gender differences in smoking and risk for oral cancer · 2012-06-08 · icancerresearch56,...
TRANSCRIPT

1996;56:5192-5197.Cancer Res Joshua E. Muscat, John P. Richie, Jr., Seth Thompson, et al. Gender Differences in Smoking and Risk for Oral Cancer
Updated Version http://cancerres.aacrjournals.org/content/56/22/5192
Access the most recent version of this article at:
Citing Articles http://cancerres.aacrjournals.org/content/56/22/5192#related-urls
This article has been cited by 25 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
[email protected] atTo order reprints of this article or to subscribe to the journal, contact the AACR Publications
To request permission to re-use all or part of this article, contact the AACR Publications
American Association for Cancer Research Copyright © 1996 on June 8, 2012cancerres.aacrjournals.orgDownloaded from

ICANCER RESEARCH56, 5192-5197. November 15. 19961
ABSTRACT
Based on studies that show gender differences in cigarette smoking andlung cancer risk, we hypothesized that sex differences also exist in the riskfor cancer of the oral cavity and pharynx. A hospital-based study of 1009patients with oral neoplasla and 923 age-matched controls was conductedfrom 1981—1990.All subjects were interviewed directly with an extensivequestionnaire containing items on tobacco smoking, alcohol consumption,and occupational exposures. Using a cumulative lifetime measure of exposure to cigarette tar, the adjusted odds ratio for men, according to
increasing quartile of tar consumption and relative to never smokers, was1.0 195% confidence interval (CI), 0.6—1.6)for the lowest category, 0.9(95% CI, 0.6—1.6)for the second category, 1.6 (95% CI, 1.0—2.5)for the
third category, and 2.1 (95% CI, 1.4—3.2)for the highest category. Amongwomen, the corresponding odds ratios were 1.8 (95% CI, 1.1—3.0),2.8(95% CI, 1.6—4.9), 3.2 (95% CI, 1.9—5.6),and 4.6 (95% CI, 2.5—8.7).The
linear increase in risk was significantly higher for women than for men.Among nonsmoking cases, there was a significantly higher proportion ofwomen than men over the age of 50 years. This was consistent for allsubsites within the oral cavity. These findings support the hypothesis thatthere are gender differences in the smokiag-related risks for oral cancerand in the risk for nonsmoking-related oral cancer as well. The role ofnutrition in relation to these findings is discussed.
INTRODUCTION
Cigarette smoking is the predominant cause of cancer of the lung,oral cavity, and pharynx. The risk of lung cancer is higher in womenthan in men per cumulative dose ofcigarette smoking (1—8),and thereis limited evidence that women have a higher susceptibility to tobaccosmoke carcinogens than men (9, 10). These observations, and aprevious analysis of risk factors for oral cancer by our group showinghigher ORs3 for current smokers in women than in men (1 1), led usto hypothesize that female smokers are also at higher risk for oralcancer than male smokers. In the current paper, we examine theassociation of smoking by gender on the development of oral cancer.Because alcohol consumption is a cofactor in oral carcinogenesis (12,13), the risk estimates were adjusted for levels of alcohol intake.Subjects (men) who smoked pipes or cigars were excluded from theanalysis. In addition, we examine the epidemiology of oral cancers innonsmokers.
MATERIALS AND METHODS
A hospital-basedstudy of oral cancer was conducted between 1981 and1990 (see “Acknowledgments―).Case patients were men and women betweenthe ages of 21 and 80 years with newly diagnosed histologically confirmedcancer of the oral cavity and pharynx (lCD, 9th Revision, codes 141, 143—146,148, and 149). Patients with cancer of the salivary gland (lCD 142) andnasopharynx (lCD 147) were excluded. Controls were hospital patients admitted for conditions unrelated to tobacco use. Controls were matched to cases by
Received 5/31/96; accepted 9/19/96.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
I Supported By NIH Grants DE-09514, CA-68384, CA-32617, and CA-17613.
2 To whom requests for reprints should be addressed, at Division of Epidemiology,
American Health Foundation, 320 East 43rd Street, New York, NY 10017.3 The abbreviations used are: OR, odds ratio; CI, confidence interval; lCD, Interna
tional Classification of Diseases.
sex, age (±five years), race, and date of admission (±three months). Eligiblepatients were identified from daily hospital admission logs. Ninety-one percentof cases and 97% of controls who were approached agreed to be interviewedby a trained interviewer and signed consent forms. Within each hospital, cases
and controls were interviewed by the same interviewer.The most detailed section of the questionnaire contained data on lifetime
smoking history. Subjects were asked to provide information for each brand of
cigarette smoked, the age they started smoking, and the duration and frequencyof smoking. Never smokers were those who never smoked cigarettes regularly.Current smokers were defined as subjects who had smoked at least one
cigarette/day during the past year. Ex-smokers were quitters who had notsmoked within the past year. The tar content of the brand of cigarette wasobtained from the 1977 and 1988 Federal Trade Commission reports (14). Acumulative tar yield measure was obtained by the following formula:
T=@(t1XDXC1)X 106
where t = tar content in milligrams, D days of smoking, andC = number of cigarettes smoked (3). The cumulative tar yield wasdivided into quartiles based on the distribution of smokers in the entirecontrol group (e.g., men and women combined), and subjects werecompared to never smokers when calculating ORs. Likewise, a packyear measure was calculated by multiplying the years of smoking bythe number of packs smoked/day for each brand of cigarette. Detailedquestions were asked on current alcohol consumption including beer,wine, and hard liquor. Alcohol consumption was divided into severalcategories. Nondrinkers were classified as subjects who never consumed alcohol or drank less than one drink/week. Occasional drinkersinclude subjects who drank > I drink/week and <1 drink/day. Subjects were asked to give a detailed employment history including jobtitle and type of occupation. For each job, subjects were askedwhether they had been exposed to one or more of 45 occupationalexposures including hydrocarbon emissions and fumes, solvents, metals, chemicals, dyes, dusts, and fibers for at least 8 h/week for oneyear or more.
