gauging pressure ulcers - healthinsight home/pru - pru... · gauging pressure ulcers: ... multiple...
TRANSCRIPT

Gauging Pressure Ulcers A Nursing Homersquos Guide to Prevention and Treatment
Gauging Pressure Ulcers Introduction Pressure ulcers are a significant problem across all ages and health care settings Multiple factors put residents at risk for developing a pressure ulcer including immobility chronic illness incontinence poor nutrition altered level of consciousness altered sensory perception and a history of having pressure ulcers1
Pressure ulcers come at a high cost to everyone They result in pain suffering diminished quality of life and even death for some residents For a nursing home they represent extra staff hours and medical supplies spent caring for a preventable condition as well as more residents hospitalized The cost of treating a single full-thickness pressure ulcer can be as high as $70000 with the total treatment cost for pressure ulcers in the US surpassing $11 billion per year2
Although pressure ulcers are preventable more than one in every 10 of Missouri nursing home residents developed a pressure ulcer in 2007 The Centers for Medicare amp Medicaid Services has long focused on helping nursing homes prevent pressure ulcers but in 2008 they extended this effort across care settings Hospitals now have a payment incentive to partner with nursing homes on pressure ulcer prevention ndash a good thing since 20 percent of nursing home pressure ulcers originate outside the nursing home generally in the acute hospital setting
No matter where you are in your prevention efforts now is the time to take a look at your care processes with fresh eyes First review what the law says about pressure ulcers See this toolkitrsquos summary of the federal guidelines ndash Understanding CMS Interpretation of Tag F314 Then use the included Pressure Ulcer Facility Assessment Checklists to take a critical look at your current practices Every one of these systems is crucial to pressure ulcer prevention so take your time completing this assessment As you assess call on other staff to help you answer questions completely and honestly Once yoursquove completed the assessment and identified key areas for improvement review the clinical reference tools reminder tools and sample forms included in this toolkit Feel free to adapt them to meet your individual needs
1 Reddy M Gill SS Rochon PA Preventing pressure ulcers A systematic review JAMA 2006 296 974-984 2 Reddy M Gill SS Rochon PA Preventing pressure ulcers A systematic review JAMA 2006296974-984
Pressure Ulcers Table of Contents This table of contents provides an overview of the assessment and clinical reference tools for pressure ulcers contained in this document For further information see the following pages for tool descriptions organized by section If yoursquore viewing this document on your computer click on the tool name in the table of contents below and you will be taken directly to the resource To download and print tools individually go to wwwprimarisorg I Guidelines and Example Policies
a Understanding CMS Interpretation of F314 b MDS Skin Condition Coding Tip Sheet
II Facility Assessment and Protocols a Facility Assessment Checklists b Sample Protocol
III Resident Assessment and Monitoring Tools a Braden Scale b Skin Tear Risk Assessment c LTC Dehydration Risk Assessment d Comprehensive Admission Skin Assessment e Licensed Nurse Weekly Skin Assessment f CNA Shower Assessment g Daily Skin Monitoring Tool h Systems Investigative Audit Tool
IV Prevention Tools a Pressure Ulcer Prediction Prevention and Treatment Pathway b Tissue Tolerance and Individualized Turning Schedule c Managing Tissue Loads d Support Surface Characteristics and Considerations
V Treatment Tools a Treatment Product Categories b Nutritional Wound Healing Guidelines c Selected Characteristics for Support Surfaces
VI Communication Among Providers a SBAR Skin Care Instructions
VII Education a Resident and Family Education (PUP) Brochure b Facilitystaff education
i Staging Guidelines from National Pressure Ulcer Advisory Panel ii Pressure Ulcer Classification Pocket Cards (see wwwprimarisorg) iii CNA Knowledge and Attitude Survey
Pressure Ulcers Tool Descriptions I Guidelines and Example Policies Understanding CMS Interpretation of F314 Summarizes the changes that CMS put into place with the revision of F-Tag 314 Any time you make changes quickly review this summary to ensure that you are meeting federal guidelines
MDS Skin Condition Coding Tip Sheet Use this tip sheet to see at a glance how your coding questions might be addressed by the RAI manual
II Facility Assessment and Protocols Facility Assessment Checklists Complete this checklist as you review your approach to pressure ulcer prevention and treatment It will help determine your planrsquos comprehensiveness its alignment with F-Tag 314 and good clinical practice
Sample Protocol Use this protocol as a guideline for establishing a comprehensive Pressure Ulcer Prevention and Management Policy Download the file as a separate Word document and modify it to suit your practices and materials
III Resident Assessment and Monitoring Tools Braden Scale The Braden Scale is a research-based risk assessment used widely in the nursing community The format allows for four separate assessments to aid in monitoring change over time
Skin Tear Risk Assessment Evaluating for skin tear risk and interventions is different than evaluating for pressure ulcer risk The skin is our first line of defense and we must protect the skin not only from pressure ulcers but from skin tears as well This assessment helps determine if a resident is at risk for skin tears and offers potential interventions and a chart review audit encouraging staff follow-through
LTC Dehydration Risk Assessment Inadequate fluid intake can place residents at increased risk for pressure ulcers This tool will help determine resident dehydration risk enabling staff to take a proactive approach
Comprehensive Admission Skin Assessment Conducting a baseline comprehensive assessment of the skin is vital Staff may use this form to guide them through the assessment
Licensed Nurse Weekly Skin Assessment All residents should have their skin assessed weekly by a licensed nurse This form encourages continuity in this documentation
CNA Shower Assessment This form recognizes the important role CNAs play in pressure ulcer prevention and empowers them to do regular skin checks It provides a formal method of communication to the licensed nurses of their review of residentsrsquo skin which then would be followed up by the licensed staff
Daily Skin Monitoring Tool This tool provides a formal approach for CNAs to report areas of concern with the residentrsquos skin daily The licensed staff would then follow-up on noted areas of concern to provide a complete assessment
Systems Investigative Audit Tool Use this tool as a guide during a chart review to ensure all appropriate steps are being taken for pressure ulcer prevention and management
continued on next page gt
Pressure Ulcers Tool Descriptions IV Prevention Tools Pressure Ulcer Prediction Prevention and Treatment Pathway This pathway assists staff in determining the appropriate care for the individual resident It aids in staff critical thinking skills to ensure all areas of concern are met
Tissue Tolerance and Individualized Turning Schedule This form can be used to document the assessment that led to the individualized turning schedule
Managing Tissue Loads Use this tool to systematically choose the right mattress or wheel chair cushion based upon a residentrsquos level of need
Support Surfaces Characteristics and Considerations Use this in-depth reference to learn more about the different support surfaces available for pressure ulcer prevention or treatment
V Treatment Tools Treatment Product Categories Use this list outlining the major types of products to ensure your nursing center carries an appropriate range of materials for pressure ulcer treatment Nursing staff should choose the most effective dressing type based on wound stage characteristics and potential concerns
Nutritional Wound Healing Guidelines This sample procedure helps enhance pressure ulcer healing by providing recommendations for nutritional intervention whenever possible These are guidelines only Individual patient and resident needs must be taken into consideration before implementation
Selected Characteristics for Support Surfaces This quick visual reference compares the characteristics of the different types of support surfaces
VI Communication Among Providers SBAR Skin Care Instructions Form Provides a standardized format for communication using the SBAR (Situation Background Assessment Recommendations) model This form would be used in communication from wound care nurse to unit nurse for the prevention andor management of pressure ulcers
VII Education Resident and Family Education Brochure (PUP) Use this brochure to proactively inform residents and families about individual risk factors and prevention techniques associated with skin breakdown so they can be be involved in prevention
Staging Guidelines (National Pressure Ulcer Advisory Panel) These are the most up-to-date guidelines for assessing the state and the subsequent documentation of pressure ulcers
Pressure Ulcer Classification Pocket Cards Two double-sided reference cards were designed to assist clinical staff in the assessment measurement and documentation of wounds Go to wwwprimarisorg to download a pdf of the cards Primaris partner homes may order laminated copies
CNA Knowledge and Attitude Survey CNAsrsquo participation is vital for the prevention of pressure ulcers This survey will assess what your CNAs know about pressure ulcers and discover areas in which they could benefit from further education
Understanding CMS Interpretation of F314
This document summarizes key points of CMS guideline Tag F314 which state surveyors use as guidance to help them assess nursing homesrsquo pressure ulcer prevention and treatment Use this as guidance for assessing the processes in place at your home with regard to pressure ulcer prevention assessment intervention monitoring and care planning
Regulations Pressure Ulcers
F314 42 CFR 48325 (c) Pressure sores Based on the comprehensive assessment of a resident the facility must ensure that ndash bull A resident who enters the facility without pressure sores does not develop pressure sores unless the
individualrsquos clinical condition demonstrates that they were unavoidable and bull A resident having pressure sores receives necessary treatment and services to promote healing prevent
infection and prevent new sores from developingrdquo
F314 Intent bull Promote the prevention of pressure ulcer development bull Promote healing of pressure ulcers that are present bull Prevent development of new pressure ulcers
Survey Pressure Sore Investigative Protocol Objective bull To determine if the identified pressure sore(s) is avoidable or unavoidable bull To determine the adequacy of the facilityrsquos pressure sore treatment interventions
Risk Management bull Identify and manage resident and facility risks bull Prevention of pressure ulcers benefits everyone bull Educate all staff on an ongoing basis bull Provide care based on accepted standards of practice (WOCN AHQR NPUAP) bull Document care based on accepted standards bull Make Care plans realistic especially when discussed with family in care plan conferences bull Watch for indicators of major system failures and initiate quality improvement activities bull Document facts not assumptions bull Rising litigation
ndash What happens when the treatment sheet is not signed off ndash What happens when one lapse in weekly assessment occurs in a period where the wound declines ndash Careful with dressings that stay on several days What happens with weekly assess ndash Carefully consider policies on wound photography may be ldquodouble-edgerdquo sword
Understanding CMS Interpretation of F314 page 2
Three Key Factors for Risk Management bull Medical record must show standard of care for pressure ulcers was adhered to bull Medical record must have documentation of resident complications risk factors andor underlying disease
that made the pressure ulcer unavoidable (if it is indeed) bull You must provide a comprehensive and aggressive program to prevent and treat the pressure ulcer (within
the parameters of resident advance directives)
Prevention bull What systems are in place in your facility
ndash How is risk communicated to staff ndash Are there protocols for repositioning and pressure relief products that are understood by staff ndash How are you sure this is done for new admissions or those with change in status ndash Residents cannot afford to wait
bull How are moisturizersbarriers stocked bull During ldquooff-hoursrdquo do staff know how to access pressure-reducing devices bull Are tracking and assessment forms stocked bull How are disposable briefs and underpads stocked and used
Assessment
Avoidable vs Unavoidable Pressure Ulcers bull Avoidable ndash Pressure ulcer developed and facility failed to do one or more
▷ Definedimplemented interventions CONSISTENT with resident needs goals ▷ Recognized standards of practice (AHCPR AMDA WOCN current literature) ▷ Monitor and evaluate impact of interventions ▷ Revise interventions appropriately
bull Unavoidable ndash Resident developed pressure ulcer although facility ▷ Evaluated clinical condition and risk factors ▷ Defined and implemented interventions consistent with residentrsquos needs goals standards of practice ▷ Monitored and evaluated impact of interventions ▷ Revised approaches appropriately
Frequency of Risk Assessment (Braden or Norton most common) bull Minimally
▷ upon admission ▷ quarterly ▷ upon Significant Change in Condition
bull Best Practice ▷ day 7 14 21 28 (post-admission) then as above ▷ during acute illness
Understanding CMS Interpretation of F314 page 3
Wound Assessment bull Assessment includes a full description of the wound and peri-wound bull Measurements alone do not constitute an assessment bull Reassess weekly at a minimum bull Reassess daily if pressure ulcer is deteriorating
Staging Assessment bull Does your facility policy address your process for staging bull Who does initial staging How is it confirmed bull What are you staging All open areas or only pressure ulcers bull Is there a facility tool for documenting staging
Risk Assessment ndash Facility Wide bull Establish written guidelines protocols algorithmsdecision trees based on risk bull Low risk does not equal no risk bull Let low scores trigger your mind clinically donrsquot just treat the conglomerate of score bull Use appropriate interventions based on the risk assessment
Interventions
Address Risk Factors bull Skincare routine inspections cleansing moisturizing avoid massage bull Repositioning 1 hour in chair by staff 15 minutes in chair by resident 2 hours in bed bull Pressurerelief for heels bull Pressurereduction devices bull Addressnutrition
bull Addressincontinence bull Toileting schedule Rehab Positioning evaluations Incontinence products
Combination of Prevention Interventions bull Adequate nutrition and hydration bull Repositioning schedule and positioning bull Appropriate support surfaces bull Care of skin
Monitoring Wound Status
Is It Better or Worse bull Objectively review wound progress measurements type of tissue PUSH tool bull Subjective assessments are problematic
ndash ldquoI donrsquot think this treatment is working Irsquom calling the MD to change the treatmenthelliprdquo ndash ldquoThe pressure ulcer is deeper than last week - of course it is worserdquo - not necessarily true
Understanding CMS Interpretation of F314 page 4
Monitoring Treatment Plan bull Is there a process for monitoring treatment bull Is there a tracking tool to document response to treatment bull Does the tracking form monitor the appropriate wound variables bull Are there protocols for changing the treatment if it is ineffective bull Healing - a systemic process affected by systemic conditions - treatment is more than a dressing bull When do you change the treatment bull What determines frequency of dsg change bull How do you handle ldquonon-traditionalrdquo recommendations or a product being used in a manner different than
its intended use
Care Planning bull Do care plans identify risk factors bull Are you treating the risk factors bull Is the resident and family aware of and in agreement with goals bull Goal must be a clear statement of intended progress and how it will be measured bull Be REALISTIC bull Determine what the goal is
ndash Maintenance ndash ImprovementHealing ndash Comfort ndash Many goals beyond healinghellip
▷ Resolution of periwound erythema in 2 weeks ▷ 25 reduction in amount of necrotic tissue by 1 week ▷ Decrease in intensity of pain during dressing changes from 6 to 3 (as reported by resident) by 1 week ▷ 1 cm reduction in wound dimensions by 2 weeks
Document available at wwwprimarisorg MO-08-11-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from CMS Provider Certification Transmittal 4 November 12 2004 HCPro Pressure Ulcer Materials 2004 amp Pressure Ulcers F-314 by Courtney Lyder September 2004
MDS Skin Condition Coding Tip Sheet
Definition According the RAI Manual ldquoA skin ulcer can be defined as a local loss of epidermis and variable levels of dermis and subcutaneous tissue or in the case of Stage 1 pressure ulcers persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relievedrdquo (RAI Manual pgs 3-159)
CodingM1 - recording of all skin ulcers if caused by pressure or circulatory problems 1 M1 - recording of all skin ulcers if caused by pressure or 4 M4 - records skin problems or lesions not caused by
circulatory problems pressure or circulatory problems 2 M2 - differentiates between pressure or venous stasis 5 M5 - records any specific or generic skin treatments
ulcers only record highest level of each 6 M6 - records specific foot problems and care 3 M3 - history of resolvedcured ulcers Definition same as for M1
Process 1 Review the record and check with appropriate nursing
staff for the presence of any skin problems 2 Examine the resident for condition (stage number) of
any skin problems Coding will be based on what is seen (ie visible tissue) during the look back period NPUAP standards cannot be used for coding on the MDS MDS defined staging is used for M1 and M2 only
3 Determine the cause of the skin ulcer If it is caused from pressure or circulation (venous or arterial) then it is coded in M1 All remaining skin ulcers then are documented in
M4 (See pg 3-159) Record the number of skin ulcers caused by either pressure or circulatory problems according to stage for M1 M2 is for coding the highest stage of pressure or venous stasis ulcers only
4 Include in M4 all skin problems not caused by pressure venous stasis circulatory problems or not coded anywhere else in Section M
5 Code all skin treatments in M5 6 Code all foot problems and care in M6
Clarification 1 Necrotic eschar prohibits accurate staging Code the skin
ulcer with eschar as Stage 4 until debrided 2 Good clinical practice dictates that the ulcer be reshy
examined and re-staged after debridement 3 If a skin ulcer is repaired with a flap graft it is coded as a
surgical wound and not as a skin ulcer
4 Skin ulcers should be coded in either M1 with further clarification in M2 or in M4 Pressure or stasis ulcers coded in M2 should not be coded in M4
5 If skin ulcers are captured in M1 or M4 good clinical practice would also have something documented in M5 under treatment
6 For MDs coding ankle problems are not considered foot problems
Documentation 1 For clinical practice facilities need to follow the NPUAP
standards in regards to pressure ulcer documentation (ie Healing stage 4 that has the appearance of tissue size and depth of a stage 2- the clinical record will state a healing stage 4 but the MDS would have Stage 2 in M1)
2 Document weekly assessments of the wound healing progress or lack of Documentation should include a thorough description of size drainage etc
3 Care planning should identify risk factors and interventions based on the identified level of risk as well as interventions to facilitate healing of existing skin problems
Example 1 Mrs B has impaired arterial circulation to her right foot She has a Stage 3 in appearance on the top of her foot She also has a
superficial skin tear on her right forearm M1 would be coded as a Stage 3 ulcer M2 would be coded with 0 (zeros) and M4a would be checked for the skin tear M5d e and g may be checked depending on specified interventions M6c would be checked
Document available at wwwprimarisorg MO-08-47-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Gauging Pressure Ulcers Introduction Pressure ulcers are a significant problem across all ages and health care settings Multiple factors put residents at risk for developing a pressure ulcer including immobility chronic illness incontinence poor nutrition altered level of consciousness altered sensory perception and a history of having pressure ulcers1
Pressure ulcers come at a high cost to everyone They result in pain suffering diminished quality of life and even death for some residents For a nursing home they represent extra staff hours and medical supplies spent caring for a preventable condition as well as more residents hospitalized The cost of treating a single full-thickness pressure ulcer can be as high as $70000 with the total treatment cost for pressure ulcers in the US surpassing $11 billion per year2
Although pressure ulcers are preventable more than one in every 10 of Missouri nursing home residents developed a pressure ulcer in 2007 The Centers for Medicare amp Medicaid Services has long focused on helping nursing homes prevent pressure ulcers but in 2008 they extended this effort across care settings Hospitals now have a payment incentive to partner with nursing homes on pressure ulcer prevention ndash a good thing since 20 percent of nursing home pressure ulcers originate outside the nursing home generally in the acute hospital setting
No matter where you are in your prevention efforts now is the time to take a look at your care processes with fresh eyes First review what the law says about pressure ulcers See this toolkitrsquos summary of the federal guidelines ndash Understanding CMS Interpretation of Tag F314 Then use the included Pressure Ulcer Facility Assessment Checklists to take a critical look at your current practices Every one of these systems is crucial to pressure ulcer prevention so take your time completing this assessment As you assess call on other staff to help you answer questions completely and honestly Once yoursquove completed the assessment and identified key areas for improvement review the clinical reference tools reminder tools and sample forms included in this toolkit Feel free to adapt them to meet your individual needs
1 Reddy M Gill SS Rochon PA Preventing pressure ulcers A systematic review JAMA 2006 296 974-984 2 Reddy M Gill SS Rochon PA Preventing pressure ulcers A systematic review JAMA 2006296974-984
