death. Ischaemic heart disease was the leading cause of death in 2008, with
cerebrovascular diseases 2nd, neoplasms 3rd, diabetes 4th, and hypertension 5th. Diabetes is a major cause of morbidity as well as
mortality. In 2006, a Food Consumption Study showed that 53% of adults were overweight or obese, women more so than men.
Data from a CFNI Physical Activity Survey showed that 43.6% of the overall population consumed alcohol, males (73%) more than
females (28%). Anecdotally, alcohol use has been linked to domestic violence and suicide.
There appears to be increasing feminisation of HIV2, particularly between 2000 and 2008, when the annual number of new HIV
transmissions reported was consistently higher among young females, though this may be influenced by active screening among
pregnant women. The male: female sex ratio was 1.16 in 2000, 0.91 in 2008 and 1.05 in 2009. Even though the proportion of deaths
attributable to AIDS has been declining, from 9.5% in 2002 to 4.7 % in 2008, AIDS was the 6th leading cause of death in 2008 (more
so for men). Overall, only 20% of women aged 15-19 use any form of contraceptive, and contraceptive prevalence was lower among
women from the interior (29%) than in urban women (34%) and women from rural coastal areas (35%).
2 Guyana Country Cooperation Strategy 2010-2015

Guyana: Gender Mainstreaming Plan of Action
5/14
Maternal mortality remains a major public health priority in Guyana, though MOH data indicate that the maternal mortality ratio
(MMR) has been steadily decreasing (162.5/100,000 live births in 2005 to 120/100,000 lb in 2007 and 86.2/100,000 in 2008). Quality
of care issues have been identified as the main contributors to the MMR, including shortage of skilled professionals, inadequate
referral and communication systems, and geographic barriers3.
The health priorities outlined in the NNHSS and CCS include:
- Communicable and Non Communicable Diseases
- Maternal, Adolescent and Child Health
- Social Determinants of Health
- Health System Strengthening, including Health Information Systems
To contribute to addressing these priorities and the health situation in Guyana, the collaboration plan presents concrete strategies
and actions to incorporate a gender perspective in health, as follows:
Goal : To achieve gender equity in health in Guyana.
Purpose : To strengthen national capacity to identify and address gender inequities in health
Lines of action/objectives/activities : See matrix below.
Gender Equality Plan - Matrix
3 Situational Analysis extracted from PAHO/WHO Guyana Country Office BWP 2012-13 and Ministry of Health Statistical Bulletin 2008

Guyana: Gender Mainstreaming Plan of Action
6/14
Lines of
Action/Objectives
Activities Responsible
partners
Budget (US$)
1. Strengthen gender
responses in the health
sector
1.1 Support formation of technical working group on gender
at the Ministry of Health (to include membership from other
sectors).
1.2 Support operations of technical working group.
1.3 Present PAHO Gender Equality Policy and Plan.
1.4 Identify needs and support training on gender and
health in MoH.
1.5 Production of annual report on gender, cultural diversity
and human rights activities by the Ministry of Health
1.6 Adapt PAHO’s gender and health training manual for
Guyana, with an inter-cultural module.
GUY Country Office
(CO)
GDR
MoH
2,000 - GUY CO
10,000 - GDR
Subtotal $12,000
2. Improve health
sector’s response to
gender-based violence
2.1 Support the review/finalization of the gender-based
violence protocol for health workers.
2.2 Support the development of curriculum for health
workers on gender-based violence (to be used in nursing
schools etc).
2.3 Support training for health personnel on domestic
GDR
GUY CO
MOH
Ministry of Human
Services

Guyana: Gender Mainstreaming Plan of Action
7/14
Lines of
Action/Objectives
Activities Responsible
partners
Budget (US$)
violence, human rights, gender and cultural diversity.
2.4. Support the integration of gender-based violence
services in the health system at the national referral
hospital.
3,000 - SDE
6,000 - GDR
4,000 - MoH
Subtotal $13,000
3. Strengthen health
information system with
emphasis on
disaggregation of data
by sex and ethnicity
3.1 Carry out a gender analysis of NCDs in Guyana.
3.2 Conduct training on gender analysis for Ministries of
Health and Human Services and Bureau of Statistics.
3.3 Compile a brochure on gender, ethnicity and health
statistics.
3.4 Produce profile on gender and health for Guyana.
3.5 Explore TCC with Belize on gender-based violence
surveillance.
GUY CO
HSS
GUY Bureau of
Statistics
MOH
HSD/NC
GDR
SDE
2,000 - GUY CO
10,000 - GDR
4,000 – HSD/NC
30,000 - TCC
Subtotal $46,000
4. Strengthen
integration of gender
approach into National
HIV prevention plan
4.1 Incorporate gender into ART guidelines
4.2 Incorporate gender and human rights approach in
training with MARPs
4.3 Support data disaggregation in M&E surveillance for
TB, HIV & STI, and gender analysis of data
GUY CO
UNAIDS
MoH (NAPS)
2,000 - GUY CO
3,000 - UNAIDS
GUY