Gender specific ORs and 95% CIs for tar quartiles were calculated.Unconditional multiple logistic regression analysis was performed toobtain maximum likelihood estimates of ORs, adjusted for the continuous covariates age (five ordinal levels) and education (four ordinallevels). Additional terms for religion, marital status, race, and bodymass index were tested by the likelihood ratio statistic. In models thatevaluated trends and interactions, T was treated as continuous byassigning the median cumulative tar yield value for each of the fourcategories. The confounding or interaction effects of alcohol consumption were also modeled as a continuous variable by assigningmedian values to each category of consumption. To determinewhether the effects of smoking were significantly greater for womenthan for men, a model that combined all subjects was evaluated, andan interaction term for gender and tar was tested. The fit of the finalmodels was evaluated by plotting the changes in the Pearson fagainst the estimated logistical probabilities (15).
RESULTS
Partial or complete information on brands of cigarettes smoked wasmissing for 56 cases and 60 controls. This left a final sample of 1009cases (687 men and 322 women) and 923 controls (619 men and 304women). The subsite distribution among cases was similar for men
5192
Gender Differences in Smoking and Risk for Oral Cancer'
Joshua E. Muscat,2 John P. Richie, Jr., Seth Thompson, and Ernst L. Wynder
Divisions ofEpidemiology (J. E. M., S. T., E. L. W.j and Nutritional Carcinogenesis If. P. RI, American Health Foundation. New York, New York 10017
American Association for Cancer Research Copyright © 1996 on June 8, 2012cancerres.aacrjournals.orgDownloaded from
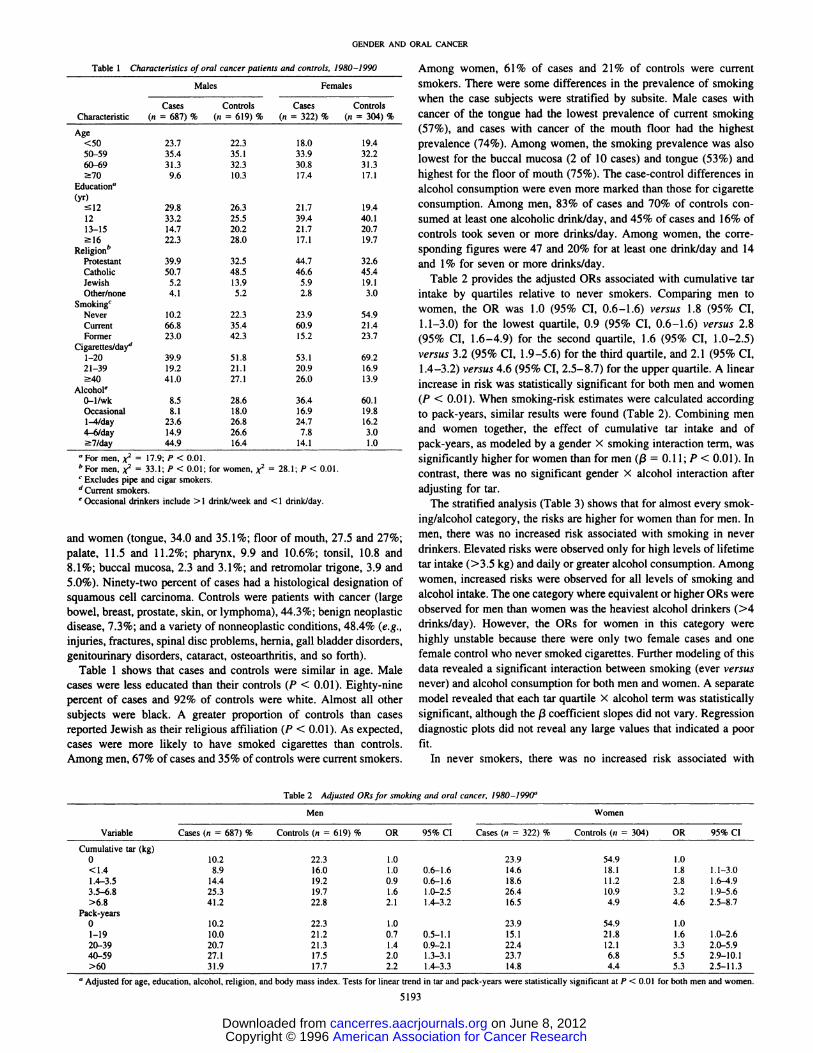
Table1 Characteristicsof oral cancer parients and controls, 1980 —1990MalesFemalesCases
ControlsCasesControlsCharacteristic(n= 687) % (n = 619) %(n 322) % (n 304)%Age<5023.7
22.318.019.450—5935.435.133.932.260—6931.332.330.831.37o9.610.317.417.1Education'@(yr)l229.8
26.321.719.41233.225.539.440.113—1514.720.221.720.7l622.328.017.119.7Religion―Protestant39.9
32.544.732.6Catholic50.748.546.645.4Jewish5.213.95.919.1Other/none4.15.22.83.0SmokingcNever10.2
22.323.954.9Current66.835.460.921.4Former23.042.315.223.7Cigarettes/cla@1—2039.9
51.853.169.221—3919.221.120.916.94041.027.126.013.9Alcohole0—l/wk8.5
28.636.460.1Occasional8.118.016.919.81—4/thy23.626.824.716.24—6/day14.926.67.83.07/day44.916.414.1 1.0
Table 2 Adjusted ORsfor smokingand oralcancer,1980—1990―MenWomenCases
(n = 687) % Controls (n = 619) %OR95% CICases (n = 322) %Controls (n 304) OR 95% CI
GENDER AND ORAL CANCER
Among women, 61 % of cases and 21 % of controls were currentsmokers. There were some differences in the prevalence of smokingwhen the case subjects were stratified by subsite. Male cases withcancer of the tongue had the lowest prevalence of current smoking(57%), and cases with cancer of the mouth floor had the highestprevalence (74%). Among women, the smoking prevalence was alsolowest for the buccal mucosa (2 of 10 cases) and tongue (53%) andhighest for the floor of mouth (75%). The case-control differences inalcohol consumption were even more marked than those for cigaretteconsumption. Among men, 83% of cases and 70% of controls consumed at least one alcoholic drink/day, and 45% of cases and 16% ofcontrols took seven or more drinks/day. Among women, the corresponding figures were 47 and 20% for at least one drink/day and 14and 1% for seven or more drinks/day.