Pressure Ulcers Table of Contents This table of contents provides an overview of the assessment and clinical reference tools for pressure ulcers contained in this document For further information see the following pages for tool descriptions organized by section If yoursquore viewing this document on your computer click on the tool name in the table of contents below and you will be taken directly to the resource To download and print tools individually go to wwwprimarisorg I Guidelines and Example Policies
a Understanding CMS Interpretation of F314 b MDS Skin Condition Coding Tip Sheet
II Facility Assessment and Protocols a Facility Assessment Checklists b Sample Protocol
III Resident Assessment and Monitoring Tools a Braden Scale b Skin Tear Risk Assessment c LTC Dehydration Risk Assessment d Comprehensive Admission Skin Assessment e Licensed Nurse Weekly Skin Assessment f CNA Shower Assessment g Daily Skin Monitoring Tool h Systems Investigative Audit Tool
IV Prevention Tools a Pressure Ulcer Prediction Prevention and Treatment Pathway b Tissue Tolerance and Individualized Turning Schedule c Managing Tissue Loads d Support Surface Characteristics and Considerations
V Treatment Tools a Treatment Product Categories b Nutritional Wound Healing Guidelines c Selected Characteristics for Support Surfaces
VI Communication Among Providers a SBAR Skin Care Instructions
VII Education a Resident and Family Education (PUP) Brochure b Facilitystaff education
i Staging Guidelines from National Pressure Ulcer Advisory Panel ii Pressure Ulcer Classification Pocket Cards (see wwwprimarisorg) iii CNA Knowledge and Attitude Survey
Pressure Ulcers Tool Descriptions I Guidelines and Example Policies Understanding CMS Interpretation of F314 Summarizes the changes that CMS put into place with the revision of F-Tag 314 Any time you make changes quickly review this summary to ensure that you are meeting federal guidelines
MDS Skin Condition Coding Tip Sheet Use this tip sheet to see at a glance how your coding questions might be addressed by the RAI manual
II Facility Assessment and Protocols Facility Assessment Checklists Complete this checklist as you review your approach to pressure ulcer prevention and treatment It will help determine your planrsquos comprehensiveness its alignment with F-Tag 314 and good clinical practice
Sample Protocol Use this protocol as a guideline for establishing a comprehensive Pressure Ulcer Prevention and Management Policy Download the file as a separate Word document and modify it to suit your practices and materials
III Resident Assessment and Monitoring Tools Braden Scale The Braden Scale is a research-based risk assessment used widely in the nursing community The format allows for four separate assessments to aid in monitoring change over time
Skin Tear Risk Assessment Evaluating for skin tear risk and interventions is different than evaluating for pressure ulcer risk The skin is our first line of defense and we must protect the skin not only from pressure ulcers but from skin tears as well This assessment helps determine if a resident is at risk for skin tears and offers potential interventions and a chart review audit encouraging staff follow-through
LTC Dehydration Risk Assessment Inadequate fluid intake can place residents at increased risk for pressure ulcers This tool will help determine resident dehydration risk enabling staff to take a proactive approach
Comprehensive Admission Skin Assessment Conducting a baseline comprehensive assessment of the skin is vital Staff may use this form to guide them through the assessment
Licensed Nurse Weekly Skin Assessment All residents should have their skin assessed weekly by a licensed nurse This form encourages continuity in this documentation
CNA Shower Assessment This form recognizes the important role CNAs play in pressure ulcer prevention and empowers them to do regular skin checks It provides a formal method of communication to the licensed nurses of their review of residentsrsquo skin which then would be followed up by the licensed staff
Daily Skin Monitoring Tool This tool provides a formal approach for CNAs to report areas of concern with the residentrsquos skin daily The licensed staff would then follow-up on noted areas of concern to provide a complete assessment
Systems Investigative Audit Tool Use this tool as a guide during a chart review to ensure all appropriate steps are being taken for pressure ulcer prevention and management
continued on next page gt
Pressure Ulcers Tool Descriptions IV Prevention Tools Pressure Ulcer Prediction Prevention and Treatment Pathway This pathway assists staff in determining the appropriate care for the individual resident It aids in staff critical thinking skills to ensure all areas of concern are met
Tissue Tolerance and Individualized Turning Schedule This form can be used to document the assessment that led to the individualized turning schedule
Managing Tissue Loads Use this tool to systematically choose the right mattress or wheel chair cushion based upon a residentrsquos level of need
Support Surfaces Characteristics and Considerations Use this in-depth reference to learn more about the different support surfaces available for pressure ulcer prevention or treatment
V Treatment Tools Treatment Product Categories Use this list outlining the major types of products to ensure your nursing center carries an appropriate range of materials for pressure ulcer treatment Nursing staff should choose the most effective dressing type based on wound stage characteristics and potential concerns
Nutritional Wound Healing Guidelines This sample procedure helps enhance pressure ulcer healing by providing recommendations for nutritional intervention whenever possible These are guidelines only Individual patient and resident needs must be taken into consideration before implementation
Selected Characteristics for Support Surfaces This quick visual reference compares the characteristics of the different types of support surfaces
VI Communication Among Providers SBAR Skin Care Instructions Form Provides a standardized format for communication using the SBAR (Situation Background Assessment Recommendations) model This form would be used in communication from wound care nurse to unit nurse for the prevention andor management of pressure ulcers
VII Education Resident and Family Education Brochure (PUP) Use this brochure to proactively inform residents and families about individual risk factors and prevention techniques associated with skin breakdown so they can be be involved in prevention
Staging Guidelines (National Pressure Ulcer Advisory Panel) These are the most up-to-date guidelines for assessing the state and the subsequent documentation of pressure ulcers
Pressure Ulcer Classification Pocket Cards Two double-sided reference cards were designed to assist clinical staff in the assessment measurement and documentation of wounds Go to wwwprimarisorg to download a pdf of the cards Primaris partner homes may order laminated copies
CNA Knowledge and Attitude Survey CNAsrsquo participation is vital for the prevention of pressure ulcers This survey will assess what your CNAs know about pressure ulcers and discover areas in which they could benefit from further education
Understanding CMS Interpretation of F314
This document summarizes key points of CMS guideline Tag F314 which state surveyors use as guidance to help them assess nursing homesrsquo pressure ulcer prevention and treatment Use this as guidance for assessing the processes in place at your home with regard to pressure ulcer prevention assessment intervention monitoring and care planning
Regulations Pressure Ulcers
F314 42 CFR 48325 (c) Pressure sores Based on the comprehensive assessment of a resident the facility must ensure that ndash bull A resident who enters the facility without pressure sores does not develop pressure sores unless the
individualrsquos clinical condition demonstrates that they were unavoidable and bull A resident having pressure sores receives necessary treatment and services to promote healing prevent
infection and prevent new sores from developingrdquo
F314 Intent bull Promote the prevention of pressure ulcer development bull Promote healing of pressure ulcers that are present bull Prevent development of new pressure ulcers
Survey Pressure Sore Investigative Protocol Objective bull To determine if the identified pressure sore(s) is avoidable or unavoidable bull To determine the adequacy of the facilityrsquos pressure sore treatment interventions
Risk Management bull Identify and manage resident and facility risks bull Prevention of pressure ulcers benefits everyone bull Educate all staff on an ongoing basis bull Provide care based on accepted standards of practice (WOCN AHQR NPUAP) bull Document care based on accepted standards bull Make Care plans realistic especially when discussed with family in care plan conferences bull Watch for indicators of major system failures and initiate quality improvement activities bull Document facts not assumptions bull Rising litigation
ndash What happens when the treatment sheet is not signed off ndash What happens when one lapse in weekly assessment occurs in a period where the wound declines ndash Careful with dressings that stay on several days What happens with weekly assess ndash Carefully consider policies on wound photography may be ldquodouble-edgerdquo sword
Understanding CMS Interpretation of F314 page 2
Three Key Factors for Risk Management bull Medical record must show standard of care for pressure ulcers was adhered to bull Medical record must have documentation of resident complications risk factors andor underlying disease
that made the pressure ulcer unavoidable (if it is indeed) bull You must provide a comprehensive and aggressive program to prevent and treat the pressure ulcer (within
the parameters of resident advance directives)
Prevention bull What systems are in place in your facility
ndash How is risk communicated to staff ndash Are there protocols for repositioning and pressure relief products that are understood by staff ndash How are you sure this is done for new admissions or those with change in status ndash Residents cannot afford to wait
bull How are moisturizersbarriers stocked bull During ldquooff-hoursrdquo do staff know how to access pressure-reducing devices bull Are tracking and assessment forms stocked bull How are disposable briefs and underpads stocked and used
Assessment
Avoidable vs Unavoidable Pressure Ulcers bull Avoidable ndash Pressure ulcer developed and facility failed to do one or more
▷ Definedimplemented interventions CONSISTENT with resident needs goals ▷ Recognized standards of practice (AHCPR AMDA WOCN current literature) ▷ Monitor and evaluate impact of interventions ▷ Revise interventions appropriately
bull Unavoidable ndash Resident developed pressure ulcer although facility ▷ Evaluated clinical condition and risk factors ▷ Defined and implemented interventions consistent with residentrsquos needs goals standards of practice ▷ Monitored and evaluated impact of interventions ▷ Revised approaches appropriately
Frequency of Risk Assessment (Braden or Norton most common) bull Minimally
▷ upon admission ▷ quarterly ▷ upon Significant Change in Condition
bull Best Practice ▷ day 7 14 21 28 (post-admission) then as above ▷ during acute illness
Understanding CMS Interpretation of F314 page 3
Wound Assessment bull Assessment includes a full description of the wound and peri-wound bull Measurements alone do not constitute an assessment bull Reassess weekly at a minimum bull Reassess daily if pressure ulcer is deteriorating
Staging Assessment bull Does your facility policy address your process for staging bull Who does initial staging How is it confirmed bull What are you staging All open areas or only pressure ulcers bull Is there a facility tool for documenting staging
Risk Assessment ndash Facility Wide bull Establish written guidelines protocols algorithmsdecision trees based on risk bull Low risk does not equal no risk bull Let low scores trigger your mind clinically donrsquot just treat the conglomerate of score bull Use appropriate interventions based on the risk assessment
Interventions
Address Risk Factors bull Skincare routine inspections cleansing moisturizing avoid massage bull Repositioning 1 hour in chair by staff 15 minutes in chair by resident 2 hours in bed bull Pressurerelief for heels bull Pressurereduction devices bull Addressnutrition
bull Addressincontinence bull Toileting schedule Rehab Positioning evaluations Incontinence products
Combination of Prevention Interventions bull Adequate nutrition and hydration bull Repositioning schedule and positioning bull Appropriate support surfaces bull Care of skin
Monitoring Wound Status
Is It Better or Worse bull Objectively review wound progress measurements type of tissue PUSH tool bull Subjective assessments are problematic
ndash ldquoI donrsquot think this treatment is working Irsquom calling the MD to change the treatmenthelliprdquo ndash ldquoThe pressure ulcer is deeper than last week - of course it is worserdquo - not necessarily true
Understanding CMS Interpretation of F314 page 4
Monitoring Treatment Plan bull Is there a process for monitoring treatment bull Is there a tracking tool to document response to treatment bull Does the tracking form monitor the appropriate wound variables bull Are there protocols for changing the treatment if it is ineffective bull Healing - a systemic process affected by systemic conditions - treatment is more than a dressing bull When do you change the treatment bull What determines frequency of dsg change bull How do you handle ldquonon-traditionalrdquo recommendations or a product being used in a manner different than
its intended use
Care Planning bull Do care plans identify risk factors bull Are you treating the risk factors bull Is the resident and family aware of and in agreement with goals bull Goal must be a clear statement of intended progress and how it will be measured bull Be REALISTIC bull Determine what the goal is
ndash Maintenance ndash ImprovementHealing ndash Comfort ndash Many goals beyond healinghellip
▷ Resolution of periwound erythema in 2 weeks ▷ 25 reduction in amount of necrotic tissue by 1 week ▷ Decrease in intensity of pain during dressing changes from 6 to 3 (as reported by resident) by 1 week ▷ 1 cm reduction in wound dimensions by 2 weeks
Document available at wwwprimarisorg MO-08-11-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from CMS Provider Certification Transmittal 4 November 12 2004 HCPro Pressure Ulcer Materials 2004 amp Pressure Ulcers F-314 by Courtney Lyder September 2004
MDS Skin Condition Coding Tip Sheet
Definition According the RAI Manual ldquoA skin ulcer can be defined as a local loss of epidermis and variable levels of dermis and subcutaneous tissue or in the case of Stage 1 pressure ulcers persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relievedrdquo (RAI Manual pgs 3-159)
CodingM1 - recording of all skin ulcers if caused by pressure or circulatory problems 1 M1 - recording of all skin ulcers if caused by pressure or 4 M4 - records skin problems or lesions not caused by
circulatory problems pressure or circulatory problems 2 M2 - differentiates between pressure or venous stasis 5 M5 - records any specific or generic skin treatments
ulcers only record highest level of each 6 M6 - records specific foot problems and care 3 M3 - history of resolvedcured ulcers Definition same as for M1
Process 1 Review the record and check with appropriate nursing
staff for the presence of any skin problems 2 Examine the resident for condition (stage number) of
any skin problems Coding will be based on what is seen (ie visible tissue) during the look back period NPUAP standards cannot be used for coding on the MDS MDS defined staging is used for M1 and M2 only
3 Determine the cause of the skin ulcer If it is caused from pressure or circulation (venous or arterial) then it is coded in M1 All remaining skin ulcers then are documented in
M4 (See pg 3-159) Record the number of skin ulcers caused by either pressure or circulatory problems according to stage for M1 M2 is for coding the highest stage of pressure or venous stasis ulcers only
4 Include in M4 all skin problems not caused by pressure venous stasis circulatory problems or not coded anywhere else in Section M
5 Code all skin treatments in M5 6 Code all foot problems and care in M6
Clarification 1 Necrotic eschar prohibits accurate staging Code the skin
ulcer with eschar as Stage 4 until debrided 2 Good clinical practice dictates that the ulcer be reshy
examined and re-staged after debridement 3 If a skin ulcer is repaired with a flap graft it is coded as a
surgical wound and not as a skin ulcer
4 Skin ulcers should be coded in either M1 with further clarification in M2 or in M4 Pressure or stasis ulcers coded in M2 should not be coded in M4
5 If skin ulcers are captured in M1 or M4 good clinical practice would also have something documented in M5 under treatment
6 For MDs coding ankle problems are not considered foot problems
Documentation 1 For clinical practice facilities need to follow the NPUAP
standards in regards to pressure ulcer documentation (ie Healing stage 4 that has the appearance of tissue size and depth of a stage 2- the clinical record will state a healing stage 4 but the MDS would have Stage 2 in M1)
2 Document weekly assessments of the wound healing progress or lack of Documentation should include a thorough description of size drainage etc
3 Care planning should identify risk factors and interventions based on the identified level of risk as well as interventions to facilitate healing of existing skin problems
Example 1 Mrs B has impaired arterial circulation to her right foot She has a Stage 3 in appearance on the top of her foot She also has a
superficial skin tear on her right forearm M1 would be coded as a Stage 3 ulcer M2 would be coded with 0 (zeros) and M4a would be checked for the skin tear M5d e and g may be checked depending on specified interventions M6c would be checked
Document available at wwwprimarisorg MO-08-47-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Table of Contents This table of contents provides an overview of the assessment and clinical reference tools for pressure ulcers contained in this document For further information see the following pages for tool descriptions organized by section If yoursquore viewing this document on your computer click on the tool name in the table of contents below and you will be taken directly to the resource To download and print tools individually go to wwwprimarisorg I Guidelines and Example Policies
a Understanding CMS Interpretation of F314 b MDS Skin Condition Coding Tip Sheet
II Facility Assessment and Protocols a Facility Assessment Checklists b Sample Protocol
III Resident Assessment and Monitoring Tools a Braden Scale b Skin Tear Risk Assessment c LTC Dehydration Risk Assessment d Comprehensive Admission Skin Assessment e Licensed Nurse Weekly Skin Assessment f CNA Shower Assessment g Daily Skin Monitoring Tool h Systems Investigative Audit Tool
IV Prevention Tools a Pressure Ulcer Prediction Prevention and Treatment Pathway b Tissue Tolerance and Individualized Turning Schedule c Managing Tissue Loads d Support Surface Characteristics and Considerations
V Treatment Tools a Treatment Product Categories b Nutritional Wound Healing Guidelines c Selected Characteristics for Support Surfaces
VI Communication Among Providers a SBAR Skin Care Instructions
VII Education a Resident and Family Education (PUP) Brochure b Facilitystaff education
i Staging Guidelines from National Pressure Ulcer Advisory Panel ii Pressure Ulcer Classification Pocket Cards (see wwwprimarisorg) iii CNA Knowledge and Attitude Survey
Pressure Ulcers Tool Descriptions I Guidelines and Example Policies Understanding CMS Interpretation of F314 Summarizes the changes that CMS put into place with the revision of F-Tag 314 Any time you make changes quickly review this summary to ensure that you are meeting federal guidelines
MDS Skin Condition Coding Tip Sheet Use this tip sheet to see at a glance how your coding questions might be addressed by the RAI manual
II Facility Assessment and Protocols Facility Assessment Checklists Complete this checklist as you review your approach to pressure ulcer prevention and treatment It will help determine your planrsquos comprehensiveness its alignment with F-Tag 314 and good clinical practice
Sample Protocol Use this protocol as a guideline for establishing a comprehensive Pressure Ulcer Prevention and Management Policy Download the file as a separate Word document and modify it to suit your practices and materials
III Resident Assessment and Monitoring Tools Braden Scale The Braden Scale is a research-based risk assessment used widely in the nursing community The format allows for four separate assessments to aid in monitoring change over time
Skin Tear Risk Assessment Evaluating for skin tear risk and interventions is different than evaluating for pressure ulcer risk The skin is our first line of defense and we must protect the skin not only from pressure ulcers but from skin tears as well This assessment helps determine if a resident is at risk for skin tears and offers potential interventions and a chart review audit encouraging staff follow-through
LTC Dehydration Risk Assessment Inadequate fluid intake can place residents at increased risk for pressure ulcers This tool will help determine resident dehydration risk enabling staff to take a proactive approach
Comprehensive Admission Skin Assessment Conducting a baseline comprehensive assessment of the skin is vital Staff may use this form to guide them through the assessment
Licensed Nurse Weekly Skin Assessment All residents should have their skin assessed weekly by a licensed nurse This form encourages continuity in this documentation
CNA Shower Assessment This form recognizes the important role CNAs play in pressure ulcer prevention and empowers them to do regular skin checks It provides a formal method of communication to the licensed nurses of their review of residentsrsquo skin which then would be followed up by the licensed staff
Daily Skin Monitoring Tool This tool provides a formal approach for CNAs to report areas of concern with the residentrsquos skin daily The licensed staff would then follow-up on noted areas of concern to provide a complete assessment
Systems Investigative Audit Tool Use this tool as a guide during a chart review to ensure all appropriate steps are being taken for pressure ulcer prevention and management
continued on next page gt
Pressure Ulcers Tool Descriptions IV Prevention Tools Pressure Ulcer Prediction Prevention and Treatment Pathway This pathway assists staff in determining the appropriate care for the individual resident It aids in staff critical thinking skills to ensure all areas of concern are met
Tissue Tolerance and Individualized Turning Schedule This form can be used to document the assessment that led to the individualized turning schedule
Managing Tissue Loads Use this tool to systematically choose the right mattress or wheel chair cushion based upon a residentrsquos level of need
Support Surfaces Characteristics and Considerations Use this in-depth reference to learn more about the different support surfaces available for pressure ulcer prevention or treatment