Guyana: Gender Mainstreaming Plan of Action
8/14
Lines of
Action/Objectives
Activities Responsible
partners
Budget (US$)
Subtotal $5,000
5. Undertake other
gender-related
collaboration
5.1 Improve analysis and use of information from surveys
(Global School Health Survey, Global School Personnel
Survey, Global Youth Tobacco Survey), and support
resulting initiatives.
5.2 Support UN collaboration on gender, human rights, and
ethnicity issues.
GUY CO
FCH
MoH
1,000 - GUY CO
1,000 - GDR
2,000 - FCH
Subtotal $4,000
Total US
$80,000
Guyana: Gender Mainstreaming Plan of Action
9/14
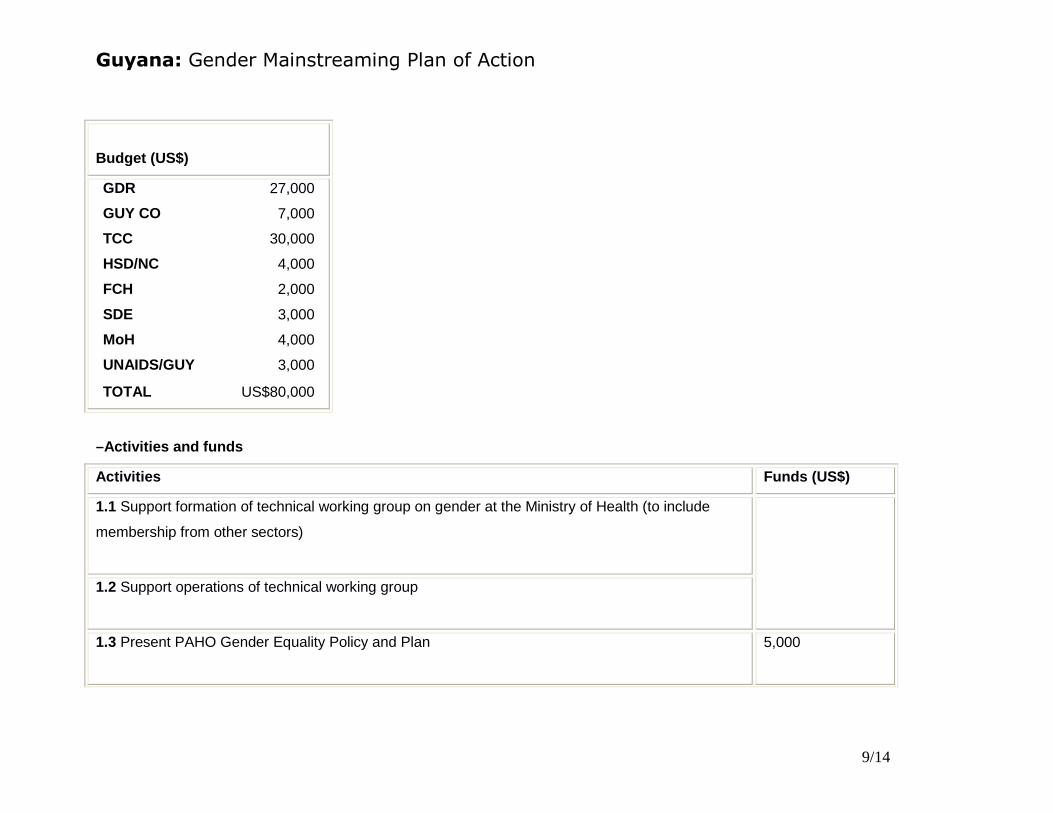
Budget (US$)
GDR 27,000
GUY CO 7,000
TCC 30,000
HSD/NC 4,000
FCH 2,000
SDE 3,000
MoH 4,000
UNAIDS/GUY 3,000
TOTAL US$80,000
–Activities and funds
Activities Funds (US$)
1.1 Support formation of technical working group on gender at the Ministry of Health (to include
membership from other sectors)
1.2 Support operations of technical working group
1.3 Present PAHO Gender Equality Policy and Plan
5,000

Guyana: Gender Mainstreaming Plan of Action
10/14
Activities Funds (US$)
1.4 Identify needs and support training on gender and health in MoH 5,000
1.5 Production of annual report on gender, cultural diversity and human rights activities by the
Ministry of Health
2,000
1.6 Adapt PAHO’s gender and health training manual for Guyana, with an inter-cultural module
2.1 Support the review/finalization of the gender-based violence protocol for health workers.
3,000
2.2 Support the development of curriculum for health workers on gender-based violence (to be used
in nursing schools etc).
3,000
2.3 Support training for health personnel on domestic violence, human rights, gender and cultural
diversity.
3,000

Guyana: Gender Mainstreaming Plan of Action
11/14
Activities Funds (US$)
2.4. Support the integration of gender-based violence services in the health system at the national
referral hospital.
4,000
3.1 Carry out a gender analysis of NCDs in Guyana.
8,000
3.2 Conduct training on gender analysis for Ministries of Health and Human Services and Bureau of
Statistics.
2,000
3.3 Compile a brochure on gender, ethnicity and health statistics.
2,000
3.4 Produce profile on gender and health for Guyana.
4,000
3.5 Explore TCC with Belize on gender-based violence surveillance. 30,000
4.1 Incorporate gender into ART guidelines
500

Guyana: Gender Mainstreaming Plan of Action
12/14
Activities Funds (US$)
4.2 Incorporate gender and human rights approach in training with MARPs
500
4.3 Support data disaggregation in M&E surveillance for TB, HIV & STI, and gender analysis of data 4000
5.1 Improve analysis and use of information from surveys (Global School Health Survey, Global
School Personnel Survey, Global Youth Tobacco Survey), and support resulting initiatives.
3,000
5.2 Support UN collaboration on gender, human rights, and ethnicity issues.
1,000
Total 80,000

Guyana: Gender Mainstreaming Plan of Action
13/14
Collaboration Strategy
The commitment of the PAHO/WHO GUY CO to contribute to the implementation of the Organization´s policy to mainstream gender
in health is evident through the past actions to build staff and national capacity on gender equality.
The strategies to achieve the objectives defined will be: close adherence to the guidelines for integrating CCPs into the BWP
process; sharing human and financial resources to accomplish activities; mobilization of regional cooperation where and when
needed, and collaboration with partners.