Table 2 provides the adjusted ORs associated with cumulative tarintake by quartiles relative to never smokers. Comparing men towomen, the OR was 1.0 (95% CI, 0.6—1.6) versus 1.8 (95% CI,1.1—3.0)for the lowest quartile, 0.9 (95% CI, 0.6—1.6) versus 2.8(95% CI, 1.6—4.9) for the second quartile, 1.6 (95% CI, 1.0—2.5)versus 3.2 (95% CI, 1.9—5.6)for the third quartile, and 2. 1 (95% CI,1.4—3.2)versus 4.6 (95% CI, 2.5—8.7)for the upper quartile. A linearincrease in risk was statistically significant for both men and women(P < 0.01). When smoking-risk estimates were calculated accordingto pack-years, similar results were found (Table 2). Combining menand women together, the effect of cumulative tar intake and ofpack-years, as modeled by a gender X smoking interaction term, wassignificantly higher for women than for men ((3 = 0.1 1; P < 0.01). Incontrast, there was no significant gender X alcohol interaction afteradjusting for tar.
The stratified analysis (Table 3) shows that for almost every smoking/alcohol category, the risks are higher for women than for men. Inmen, there was no increased risk associated with smoking in neverdrinkers. Elevated risks were observed only for high levels of lifetimetar intake (>3.5 kg) and daily or greater alcohol consumption. Among
women, increased risks were observed for all levels of smoking andalcohol intake. The one category where equivalent or higher ORs wereobserved for men than women was the heaviest alcohol drinkers (>4drinks/day). However, the ORs for women in this category werehighly unstable because there were only two female cases and onefemale control who never smoked cigarettes. Further modeling of thisdata revealed a significant interaction between smoking (ever versusnever) and alcohol consumption for both men and women. A separatemodel revealed that each tar quartile X alcohol term was statisticallysignificant, although the (3coefficient slopes did not vary. Regressiondiagnostic plots did not reveal any large values that indicated a poorfit.
In never smokers, there was no increased risk associated with
‘,For men, X2 17.9; P < 0.01.
b For men, @2= 33.1; P < 0.01; for women,@ = 28.1; P < 0.01.
C Excludes pipe and cigar smokers.
d Current smokers.
e Occasional drinkers include >1 drink/week and < 1 drink/day.
and women (tongue, 34.0 and 35.1%; floor of mouth, 27.5 and 27%;palate, 11.5 and 11.2%; pharynx, 9.9 and 10.6%; tonsil, 10.8 and8.1%;buccalmucosa,2.3and3.1%;andretromolartrigone,3.9and5.0%). Ninety-two percent of cases had a histological designation ofsquamous cell carcinoma. Controls were patients with cancer (largebowel, breast, prostate, skin, or lymphoma), 44.3%; benign neoplasticdisease, 7.3%; and a variety of nonneoplastic conditions, 48.4% (e.g.,injuries, fractures, spinal disc problems, hernia, gall bladder disorders,gemtounnary disorders, cataract, osteoarthritis, and so forth).
Table 1 shows that cases and controls were similar in age. Malecases were less educated than their controls (P < 0.01). Eighty-ninepercent of cases and 92% of controls were white. Almost all othersubjects were black. A greater proportion of controls than casesreported Jewish as their religious affiliation (P < 0.01). As expected,cases were more likely to have smoked cigarettes than controls.Among men, 67% of cases and 35% of controls were current smokers.
10.222.31.023.954.91.08.916.01.00.6—1.614.618.11.81.1—3.014.419.20.90.6—1.618.611.22.81.6—4.925.319.71.61.0—2.526.410.93.21.9—5.641.222.82.11.4—3.216.54.94.62.5—8.7
Variable
Cumulative tar (kg)0<1.41.4—3.53.5—6.8>6.8
Pack-years0 10.2 22.3 1.0 23.9 54.9 1.01—19 10.0 21.2 0.7 0.5—1.1 15.1 21.8 1.6 1.0—2.620—39 20.7 21.3 1.4 0.9—2.1 22.4 12.1 3.3 2.0—5.940—59 27.1 17.5 2.0 1.3—3.1 23.7 6.8 5.5 2.9—10.1>60 31.9 17.7 2.2 1.4—3.3 14.8 4.4 5.3 2.5—11.3
a Adjusted for age, education, alcohol, religion, and body mass index. Tests for linear trend in tar and pack-years were statistically significant at P < 0.01 for both men and women.