V Treatment Tools Treatment Product Categories Use this list outlining the major types of products to ensure your nursing center carries an appropriate range of materials for pressure ulcer treatment Nursing staff should choose the most effective dressing type based on wound stage characteristics and potential concerns
Nutritional Wound Healing Guidelines This sample procedure helps enhance pressure ulcer healing by providing recommendations for nutritional intervention whenever possible These are guidelines only Individual patient and resident needs must be taken into consideration before implementation
Selected Characteristics for Support Surfaces This quick visual reference compares the characteristics of the different types of support surfaces
VI Communication Among Providers SBAR Skin Care Instructions Form Provides a standardized format for communication using the SBAR (Situation Background Assessment Recommendations) model This form would be used in communication from wound care nurse to unit nurse for the prevention andor management of pressure ulcers
VII Education Resident and Family Education Brochure (PUP) Use this brochure to proactively inform residents and families about individual risk factors and prevention techniques associated with skin breakdown so they can be be involved in prevention
Staging Guidelines (National Pressure Ulcer Advisory Panel) These are the most up-to-date guidelines for assessing the state and the subsequent documentation of pressure ulcers
Pressure Ulcer Classification Pocket Cards Two double-sided reference cards were designed to assist clinical staff in the assessment measurement and documentation of wounds Go to wwwprimarisorg to download a pdf of the cards Primaris partner homes may order laminated copies
CNA Knowledge and Attitude Survey CNAsrsquo participation is vital for the prevention of pressure ulcers This survey will assess what your CNAs know about pressure ulcers and discover areas in which they could benefit from further education
Understanding CMS Interpretation of F314
This document summarizes key points of CMS guideline Tag F314 which state surveyors use as guidance to help them assess nursing homesrsquo pressure ulcer prevention and treatment Use this as guidance for assessing the processes in place at your home with regard to pressure ulcer prevention assessment intervention monitoring and care planning
Regulations Pressure Ulcers
F314 42 CFR 48325 (c) Pressure sores Based on the comprehensive assessment of a resident the facility must ensure that ndash bull A resident who enters the facility without pressure sores does not develop pressure sores unless the
individualrsquos clinical condition demonstrates that they were unavoidable and bull A resident having pressure sores receives necessary treatment and services to promote healing prevent
infection and prevent new sores from developingrdquo
F314 Intent bull Promote the prevention of pressure ulcer development bull Promote healing of pressure ulcers that are present bull Prevent development of new pressure ulcers
Survey Pressure Sore Investigative Protocol Objective bull To determine if the identified pressure sore(s) is avoidable or unavoidable bull To determine the adequacy of the facilityrsquos pressure sore treatment interventions
Risk Management bull Identify and manage resident and facility risks bull Prevention of pressure ulcers benefits everyone bull Educate all staff on an ongoing basis bull Provide care based on accepted standards of practice (WOCN AHQR NPUAP) bull Document care based on accepted standards bull Make Care plans realistic especially when discussed with family in care plan conferences bull Watch for indicators of major system failures and initiate quality improvement activities bull Document facts not assumptions bull Rising litigation
ndash What happens when the treatment sheet is not signed off ndash What happens when one lapse in weekly assessment occurs in a period where the wound declines ndash Careful with dressings that stay on several days What happens with weekly assess ndash Carefully consider policies on wound photography may be ldquodouble-edgerdquo sword
Understanding CMS Interpretation of F314 page 2
Three Key Factors for Risk Management bull Medical record must show standard of care for pressure ulcers was adhered to bull Medical record must have documentation of resident complications risk factors andor underlying disease
that made the pressure ulcer unavoidable (if it is indeed) bull You must provide a comprehensive and aggressive program to prevent and treat the pressure ulcer (within
the parameters of resident advance directives)
Prevention bull What systems are in place in your facility
ndash How is risk communicated to staff ndash Are there protocols for repositioning and pressure relief products that are understood by staff ndash How are you sure this is done for new admissions or those with change in status ndash Residents cannot afford to wait
bull How are moisturizersbarriers stocked bull During ldquooff-hoursrdquo do staff know how to access pressure-reducing devices bull Are tracking and assessment forms stocked bull How are disposable briefs and underpads stocked and used
Assessment
Avoidable vs Unavoidable Pressure Ulcers bull Avoidable ndash Pressure ulcer developed and facility failed to do one or more
▷ Definedimplemented interventions CONSISTENT with resident needs goals ▷ Recognized standards of practice (AHCPR AMDA WOCN current literature) ▷ Monitor and evaluate impact of interventions ▷ Revise interventions appropriately
bull Unavoidable ndash Resident developed pressure ulcer although facility ▷ Evaluated clinical condition and risk factors ▷ Defined and implemented interventions consistent with residentrsquos needs goals standards of practice ▷ Monitored and evaluated impact of interventions ▷ Revised approaches appropriately
Frequency of Risk Assessment (Braden or Norton most common) bull Minimally
▷ upon admission ▷ quarterly ▷ upon Significant Change in Condition
bull Best Practice ▷ day 7 14 21 28 (post-admission) then as above ▷ during acute illness
Understanding CMS Interpretation of F314 page 3
Wound Assessment bull Assessment includes a full description of the wound and peri-wound bull Measurements alone do not constitute an assessment bull Reassess weekly at a minimum bull Reassess daily if pressure ulcer is deteriorating
Staging Assessment bull Does your facility policy address your process for staging bull Who does initial staging How is it confirmed bull What are you staging All open areas or only pressure ulcers bull Is there a facility tool for documenting staging
Risk Assessment ndash Facility Wide bull Establish written guidelines protocols algorithmsdecision trees based on risk bull Low risk does not equal no risk bull Let low scores trigger your mind clinically donrsquot just treat the conglomerate of score bull Use appropriate interventions based on the risk assessment
Interventions
Address Risk Factors bull Skincare routine inspections cleansing moisturizing avoid massage bull Repositioning 1 hour in chair by staff 15 minutes in chair by resident 2 hours in bed bull Pressurerelief for heels bull Pressurereduction devices bull Addressnutrition
bull Addressincontinence bull Toileting schedule Rehab Positioning evaluations Incontinence products
Combination of Prevention Interventions bull Adequate nutrition and hydration bull Repositioning schedule and positioning bull Appropriate support surfaces bull Care of skin
Monitoring Wound Status
Is It Better or Worse bull Objectively review wound progress measurements type of tissue PUSH tool bull Subjective assessments are problematic
ndash ldquoI donrsquot think this treatment is working Irsquom calling the MD to change the treatmenthelliprdquo ndash ldquoThe pressure ulcer is deeper than last week - of course it is worserdquo - not necessarily true
Understanding CMS Interpretation of F314 page 4
Monitoring Treatment Plan bull Is there a process for monitoring treatment bull Is there a tracking tool to document response to treatment bull Does the tracking form monitor the appropriate wound variables bull Are there protocols for changing the treatment if it is ineffective bull Healing - a systemic process affected by systemic conditions - treatment is more than a dressing bull When do you change the treatment bull What determines frequency of dsg change bull How do you handle ldquonon-traditionalrdquo recommendations or a product being used in a manner different than
its intended use
Care Planning bull Do care plans identify risk factors bull Are you treating the risk factors bull Is the resident and family aware of and in agreement with goals bull Goal must be a clear statement of intended progress and how it will be measured bull Be REALISTIC bull Determine what the goal is
ndash Maintenance ndash ImprovementHealing ndash Comfort ndash Many goals beyond healinghellip
▷ Resolution of periwound erythema in 2 weeks ▷ 25 reduction in amount of necrotic tissue by 1 week ▷ Decrease in intensity of pain during dressing changes from 6 to 3 (as reported by resident) by 1 week ▷ 1 cm reduction in wound dimensions by 2 weeks
Document available at wwwprimarisorg MO-08-11-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from CMS Provider Certification Transmittal 4 November 12 2004 HCPro Pressure Ulcer Materials 2004 amp Pressure Ulcers F-314 by Courtney Lyder September 2004
MDS Skin Condition Coding Tip Sheet
Definition According the RAI Manual ldquoA skin ulcer can be defined as a local loss of epidermis and variable levels of dermis and subcutaneous tissue or in the case of Stage 1 pressure ulcers persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relievedrdquo (RAI Manual pgs 3-159)
CodingM1 - recording of all skin ulcers if caused by pressure or circulatory problems 1 M1 - recording of all skin ulcers if caused by pressure or 4 M4 - records skin problems or lesions not caused by
circulatory problems pressure or circulatory problems 2 M2 - differentiates between pressure or venous stasis 5 M5 - records any specific or generic skin treatments
ulcers only record highest level of each 6 M6 - records specific foot problems and care 3 M3 - history of resolvedcured ulcers Definition same as for M1
Process 1 Review the record and check with appropriate nursing
staff for the presence of any skin problems 2 Examine the resident for condition (stage number) of
any skin problems Coding will be based on what is seen (ie visible tissue) during the look back period NPUAP standards cannot be used for coding on the MDS MDS defined staging is used for M1 and M2 only
3 Determine the cause of the skin ulcer If it is caused from pressure or circulation (venous or arterial) then it is coded in M1 All remaining skin ulcers then are documented in
M4 (See pg 3-159) Record the number of skin ulcers caused by either pressure or circulatory problems according to stage for M1 M2 is for coding the highest stage of pressure or venous stasis ulcers only
4 Include in M4 all skin problems not caused by pressure venous stasis circulatory problems or not coded anywhere else in Section M
5 Code all skin treatments in M5 6 Code all foot problems and care in M6
Clarification 1 Necrotic eschar prohibits accurate staging Code the skin
ulcer with eschar as Stage 4 until debrided 2 Good clinical practice dictates that the ulcer be reshy
examined and re-staged after debridement 3 If a skin ulcer is repaired with a flap graft it is coded as a
surgical wound and not as a skin ulcer
4 Skin ulcers should be coded in either M1 with further clarification in M2 or in M4 Pressure or stasis ulcers coded in M2 should not be coded in M4
5 If skin ulcers are captured in M1 or M4 good clinical practice would also have something documented in M5 under treatment
6 For MDs coding ankle problems are not considered foot problems
Documentation 1 For clinical practice facilities need to follow the NPUAP
standards in regards to pressure ulcer documentation (ie Healing stage 4 that has the appearance of tissue size and depth of a stage 2- the clinical record will state a healing stage 4 but the MDS would have Stage 2 in M1)
2 Document weekly assessments of the wound healing progress or lack of Documentation should include a thorough description of size drainage etc
3 Care planning should identify risk factors and interventions based on the identified level of risk as well as interventions to facilitate healing of existing skin problems
Example 1 Mrs B has impaired arterial circulation to her right foot She has a Stage 3 in appearance on the top of her foot She also has a
superficial skin tear on her right forearm M1 would be coded as a Stage 3 ulcer M2 would be coded with 0 (zeros) and M4a would be checked for the skin tear M5d e and g may be checked depending on specified interventions M6c would be checked
Document available at wwwprimarisorg MO-08-47-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Tool Descriptions I Guidelines and Example Policies Understanding CMS Interpretation of F314 Summarizes the changes that CMS put into place with the revision of F-Tag 314 Any time you make changes quickly review this summary to ensure that you are meeting federal guidelines
MDS Skin Condition Coding Tip Sheet Use this tip sheet to see at a glance how your coding questions might be addressed by the RAI manual
II Facility Assessment and Protocols Facility Assessment Checklists Complete this checklist as you review your approach to pressure ulcer prevention and treatment It will help determine your planrsquos comprehensiveness its alignment with F-Tag 314 and good clinical practice
Sample Protocol Use this protocol as a guideline for establishing a comprehensive Pressure Ulcer Prevention and Management Policy Download the file as a separate Word document and modify it to suit your practices and materials
III Resident Assessment and Monitoring Tools Braden Scale The Braden Scale is a research-based risk assessment used widely in the nursing community The format allows for four separate assessments to aid in monitoring change over time
Skin Tear Risk Assessment Evaluating for skin tear risk and interventions is different than evaluating for pressure ulcer risk The skin is our first line of defense and we must protect the skin not only from pressure ulcers but from skin tears as well This assessment helps determine if a resident is at risk for skin tears and offers potential interventions and a chart review audit encouraging staff follow-through
LTC Dehydration Risk Assessment Inadequate fluid intake can place residents at increased risk for pressure ulcers This tool will help determine resident dehydration risk enabling staff to take a proactive approach
Comprehensive Admission Skin Assessment Conducting a baseline comprehensive assessment of the skin is vital Staff may use this form to guide them through the assessment
Licensed Nurse Weekly Skin Assessment All residents should have their skin assessed weekly by a licensed nurse This form encourages continuity in this documentation
CNA Shower Assessment This form recognizes the important role CNAs play in pressure ulcer prevention and empowers them to do regular skin checks It provides a formal method of communication to the licensed nurses of their review of residentsrsquo skin which then would be followed up by the licensed staff
Daily Skin Monitoring Tool This tool provides a formal approach for CNAs to report areas of concern with the residentrsquos skin daily The licensed staff would then follow-up on noted areas of concern to provide a complete assessment
Systems Investigative Audit Tool Use this tool as a guide during a chart review to ensure all appropriate steps are being taken for pressure ulcer prevention and management
continued on next page gt
Pressure Ulcers Tool Descriptions IV Prevention Tools Pressure Ulcer Prediction Prevention and Treatment Pathway This pathway assists staff in determining the appropriate care for the individual resident It aids in staff critical thinking skills to ensure all areas of concern are met
Tissue Tolerance and Individualized Turning Schedule This form can be used to document the assessment that led to the individualized turning schedule
Managing Tissue Loads Use this tool to systematically choose the right mattress or wheel chair cushion based upon a residentrsquos level of need
Support Surfaces Characteristics and Considerations Use this in-depth reference to learn more about the different support surfaces available for pressure ulcer prevention or treatment
V Treatment Tools Treatment Product Categories Use this list outlining the major types of products to ensure your nursing center carries an appropriate range of materials for pressure ulcer treatment Nursing staff should choose the most effective dressing type based on wound stage characteristics and potential concerns
Nutritional Wound Healing Guidelines This sample procedure helps enhance pressure ulcer healing by providing recommendations for nutritional intervention whenever possible These are guidelines only Individual patient and resident needs must be taken into consideration before implementation
Selected Characteristics for Support Surfaces This quick visual reference compares the characteristics of the different types of support surfaces
VI Communication Among Providers SBAR Skin Care Instructions Form Provides a standardized format for communication using the SBAR (Situation Background Assessment Recommendations) model This form would be used in communication from wound care nurse to unit nurse for the prevention andor management of pressure ulcers
VII Education Resident and Family Education Brochure (PUP) Use this brochure to proactively inform residents and families about individual risk factors and prevention techniques associated with skin breakdown so they can be be involved in prevention
Staging Guidelines (National Pressure Ulcer Advisory Panel) These are the most up-to-date guidelines for assessing the state and the subsequent documentation of pressure ulcers
Pressure Ulcer Classification Pocket Cards Two double-sided reference cards were designed to assist clinical staff in the assessment measurement and documentation of wounds Go to wwwprimarisorg to download a pdf of the cards Primaris partner homes may order laminated copies
CNA Knowledge and Attitude Survey CNAsrsquo participation is vital for the prevention of pressure ulcers This survey will assess what your CNAs know about pressure ulcers and discover areas in which they could benefit from further education
Understanding CMS Interpretation of F314
This document summarizes key points of CMS guideline Tag F314 which state surveyors use as guidance to help them assess nursing homesrsquo pressure ulcer prevention and treatment Use this as guidance for assessing the processes in place at your home with regard to pressure ulcer prevention assessment intervention monitoring and care planning
Regulations Pressure Ulcers
F314 42 CFR 48325 (c) Pressure sores Based on the comprehensive assessment of a resident the facility must ensure that ndash bull A resident who enters the facility without pressure sores does not develop pressure sores unless the
individualrsquos clinical condition demonstrates that they were unavoidable and bull A resident having pressure sores receives necessary treatment and services to promote healing prevent
infection and prevent new sores from developingrdquo
F314 Intent bull Promote the prevention of pressure ulcer development bull Promote healing of pressure ulcers that are present bull Prevent development of new pressure ulcers
Survey Pressure Sore Investigative Protocol Objective bull To determine if the identified pressure sore(s) is avoidable or unavoidable bull To determine the adequacy of the facilityrsquos pressure sore treatment interventions
Risk Management bull Identify and manage resident and facility risks bull Prevention of pressure ulcers benefits everyone bull Educate all staff on an ongoing basis bull Provide care based on accepted standards of practice (WOCN AHQR NPUAP) bull Document care based on accepted standards bull Make Care plans realistic especially when discussed with family in care plan conferences bull Watch for indicators of major system failures and initiate quality improvement activities bull Document facts not assumptions bull Rising litigation
ndash What happens when the treatment sheet is not signed off ndash What happens when one lapse in weekly assessment occurs in a period where the wound declines ndash Careful with dressings that stay on several days What happens with weekly assess ndash Carefully consider policies on wound photography may be ldquodouble-edgerdquo sword
Understanding CMS Interpretation of F314 page 2
Three Key Factors for Risk Management bull Medical record must show standard of care for pressure ulcers was adhered to bull Medical record must have documentation of resident complications risk factors andor underlying disease
that made the pressure ulcer unavoidable (if it is indeed) bull You must provide a comprehensive and aggressive program to prevent and treat the pressure ulcer (within
the parameters of resident advance directives)
Prevention bull What systems are in place in your facility
ndash How is risk communicated to staff ndash Are there protocols for repositioning and pressure relief products that are understood by staff ndash How are you sure this is done for new admissions or those with change in status ndash Residents cannot afford to wait
bull How are moisturizersbarriers stocked bull During ldquooff-hoursrdquo do staff know how to access pressure-reducing devices bull Are tracking and assessment forms stocked bull How are disposable briefs and underpads stocked and used
Assessment
Avoidable vs Unavoidable Pressure Ulcers bull Avoidable ndash Pressure ulcer developed and facility failed to do one or more
▷ Definedimplemented interventions CONSISTENT with resident needs goals ▷ Recognized standards of practice (AHCPR AMDA WOCN current literature) ▷ Monitor and evaluate impact of interventions ▷ Revise interventions appropriately
bull Unavoidable ndash Resident developed pressure ulcer although facility ▷ Evaluated clinical condition and risk factors ▷ Defined and implemented interventions consistent with residentrsquos needs goals standards of practice ▷ Monitored and evaluated impact of interventions ▷ Revised approaches appropriately
Frequency of Risk Assessment (Braden or Norton most common) bull Minimally
▷ upon admission ▷ quarterly ▷ upon Significant Change in Condition
bull Best Practice ▷ day 7 14 21 28 (post-admission) then as above ▷ during acute illness
Understanding CMS Interpretation of F314 page 3
Wound Assessment bull Assessment includes a full description of the wound and peri-wound bull Measurements alone do not constitute an assessment bull Reassess weekly at a minimum bull Reassess daily if pressure ulcer is deteriorating
Staging Assessment bull Does your facility policy address your process for staging bull Who does initial staging How is it confirmed bull What are you staging All open areas or only pressure ulcers bull Is there a facility tool for documenting staging
Risk Assessment ndash Facility Wide bull Establish written guidelines protocols algorithmsdecision trees based on risk bull Low risk does not equal no risk bull Let low scores trigger your mind clinically donrsquot just treat the conglomerate of score bull Use appropriate interventions based on the risk assessment