5193
American Association for Cancer Research Copyright © 1996 on June 8, 2012cancerres.aacrjournals.orgDownloaded from

A.MenCumulative
TarAlcohol0—<l/wkOccasional―1-4/day>4/day<1.40.7
0.3—1.8(8, 29)0.9
0.3—2.3(10, 21)1.0
0.4—2.1(21, 34)2.1
0.7—5.9(14,7)1.4—3.50.30.1—1.1
(4, 29)0.50.2—1.5 (6, 24)1.50.7—3.2 (27, 29)2.71.1—6.6
(49,21)3.5—6.81.0 0.5—2.6(12, 19)1
.2 0.4—3.7(10, 18)1
.8 0.8—3.8(34, 31)4.7
2.0—11.3(88,25)>6.81.00.4—2.8
(8, 7)1.60.6—4.7 (13, 19)2.51.1—5.2
(57, 40)6.12.6—14.4
(145,36)B.WomenAlcohol0—<
1/weekOccasional―1-4/day>4/day―<1.41.2
0.6—2.4(17,29)1.4
0.5—4.3(10,15)5.9
1.7—20.5(13,8)1.0
0.01—27.9(6,3)1.4—3.53.0
1.3—7.0(16,11)1.2
0.4—3.6(8,14)9.5
2.8—32.0(19,7)4.3
0.1—116.9(17,2)3.5—6.82.0
1.0—4.0(19, 20)5.8
1.7—20.3(15, 5)14.0
4.1—48.5(24, 6)6.5
0.1—174.2(26,2)>6.82.4
0.8—6.9(8, 7)16.7
1.8—152.6(9, 1)18.6
4.0—86.8(16, 3)2.40.0-55.1 (19,4)
Table4 Agedistributionin nonsmokingcasesandcontrols―NS
casesMen
WomenSite―
<50 yr 50 yr <50 yr 50yrTongue
18 (56.3%) 14 (43.7%) 14 (40.0%) 21(60.0%)Floor6 (42.9%) 8 (57.1%) 3 (17.7%)14(82.4%)Palate5 (45.5%) 6 (54.5%) 3 (25.0%) 9(75.0%)Tonsil2 (22.2%) 7 (77.8%) 0 (0.0%) 5(100.0%)Other3 (75.0%) 1 (25.0%) 2 (25.0%) 6(75.0%)TOtal'
34 (48.6%) 36 (5 1.4%) 22 (28.6%) 55(71.4%)NS
controls 29.0% 7 1.0% 18.6%81.4%a
NS, neversmokers.b
Percentages are rowpercentages.Differences
in age between men and women; P < 0.05.
GENDER AND ORAL CANCER
Table 3 ORs of smoking and oral cancer by levels of alcohol consumptionReference category is never smokers. All ORs adjusted for age and education. Numbers in parentheses are numbers of cases and controls.
a Greater than or equal to 1/week and less than 1/day.
b Crude ORs and exact confidence limits. Only two female cases and one female control were never smokers in this category.
drinking. The adjusted OR for men, relative to never drinkers, was 1.2(95%CI, 0.6—1.2)for occasionaldrinkers,1.4(95%CI, 0.7—3.1)for1—4drinks/day, and 1.6 (95% CI, 0.6—4.2) for >4 drinks/day. Inwomen, the corresponding ORs were 0.9 (95% CI, 0.4—2.1),0.6(95%CI, 0.2—1.4),and 4.6 (95% CI, 0.4—52.2).
Oral snuff use and chewing tobacco were unrelated to oral cancerrisk. Among men, 9 cases (1.3%) and 10 controls (1.6%) reportedusing snuff at least once a week for one or more years. Amongwomen, only two cases and one control reported snuff use. Thirtyeight cases (5.5%) and 33 controls (5.3%) reported using chewingtobacco at least once a week for at least one year. Among the tobaccochewers, there were no case-control differences in the frequency ofchewing. None of the women reported using chewing tobacco regularly.
Among cases, the percentage of nonsmokers was greater in womenthan in men (24 versus 10%). Table 4 shows the age distribution in thenonsmoking cases. There were relatively more women than men overthe age of 50 (71 versus 51%; P < 0.05). The employment history ofall nonsmoking cases and controls was examined to determine possible gender differences in chemical, environmental, or other exposures.No pattern of risk was evident with any single occupation, categoriesof similar occupations (e.g. , construction workers), or any specificoccupational exposures.
5194
DISCUSSION
Few reports have had gender-specific risk estimates for smokingand oral cancer. A recalculation of case-control data published in 1957by Wynder et a!. (16) yields a higher crude OR for women than men(8.1 versus 4.6) associated with 21 cigarettes/day. In contrast,slightly higher smoking-related risks were reported for men thanwomen in Puerto Rico in 1969 (17) and in a hospital-based study in1977 (18). These early studies were conducted when men smokedcigarettes with much higher tar content than women, and findingswere unadjusted for the higher tar intake and alcohol consumption inmen. More recently, in a population-based study of 1114 oral cancercases conducted by Blot et a!. (19), the alcohol-adjusted ORs forwomen and men were I .0 versus 0.8 for 1—19pack-years, 2.9 versus1.9 for 20—39pack-years, and 5.0 versus 1.8 for 40+ pack-years. Ina pooled analysis of three large case-control studies of oral cancer,Macfarlane et a!. (20) reported that the smoking OR in nondrinkers,among men, was 1.1 for 1—33pack-years and 1.3 for >33 pack-years.In women, the OR in nondrinkers was 2.6 (P < 0.05) for 1—18pack-years and 4.6 for >18 pack-years (P < 0.05). Using part of thedata from the current study, Kabat et a!. (11) found higher ORs forwomen than men among current (4.3 versus 3.3) and former smokers(1.4versus1.1).Thecurrentfindingsshowasignificantlyhighertrendin the ORs for women than men for both the cumulative tar measureand the pack-year measure after adjustment for alcohol and otherconfounding variables. Our data and those described by Blot et a!.(19) both show that 40 pack-years of smoking approximately increases the risk of oral cancer 2-fold in men and 5-fold in womenrelative to nonsmokers.
The prevalence of smoking was highest for subjects with cancer ofthe mouth floor and lowest for cancer of the tongue in both men andwomen. These findings are consistent with the results from earliercase-control studies (16). The percentage of mouth cancers that werelocated in the tongue and mouth floor was equal for men and women.
No significant interaction between gender and alcohol consumptionwas found after adjustment for smoking, although these findingsshould be interpreted with caution because the heaviest drinkers werepredominantly men and because of possible misclassification. In a
American Association for Cancer Research Copyright © 1996 on June 8, 2012cancerres.aacrjournals.orgDownloaded from

Table 5 Types of cigarette smoked among ever-smoking cases andcontrols―MalesFemalesCasesControlsORCasesControlsORFilter
SW 20+―SW 1—19'Nonfilter37.1
28.712.421.844.0
22.817.216.11.0
1.50.91.649.8
27.913.19.360.2
20.39.89.81.0
1.71.61.1
GENDER AND ORAL CANCER
a SW, switched from smoking nonfilter to filter.b Switched from smoking nonfilter to filter 20 years before diagnosis.
@ Switched from smoking nonfilter to filter 10 years before diagnosis.
case-control study of oral cavity cancer in Italy, Franceschi et a!. (21)observed similar alcohol-related risks for men and women. We didobserve a significant interaction between ever smoking and alcohol inboth men and women, although this effect did not vary by levels oflifetime tar consumption.
The main limitations of this study are its hospital-based nature andlack of information on nutritional factors. Possible biases that couldaccount for the current findings include a greater underreporting ofsmoking consumption in women than in men. However, Wagenknechtet a!. (22) found no gender differences in the misclassification rates(under 3% for white subjects) in a study of 3445 healthy reportednonsmokers when validated against serum cotinine. Previous studiesof the reproducibility of questions on smoking and hard liquor consumption in this data found very high intraclass correlation coefficients in men and in women (23). Still, the validity of reported alcoholconsumption in heavy drinkers may be problematic. Women may tendto underreport heavy alcohol consumption as social drinking, althoughthis may occur among men as well. Some studies have demonstratedthe unreliability of self-reported alcohol consumption among problemdrinkers (24). Because relatively few women drink heavily, misclassification of heavy drinkers as moderate drinkers would result in aslightly spurious effect associated with moderate levels of alcoholconsumption but would result in a substantial underestimation of riskin the heavy alcohol consumption category.
When interpreting gender-specific risks in case-control data, it isnecessary to consider the absolute rates of cancer in nonsmokers.In a pooled analysis, Risch et a!. (25) calculated that the female:male ratio of age-adjusted lung cancer rates was 0.7. This difference, which may reflect a greater exposure to occupational carcinogens (26, 27), does not account for the 2—3-foldhigher relativerisks of lung cancer among female smokers than male nonsmokers(25). However, there is little population-based data of oral cancerrates in nonsmokers. In a 1960 study of one million men andwomen, Hammond (28) calculated a oropharyngeal mortality rateof 7 per 100,000 in nonsmoking men ages 65—79.This was basedon five deaths after three years of follow-up. The rate for womenin this age group was also seven, although this number includedlarynx and esophagus deaths as well. Some data indirectly suggestthat men do not have a higher baseline risk of oral cancer thanwomen. For example, several studies have found little evidence foroccupational oral carcinogens (29—36). Occupation and occupational exposures were unrelated to oral cancer risk in this study.The use of oral snuff may be associated with increased rates of oralcancer in men (37), although combined data from the MortalityFollowback Survey and National Health Interview Survey show noincreased risk of oral cancer from any form of smokeless tobacco.There has been an increase in the incidence of snuff use amongyoung men (38) and an increase in the incidence of tongue cancersin men under age 40 since the 1950s in the United States (39, 40)and Scotland (41). In our data, snuff use was unrelated to oralcancer risk. This did not seem to reflect the low prevalence of snuffuse in controls (1 .6%). There was 80% statistical power to detect
an OR of 2.8 given this level of exposure in controls. Among thenonsmoking cases, there was a slightly higher percentage of men
than women under the age of 40 (26% versus 18%), although thisdifference was not statistically significant. If the age differencesbetween nonsmoking male and female cases do reflect a malespecific risk factor besides snuff, it would not seem to account for
the differences in smoking-related risks between men and womenin this study.
Possible biological explanations for the higher risks of oralcancer in women than in men include nutritional deficiencies.
There was a higher proportion of nonsmoking female cases thannonsmoking male cases (24% versus 10%). In nonsmoking casesover age 50, there was a significantly greater percentage of womenthan men (Table 4). Ahlbom was among the first investigators torelate the occurrence of Plummer-Vinson syndrome in Sweden(42), a precancerous condition resulting from chronic iron deficiency and associated anemia during the menstrual years, to an
increased risk of oral and other cancers in almost exclusively olderwomen. Riboflavin deficiency is also characteristic of PlummerVinson disease. In a study of 810 mostly nonsmoking patients witha variety of alimentary tract cancers in Sweden, Wynder et a!. (43)found a higher percentage of women with oral cancer in older agegroups than men with oral cancer and a significant association with
Plummer-Vinson symptoms in these women. The similar findingswith respect to the higher prevalence of older women than men inthe current data could reflect a subclinical condition, similar toPlummer-Vinson syndrome, associated with iron depletion and lowintake of vitamins and minerals. Iron and riboflavin deficiency inmice leads to cell atrophy in upper alimentary tract epithelium,
conditions similar to patients with Plummer-Vinson disease (44—
46). Subsequent hyperplasia has been observed with riboflavindeficiency (42). Rats fed diets deficient in zinc also have similar
morphological changes in the buccal mucosa (47).