Interventions
Address Risk Factors bull Skincare routine inspections cleansing moisturizing avoid massage bull Repositioning 1 hour in chair by staff 15 minutes in chair by resident 2 hours in bed bull Pressurerelief for heels bull Pressurereduction devices bull Addressnutrition
bull Addressincontinence bull Toileting schedule Rehab Positioning evaluations Incontinence products
Combination of Prevention Interventions bull Adequate nutrition and hydration bull Repositioning schedule and positioning bull Appropriate support surfaces bull Care of skin
Monitoring Wound Status
Is It Better or Worse bull Objectively review wound progress measurements type of tissue PUSH tool bull Subjective assessments are problematic
ndash ldquoI donrsquot think this treatment is working Irsquom calling the MD to change the treatmenthelliprdquo ndash ldquoThe pressure ulcer is deeper than last week - of course it is worserdquo - not necessarily true
Understanding CMS Interpretation of F314 page 4
Monitoring Treatment Plan bull Is there a process for monitoring treatment bull Is there a tracking tool to document response to treatment bull Does the tracking form monitor the appropriate wound variables bull Are there protocols for changing the treatment if it is ineffective bull Healing - a systemic process affected by systemic conditions - treatment is more than a dressing bull When do you change the treatment bull What determines frequency of dsg change bull How do you handle ldquonon-traditionalrdquo recommendations or a product being used in a manner different than
its intended use
Care Planning bull Do care plans identify risk factors bull Are you treating the risk factors bull Is the resident and family aware of and in agreement with goals bull Goal must be a clear statement of intended progress and how it will be measured bull Be REALISTIC bull Determine what the goal is
ndash Maintenance ndash ImprovementHealing ndash Comfort ndash Many goals beyond healinghellip
▷ Resolution of periwound erythema in 2 weeks ▷ 25 reduction in amount of necrotic tissue by 1 week ▷ Decrease in intensity of pain during dressing changes from 6 to 3 (as reported by resident) by 1 week ▷ 1 cm reduction in wound dimensions by 2 weeks
Document available at wwwprimarisorg MO-08-11-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from CMS Provider Certification Transmittal 4 November 12 2004 HCPro Pressure Ulcer Materials 2004 amp Pressure Ulcers F-314 by Courtney Lyder September 2004
MDS Skin Condition Coding Tip Sheet
Definition According the RAI Manual ldquoA skin ulcer can be defined as a local loss of epidermis and variable levels of dermis and subcutaneous tissue or in the case of Stage 1 pressure ulcers persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relievedrdquo (RAI Manual pgs 3-159)
CodingM1 - recording of all skin ulcers if caused by pressure or circulatory problems 1 M1 - recording of all skin ulcers if caused by pressure or 4 M4 - records skin problems or lesions not caused by
circulatory problems pressure or circulatory problems 2 M2 - differentiates between pressure or venous stasis 5 M5 - records any specific or generic skin treatments
ulcers only record highest level of each 6 M6 - records specific foot problems and care 3 M3 - history of resolvedcured ulcers Definition same as for M1
Process 1 Review the record and check with appropriate nursing
staff for the presence of any skin problems 2 Examine the resident for condition (stage number) of
any skin problems Coding will be based on what is seen (ie visible tissue) during the look back period NPUAP standards cannot be used for coding on the MDS MDS defined staging is used for M1 and M2 only
3 Determine the cause of the skin ulcer If it is caused from pressure or circulation (venous or arterial) then it is coded in M1 All remaining skin ulcers then are documented in
M4 (See pg 3-159) Record the number of skin ulcers caused by either pressure or circulatory problems according to stage for M1 M2 is for coding the highest stage of pressure or venous stasis ulcers only
4 Include in M4 all skin problems not caused by pressure venous stasis circulatory problems or not coded anywhere else in Section M
5 Code all skin treatments in M5 6 Code all foot problems and care in M6
Clarification 1 Necrotic eschar prohibits accurate staging Code the skin
ulcer with eschar as Stage 4 until debrided 2 Good clinical practice dictates that the ulcer be reshy
examined and re-staged after debridement 3 If a skin ulcer is repaired with a flap graft it is coded as a
surgical wound and not as a skin ulcer
4 Skin ulcers should be coded in either M1 with further clarification in M2 or in M4 Pressure or stasis ulcers coded in M2 should not be coded in M4
5 If skin ulcers are captured in M1 or M4 good clinical practice would also have something documented in M5 under treatment
6 For MDs coding ankle problems are not considered foot problems
Documentation 1 For clinical practice facilities need to follow the NPUAP
standards in regards to pressure ulcer documentation (ie Healing stage 4 that has the appearance of tissue size and depth of a stage 2- the clinical record will state a healing stage 4 but the MDS would have Stage 2 in M1)
2 Document weekly assessments of the wound healing progress or lack of Documentation should include a thorough description of size drainage etc
3 Care planning should identify risk factors and interventions based on the identified level of risk as well as interventions to facilitate healing of existing skin problems
Example 1 Mrs B has impaired arterial circulation to her right foot She has a Stage 3 in appearance on the top of her foot She also has a
superficial skin tear on her right forearm M1 would be coded as a Stage 3 ulcer M2 would be coded with 0 (zeros) and M4a would be checked for the skin tear M5d e and g may be checked depending on specified interventions M6c would be checked
Document available at wwwprimarisorg MO-08-47-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Tool Descriptions IV Prevention Tools Pressure Ulcer Prediction Prevention and Treatment Pathway This pathway assists staff in determining the appropriate care for the individual resident It aids in staff critical thinking skills to ensure all areas of concern are met
Tissue Tolerance and Individualized Turning Schedule This form can be used to document the assessment that led to the individualized turning schedule
Managing Tissue Loads Use this tool to systematically choose the right mattress or wheel chair cushion based upon a residentrsquos level of need
Support Surfaces Characteristics and Considerations Use this in-depth reference to learn more about the different support surfaces available for pressure ulcer prevention or treatment
V Treatment Tools Treatment Product Categories Use this list outlining the major types of products to ensure your nursing center carries an appropriate range of materials for pressure ulcer treatment Nursing staff should choose the most effective dressing type based on wound stage characteristics and potential concerns
Nutritional Wound Healing Guidelines This sample procedure helps enhance pressure ulcer healing by providing recommendations for nutritional intervention whenever possible These are guidelines only Individual patient and resident needs must be taken into consideration before implementation
Selected Characteristics for Support Surfaces This quick visual reference compares the characteristics of the different types of support surfaces
VI Communication Among Providers SBAR Skin Care Instructions Form Provides a standardized format for communication using the SBAR (Situation Background Assessment Recommendations) model This form would be used in communication from wound care nurse to unit nurse for the prevention andor management of pressure ulcers
VII Education Resident and Family Education Brochure (PUP) Use this brochure to proactively inform residents and families about individual risk factors and prevention techniques associated with skin breakdown so they can be be involved in prevention
Staging Guidelines (National Pressure Ulcer Advisory Panel) These are the most up-to-date guidelines for assessing the state and the subsequent documentation of pressure ulcers
Pressure Ulcer Classification Pocket Cards Two double-sided reference cards were designed to assist clinical staff in the assessment measurement and documentation of wounds Go to wwwprimarisorg to download a pdf of the cards Primaris partner homes may order laminated copies
CNA Knowledge and Attitude Survey CNAsrsquo participation is vital for the prevention of pressure ulcers This survey will assess what your CNAs know about pressure ulcers and discover areas in which they could benefit from further education
Understanding CMS Interpretation of F314
This document summarizes key points of CMS guideline Tag F314 which state surveyors use as guidance to help them assess nursing homesrsquo pressure ulcer prevention and treatment Use this as guidance for assessing the processes in place at your home with regard to pressure ulcer prevention assessment intervention monitoring and care planning
Regulations Pressure Ulcers
F314 42 CFR 48325 (c) Pressure sores Based on the comprehensive assessment of a resident the facility must ensure that ndash bull A resident who enters the facility without pressure sores does not develop pressure sores unless the
individualrsquos clinical condition demonstrates that they were unavoidable and bull A resident having pressure sores receives necessary treatment and services to promote healing prevent
infection and prevent new sores from developingrdquo
F314 Intent bull Promote the prevention of pressure ulcer development bull Promote healing of pressure ulcers that are present bull Prevent development of new pressure ulcers
Survey Pressure Sore Investigative Protocol Objective bull To determine if the identified pressure sore(s) is avoidable or unavoidable bull To determine the adequacy of the facilityrsquos pressure sore treatment interventions
Risk Management bull Identify and manage resident and facility risks bull Prevention of pressure ulcers benefits everyone bull Educate all staff on an ongoing basis bull Provide care based on accepted standards of practice (WOCN AHQR NPUAP) bull Document care based on accepted standards bull Make Care plans realistic especially when discussed with family in care plan conferences bull Watch for indicators of major system failures and initiate quality improvement activities bull Document facts not assumptions bull Rising litigation
ndash What happens when the treatment sheet is not signed off ndash What happens when one lapse in weekly assessment occurs in a period where the wound declines ndash Careful with dressings that stay on several days What happens with weekly assess ndash Carefully consider policies on wound photography may be ldquodouble-edgerdquo sword
Understanding CMS Interpretation of F314 page 2
Three Key Factors for Risk Management bull Medical record must show standard of care for pressure ulcers was adhered to bull Medical record must have documentation of resident complications risk factors andor underlying disease
that made the pressure ulcer unavoidable (if it is indeed) bull You must provide a comprehensive and aggressive program to prevent and treat the pressure ulcer (within
the parameters of resident advance directives)
Prevention bull What systems are in place in your facility
ndash How is risk communicated to staff ndash Are there protocols for repositioning and pressure relief products that are understood by staff ndash How are you sure this is done for new admissions or those with change in status ndash Residents cannot afford to wait
bull How are moisturizersbarriers stocked bull During ldquooff-hoursrdquo do staff know how to access pressure-reducing devices bull Are tracking and assessment forms stocked bull How are disposable briefs and underpads stocked and used
Assessment
Avoidable vs Unavoidable Pressure Ulcers bull Avoidable ndash Pressure ulcer developed and facility failed to do one or more
▷ Definedimplemented interventions CONSISTENT with resident needs goals ▷ Recognized standards of practice (AHCPR AMDA WOCN current literature) ▷ Monitor and evaluate impact of interventions ▷ Revise interventions appropriately
bull Unavoidable ndash Resident developed pressure ulcer although facility ▷ Evaluated clinical condition and risk factors ▷ Defined and implemented interventions consistent with residentrsquos needs goals standards of practice ▷ Monitored and evaluated impact of interventions ▷ Revised approaches appropriately
Frequency of Risk Assessment (Braden or Norton most common) bull Minimally
▷ upon admission ▷ quarterly ▷ upon Significant Change in Condition
bull Best Practice ▷ day 7 14 21 28 (post-admission) then as above ▷ during acute illness
Understanding CMS Interpretation of F314 page 3
Wound Assessment bull Assessment includes a full description of the wound and peri-wound bull Measurements alone do not constitute an assessment bull Reassess weekly at a minimum bull Reassess daily if pressure ulcer is deteriorating
Staging Assessment bull Does your facility policy address your process for staging bull Who does initial staging How is it confirmed bull What are you staging All open areas or only pressure ulcers bull Is there a facility tool for documenting staging
Risk Assessment ndash Facility Wide bull Establish written guidelines protocols algorithmsdecision trees based on risk bull Low risk does not equal no risk bull Let low scores trigger your mind clinically donrsquot just treat the conglomerate of score bull Use appropriate interventions based on the risk assessment
Interventions
Address Risk Factors bull Skincare routine inspections cleansing moisturizing avoid massage bull Repositioning 1 hour in chair by staff 15 minutes in chair by resident 2 hours in bed bull Pressurerelief for heels bull Pressurereduction devices bull Addressnutrition
bull Addressincontinence bull Toileting schedule Rehab Positioning evaluations Incontinence products
Combination of Prevention Interventions bull Adequate nutrition and hydration bull Repositioning schedule and positioning bull Appropriate support surfaces bull Care of skin
Monitoring Wound Status
Is It Better or Worse bull Objectively review wound progress measurements type of tissue PUSH tool bull Subjective assessments are problematic
ndash ldquoI donrsquot think this treatment is working Irsquom calling the MD to change the treatmenthelliprdquo ndash ldquoThe pressure ulcer is deeper than last week - of course it is worserdquo - not necessarily true
Understanding CMS Interpretation of F314 page 4
Monitoring Treatment Plan bull Is there a process for monitoring treatment bull Is there a tracking tool to document response to treatment bull Does the tracking form monitor the appropriate wound variables bull Are there protocols for changing the treatment if it is ineffective bull Healing - a systemic process affected by systemic conditions - treatment is more than a dressing bull When do you change the treatment bull What determines frequency of dsg change bull How do you handle ldquonon-traditionalrdquo recommendations or a product being used in a manner different than
its intended use
Care Planning bull Do care plans identify risk factors bull Are you treating the risk factors bull Is the resident and family aware of and in agreement with goals bull Goal must be a clear statement of intended progress and how it will be measured bull Be REALISTIC bull Determine what the goal is
ndash Maintenance ndash ImprovementHealing ndash Comfort ndash Many goals beyond healinghellip
▷ Resolution of periwound erythema in 2 weeks ▷ 25 reduction in amount of necrotic tissue by 1 week ▷ Decrease in intensity of pain during dressing changes from 6 to 3 (as reported by resident) by 1 week ▷ 1 cm reduction in wound dimensions by 2 weeks
Document available at wwwprimarisorg MO-08-11-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from CMS Provider Certification Transmittal 4 November 12 2004 HCPro Pressure Ulcer Materials 2004 amp Pressure Ulcers F-314 by Courtney Lyder September 2004
MDS Skin Condition Coding Tip Sheet
Definition According the RAI Manual ldquoA skin ulcer can be defined as a local loss of epidermis and variable levels of dermis and subcutaneous tissue or in the case of Stage 1 pressure ulcers persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relievedrdquo (RAI Manual pgs 3-159)
CodingM1 - recording of all skin ulcers if caused by pressure or circulatory problems 1 M1 - recording of all skin ulcers if caused by pressure or 4 M4 - records skin problems or lesions not caused by
circulatory problems pressure or circulatory problems 2 M2 - differentiates between pressure or venous stasis 5 M5 - records any specific or generic skin treatments
ulcers only record highest level of each 6 M6 - records specific foot problems and care 3 M3 - history of resolvedcured ulcers Definition same as for M1
Process 1 Review the record and check with appropriate nursing
staff for the presence of any skin problems 2 Examine the resident for condition (stage number) of
any skin problems Coding will be based on what is seen (ie visible tissue) during the look back period NPUAP standards cannot be used for coding on the MDS MDS defined staging is used for M1 and M2 only
3 Determine the cause of the skin ulcer If it is caused from pressure or circulation (venous or arterial) then it is coded in M1 All remaining skin ulcers then are documented in
M4 (See pg 3-159) Record the number of skin ulcers caused by either pressure or circulatory problems according to stage for M1 M2 is for coding the highest stage of pressure or venous stasis ulcers only
4 Include in M4 all skin problems not caused by pressure venous stasis circulatory problems or not coded anywhere else in Section M
5 Code all skin treatments in M5 6 Code all foot problems and care in M6
Clarification 1 Necrotic eschar prohibits accurate staging Code the skin
ulcer with eschar as Stage 4 until debrided 2 Good clinical practice dictates that the ulcer be reshy
examined and re-staged after debridement 3 If a skin ulcer is repaired with a flap graft it is coded as a
surgical wound and not as a skin ulcer
4 Skin ulcers should be coded in either M1 with further clarification in M2 or in M4 Pressure or stasis ulcers coded in M2 should not be coded in M4
5 If skin ulcers are captured in M1 or M4 good clinical practice would also have something documented in M5 under treatment
6 For MDs coding ankle problems are not considered foot problems
Documentation 1 For clinical practice facilities need to follow the NPUAP
standards in regards to pressure ulcer documentation (ie Healing stage 4 that has the appearance of tissue size and depth of a stage 2- the clinical record will state a healing stage 4 but the MDS would have Stage 2 in M1)
2 Document weekly assessments of the wound healing progress or lack of Documentation should include a thorough description of size drainage etc
3 Care planning should identify risk factors and interventions based on the identified level of risk as well as interventions to facilitate healing of existing skin problems
Example 1 Mrs B has impaired arterial circulation to her right foot She has a Stage 3 in appearance on the top of her foot She also has a
superficial skin tear on her right forearm M1 would be coded as a Stage 3 ulcer M2 would be coded with 0 (zeros) and M4a would be checked for the skin tear M5d e and g may be checked depending on specified interventions M6c would be checked
Document available at wwwprimarisorg MO-08-47-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Understanding CMS Interpretation of F314
This document summarizes key points of CMS guideline Tag F314 which state surveyors use as guidance to help them assess nursing homesrsquo pressure ulcer prevention and treatment Use this as guidance for assessing the processes in place at your home with regard to pressure ulcer prevention assessment intervention monitoring and care planning
Regulations Pressure Ulcers
F314 42 CFR 48325 (c) Pressure sores Based on the comprehensive assessment of a resident the facility must ensure that ndash bull A resident who enters the facility without pressure sores does not develop pressure sores unless the
individualrsquos clinical condition demonstrates that they were unavoidable and bull A resident having pressure sores receives necessary treatment and services to promote healing prevent
infection and prevent new sores from developingrdquo
F314 Intent bull Promote the prevention of pressure ulcer development bull Promote healing of pressure ulcers that are present bull Prevent development of new pressure ulcers
Survey Pressure Sore Investigative Protocol Objective bull To determine if the identified pressure sore(s) is avoidable or unavoidable bull To determine the adequacy of the facilityrsquos pressure sore treatment interventions
Risk Management bull Identify and manage resident and facility risks bull Prevention of pressure ulcers benefits everyone bull Educate all staff on an ongoing basis bull Provide care based on accepted standards of practice (WOCN AHQR NPUAP) bull Document care based on accepted standards bull Make Care plans realistic especially when discussed with family in care plan conferences bull Watch for indicators of major system failures and initiate quality improvement activities bull Document facts not assumptions bull Rising litigation
ndash What happens when the treatment sheet is not signed off ndash What happens when one lapse in weekly assessment occurs in a period where the wound declines ndash Careful with dressings that stay on several days What happens with weekly assess ndash Carefully consider policies on wound photography may be ldquodouble-edgerdquo sword
Understanding CMS Interpretation of F314 page 2
Three Key Factors for Risk Management bull Medical record must show standard of care for pressure ulcers was adhered to bull Medical record must have documentation of resident complications risk factors andor underlying disease
that made the pressure ulcer unavoidable (if it is indeed) bull You must provide a comprehensive and aggressive program to prevent and treat the pressure ulcer (within
the parameters of resident advance directives)
Prevention bull What systems are in place in your facility
ndash How is risk communicated to staff ndash Are there protocols for repositioning and pressure relief products that are understood by staff ndash How are you sure this is done for new admissions or those with change in status ndash Residents cannot afford to wait
bull How are moisturizersbarriers stocked bull During ldquooff-hoursrdquo do staff know how to access pressure-reducing devices bull Are tracking and assessment forms stocked bull How are disposable briefs and underpads stocked and used
Assessment
Avoidable vs Unavoidable Pressure Ulcers bull Avoidable ndash Pressure ulcer developed and facility failed to do one or more
▷ Definedimplemented interventions CONSISTENT with resident needs goals ▷ Recognized standards of practice (AHCPR AMDA WOCN current literature) ▷ Monitor and evaluate impact of interventions ▷ Revise interventions appropriately