Populations that consume low amounts of fruits experienceelevated rates of oral cancer. Decreased blood nutrients of vitaminsA and B2 and /3-carotene have been detected in patients with oralcancer (48). Similarly, vitamin A-deficient animals are moresusceptible to tobacco smoke polycyclic aromatic hydrocarbons(49). Nutritional deficiencies associated with oral cancer may alsoarise indirectly through excessive alcohol consumption because alarge percentage of daily caloric intake in alcoholics comes fromalcohol (50). Intake of fruits and vegetables is likely to be low inpersons with excessive alcohol consumption. Alcohol consumptioncan also directly inhibit the absorption of nutrients and vitamins(51).
The effects of a higher absolute risk of oral cancer in nonsmokingolder women resulting from menstrual-associated nutritional deficiencies during the reproductive years would result in an underestimate of
the smoking effects in women by increasing the numbers of nonsmoking female cases relative to nonsmoking male cases. However, although nutritional deficiencies may be a risk factor for oral cancer, theetiology of nonsmoking-related oral tumors remains largely unknown.
5195
American Association for Cancer Research Copyright © 1996 on June 8, 2012cancerres.aacrjournals.orgDownloaded from

GENDER AND ORAL CANCER
Only beer consumption in men and low body weight in women havealso been identified as possible causes (52). It has been hypothesizedthat human papilloma virus may cause oral cancer in nonsmokers (53,54).We did not find anydifferencesin educationallevelsbetweenpostmenopausal nonsmoking cases and controls. There may be otherunidentified risk factors that are gender-specific and thus could have
confounded our results.Another possible interpretation of this data is that there is a
greater exposure to tobacco juice among female smokers than malesmokers. Filter cigarettes reduce the contact with tobacco juicerelative to nonfilter cigarettes and reduce the risk for oral cancer.In the previous report by Kabat et a!. (1 1), the independent effectsof filter use compared to nonfilter use on the risk of oral cancerwere similar for men and women. Table 5 shows that few womenhave smoked nonfilter cigarettes exclusively, whereas more menhave smoked nonfilter cigarettes exclusively. Thus, the currentfindings are unlikely to be due to a greater oral contact withtobacco juice among women.
Estrogens may be involved in the promotion of oral cancer. Usingthe Surveillance, Epidemiology, and End Results (SEER) Programdata, Begg et a!. (55) found that women also had a higher risk thanmen of developing second primaries of the head and neck, as well aslung, esophagus, urinary bladder, and kidney cancers.
We noted that the higher proportion of postmenopausal cases,compared to male cases over age 50, was reported as early as 1957(16) and have suggested that possible risk factors more specific towomen include iron, vitamin, and mineral deficiency. In addition,glutathione, an active antioxidant, is found to be depleted in theelderly (56) and associated with age-related morbidity (57). Lowblood glutathione levels and low dietary glutathione intake mayalso play a role in oral cancer risk (58). Further investigationsshould consider the effects of age in nonsmokers by subsite.Cancer of the tonsil in nonsmokers occurs almost exclusively inolder individuals, and this may provide further clues to the originsof mouth cancer.
ACKNOWLEDGMENTS
We thank Dr. Edith Zang for statistical assistance and comments. We aregrateful to the following collaborators: Dr. Edward S. Garrity, Jr. (LoyolaUniversity Hospital, Chicago, IL); Dr. John Sharp (Hines Veterans Hospital,Hines, IL); Dr. Christine Johnson (Henry Ford Hospital, Detroit, MI); Dr.Kanti R. Rai (Long Island Jewish Hillside Medical Center, New Hyde Park,
NY); Drs. Elliot Strong and Stimson Schantz (Memorial Sloan-KetteringCancer Center, New York, NY); Dr. Linga Raju (Nassau County Medical
Center, East Meadow, NY); Dr. James Colberg (Thomas Jefferson UniversityHospital, Philadelphia, PA); and Dr. Paul Stolley (Hospital ofthe University of
Pennsylvania, Philadelphia, PA).
REFERENCES
1. McDuffie, H. H., Klassen, D. J., and Dosman, J. A. Female-male differences inpatients with primary lung cancer. Cancer (Phila.), 59: 1825—1830,1987.
2. McDuffle,H. H., Klassen,D. 3.,andDosman,J.A. Men,women,andprimarylungcancer: a Saskatchewan personal interview study. J. Clin. Epidemiol., 44: 537—544,1991.
3. Zang, E. A., and Wynder, E. L. Cumulative tar exposure. A new index for estimatinglung cancer risk among cigarette smokers. Cancer (Phila.), 70: 69—76,1992.
4. Brownson,R.C.,Chang,J. C.,andDavis,J. R.Genderandhistologic-typevariationsin smoking-related risk of lung cancer. Epidemiology, 3: 61—64,1992.
5. Risch, H. A., Howe, 0. R., Jam, M., Burch, D. J., Holoway, E. J., and Miller, A. B.Are female smokers at higher risk for lung cancer than male smokers? A case-controlanalysis by histologic type. Am. J. Epidemiol., 138: 281—293,1993.
6. Osann,K.E.,Anton-Culver,H.,Kurosaki,T.,andTaylor,T. Sexdifferencesin lungcancer risk associated with cigarette smoking. Int. J. Cancer, 54: 44—48, 1993.
7. Dwyer, T., Blizzard, L., Shug, D., Hill, D., and Ansari, M. Z. Higher lung cancer ratesin young women than young men: Tasmania. 1983 to 1992. Cancer Causes & Control,5: 351—358, 1994.
8. Zang, E. A., and Wynder, E. L. Differences in lung cancer risk between men and
women:examinationof theevidence.J. Natl.CancerInst.,88: 183—192,1996.9. Ryberg, D., Hewer, A., Phillips, D. H., and Haugen. A. Different susceptibility to
smoking-induced DNA damage among male and female lung cancer patients. CancerRes., 44: 833—839,1989.