bull Unavoidable ndash Resident developed pressure ulcer although facility ▷ Evaluated clinical condition and risk factors ▷ Defined and implemented interventions consistent with residentrsquos needs goals standards of practice ▷ Monitored and evaluated impact of interventions ▷ Revised approaches appropriately
Frequency of Risk Assessment (Braden or Norton most common) bull Minimally
▷ upon admission ▷ quarterly ▷ upon Significant Change in Condition
bull Best Practice ▷ day 7 14 21 28 (post-admission) then as above ▷ during acute illness
Understanding CMS Interpretation of F314 page 3
Wound Assessment bull Assessment includes a full description of the wound and peri-wound bull Measurements alone do not constitute an assessment bull Reassess weekly at a minimum bull Reassess daily if pressure ulcer is deteriorating
Staging Assessment bull Does your facility policy address your process for staging bull Who does initial staging How is it confirmed bull What are you staging All open areas or only pressure ulcers bull Is there a facility tool for documenting staging
Risk Assessment ndash Facility Wide bull Establish written guidelines protocols algorithmsdecision trees based on risk bull Low risk does not equal no risk bull Let low scores trigger your mind clinically donrsquot just treat the conglomerate of score bull Use appropriate interventions based on the risk assessment
Interventions
Address Risk Factors bull Skincare routine inspections cleansing moisturizing avoid massage bull Repositioning 1 hour in chair by staff 15 minutes in chair by resident 2 hours in bed bull Pressurerelief for heels bull Pressurereduction devices bull Addressnutrition
bull Addressincontinence bull Toileting schedule Rehab Positioning evaluations Incontinence products
Combination of Prevention Interventions bull Adequate nutrition and hydration bull Repositioning schedule and positioning bull Appropriate support surfaces bull Care of skin
Monitoring Wound Status
Is It Better or Worse bull Objectively review wound progress measurements type of tissue PUSH tool bull Subjective assessments are problematic
ndash ldquoI donrsquot think this treatment is working Irsquom calling the MD to change the treatmenthelliprdquo ndash ldquoThe pressure ulcer is deeper than last week - of course it is worserdquo - not necessarily true
Understanding CMS Interpretation of F314 page 4
Monitoring Treatment Plan bull Is there a process for monitoring treatment bull Is there a tracking tool to document response to treatment bull Does the tracking form monitor the appropriate wound variables bull Are there protocols for changing the treatment if it is ineffective bull Healing - a systemic process affected by systemic conditions - treatment is more than a dressing bull When do you change the treatment bull What determines frequency of dsg change bull How do you handle ldquonon-traditionalrdquo recommendations or a product being used in a manner different than
its intended use
Care Planning bull Do care plans identify risk factors bull Are you treating the risk factors bull Is the resident and family aware of and in agreement with goals bull Goal must be a clear statement of intended progress and how it will be measured bull Be REALISTIC bull Determine what the goal is
ndash Maintenance ndash ImprovementHealing ndash Comfort ndash Many goals beyond healinghellip
▷ Resolution of periwound erythema in 2 weeks ▷ 25 reduction in amount of necrotic tissue by 1 week ▷ Decrease in intensity of pain during dressing changes from 6 to 3 (as reported by resident) by 1 week ▷ 1 cm reduction in wound dimensions by 2 weeks
Document available at wwwprimarisorg MO-08-11-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from CMS Provider Certification Transmittal 4 November 12 2004 HCPro Pressure Ulcer Materials 2004 amp Pressure Ulcers F-314 by Courtney Lyder September 2004
MDS Skin Condition Coding Tip Sheet
Definition According the RAI Manual ldquoA skin ulcer can be defined as a local loss of epidermis and variable levels of dermis and subcutaneous tissue or in the case of Stage 1 pressure ulcers persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relievedrdquo (RAI Manual pgs 3-159)
CodingM1 - recording of all skin ulcers if caused by pressure or circulatory problems 1 M1 - recording of all skin ulcers if caused by pressure or 4 M4 - records skin problems or lesions not caused by
circulatory problems pressure or circulatory problems 2 M2 - differentiates between pressure or venous stasis 5 M5 - records any specific or generic skin treatments
ulcers only record highest level of each 6 M6 - records specific foot problems and care 3 M3 - history of resolvedcured ulcers Definition same as for M1
Process 1 Review the record and check with appropriate nursing
staff for the presence of any skin problems 2 Examine the resident for condition (stage number) of
any skin problems Coding will be based on what is seen (ie visible tissue) during the look back period NPUAP standards cannot be used for coding on the MDS MDS defined staging is used for M1 and M2 only
3 Determine the cause of the skin ulcer If it is caused from pressure or circulation (venous or arterial) then it is coded in M1 All remaining skin ulcers then are documented in
M4 (See pg 3-159) Record the number of skin ulcers caused by either pressure or circulatory problems according to stage for M1 M2 is for coding the highest stage of pressure or venous stasis ulcers only
4 Include in M4 all skin problems not caused by pressure venous stasis circulatory problems or not coded anywhere else in Section M
5 Code all skin treatments in M5 6 Code all foot problems and care in M6
Clarification 1 Necrotic eschar prohibits accurate staging Code the skin
ulcer with eschar as Stage 4 until debrided 2 Good clinical practice dictates that the ulcer be reshy
examined and re-staged after debridement 3 If a skin ulcer is repaired with a flap graft it is coded as a
surgical wound and not as a skin ulcer
4 Skin ulcers should be coded in either M1 with further clarification in M2 or in M4 Pressure or stasis ulcers coded in M2 should not be coded in M4
5 If skin ulcers are captured in M1 or M4 good clinical practice would also have something documented in M5 under treatment
6 For MDs coding ankle problems are not considered foot problems
Documentation 1 For clinical practice facilities need to follow the NPUAP
standards in regards to pressure ulcer documentation (ie Healing stage 4 that has the appearance of tissue size and depth of a stage 2- the clinical record will state a healing stage 4 but the MDS would have Stage 2 in M1)
2 Document weekly assessments of the wound healing progress or lack of Documentation should include a thorough description of size drainage etc
3 Care planning should identify risk factors and interventions based on the identified level of risk as well as interventions to facilitate healing of existing skin problems
Example 1 Mrs B has impaired arterial circulation to her right foot She has a Stage 3 in appearance on the top of her foot She also has a
superficial skin tear on her right forearm M1 would be coded as a Stage 3 ulcer M2 would be coded with 0 (zeros) and M4a would be checked for the skin tear M5d e and g may be checked depending on specified interventions M6c would be checked
Document available at wwwprimarisorg MO-08-47-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Understanding CMS Interpretation of F314 page 2
Three Key Factors for Risk Management bull Medical record must show standard of care for pressure ulcers was adhered to bull Medical record must have documentation of resident complications risk factors andor underlying disease
that made the pressure ulcer unavoidable (if it is indeed) bull You must provide a comprehensive and aggressive program to prevent and treat the pressure ulcer (within
the parameters of resident advance directives)
Prevention bull What systems are in place in your facility
ndash How is risk communicated to staff ndash Are there protocols for repositioning and pressure relief products that are understood by staff ndash How are you sure this is done for new admissions or those with change in status ndash Residents cannot afford to wait
bull How are moisturizersbarriers stocked bull During ldquooff-hoursrdquo do staff know how to access pressure-reducing devices bull Are tracking and assessment forms stocked bull How are disposable briefs and underpads stocked and used
Assessment
Avoidable vs Unavoidable Pressure Ulcers bull Avoidable ndash Pressure ulcer developed and facility failed to do one or more
▷ Definedimplemented interventions CONSISTENT with resident needs goals ▷ Recognized standards of practice (AHCPR AMDA WOCN current literature) ▷ Monitor and evaluate impact of interventions ▷ Revise interventions appropriately
bull Unavoidable ndash Resident developed pressure ulcer although facility ▷ Evaluated clinical condition and risk factors ▷ Defined and implemented interventions consistent with residentrsquos needs goals standards of practice ▷ Monitored and evaluated impact of interventions ▷ Revised approaches appropriately
Frequency of Risk Assessment (Braden or Norton most common) bull Minimally
▷ upon admission ▷ quarterly ▷ upon Significant Change in Condition
bull Best Practice ▷ day 7 14 21 28 (post-admission) then as above ▷ during acute illness
Understanding CMS Interpretation of F314 page 3
Wound Assessment bull Assessment includes a full description of the wound and peri-wound bull Measurements alone do not constitute an assessment bull Reassess weekly at a minimum bull Reassess daily if pressure ulcer is deteriorating
Staging Assessment bull Does your facility policy address your process for staging bull Who does initial staging How is it confirmed bull What are you staging All open areas or only pressure ulcers bull Is there a facility tool for documenting staging
Risk Assessment ndash Facility Wide bull Establish written guidelines protocols algorithmsdecision trees based on risk bull Low risk does not equal no risk bull Let low scores trigger your mind clinically donrsquot just treat the conglomerate of score bull Use appropriate interventions based on the risk assessment
Interventions
Address Risk Factors bull Skincare routine inspections cleansing moisturizing avoid massage bull Repositioning 1 hour in chair by staff 15 minutes in chair by resident 2 hours in bed bull Pressurerelief for heels bull Pressurereduction devices bull Addressnutrition
bull Addressincontinence bull Toileting schedule Rehab Positioning evaluations Incontinence products
Combination of Prevention Interventions bull Adequate nutrition and hydration bull Repositioning schedule and positioning bull Appropriate support surfaces bull Care of skin
Monitoring Wound Status
Is It Better or Worse bull Objectively review wound progress measurements type of tissue PUSH tool bull Subjective assessments are problematic
ndash ldquoI donrsquot think this treatment is working Irsquom calling the MD to change the treatmenthelliprdquo ndash ldquoThe pressure ulcer is deeper than last week - of course it is worserdquo - not necessarily true
Understanding CMS Interpretation of F314 page 4
Monitoring Treatment Plan bull Is there a process for monitoring treatment bull Is there a tracking tool to document response to treatment bull Does the tracking form monitor the appropriate wound variables bull Are there protocols for changing the treatment if it is ineffective bull Healing - a systemic process affected by systemic conditions - treatment is more than a dressing bull When do you change the treatment bull What determines frequency of dsg change bull How do you handle ldquonon-traditionalrdquo recommendations or a product being used in a manner different than
its intended use
Care Planning bull Do care plans identify risk factors bull Are you treating the risk factors bull Is the resident and family aware of and in agreement with goals bull Goal must be a clear statement of intended progress and how it will be measured bull Be REALISTIC bull Determine what the goal is
ndash Maintenance ndash ImprovementHealing ndash Comfort ndash Many goals beyond healinghellip
▷ Resolution of periwound erythema in 2 weeks ▷ 25 reduction in amount of necrotic tissue by 1 week ▷ Decrease in intensity of pain during dressing changes from 6 to 3 (as reported by resident) by 1 week ▷ 1 cm reduction in wound dimensions by 2 weeks
Document available at wwwprimarisorg MO-08-11-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from CMS Provider Certification Transmittal 4 November 12 2004 HCPro Pressure Ulcer Materials 2004 amp Pressure Ulcers F-314 by Courtney Lyder September 2004
MDS Skin Condition Coding Tip Sheet
Definition According the RAI Manual ldquoA skin ulcer can be defined as a local loss of epidermis and variable levels of dermis and subcutaneous tissue or in the case of Stage 1 pressure ulcers persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relievedrdquo (RAI Manual pgs 3-159)
CodingM1 - recording of all skin ulcers if caused by pressure or circulatory problems 1 M1 - recording of all skin ulcers if caused by pressure or 4 M4 - records skin problems or lesions not caused by
circulatory problems pressure or circulatory problems 2 M2 - differentiates between pressure or venous stasis 5 M5 - records any specific or generic skin treatments
ulcers only record highest level of each 6 M6 - records specific foot problems and care 3 M3 - history of resolvedcured ulcers Definition same as for M1
Process 1 Review the record and check with appropriate nursing
staff for the presence of any skin problems 2 Examine the resident for condition (stage number) of
any skin problems Coding will be based on what is seen (ie visible tissue) during the look back period NPUAP standards cannot be used for coding on the MDS MDS defined staging is used for M1 and M2 only
3 Determine the cause of the skin ulcer If it is caused from pressure or circulation (venous or arterial) then it is coded in M1 All remaining skin ulcers then are documented in
M4 (See pg 3-159) Record the number of skin ulcers caused by either pressure or circulatory problems according to stage for M1 M2 is for coding the highest stage of pressure or venous stasis ulcers only
4 Include in M4 all skin problems not caused by pressure venous stasis circulatory problems or not coded anywhere else in Section M
5 Code all skin treatments in M5 6 Code all foot problems and care in M6
Clarification 1 Necrotic eschar prohibits accurate staging Code the skin
ulcer with eschar as Stage 4 until debrided 2 Good clinical practice dictates that the ulcer be reshy
examined and re-staged after debridement 3 If a skin ulcer is repaired with a flap graft it is coded as a
surgical wound and not as a skin ulcer
4 Skin ulcers should be coded in either M1 with further clarification in M2 or in M4 Pressure or stasis ulcers coded in M2 should not be coded in M4
5 If skin ulcers are captured in M1 or M4 good clinical practice would also have something documented in M5 under treatment
6 For MDs coding ankle problems are not considered foot problems
Documentation 1 For clinical practice facilities need to follow the NPUAP
standards in regards to pressure ulcer documentation (ie Healing stage 4 that has the appearance of tissue size and depth of a stage 2- the clinical record will state a healing stage 4 but the MDS would have Stage 2 in M1)
2 Document weekly assessments of the wound healing progress or lack of Documentation should include a thorough description of size drainage etc
3 Care planning should identify risk factors and interventions based on the identified level of risk as well as interventions to facilitate healing of existing skin problems
Example 1 Mrs B has impaired arterial circulation to her right foot She has a Stage 3 in appearance on the top of her foot She also has a
superficial skin tear on her right forearm M1 would be coded as a Stage 3 ulcer M2 would be coded with 0 (zeros) and M4a would be checked for the skin tear M5d e and g may be checked depending on specified interventions M6c would be checked
Document available at wwwprimarisorg MO-08-47-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Understanding CMS Interpretation of F314 page 3
Wound Assessment bull Assessment includes a full description of the wound and peri-wound bull Measurements alone do not constitute an assessment bull Reassess weekly at a minimum bull Reassess daily if pressure ulcer is deteriorating
Staging Assessment bull Does your facility policy address your process for staging bull Who does initial staging How is it confirmed bull What are you staging All open areas or only pressure ulcers bull Is there a facility tool for documenting staging
Risk Assessment ndash Facility Wide bull Establish written guidelines protocols algorithmsdecision trees based on risk bull Low risk does not equal no risk bull Let low scores trigger your mind clinically donrsquot just treat the conglomerate of score bull Use appropriate interventions based on the risk assessment
Interventions
Address Risk Factors bull Skincare routine inspections cleansing moisturizing avoid massage bull Repositioning 1 hour in chair by staff 15 minutes in chair by resident 2 hours in bed bull Pressurerelief for heels bull Pressurereduction devices bull Addressnutrition
bull Addressincontinence bull Toileting schedule Rehab Positioning evaluations Incontinence products
Combination of Prevention Interventions bull Adequate nutrition and hydration bull Repositioning schedule and positioning bull Appropriate support surfaces bull Care of skin
Monitoring Wound Status
Is It Better or Worse bull Objectively review wound progress measurements type of tissue PUSH tool bull Subjective assessments are problematic
ndash ldquoI donrsquot think this treatment is working Irsquom calling the MD to change the treatmenthelliprdquo ndash ldquoThe pressure ulcer is deeper than last week - of course it is worserdquo - not necessarily true
Understanding CMS Interpretation of F314 page 4
Monitoring Treatment Plan bull Is there a process for monitoring treatment bull Is there a tracking tool to document response to treatment bull Does the tracking form monitor the appropriate wound variables bull Are there protocols for changing the treatment if it is ineffective bull Healing - a systemic process affected by systemic conditions - treatment is more than a dressing bull When do you change the treatment bull What determines frequency of dsg change bull How do you handle ldquonon-traditionalrdquo recommendations or a product being used in a manner different than
its intended use
Care Planning bull Do care plans identify risk factors bull Are you treating the risk factors bull Is the resident and family aware of and in agreement with goals bull Goal must be a clear statement of intended progress and how it will be measured bull Be REALISTIC bull Determine what the goal is
ndash Maintenance ndash ImprovementHealing ndash Comfort ndash Many goals beyond healinghellip
▷ Resolution of periwound erythema in 2 weeks ▷ 25 reduction in amount of necrotic tissue by 1 week ▷ Decrease in intensity of pain during dressing changes from 6 to 3 (as reported by resident) by 1 week ▷ 1 cm reduction in wound dimensions by 2 weeks
Document available at wwwprimarisorg MO-08-11-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from CMS Provider Certification Transmittal 4 November 12 2004 HCPro Pressure Ulcer Materials 2004 amp Pressure Ulcers F-314 by Courtney Lyder September 2004
MDS Skin Condition Coding Tip Sheet
Definition According the RAI Manual ldquoA skin ulcer can be defined as a local loss of epidermis and variable levels of dermis and subcutaneous tissue or in the case of Stage 1 pressure ulcers persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relievedrdquo (RAI Manual pgs 3-159)
CodingM1 - recording of all skin ulcers if caused by pressure or circulatory problems 1 M1 - recording of all skin ulcers if caused by pressure or 4 M4 - records skin problems or lesions not caused by
circulatory problems pressure or circulatory problems 2 M2 - differentiates between pressure or venous stasis 5 M5 - records any specific or generic skin treatments
ulcers only record highest level of each 6 M6 - records specific foot problems and care 3 M3 - history of resolvedcured ulcers Definition same as for M1
Process 1 Review the record and check with appropriate nursing
staff for the presence of any skin problems 2 Examine the resident for condition (stage number) of
any skin problems Coding will be based on what is seen (ie visible tissue) during the look back period NPUAP standards cannot be used for coding on the MDS MDS defined staging is used for M1 and M2 only
3 Determine the cause of the skin ulcer If it is caused from pressure or circulation (venous or arterial) then it is coded in M1 All remaining skin ulcers then are documented in
M4 (See pg 3-159) Record the number of skin ulcers caused by either pressure or circulatory problems according to stage for M1 M2 is for coding the highest stage of pressure or venous stasis ulcers only
4 Include in M4 all skin problems not caused by pressure venous stasis circulatory problems or not coded anywhere else in Section M
5 Code all skin treatments in M5 6 Code all foot problems and care in M6
Clarification 1 Necrotic eschar prohibits accurate staging Code the skin
ulcer with eschar as Stage 4 until debrided 2 Good clinical practice dictates that the ulcer be reshy
examined and re-staged after debridement 3 If a skin ulcer is repaired with a flap graft it is coded as a
surgical wound and not as a skin ulcer
4 Skin ulcers should be coded in either M1 with further clarification in M2 or in M4 Pressure or stasis ulcers coded in M2 should not be coded in M4
5 If skin ulcers are captured in M1 or M4 good clinical practice would also have something documented in M5 under treatment
6 For MDs coding ankle problems are not considered foot problems
Documentation 1 For clinical practice facilities need to follow the NPUAP
standards in regards to pressure ulcer documentation (ie Healing stage 4 that has the appearance of tissue size and depth of a stage 2- the clinical record will state a healing stage 4 but the MDS would have Stage 2 in M1)
2 Document weekly assessments of the wound healing progress or lack of Documentation should include a thorough description of size drainage etc
3 Care planning should identify risk factors and interventions based on the identified level of risk as well as interventions to facilitate healing of existing skin problems
Example 1 Mrs B has impaired arterial circulation to her right foot She has a Stage 3 in appearance on the top of her foot She also has a
superficial skin tear on her right forearm M1 would be coded as a Stage 3 ulcer M2 would be coded with 0 (zeros) and M4a would be checked for the skin tear M5d e and g may be checked depending on specified interventions M6c would be checked
Document available at wwwprimarisorg MO-08-47-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Understanding CMS Interpretation of F314 page 4