10. Muscat,J., Carmella,S., Scott,D.,Hecht,S. S., Richie,J. P.,Jr. Genderdifferencesin the metabolism of the tobacco-specific nitrosamine 4-(methylnitrosamino)-l-(3-pyridyl)-1-butanone (NNK). Proc. Am. Assoc. Cancer Res., 37: 253, 1996.
11. Kabat, G. C., Chang, C. J., and Wynder, E. L. The role of tobacco, alcohol use, and bodymass index in oral and phazyngealcancer. Its. J. Epidemiol.,23: 1137—1144, 1994.
12. Kato, I., and Nomura, A. M. Alcohol in the aetiology of upper aerodigestive tractcancer. Eur. J. Cancer, 30B (Oral Oncology): 165—178,1994.
13. IARC. Alcohol drinking. in: IARC Monographs on the Evaluation of CarcinogenicRisk to Humans, Vol. 44, pp. . Lyon, France: IARC, 1988.
14. Federal Trade Register, Part IV, Federal Trade Commission. “Tar,―nicotine, andcarbon monoxide content of domestic cigarettes. Washington, DC: U.S. GovernmentPrinting Office, 1977 and 1988.
15. Hosmer, D. W., and Lemeshow, S. L. Applied Logistic Regression. New York: JohnWiley & Sons, Inc., 1989.
16. Wynder,E. L.,Bross,I. J., andFeldman,R. M.A studyof theetiologicalfactorsincancer of the mouth. Cancer (Phila.), 10: 1300—1323, 1957.
17. Martinez, I. Factors associated with cancer of the esophagus. mouth, and pharynx inPuerto Rico. J. NatI. Cancer Inst., 42: 1069—1094, 1969.
18. Wynder, E. L., and Stellman, S. D. The comparative epidemiology of tobacco-relatedcancers. Cancer Res., 37: 4608—4622, 1977.
19. Blot, W. J., McLaughlin, J. K., Winn, D. M., Austin, D. F., Greenberg, R. S.,Preston-Martin, S., Bernstein, L., Schoenberg, J. B., Stemhagen, A., and Fraumen,J. F.Jr. Smokinganddrinkinginrelationto oralandpharyngealcancer.CancerRet.,48: 3282—3287,1988.
20. Macfarlane, G. J., Zheng, T., Marshall, J. R., Boffeua, P., Niu, S., Brasure, J.,Merletti, F., and Boyle, P. Alcohol, tobacco, diet, and the risk of oral cancer: a pooledanalysis of three case-control studies. Eur. J. Cancer, 31B: 181—187,1995.
21. Franceschi, S., Bidoli, E., Negri, E., Barbone, F., and La Vecchia, C. Alcohol andcancers of the upper aerodigestive tract in men and women. Cancer Epidemiol.,Biomarkers & Prey., 3: 299—304, 1994.
22. Wagenknecht, L. E., Burke, G. L., Perkins, L. L., Haley, N. J., and Friedman, G. D.Misclassification of smoking status in the CARDIA study: a comparison of self-reportwith serum cotinine levels. Am. J. Public Health, 82: 33—36,1992.
23. Morabia, A., Moore, M., and Wynder, E. L Reproducibility of food frequency measurements and inferences from a case-control study. Epidemiology, 1: 1305—1310,1990.
24. Babor, T., Stevens, R., and Marlatt, A. Verbal report methods in clinical research onalcoholism: response bias and minimization. J. Stud. Alcohol, 48: 410—424, 1987.
25. Risch, H. A., Howe, G. R., Jam, M., and Burch, J. D. Re: “Lungcancer risk for femalenonsmokers― (Letter). Science (Washington DC), 1206—1208, 1994.
26. Wilcox, A. J. Re: “Arefemale smokers at higher risk for lung cancer than malesmokers? A case-control analysis by histologic type―(Letter). Am. J. Epidemiol.,140: 186, 1994.
27. Hoover, D. R. Re: “Arefemale smokers at higher risk for lung cancer than malesmokers? A case-control analysis by histologic type―(Letter). Am. J. Epidemiol.,140:186—187,1994.
28. Hammond, E. C. Smoking in relation to the death rates of one million men andwomen. in: W. Haenszel(ed.), National Cancer Institute Monograph 19,pp. 127—204.Bethesda, MD: U.S. Department of Health, Education and Welfare, 1966.
29. Merletti, F., Boffetta, P., Ferro, G., Pisani, P., and Terracini, B. Occupation andcancer of the oral cavity or oropharynx in Turin, Italy. Scand. J. Work, Environ. &Health, 17: 248—254,1991.
30. Pukkala, E., Soderholm, A. L., and Lindqvist, C. Cancers of the lip and orophaiynx indifferentsocialand occupationalgroups in Finland.Eur. J. Cancer,30B (Oral Oncology):209—215,1994.
31. Huebner, W. W., Schoenberg, J. B., Kelsey, J. L., Wilcox, H. B., McLaughlin, J. K.,Greenberg, R. S., Preston-Martin, S., Austin, D. F., Stembagen, A., Blot, W. J., Winn,D. M., and Fraumeni, J. F., Jr. Oral and pharyngeal cancer and occupation: acase-control study. Epidemiology, 3: 300—309, 1992.
32. Blair, A., Stewart, P., O'Berg, M., Gaffey, W., Walrath, J., Bales, R., Kaplan, S., andCubit, D. Mortality among industrial workers exposed to formaldehyde. J. Nail.Cancer Inst., 76: 107 1—1084,1986.
33. Skov, T., Weiner, J., Pukkala, E., Malker, H., Andersen, A., and Lynge, E. Risk forcancer of the pharynx and oral cavity among male printers in the Nordic countries.Arch. Environ. Health, 48: 176—180,1993.