Monitoring Treatment Plan bull Is there a process for monitoring treatment bull Is there a tracking tool to document response to treatment bull Does the tracking form monitor the appropriate wound variables bull Are there protocols for changing the treatment if it is ineffective bull Healing - a systemic process affected by systemic conditions - treatment is more than a dressing bull When do you change the treatment bull What determines frequency of dsg change bull How do you handle ldquonon-traditionalrdquo recommendations or a product being used in a manner different than
its intended use
Care Planning bull Do care plans identify risk factors bull Are you treating the risk factors bull Is the resident and family aware of and in agreement with goals bull Goal must be a clear statement of intended progress and how it will be measured bull Be REALISTIC bull Determine what the goal is
ndash Maintenance ndash ImprovementHealing ndash Comfort ndash Many goals beyond healinghellip
▷ Resolution of periwound erythema in 2 weeks ▷ 25 reduction in amount of necrotic tissue by 1 week ▷ Decrease in intensity of pain during dressing changes from 6 to 3 (as reported by resident) by 1 week ▷ 1 cm reduction in wound dimensions by 2 weeks
Document available at wwwprimarisorg MO-08-11-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from CMS Provider Certification Transmittal 4 November 12 2004 HCPro Pressure Ulcer Materials 2004 amp Pressure Ulcers F-314 by Courtney Lyder September 2004
MDS Skin Condition Coding Tip Sheet
Definition According the RAI Manual ldquoA skin ulcer can be defined as a local loss of epidermis and variable levels of dermis and subcutaneous tissue or in the case of Stage 1 pressure ulcers persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relievedrdquo (RAI Manual pgs 3-159)
CodingM1 - recording of all skin ulcers if caused by pressure or circulatory problems 1 M1 - recording of all skin ulcers if caused by pressure or 4 M4 - records skin problems or lesions not caused by
circulatory problems pressure or circulatory problems 2 M2 - differentiates between pressure or venous stasis 5 M5 - records any specific or generic skin treatments
ulcers only record highest level of each 6 M6 - records specific foot problems and care 3 M3 - history of resolvedcured ulcers Definition same as for M1
Process 1 Review the record and check with appropriate nursing
staff for the presence of any skin problems 2 Examine the resident for condition (stage number) of
any skin problems Coding will be based on what is seen (ie visible tissue) during the look back period NPUAP standards cannot be used for coding on the MDS MDS defined staging is used for M1 and M2 only
3 Determine the cause of the skin ulcer If it is caused from pressure or circulation (venous or arterial) then it is coded in M1 All remaining skin ulcers then are documented in
M4 (See pg 3-159) Record the number of skin ulcers caused by either pressure or circulatory problems according to stage for M1 M2 is for coding the highest stage of pressure or venous stasis ulcers only
4 Include in M4 all skin problems not caused by pressure venous stasis circulatory problems or not coded anywhere else in Section M
5 Code all skin treatments in M5 6 Code all foot problems and care in M6
Clarification 1 Necrotic eschar prohibits accurate staging Code the skin
ulcer with eschar as Stage 4 until debrided 2 Good clinical practice dictates that the ulcer be reshy
examined and re-staged after debridement 3 If a skin ulcer is repaired with a flap graft it is coded as a
surgical wound and not as a skin ulcer
4 Skin ulcers should be coded in either M1 with further clarification in M2 or in M4 Pressure or stasis ulcers coded in M2 should not be coded in M4
5 If skin ulcers are captured in M1 or M4 good clinical practice would also have something documented in M5 under treatment
6 For MDs coding ankle problems are not considered foot problems
Documentation 1 For clinical practice facilities need to follow the NPUAP
standards in regards to pressure ulcer documentation (ie Healing stage 4 that has the appearance of tissue size and depth of a stage 2- the clinical record will state a healing stage 4 but the MDS would have Stage 2 in M1)
2 Document weekly assessments of the wound healing progress or lack of Documentation should include a thorough description of size drainage etc
3 Care planning should identify risk factors and interventions based on the identified level of risk as well as interventions to facilitate healing of existing skin problems
Example 1 Mrs B has impaired arterial circulation to her right foot She has a Stage 3 in appearance on the top of her foot She also has a
superficial skin tear on her right forearm M1 would be coded as a Stage 3 ulcer M2 would be coded with 0 (zeros) and M4a would be checked for the skin tear M5d e and g may be checked depending on specified interventions M6c would be checked
Document available at wwwprimarisorg MO-08-47-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

MDS Skin Condition Coding Tip Sheet
Definition According the RAI Manual ldquoA skin ulcer can be defined as a local loss of epidermis and variable levels of dermis and subcutaneous tissue or in the case of Stage 1 pressure ulcers persistent area of skin redness (without a break in the skin) that does not disappear when pressure is relievedrdquo (RAI Manual pgs 3-159)
CodingM1 - recording of all skin ulcers if caused by pressure or circulatory problems 1 M1 - recording of all skin ulcers if caused by pressure or 4 M4 - records skin problems or lesions not caused by
circulatory problems pressure or circulatory problems 2 M2 - differentiates between pressure or venous stasis 5 M5 - records any specific or generic skin treatments
ulcers only record highest level of each 6 M6 - records specific foot problems and care 3 M3 - history of resolvedcured ulcers Definition same as for M1
Process 1 Review the record and check with appropriate nursing
staff for the presence of any skin problems 2 Examine the resident for condition (stage number) of
any skin problems Coding will be based on what is seen (ie visible tissue) during the look back period NPUAP standards cannot be used for coding on the MDS MDS defined staging is used for M1 and M2 only
3 Determine the cause of the skin ulcer If it is caused from pressure or circulation (venous or arterial) then it is coded in M1 All remaining skin ulcers then are documented in
M4 (See pg 3-159) Record the number of skin ulcers caused by either pressure or circulatory problems according to stage for M1 M2 is for coding the highest stage of pressure or venous stasis ulcers only
4 Include in M4 all skin problems not caused by pressure venous stasis circulatory problems or not coded anywhere else in Section M
5 Code all skin treatments in M5 6 Code all foot problems and care in M6
Clarification 1 Necrotic eschar prohibits accurate staging Code the skin
ulcer with eschar as Stage 4 until debrided 2 Good clinical practice dictates that the ulcer be reshy
examined and re-staged after debridement 3 If a skin ulcer is repaired with a flap graft it is coded as a
surgical wound and not as a skin ulcer
4 Skin ulcers should be coded in either M1 with further clarification in M2 or in M4 Pressure or stasis ulcers coded in M2 should not be coded in M4
5 If skin ulcers are captured in M1 or M4 good clinical practice would also have something documented in M5 under treatment
6 For MDs coding ankle problems are not considered foot problems
Documentation 1 For clinical practice facilities need to follow the NPUAP
standards in regards to pressure ulcer documentation (ie Healing stage 4 that has the appearance of tissue size and depth of a stage 2- the clinical record will state a healing stage 4 but the MDS would have Stage 2 in M1)
2 Document weekly assessments of the wound healing progress or lack of Documentation should include a thorough description of size drainage etc
3 Care planning should identify risk factors and interventions based on the identified level of risk as well as interventions to facilitate healing of existing skin problems
Example 1 Mrs B has impaired arterial circulation to her right foot She has a Stage 3 in appearance on the top of her foot She also has a
superficial skin tear on her right forearm M1 would be coded as a Stage 3 ulcer M2 would be coded with 0 (zeros) and M4a would be checked for the skin tear M5d e and g may be checked depending on specified interventions M6c would be checked
Document available at wwwprimarisorg MO-08-47-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Facility Assessment Checklists
A facility system assessment is a starting point for a quality improvement project The checklists included in this booklet will be most useful if you take a critical look at your current practices
Directions for Pressure Ulcers Facility Assessment Overview Questionnaire bull Tobecompletedbyadirectcareorinterdisciplinaryteam bull Consultwithappropriatestaffinansweringcertainquestionsandcompletingchecklists bull IfyouanswerldquoNordquotoanyofthequestionsbelowpleaseproceedimmediatelytothechecklist
referencedbythepageafterthequestion bull IfyouanswerldquoYesrdquotoaquestiontheprocessisalwayscompleteanddonesoconsistentlyPlease
continuetothenextquestion bull IfyouanswerldquoInProgressrdquotoanyofthebelowquestionstheneedisbeingaddressedbutneedsimprovement
Pressure Ulcers Facility Assessment Yes No In Progress
Does your facility have a process to screen residents for pressure ulcer risk (page 2) o o o Does your facility have a process to develop and implement care plans for residents who have been found to be at risk or have a pressure ulcer (pages 3-4)
o o o
Does your facility complete a comprehensive assessment for residents who are found to have pressure ulcers upon screening or if there is no screening process in place another time (page 5)
o o o
For residents who have pressure ulcers does your facility have a process for monitoring treatment and prevention (page 6) o o o
Does your facility have a policy for pressure ulcer prevention and management (page 7) o o o
Does your facility have initial and ongoing education on pressure ulcer prevention and management for all relevant staff (page 8) o o o
When completing each checklist on the following pages bull IfyouanswerldquoYesrdquotoallofthequestionstheprocessisalwayscompleteanddonesoconsistently
Continuetothenextchecklist bull IfyouarenotsureoranswerldquoNordquotooneofthequestionschooseoneormoreelementsonwhichtofocus
yourqualityimprovement bull IfyouanswerldquoNeedsImprovementrdquotooneormoreofthequestionstheprocessisnotalwayscomplete
andornotalwaysdoneconsistently
Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Facility Assessment Checklists page 2
Pressure Ulcers Screening for Pressure Ulcer Risk Ascreeningassessmentisabriefassessmentorquestionthatdeterminesiftheresidentisatriskforpressure ulcersItdoesnotincludeathoroughassessmentofthepressureulcerorwhatneedstobedoneiftheresidentis foundtohaveapressureulceruponscreening
Does your facilityrsquos screening process include the following components Needs
Yes No Improvement Do you screen all residents for pressure ulcer risk at the following times
Upon admission o o o Upon readmission o o o When change in condition o o o With each MDS assessment o o o
If resident is not currently deemed at risk is there a plan to rescreen at regular intervals o o o Do you use either the Norton or Braden pressure ulcer risk assessment tool (If yes STOP If No please continue to next question) Note Federal regulations (F-314) recommend the use of standardized risk assessment tools
o o o
If you are not using the Norton or Braden risk assessment does your screening address the following areas Impaired mobility
Bed o o o
Chair o o o Incontinence
Urine o o o
Stool o o o Nutritional deficits
Malnutrition o o o Feeding difficulties o o o
Diagnosis of Diabetes mellitus o o o Peripheral vascular disease o o o
Contractures o o o Hx of pressure ulcers o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Facility Assessment Checklists page 3
Pressure Ulcers Developing Care Plans
Does the resident care plan address the following interventions and risk factors (as they apply) Needs
Yes No Improvement Impaired mobility
Assist with turning rising position o o o Encourage ambulation o o o Limit static sitting to 1 hour at any one time o o o
Pressure relief Support surfaces ndash bed o o o Support surfaces ndash chair o o o Pressure relieving devices o o o Repositioning o o o Check for ldquobottoming outrdquo in bed and chair (To determine if a patient has bottomed out the caregiver should place his or her outstretched hand palm-up under the mattress overlay below the existing pressure ulcer or that part of the body at risk for pressure o o o formation If the caregiver can feel that the support material is less than an inch thick at this site the patient has bottomed out)
Nutritional improvement Supplements o o o Feeding assistance o o o Adequate fluid intake o o o Dietician consult as needed o o o
Urinary incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Wet checks o o o Treat causes o o o Assist with hygiene o o o
Fecal incontinence Cause identified and treated as appropriate o o o Toileting plan o o o Soiled checks o o o
Skin condition check Check intactness o o o Color o o o Sensation o o o Temperature o o o
continued on next page gt
Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Facility Assessment Checklists page 4
Pressure Ulcers Developing Care Plans
Needs Yes No Improvement
Treatment Physician prescribed regimen o o o Appropriateness to wound staging o o o Treatment reassessment time frame o o o
Pain Screen for pain related to ulcer o o o Choose appropriate pain med o o o Provide regular pain med administration o o o Reassess effectiveness of med o o o Assesstreat side effects o o o Change increase or decease pain med as needed o o o
Infection Dressing containment o o o Keep dressing dryintact o o o Assess for ssx infection o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Facility Assessment Checklists page 5
Pressure Ulcers Assessment and Reassessment
Does your comprehensive pressure ulcer assessment include the following components
Needs Yes No Improvement
Do you have a tool available to document pressure ulcer assessment o o o Does your current assessment of pressure ulcers include
Location o o o Stage o o o Size o o o Underminingtunneling o o o Wound bed (tissue) o o o Drainageexudate o o o Peri wound tissue (color temp bogginess and fluctuation) o o o Need for debridement o o o
Is the residentrsquos pressure ulcer reassessed
Weekly o o o Daily if worsening or high risk o o o
Does reassessment include
Size o o o Tunneling o o o Sinus tracts o o o Presence of necrotic tissue o o o Exudate o o o Granulation o o o Epithelialization o o o Color photos diagram or drawing o o o
Are the following related factors considered in your assessmentreassessment
Mechanical forces (shearing friction pressure) o o o Pronounced bony prominences o o o Poor nutrition o o o Altered cutaneous sensation o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Facility Assessment Checklists page 6
Pressure Ulcers Monitoring Treatment and Prevention
Does your facilityrsquos process for monitoring treatment and prevention include the following Needs
Yes No Improvement Does your facility use a pressure ulcer tracking tool to document treatment and healing (If ldquoNordquo skip to question 3) o o o Does the tracking form include the following
Date
Stage
Current treatment
Color photo diagram or drawing
Size
Depth
Appearance (eg redness presence of discharge eschar formation)
o o o o o o o
o o o o o o o
o o o o o o o
Does your facility have protocols to follow if current pressure ulcer treatment is ineffective o o o Does your facility have protocols to follow if ulcers are found to be non-healing o o o Does your facility monitor pressure ulcers for the presence of infection (eg foul smell greenish drainage cellulitis osteomyelitis) o o o Is there a list of possible interventions for the resident at each level of risk (low moderate or high) that nursing staff may implement to prevent pressure ulcer development o o o Does your facility have a protocol for management of tissue loads (eg positioning pressure relieving mattresses dynamic mattress overlay) o o o Are there adequate supplies to provide preventive interventions to all residents who require them (eg adequate pressure reducing or relieving mattresseschair cushions) o o o Are pressure reducing or pressure relieving mattresseschair cushions in good repair o o o Are pressure reducingrelieving supplies available to staff on all shifts and whenever needed o o o Does your facility have protocols regarding pressure ulcer prevention that includes the following
Monitoring residents for incontinence o o o Need for assistance with mobility and bed mobility o o o Weight loss o o o Nutritional deficiency o o o Dehydration o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Facility Assessment Checklists page 7
Pressure Ulcers Elimination
Does the pressure ulcer elimination process include the following components Needs
Yes No Improvement Does your facilityrsquos policy include a statement regarding your facilityrsquos commitment to pressure ulcer prevention and management o o o
Does your facilityrsquos policy include screening assessment and monitoring of residents for pressure ulcers o o o
Does your facilityrsquos policy address measures that should be taken to prevent pressure ulcers in residents o o o
If the resident is not currently deemed at risk does your facilityrsquos policy state that residents should be screened for pressure ulcer risk at regular intervals o
Does your facilityrsquos policy state that residents who are at risk for pressure ulcers be screened at the following times
Upon admission o Upon readmission o When a change in condition occurs o With each MDS assessment o
o
o o o o
o
o o o o
Does your facilityrsquos policy state that residents at high risk for pressure ulcers should be screened daily o
Does your facilityrsquos policy include who how and when pressure ulcer program effectiveness should be monitored and evaluated
Prompt assessment and treatment o Specification of appropriate pressure ulcer risk and monitoring tools o Steps to be taken to monitor treatment effectiveness o Pressure ulcer treatment techniques that are consistent with clinically-based guidelines o Optimize the residentrsquos ability to perform ADLs and participate in activities o
o
o o o o o
o
o o o o o
Does your facilityrsquos policy address steps to be taken if pressure ulcer is not healing o o o Does your facilityrsquos policy address a protocol for communication of reporting pressure ulcer staginghealing to the designated MDS personnel to ensure correct coding o o o
Completedby_______________________________________ Date______________________________
Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Facility Assessment Checklists page 8
Pressure Ulcers Staff Training and Education
Does your facilityrsquos training and education program include the following components Needs
Yes No Improvement Are new staff assessed for their need for education on pressure ulcer prevention and management o o o
Are current staff provided with ongoing education on the principles of pressure ulcer prevention and management o o o
Does education staff provide discipline-specific education for pressure ulcer prevention and management o o o
Is there a designated clinical ldquoexpertrdquo available at the facility to answer questions from all staff about pressure ulcer prevention and management o o o
Is the education provided at the appropriate level for the learner (eg CNA vs RN) o o o Does the education include staff training on documentation methods related to pressure ulcers (eg location stage size depth appearance exudate current treatment effect on o o o ADLrsquos pressure relieving devices used nutritional support)
Completedby_______________________________________ Date______________________________
Document available at wwwprimarisorg MO-08-16-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Sample Protocol
Implement a protocol and accompanying strategies such as those below to help guide the care of residents at risk for developing pressure ulcers
At Risk Moderate Risk
High Risk Very High Risk
Systematic skin inspection bullbullbullbull bull bull bull
Turnreposition every 2 hours (if mobility impaired) or more often if needed bullbullbullbull
Turnreposition every 2 hours and prevent direct contact between bony prominences
bull bull bull
Protect heels bullbullbullbull bull bull bull
If bedfast provide pressureshyreducing support surface bullbullbullbull bull bull bull If in wheelchair provide pressureshyreducing seat cushion bullbullbullbull bull bull bull If appropriate initiate remobilization program (therapy if appropriate ambulation standshypivot transfers restorative nursing etc)
bullbullbullbull bull bull bull
Manage moisture (from incontinence) bullbullbullbull bull bull bull
Manage nutrition bullbullbullbull bull bull bull
Reduce frictionshear bullbullbullbull bull bull bull
Provide wedgesrepositioning aids for 30 degree lateral positioning bull bull bull Supplement turning schedule with small position shifts (hourly) bull bull Obtain rehab assessment to
shy Determine need for pressure relief cushion
shy Assess correct seat height and wc positioning
bull bull
Consider a pressure relieving support surface or powered mattress overlay bullbullbullbullWritten plan of care
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbullStaff education
bullbullbullbull bullbullbullbull bullbullbullbull bullbullbullbull
Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Sample Protocol page 2
Sample risk reduction strategies Skin inspection All residents should be inspected at least daily This can be done with dressing
undressing toileting bathing perishycare etc Pay particular attention to bony prominences Minimize exposure to low humidity Moisturize dry skin
Turning and repositioning Keep bony prominences from direct contact using systematic turning and repositioning and positioning devices such as pillows or foam wedges Avoid positioning directly on the trochanter Determine tissue tolerance
Wheelchair Positioning OT evaluate for proper fit to wheelchair and appropriate pressure relieving device Reposition and off load eight hourly ndash stand if possible Try to use at least three different chair types daily to alter pressure points If residents are able teach or cue them to shift their own weight every hour Use a pressureshyreducing device such as those made of foam gel air or a combination of the two Do not use donutshytype devices
Heel Protection ndash Friction To prevent friction use ldquogripperrdquo socks sheepskin at foot of bed
transparent dressings or skin sealants protective dressings (such as hydrocolloids) moisturizers Heel Protection ndash Pressure Keep ALL weight off residentsrsquo heels Elevate lower extremities with
pillows lengthshywise under lower legs multishypodus boots heelshylift boots loosen bed linens at foot of bed foot cradle
Manage Incontinence Initiate bowelbladder program or scheduled toileting incontinent care every two hours incontinence barriers briefs absorbent underpads (made with materials that absorb moisture amp present a quick drying surface to the skin) fecal bag (if frequent stools) Avoid hot water and use a mild cleansing agent that minimizes irritation and dryness
Manage Nutrition Monitor for weight loss Assess for chewing or swallowing problems Provide a combination of dietician consults supplements vitamin supplements hydration feeding assistance adaptive equipment
Reduce frictionshear Draw sheet or lift pad for bed movement trapeze moisturize skin limit head of bed elevation to 30 degrees (and only as required) long sleeve garmentselbow protectors
careful cleansing during incontinencehygiene care gait belt transfers (as appropriate) mechanical lift
Pressure relieving mattressoverlay Pressure reducing mattress types include foam static air alternating air gel or water mattresses
Written plan of care Each residentrsquos care plan should be unique including specific turning andrepositioning plans Indentify and address each factor noted in the Risk Assessment
Staff Education Target prevention at all levels of health care from providers to residents and families Identify the role each plays in pressure ulcer prevention Implement a comprehensive pressure ulcer prevention program
References Agency for Health Care Policy and Research (1994) Treatment of Pressure Ulcers AHCPR Pub No 95shy0652 University of Iowa Nursing Interventions Research Center Prevention of Pressure Ulcers American Medical Directors Association Pressure Ulcers in the LongshyTerm Care Setting Clinical Practice Guideline Columbia MD AMDA
2008
Source QIPMO University of MOshyColumbia Sinclair School of Nursing April 2008
MOshy08shy14shyPU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for
Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS
Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Braden Scale for Predicting Pressure Sore Risk
Resident Name (Last First Middle) ___________________________________________________________
Room _________ Attending Physician_________________________Date of Assessment _____________
Assessment Date
Risk Factor ScoreDescription 1 2 3 4
Sensory Perception Ability to respond meaningfully to pressure-related discomfort
1 = Completely Limited 2 = Very Limited 3 = Slightly Limited 4 = No impairment
Moisture Degree to which skin is exposed to moisture
1 = Constantly Moist 2 = Often Moist 3 = Occasionally Moist 4 = Rarely Moist
Activity Degree of physical activity
1 = Bedfast 2 = Chairfast 3 = Walks Occasionally 4 = Walks Freqeuently
Mobility Ability to change and control body position
1 = Completely Immobile 2 = Very Limited 3 = Slightly Limited 4 = No Limitations
Nutrition Usual food intake pattern 1NPO Nothing by mouth 2IV Intravenously 3TPN Total parenteral nutrition
1 = Very Poor 2 = Probably Inadequate 3 = Adequate 4 = Excellent
Friction and Shear 1 = Problem 2 = Potential Problem 3 = No Apparent Problem
Total Score
High Risk Total score le 12 Moderate Risk Total score 13-14 Low Risk Total score 15-16 if under 75 years old or 15-18 if over 75 years old
For Detailed Descriptions see page 2
Assess Date Evaluator signaturetitle Assess Date Evaluator signaturetitle
1 3
2 4
NOTE This form is copyrighted Permission to reproduce this form may be obtained at no charge by accessing wwwbradenscalecomcopyrightasp
page 1 of 2
Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Braden Scale for Predicting Pressure Sore Risk page 2
Sensory Perception 1 = Completely Limited Unresponsive (does not moan flinch
or grasp) to painful stimuli due to diminished level of consciousness or sedation OR limited ability to feel pain over most of body
2 = Very Limited Responds only to painful stimuli Cannot communicate discomfort except by moaning or restlessness OR has a sensory impairment which limits the ability to feel pain or discomfort over frac12 of body
3 = Slightly Limited Responds to verbal commands but cannot always communicate discomfort or the need to be turned OR has some sensory impairment which limits ability to feel pain or discomfort in 1 or 2 extremities
4 = No impairment Responds to verbal commands Has no sensory deficit which would limit ability to feel or voice pain or discomfort
Moisture 1 = Constantly Moist Skin is kept moist almost constantly by
perspiration urine etc Dampness is detected every time patient is moved or turned
2 = Often Moist Skin is often but not always moist Linen must be changed at least once a shift
3 = Occasionally Moist Skin is occasionally moist requiring an extra linen change approximately once a day
4 = Rarely Moist Skin is usually dry linen only requires changing at routine intervals
Activity 1 = Bedfast Confined to bed 2 = Chairfast Ability to walk severely limited or nonexistent
Cannot bear own weight andor must be assisted into chair or wheelchair
3 = Walks Occasionally Walks occasionally during day but for very short distances with or without assistance Spends majority of each shift in bed or chair
4 = Walks Frequently Walks outside room at least twice a day and inside room at least once every 2 hours during waking hours
Mobility 1 = Completely Immobile Does not make even slight changes
in body or extremity position without assistance 2 = Very Limited Makes occasional slight changes in body
or extremity position but unable to make frequent or significant changes independently
3 = Slightly Limited Makes frequent though slight changes in body or extremity position independently
4 = No Limitations Makes major and frequent changes in position without assistance
Nutrition 1 = Very Poor Never eats a complete meal Rarely eats more
than frac12 of any food offered Eats 2 servings or less of protein (meat or dairy products) per day Takes fluids poorly Does not take a liquid dietary supplement OR is NPO1 andor maintained on clear liquids or IV2 for more than 5 days
2 = Probably Inadequate Rarely eats a complete meal and generally eats only about frac12 of any food offered Protein intake includes only 3 servings of meat or dairy products per day Occasionally will take a dietary supplement OR receives less than optimum amount of liquid diet or tube feeding
3 = Adequate Eats over half of most meals Eats a total of 4 servings of protein (meat dairy products) per day Occasionally will refuse a meal but will usually take a supplement if offered OR is on a tube feeding or TPN3 regimen which probably meets most of nutritional needs
4 = Excellent Eats most of every meal Never refuses a meal Usually eats a total of 4 or more servings of meat and dairy products Occasionally eats between meals Does not require supplementation
Friction and Shear 1 = Problem Requires moderate to maximum assistance in
moving Complete lifting without sliding against sheets is impossible Frequently slides down in bed or chair requiring frequent repositioning with maximum assistance Spasticity contractures or agitation leads to almost constant friction
2 = Potential Problem Moves feebly or requires minimum assistance During a move skin probably slides to some extent against sheets chair restraints or other devices Maintains relatively good position in chair or bed most of the time but occasionally slides down
3 = No Apparent Problem Moves in bed and in chair independently and has sufficient muscle strength to lift up completely during move Maintains good position in bed or chair at all times
Document available at wwwprimarisorg MO-08-12-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
copy Copyright Barbara Braden and Nancy Bergstrom 1988 Reprinted with permission
Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Skin Tear Risk Assessment
Resident ___________________________________________________________ Date_________________ This form should be completed in conjunction with the Skin Risk Assessment in accordance with facility policy (on admission readmission quarterly and with a significant change in condition) Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to three or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo
Skin Tear Risk Assessment Yes No Yes No Reduced mental status
Poor nutritional status
History of skin tears
Dehydration
Self-abusive behavior
Thin translucent skin
o o o
o
o o
o o o
o
o o
History of syncope or unsteady gait
History of aggressive behavior
Resistant to care
Bruises easily (If yes total number of bruises__________)
Skin Tear Prevention Protocol To Be Implemented
o o o
o
o
o o o
o
o
Skin Tear Prevention Protocol
When the Skin Tear Risk Assessment identifies that the resident is at risk for skin tears the nurse will review this protocol and indicated pertinent interventions on the treatment record The nurses on the unit not the treatment nurse manage this protocol which includes 1 Provide covering for legs such as long pants heavy stockings tube socks or stockinet 2 Provide covering for arms such as stockinet long sleeved shirts or gowns 3 Application of Kling for arms or legs ensuring no tape on skin 4 Send inappropriate clothing home with the family so that it is not put on the resident by mistake If the resident has no
family put the clothing in storage with the residentrsquos name on it 5 Re-evaluate the necessity of side rails and if still necessary pad the side rails on the bed Care plan for potential
isolation due to the use of padded side rails 6 Notify activities not to place the resident very close to another resident 7 Use two staff members for all care performed as appropriate 8 If the resident becomes combative or resists care stop the care and return after the resident calms down Try to identify
what triggered the behavior Adjust the care plan as necessary to include potential interventions 9 Provide lotion to the skin routinely 10 Assess the residentrsquos overall skin condition on a weekly basis ndash mark completion of this task on the treatment record 11 Maintain hydration for the resident 12 Examine equipment (eg wheelchair bed bedrails) for sharp edges that could potentially harm the resident Notify
maintenance if appropriate Consult therapy in assisting with appropriate padding when necessary 13 Notify Dietician to adjust diet as necessary
Nurse Signature _________________________________________ Date Protocol Initiated __________________
Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Skin Tear Risk Assessment page 2
Skin Tear Risk Assessment and Prevention ProtocolmdashAudit
Related Federal Standard ldquoQuality of Carerdquo Audit Objectives
To evaluate the application and use of the facilityrsquos skin tear risk assessment To evaluate the application and use of the facilityrsquos skin tear prevention protocol To identify that identified residents receive care based on the skin tear prevention protocol
Resident Sample All residents in the facility who have received a risk assessment and residents that have been identified to be at risk for developing skin tears
Audit Sample Size _____ residents that were assessed for skin tear risk _____ residents that were placed on the skin tear prevention protocol
Time Period of Evaluation ________________________________________________ through __________________
Commencement Date of Study _____________________Expected Completion Date of Study __________________
Criterion No Audit Criteria Exceptions Instructions for
Data Retrieval The Skin Care Risk Assessment is used to assess for risk of skin tear
1 a b
Upon admission Upon readmission None Skin Care Risk
Assessment c Each quarter d With a significant change in status
The Skin Tear Risk Assessment is complete a Resident name
2 b c
Total score is indicated Indication if Skin Tear Protocol is to be implemented None Skin Care Risk
Assessment d Date assessment completed e Nursersquos signature
If Prevention Protocol was indicated it was implemented a Interventions were identified on the protocol form
3 b c
Interventions were placed on treatment record Interventions were identified on care plan
Residents at risk for skin care
Skin Care Prevention Protocol
d Implementation date is indicated e Nursersquos signature is present
Document available at wwwprimarisorg MO-08-08-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

_________________________________________________________________________________________ _________________________________________________________________________________________
LTC Dehydration Risk Assessment
Resident Name____________________________________________________ Date __________________
Check all conditions that apply to this resident The greater the number of items checked the greater the risk for dehydration Initiate a plan of care if necessary based on your findings
Medical ConditionsHistory oDiabetes oCHF oCVA oDementia oDepression oMajor Psychiatric Disorder oRenal Disease ogt 4 Chronic Conditions
History of oRepeated infections oDehydration oMalnutrition oConstipation Current Status oAge ge 85 oFemale gender oLanguagespeech difficulties oCognitive Impairment oUnable to request fluids oUnaware of thirst
oRecent change in mental status oAny physical immobility oRecent change in ability to carry out ADLs oRestraints oFalling episodes oUrinary incontinence oDecreased urinary output oConstipation or diarrhea oCurrent fever andor infection oVomiting oRecent rapid weight loss (gt3 30 days) oDraining wound oLethargyweakness oIncreased combativenessconfusion oReadmission from gt 1 day hospital stay oLabStudies involving NPO or dyes
Medications oge 4 medications oDiuretics oLaxatives oSteroids oACE inhibitors oPsychotropicsantipsychotics oAntianxiolytics oTricyclic Antidepressants or Lithium Intake Ability Status oSwallowing difficulties oRefuses fluids oDislikes fluidsfoods offered oFluid restriction oRequires assistance to eatdrink oPoor eater (eats lt 50 of each meal) oHolds foodfluid in mouth oDrools oSpits out foodfluid oSpills fluids oTube fed oIV fluid therapy Laboratory Abnormalities
(or steady increase even if within normal range) oUrine Specific Gravity oUrine color dare yellow gt 4 oBUNCreatinine gt 201 -orshyo in BUN + stable Creatinine level
oSerum Sodium oSerum Osmolality oHematocrit gt normal oBMI lt 2 or gt 27 Knowledge Issues oLack of understanding about fluid needs oLack of understanding about causes of dehydration oCultural barriers about hydration reporting thirst end
of life issues Comments _______________________________________________________________________________
Nursersquos Signature__________________________________________________________________________
Document available at wwwprimarisorg MO-08-05-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
__________________________________________________________________________________________________
Comprehensive Admission Skin Assessment
Resident _______________________________________________ Date_____________________________ Perform a visual assessment of a residentrsquos skin upon admission Report any areas of concern to the charge nurse immediately Forward any areas of concern to the next shift Initiate a plan of care to address the problem and alert the CNAs Use this form to show the exact location and description of the abnormality Using the body chart below describe and chart all abnormalities by number
Indicate on the body chart any areas of concern A = Abrasion(s) ST = Skin Tear(s)
B = Bruise(s) SU = Stasis Ulcer(s)
PU = Pressure Ulcer(s) SW = Surgical wound(s)
S = Scar(s) O = Other
Narrative Note Note site length width depth drainage odor pain and any other defining characteristics
Nurse Signature _______________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-07-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Licensed Nurse Weekly Skin Assessment
Resident ______________________________________________________________ Date____________________Room _________________ This form should be completed weekly on all residents per facility policy Any areas of skin requiring treatment should have a thorough record of documentation in addition to this form located elsewhere in the chart per facility protocol Check ldquoYesrdquo or ldquoNordquo if the item reflects the residentrsquos assessment If the answer is ldquoyesrdquo to 3 or more of the items listed below consider implementation of the ldquoSkin Tear Prevention Protocolrdquo Review the care plan to ensure skin care is included as necessary
If any questions are answered ldquoyesrdquo indicate location on body outline with number of question
Weekly Skin Assessment Yes No Any reddened areas that remain after 30 minutes of
1 pressure reduction Comments __________________ o o
Any rashes Comments ________________________2 o o
Any bruises Comments________________________3 o o
Any open lesions cuts lacerations or skin tears 4 (Indicate even if being treated) Comments ________ o o
Any blisters Comments________________________5 o o
Any open ulcers (indicate even if being treated) 6 Comments ___________________________________ o o
Excessively dry or flaky skin Comments___________7 o o
Any edema Location__________________________8 o o
Licensed Nurse Signature _________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-09-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

_________________________________________________________________________________________________
_________________________________________________________________________________________________
Skin Monitoring Comprehensive CNA Shower Review
Perform a visual assessment of a residentrsquos skin when giving the resident a shower Report any abnormal looking skin (as described below) to the charge nurse immediately Forward any problems to the DON for review Use this form to show the exact location and description of the abnormality Using the body chart below describe and graph all abnormalities by number
Resident _______________________________________________ Date_______________________
Visual Assessment 1 Bruising 2 Skin tears 3 Rashes 4 Swelling 5 Dryness 6 Soft heels 7 Lesions 8 Decubitus 9 Blisters
10 Scratches 11 Abnormal color 12 Abnormal skin 13 Abnormal skin temp (h-hotc-cold) 14 Hardened skin (orange peel texture) 15 Other _________________________
CNA Signature_________________________________________________________ Date ____________________
Does the resident need hisher toenails cut
Yes No
Charge Nurse Signature ________________________________________________ Date ____________________
Charge Nurse Assessment___________________________________________________________________________
Intervention ______________________________________________________________________________________
Forwarded to DON
Yes No
DON Signature ________________________________________________________ Date ____________________
Document available at wwwprimarisorg MO-06-42-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Skin Monitoring Daily Skin Check
Skin checks are to be completed daily for residents A good time to do them is during AM and PM care and during bathing time List the resident name type and site (as listed below) of observed impaired skin integrity
Diagram Key Types Sites bull Bruises(B) bull EarsRTorLT(E) bull Skintears(ST) bull Shoulders(S) bull Pressureulcers(PU) bull Arms(A) bull Scabs(S) bull BackofHead(H) bull Other(O) bull Coccyx(CO) bull Legs(L) bull Shin(SH) bull Knees(K) bull Feet(F) bull Heels(HE) bull Handsfront(HF) bull Handsback(HB) bull Other(O)
E E
AA
HF HF L L
KK
SH SH
FF
E EH
S S
AA CO
L L
HE HE
Resident Name Type Site
Staff Name _____________________________________________ Completion Date___________________
Document available at wwwprimarisorg MO-08-43-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Systems Investigative Audit Pressure Ulcer PreventionTreatment
Purpose To evaluate the decision-making process and adequacy of the facilityrsquos process in the prevention of pressure ulcers and appropriateness of treatment protocols bull NOTEthefollowingauditcriteriaarebroadSelectacurrentclinicalpracticeguideline(CPG)orutilizethefacilityassessmenttoolforpressure
ulcers to guide your detailed audit Criteria
1 Residentisscreenedwithin24hoursofadmissionforriskofskin breakdownusingastandardizedrisk-screeningtool
2 Anappropriatepressureulcerpreventionortreatmentcareplanwas putintoplacewithinthefirst24hoursofadmissionforallresidents whetherhighorlowriskandaccordingtocurrentCPGs
3 Skinwoundassessmentsreassessmentweredoneatappropriate intervalsaccordingtodeterminedlevelsofriskandcurrentCPGs bull Fullskinassessmentatleastweeklywithdetaileddocumentation
accordingtoCPGsofwoundconditionifpresent bull Atleastdailymonitorpressuresitesandareasofskinchanges bull Progressofwoundhealingisreassessedq2-4weeksandtreatment
plan re-evaluated if no evidence of progress noted 4 Thecareplanincorporatedthefollowingcareneedsaswellasall
identifiedriskfactors bull Needsforturningpositioningwereidentified bull Positioningpressurereliefproductneedswereidentifiedand
utilizedconsistentlyandproperly bull Nutritionassessmentwascompletedandidentifiedneeds
included in the care plan bull Individualizedskincareneedswereidentifiedandincludedinthe
care plan bull Interventionswereincludedfromalldisciplinesforeitherpressure
ulcer prevention or treatment 5 Careplaninterventionswereimplementedasindicated
6 Careplanwasconsistentlyevaluatedandrevisedbasedoncurrent resident assessed needs
7 Documentationofskinconditioninterventionforriskfactors treatment of existing pressure ulcers and evaluation of effectiveness wastimelyconsistentandfollowsrecommendedCPGs
8 Anappropriatesystemforcommunicatingtoalldirect-carestaffskin riskfactorsinterventionsandchangesintheplanofcarewasinplace and functioned properly
9 Responsibilityandaccountabilitywasassignedforeachphaseofthe pressureulcerpreventiontreatmentprocess bull Thosedesignatedasresponsibleandaccountableformonitoring
theprocessesofpressureulcerpreventiontreatmentcarriedout theirresponsibilitiesinatimelymanner
10Policyandprotocolsareupdatedandcommunicatedtoallstaff according to current clinical practice guidelines
11TheQACQIcommitteehadprocessesinplacetotrackandidentify patternsandtodeterminetherootcauseofskinbreakdownevents bull Identifiedsolutionsweresystem-oriented bull Contentofstaffeducationwasdeterminedbycompetency
evaluationsandidentifiedareasofweakness12Ifresidentself-determinationwasacontributingfactorinpressure
ulcerdevelopmentreasonablecounseleducationandalternatives wereprovided
Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Systems Investigative Audit Pressure Ulcer PreventionTreatment Page 2
Reviewer______________________________________________ Dateofreview _____________________________
Chart 1 Chart 2 Chart 3 Chart 4 Chart 5 Chart 6 Comments 1 Admission risk assessment completed with
appropriate tool
2 Skin needs care plan was in place within 24 hrs of admission
3 Assessments and reassessments done at appropriate intervals
4 Care plan incorporates all identified risk factors
5 Interventions are implemented as indicated
6 Care plan shows evidence of timely revisions based on assessed resident needs
7 Skin condition interventions and evaluation of interventions documented
8 Staff demonstrates awareness understanding of care plan content
9 Accountability is evidenced by those responsible for monitoring assessment and follow-up
10 Skin policyprotocols are current amp followed consistently
11 QACQI meetings focus on root-cause analyses
12 Residentfamily education provided
Document available at wwwprimarisorg MO-08-17-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcer Prediction Prevention and Treatment Pathway
Step One Assess Skin Condition