34. Maier, H., Dicta, A., Gewelke, U., and Heller, W. D. Occupational exposure tohazardous substances and risk of cancer in the area of the mouth cavity, oropharynx,hypopharynx, and larynx. A case-control study (in German). Laryngo-Rhino-Otologie, 70: 93—98,1991.
35. Whitaker, C. J., Moss, E., Lee, W. R., and Cunliffe, S. Oral and pharyngeal cancer inthe Northwest and West Yorkshire regions of England, and occupation. Br. J. Ind.Med., 36: 292—298,1979.
36. Liebling, T., Rosenman, K. D., Pastides, H., Griffith, R. G., and Lemeshow, S. Cancermortalityamong workersexposedto formaldehyde.Am. J. Ind. Med.,5: 423—428,1984.
37. Mattson, M. E., and Winn, D. M. Smokeless tobacco: association with increasedcancer risk. NCI Monographs, 8: 13—16,1989.
38. Tomar, S. C., Giovino, G. A., and Eriksen, M. P. Smokeless tobacco brand preferenceand brand switching among U.S. adolescents and young adults. Tobacco Control, 4:67—72,1995.
39. Davis, S., and Severson, R. K. Increasing incidence of cancer of the tongue in theUnited States among young adults. Lancet, 2: 910—911, 1987.
40. Depue, R. H. Re: “Risingmortality from cancers of the tongue in young white males―(Letter). N. Engl. J. Med., 315: 647, 1986.
5196
American Association for Cancer Research Copyright © 1996 on June 8, 2012cancerres.aacrjournals.orgDownloaded from

GENDER AND ORAL CANCER
41. Macfarlane, G. J., Boyle, P., and Scully, C. Rising mortality from cancer of the tonguein young Scottish males. Lancet, 2: 912, 1987.
42. Ahlbom, H. E. Pradisponierende Fakstoren fürPlattenepithelkarzinom in Mund, Halsund SpeiserOhre; eine statistche Untersuchung am Material des Radiumbemmets,Stockholm. Acta Radiol., 18: 163—185,1937.
43. Wynder, E. L., Hultberg, S., Jacobsson, F., and Bross, I. J. Environmental factors incancer of the upper alimentary tract. Cancer (Phila.), JO: 470—487, 1957.
44. Fairbanks, V. F. Nutrient deficiencies in man: iron. in: M. Recheigl, Jr. (ed), CRC
Handbook Series in Nutrition and Food, Vol. III, pp. 183—221. West Palm Beach, FL:CRC Press, 1978.
45. Furugouri, K. Effect of nutrient deficiencies in animals: iron. in: M. Reicheigl, Jr.(ed), CRC Handbook Series in Nutrition and Food, Vol. III, pp. 265—294.West PalmBeach, FL: CRC Press, 1978.
46. Wynder, E. L., and Klein, U. E. The possible role of riboflavin deficiency in epithelialneoplasia. I. Epithelial changes of mice in simple deficiency. Cancer (Phila.), 18:167—180,1965.
47. Gerson, S. J., and Meyer, J. Increased lactate dehydrogenase activity in buccalepithelium of zinc deficient rats. J. Nutr., 107: 724—729, 1977.
48. Richie, J. P., Jr. Role of nutrition in cancer of the oral cavity. J. AppI. Nutr., 43:49—57,1991.
49. Sporn, M. B., Dunlop, N. M., Newton, D. L., and Smith, J. M. Prevention of chemicalcarcinogenesis by vitamin A and its synthetic analogs (retinoids). Fed. Proc., 35:1332—1338,1976.
50. Leevy, C. M., Baker, H., tenHove, W., Frank. 0., and Chemck. G. R. B-complex
vitamins in liver disease of the alcoholic. Am. J. Clin. Nutr., 16: 339—346,1965.51. Vitale, J. J., and Coffey, J. Alcoholism and vitamin metabolism. in: B. Kissin and H.
Begleiter (edt.), The Biology of Alcoholism, Vol. 1, pp. 327—352,New York: PlenumPublishing Corp., 1971.
52. Ng, S. C., Karat, G. C., and Wander, E. L. Oral cavity cancer in non-users of tobacco.J. Nail. Cancer Inst., 85: 743—745,1993.
53. Maitland, N. J., Cox, M. F., Lynar. C., Prime, S. S., Meanwell, C. A., and Scully, C.Detection of human papilloma virus DNA in biopsies of human oral tissue. Br. J.Cancer, 56: 245—250,1987.
54. Maden, C., Beckmann, A. M., Thomas, D. B., Mcknight, B., Sherman, K. J., Ashley,R. L., Corey, L., and Daling, J. R. Human papilloma virus, herpes simplex viruses,and the risk of oral cancer in men. Am. J. Epidemiol., 135: 1093—1102, 1992.
55. Begg, C. B., Zhang, Z-F., Sun, M., Herr, H. W., and Schantz, S. P. Methodology forevaluating the incidence of second primary cancers with application to smokingrelated cancers from the Surveillance, Epidemiology, and End Results (SEER) Program. Am. J. Epidemiol., 142: 653—665, 1995.
56. Lang, C. A., Naryshkin, S., Schneider, D. L., Mills, B. J., and Lindeman, R. D. Lowblood glutathione levels in healthy aging adults. J. Lab. Clin. Med., 120: 720—725,1992.
57. Julius, M., Lang, C. A., Gleiberman, L., Harburg, E., DiFranceisco, W., and Schork,A. Glutathione and morbidity in a community-based sample of elderly. J. Clin.Epidemiol., 47: 1021—1026,1994.
58. Richie, J. P., Jr. The role of glutathione in aging and cancer. Exp. Gerontol., 27:615—626,1992.
S 197
American Association for Cancer Research Copyright © 1996 on June 8, 2012cancerres.aacrjournals.orgDownloaded from