Resident is admitted or readmitted to SNF
Head-to-toe skin assessment (upon admission and weekly)
Does the resident have a pressure ulcer
Report findings to physician
Obtain treatment order from
physician
Notify Family
Turn page Go to Step 2
Pressure Ulcer Documentation Length bull Width bull Depth bull Location bull Stage bull Exudate bull
Tunneling bull Necrosis bull Granulation bull Undermining bull Sinus tracts bull Pain bull
Yes No
Overall Skin Condition Documentation bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact skin bull Bruises bull Burns
Report anything abnormal to physician
Notify Family
Turn page Go to Step 2
Obtain treatment order from physician if
appropriate
Remember if a patient is at risk or has a pressure ulcer repeat Step One on a weekly basis
Document available at wwwprimarisorg
Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Yes
Yes
Yes
Yes
Pressure Ulcer Prediction Prevention and Treatment Pathway
Step Two Complete Risk Assessment to Identify Risk Factors and Care Plan Interventions
At Risk Remember that those with a pressure ulcer are automatically at risk
Repeat skin risk assessment at least every 90 days and significant change or per facility protocol
Care Plan Actual Skin Problem Care Plan Potential Skin Problem
Complete Care Plan Problem Statement Skin integrity impaired actual as evidenced by (AEB) (Wound-specific description Location stage and measurements) related to (RT) identified risk factors
Complete Care Plan Problem Statement Potential for impaired skin integrity as evidenced by (AEB) risk assessment indicates that the resident is at risk for skin breakdown related to (RT) identified risk factors
Bed TR schedulebull Pressure reducingrelieving device bull Therapy consult bull
Chair Repositioning schedule bull Pressure-relieving cushion bull Assessment of chair fit bull
FrictionShear Padding to prevent skin contact bull Bootiesheel protectors elevate heels bull HOB in lowest position possible unless contraindicated by medical condition bull Positioning devices bull
Does the resident have a pressure ulcer
Incontinence Peri care after each incontinence bull Clean as soon as possible after soiling bull Barrier cream bull Incontinent pads incontinent briefs bull
Moisture Remove incontinence brief while bull in bed Moisture barrier bull
Nutrition and body weight
Weekly weight bull Dietician consult bull Labsbull Food supplements bull Speech therapy bull
Vitaminmedication supplements bull Hydration bull Feeding assistance bull Assessment for chewing and swallowing problems bull
Other Add anyall interventions related to identified specific risk factors bull
BedChair Mobility
BB Incontinence
and Moisture
Nutrition and Body
Weight
Other Resident-
specific Risk Factors
Friction andor Shear
Yes
Yes No
No
No
No
No
Yes
Possible Care Planning Interventions Address Possible Risk Factors
Perform Step Two at least every 90 days and with any significant change Adjust care plan as needed
Complete Skin Risk Assessment
No
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

ldquo rdquo ldquo rdquo ldquo rdquo ldquo rdquo
Tissue Tolerance and Individualized Turning Schedule
Resident ______________________________________________________________ Date____________________Room _________________ Recommended times for change in position are noted with desired position
Codes RS ( right side) LS ( left side) B (back) OOB ( liftshift in chair) WC HOB ( head of bed raised seating) T (toileted)When repositioning check after 30 minutes to see if the bony prominence is still red Report to nurse
Change every hour in WC and at least ever 2 hours in bed Do not raise HOB higher than 30 degrees unless directed by nurse
Date
Check back after Check back after Check back after Check back after turned red after 30 turned red after 30 turned red after 30 turned red after 30
Actual min Indicate no Actual min Indicate no Actual min Indicate no Actual min Indicate no
Time Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
Desired position
position amp initials
or Location that is still red
1130 pm
130 am
330 am
530 am
730 am
930 am
1130 am
130 pm
330 pm
530 pm
730 pm
930 pm
Initial Name Initial Name Initial Name Initial Name
Document available at wwwprimarisorg MO-08-13-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy Adapted from Ratliff Care Center
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-
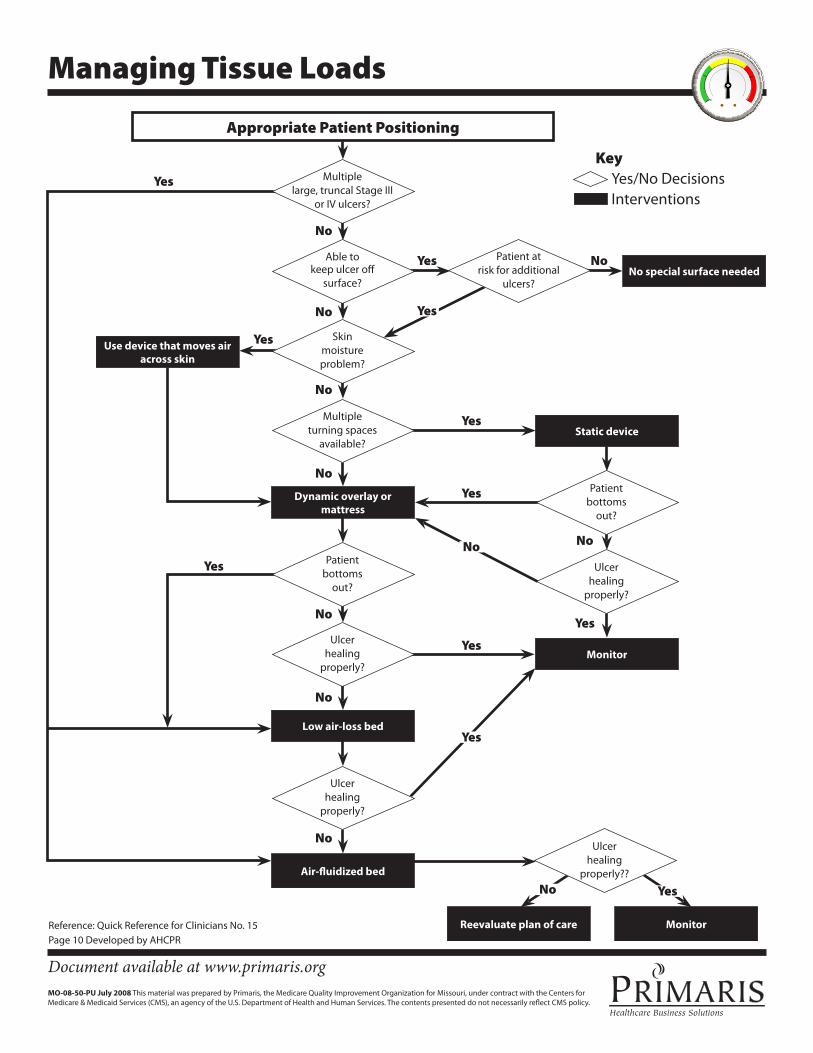
Managing Tissue Loads
Appropriate Patient Positioning
Reevaluate plan of care Monitor
Patient at risk for additional
ulcers No special surface needed
Use device that moves air across skin
Dynamic overlay or mattress
Air-fluidized bed
Multiple large truncal Stage III
or IV ulcers
Able to keep ulcer off
surface
Skin moisture problem
Multiple turning spaces
available
Patient bottoms
out
Ulcer healing
properly
Low air-loss bed
Ulcer healing
properly
Monitor
Static device
Ulcer healing
properly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Ulcer healing
properly
Yes No
No
No
No
No
No No
No
No
No
No
Patient bottoms
out
Key YesNo Decisions Interventions
Reference Quick Reference for Clinicians No 15 Page 10 Developed by AHCPR
Document available at wwwprimarisorg MO-08-50-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Support Surfaces Characteristics and Considerations
Specialty Beds
Air-fluidized bed (also known as a ldquobead bedrdquo or ldquosand bed rdquo) Product Characteristics This is a bed frame containing silicone-coated beads incorporated in Gortexreg covering When air is pumped through the beads they behave like a liquid creating air and fluid support The resident ldquofloatsrdquo on a sheet with one third of the body above the surface and the remainder of the body immersed in the warm dry fluidized beads When bed is turned off the surface becomes firm to allow for repositioning Helps manage copious wound drainage or incontinence by absorbing fluids into bed of silicone beads Although there is some evidence that air-fluidized beds enhance pressure ulcer healing rates surface interface pressure remains sufficiently high to occlude capillary perfusion Occipital and heel ulcers have been reported to develop in patients while on an air-fluidized bed (Parish amp Witkowski 1980) Considerations
bull Not recommended for mobile patients patients with pulmonary disease or patients with unstable spine bull Continuous circulation of warm dry air may dehydrate patient or desiccate wound bed bull Bed may get too hot or make room hot bull Head of bed cannot be raised semi-Fowlerrsquos position achieved by using foam wedges or movable sling-type device bull Coughing less effective in mobilizing secretions bull Leakage of beads may irritate the eyes and respiratory track and make floor slippery bull Width of bed may preclude care to obese patients or patients with a contracture bull Height of bed makes some nursing care difficult and a step is needed to facilitate care bull Transfer of patient out of bed is difficult bull Bed is heavy and not easily transferable bull Some patients become disoriented or complain of feeling weightless while on surface bull Dependent drainage of catheters may be compromised because the patient is immersed in the bed bull Sharp objects may damage the surface bull Size and weight may be too large for use in home setting bull Set up and maintenance provided by company
Low air-loss bed
Product Characteristics A bed frame with a series of connected air-filled pillows that can be calibrated for varying amounts of pressure to provide maximum pressure reduction for residents Dry air flow between the patient and bed surface helps control moisture and heat buildup and prevents maceration and friction Some models are designed to counteract the effects of immobility on pooling of respiratory secretions and urinary stasis by providing oscillation therapy Other models feature kinetic therapy (rotating slowly side to side) although this is limited to a 20-degree rotation and does not have the same effect as manually rotating the resident side-to-side Considerations
bull Head and foot of bed can be raised and lowered bull Transfers in and out of bed easily accomplished bull Portable motor available to maintain inflation during bed transfers
bull Motor may be noisy bull Proper inflation essential to maintain effectiveness bull Sharp objects may damage the surface
Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Support Surfaces Characteristics and Considerations page 2
bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Set up and maintenance provided by company
Dynamic Overlays
Alternating air-filled overlay Product Characteristics Air is pumped through overlay chambers at regular intervals to provide cyclical pressure changes creating a low-pressure and a high-pressure area These surfaces constantly change pressure points and create pressure gradients that enhance blood flow Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of not less than 3 inches is recommended Considerations
bull Surface is easy to clean bull Assembly required bull Sensation of inflation and deflation may bother patient bull Electricity required bull Motor may be noisy bull Excessive or sudden surface movement may disturb sleep bull Sharp objects may damage the surface bull Bed surface is slippery patients may slide down or out of bed with being transferred bull Heels need to be ldquofloatedrdquo to totally relieve pressure
Static Overlays
Foam Overlay Product Characteristics A foam surface applied over the surface of an existing hospital mattress The following characteristics of foam influence the effectiveness of the overlay base height density and indentation load deflection (ILD) Base height refers to the height of the foam from the base to where the foam ridges begin and should be 3 to 4 inches to be effective in reducing pressure Density refers to the weight per cubic foot and reflects the foamrsquos ability to support the personrsquos weight Foam densities of 13 to 16 pounds per cubic foot are generally effective in supporting an average size adult ILD is a measure of the firmness of the foam It describes the foamrsquos compressibility and conformability It also indicates the ability of the foam to distribute the mechanical load Measurement of ILD is expressed as the number of pounds required to indent a sample of foam with a circular plate to a depth of 25 of the thickness of the foam An ILD of approximately 30 pounds is recommended Optimal support and conformability of foam is achieved when the relationship between 60 ILD and 25 ILD is 25 or greater (Krouskop amp Garber 1987 Whittemore 1998) Considerations
bull Plastic protective sheet is usually required for incontinent patients bull Foam may trap perspiration and be hot bull Washing removes flame-retardant coating bull One-time charge no reoccurring charges bull No set up or maintenance fees bull Cannot be punctured by needle or metal traction bull Light weight
Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Support Surfaces Characteristics and Considerations page 3
bull Requires no maintenance bull No electricity required to operate bull May be hot and trap perspiration bull Foam has a limited life bull Lack of firm edge creates unsure surface when patient transferring on and off surface bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Must be discarded when wet from drainage or incontinence bull Adds height to the bed
Air Overlay
Product Characteristics Interconnected bubble-like cells that are inflated with an air blower to an appropriate pressure level Optimum air level is defined as 1 inch or more of uncompressed support surface between bony area of the residentrsquos body and the caregiverrsquos hand when placed under the support surface Cells with larger diameter and depth produce greater pressure relief over the body A cell depth of 3 in or greater is recommended Considerations
bull Easy to clean bull Low maintenance bull Repair of some products is possible bull Durable bull Can be damaged by sharp objects bull Requires regular monitoring to determine proper inflation and need for reinflation bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Adds height to bed bull Lacks a firm edge so transfer on and off surface may be difficult
Water Overlay
Product Characteristics A vinyl chamber that can be filled with water to appropriate level to distribute body weight evenly over the entire supporting surface Recommended depth is 3 in or greater Some models contain a baffle system to control motion effects Considerations
bull Readily available in the community bull Easy to clean bull Requires water heater to maintain comfortable water temperature bull Fluid motion makes procedures difficult (eg positioning) bull Patient transfers may be difficult bull Inadvertent needle punctures will create leaks bull Maintenance is needed to prevent microorganism growth bull Surface is heavy bull Cannot raise head of bed unless mattress has compartments bull Can be overfilled (causing too firm a surface) or underfilled (decreasing pressure reducing benefit)
Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Support Surfaces Characteristics and Considerations page 4
Gel Overlay
Product Characteristics A pad constructed of Silastic silicone or polyvinyl chloride Lack air-flow for moisture control and friction control is variable depending on the surface of the gel Recommended depth for effective support is 2 in or more Gel filled pads are particularly useful in wheelchairs Considerations
bull Low maintenance bull Easy to clean bull Multiple-patient use bull Impermeable to punctures with needles bull Surface is heavy bull Expensive purchase price bull Heels need to be ldquofloatedrdquo to totally relieve pressure bull Research on effectiveness is limited bull Some surfaces may be slippery patient may slide down or out of bed during transfers
Replacement Mattress
Product Characteristics Mattress made of foam and gel combinations or layers of different foam densities Some models have replaceable foam shapes and some have a replaceable foam core Other replacement mattresses contain a series of air-filled chambers covered with a foam structure All models are covered with a comfortable water-repellent bacteriostatic cover that can be maintained with routine cleaning Mattresses with foam should be antimicrobial and have appropriate foam ILD with high resiliency Evidence is increasing that replacement mattresses are superior to standard hospital mattresses and may be more effective than some overlays (Vyhlidal et al 1997) Considerations
bull Reduce use of overlay mattresses bull Reduce staff time bull Do not add height to mattress bull Provide certain level of pressure reduction automatically bull Multiple-patient use bull Easy to clean bull Use standard hospital linens bull Low maintenance bull Initial expense is high bull Some mattresses have removable sections which may be misplaced bull May not control moisture bull Potential for excessive delay in using other support surface bull No objective method for determining when or if product loses effectiveness bull Life of product is not known
Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Support Surfaces Characteristics and Considerations page 5
Additional References
Hess CT Wound care Springhouse Pennsylvania 2000 Springhouse Corporation
Krouskop TA Garber SL The role of technology in the prevention of pressure sores Ostomy amp Wound Management 1645 1987
Maklebust J An Update on Horizontal Patient Support Surfaces Ostomy amp Wound Management 45 No 1A (suppl) 70S to 77S 1999
Maklebust J Sieggreen M Pressure ulcers guidelines for prevention and management Pennsylvania 2001 Springhouse Corporation
Parish IC Witkowski JA Clinitron therapy and the decubitus ulcer preliminary dermatologic studies Dermatology 19517 1980
Vyhlidal S et al Mattress replacement or foam overlay A prospective study on the incidence of pressure ulcers Applied Nursing Research 10(3)111 1997
Whittemore R Pressure reduction support surfaces A review of the literature JWOCCN 256-25 1998
Source National Nursing Home Improvement Collaborative Coordinated by Qualis Health Learning Session Two January 2004
Document available at wwwprimarisorg MO-08-48-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Treatment Product Categories
Pressure ulcers require consistency in treatment to promote healing Use this list that includes the major types of products to ensure your nursing center carries an appropriate range of materials Nursing staff then can choose the most effective dressing type based on wound stage characteristics and potential concerns
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Polyurethane Film Tegadermtrade Op-siteloz EpiVIEWtrade others
Adhesive and transparent Stages 1-2 Occlusive and waterproof Retains water Impermeable to bacteria amp contamination Promotes moist wound healing Nonabsorbent May be changed every 3 to 7 days May be used as a secondary dressing over a more absorbent product
Should not be used with moderate to heavy exudate wounds May macerate surrounding skin
Hydrocolloid DuoDERMreg Replicarereg Comfeelreg Others
Adhesive wafers composed of gelatin pectin and carboxymethyl-cellulose
Stages 1-4 Occlusive and waterproof Retains moisture Impermeable Promote moist wound healing Moderately absorbent Easy to apply
Should not be used with heavy exudate wounds Should not be used if infection is present May have odor upon removal May be difficult to remove
Hydrogels Hypergelreg Carrasynreg DuoDERMreg Elasto-Gel Sheettrade SoloSiteloz Others
Glycerin or water based gels wafers sheets and impregnated gauze with or without adhesive borders
Stages 2-4 Non-adherent Fills dead space Semi-occlusive Promotes moist wound healing Easy to apply amp remove Minimally absorbent Retains moisture and rehydrates wound
May macerate surrounding tissues Secondary dressing required Daily application required unless applied with adhesive borders Dries out easily Risk of candidiases
Foams PolyMemreg Allevynloz Lyofoamreg Others
Hydrophilic polyurethane foam available in wafers sheets and pillow with foam covering
Stages 2-4 Non-adherent Easy to apply and remove Highly absorbent
Can be used on various levels of exudate Additional fixation is required unless has an adhesive border
Alginates SORBSANtrade KALTOSTATreg Algisite Mloz Others
Non woven fibers containing calcium sodium salts of alginic acid available in pads or ropes
Stage 2 wounds with a lot of exudate Stages 3-4
Non-adherent Promotes moist wound healing Can be used on infected wounds
Should not be used on dry or low exudate wounds the wound may get dehydrated Secondary dressing required Typically requires daily application
Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers Treatment Product Categories Page 2
Treatment Products Description
Appropriate Wound Stage Characteristics Concerns
Antimicrobial ACTICOATloz SilvaSorbreg IODOSORBloz ALLEVYN Agloz Optifoam AGreg Others
Ionic silver and cadexomer iodine that provides sustained antimicrobial barrier to multiple bacteria including strains of MRSA and VRE Can be found in different types of products including alginates gels and polyurethane film
Stage 2 wounds when antimicrobial treatment is needed Stages 3-4
Manages bacterial burden Non-cytotoxic
Do not use with a resident with a known sensitivity to silver Iodine products should be avoided if known sensitivity or thyroid disorder Do not use in conjunction with topical antibiotics
Collagen Biosteploz Prismareg Promogranreg Puracolreg Others
Collagen provides the matrix for the bodyrsquos tissue structure Stimulates wound healing Can be found in different delivery systems dried collagen matrix hydrogel with collagen hydrogel base
Wounds that have stalled in healing Chronic wounds
Promotes new tissue growth Wound debridement Pulls wound edges together
Do not use on dry wounds Do not use with patients sensitive to bovine products
Gauze Dry or Wet Woven natural cotton fibers non woven rayon and plastic blends available in pads and rolls sterile and non sterile
Stages 2-4 especially if wound is deep or has tissue that needs debridement
May be dampened with saline or water Inexpensive Facilitates moist to dry debridement Non-adherent when used as a wet to moist dressing Minimal to moderate absorbency
Moist to dry debridement can be painful damaging healthy tissue Woven gauze is abrasive Requires frequent changes Packing may harden causing further pressure injury
Related Wound Treatments
Treatment Products Description Indications Contraindications ConcernsPrecuations
Vacuum Controlled Assisted Closure (VAC) KCI VACreg Engenextrade EZCAREloz V1STAloz
System that uses controlled negative pressure to help promote wound healing VAC system pulls infectious materials and excess interstitial fluid from the wound
Pressure ulcers Traumatic wounds Post op-dehisced amp surgical wounds
Malignancy Untreated osteomyelitis Unexplored fistulas into the body cavity or to an organ Necrotic tissue with eschar in the wound abed Exposed arteries or veins Uncontrolled pain
Active bleeding Difficult hemostasis Anticoagulant therapy
Brands are listed for reference purposes only We do not recommend use of one brand over another
Document available at wwwprimarisorg MO-08-45-PU June 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Policy
Nutritional Wound Healing Guidelines
This sample procedure is to help enhance the healing of pressure ulcers by the use of nutritional intervention whenever possible These are guidelines only and individual patient and resident needs must be taken into consideration before implementation
Procedure
bull The nursing department reports all pressure ulcers and their stage to food and nutrition services bull The available dietician is contacted and reviews each case to make an individualized nutrition care plan bull Food and nutrition services may implement the following interventions based upon the stage of residentrsquos
pressure ulcers Note that vitamin and mineral supplementation would require a physicianrsquos order raquo Stage 1 4 Vitamin C-rich food high protein afternoon snack and a daily MVI with minerals raquo Stage 2 Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day and MVI with
minerals daily raquo Stage 3 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks twice a day and MVI with minterals raquo Stage 4 8 oz Arginine-intensive nutritional supplement (8 oz Arginaid Extra) twice a day high-protein
snacks three times a day and MVI with minerals
Other nutritional considerations
bull Think about other options to enhance nutritional status such as raquo Increase eggs milk meat and cheese for additional HBV protein raquo Add protein powder to foods raquo Add other foods high in Vitamin C if the resident or patient dislikes orange juice raquo Use Arginaid powder in place of Arginaid Extra if the patient is obese
bull Continue nutritional interventions until wound has been healed for two weeks bull Avoid zinc supplementation for more than two months at a time bull Goal caloric intake is 30-35 kcal per kg or BMR x 15 stress factor x 12 (bed) or 13 (out of bed) bull Goal protein intake with no renal considerations is as follows
raquo Stage 1 12-14 g per kg raquo Stage 2 14-16 g per kg raquo Stage 3 16-18 g per kg raquo Stage 4 18-2 g per kg
bull Goal of fluid is 30-35 ml fluid per kg bull If on chronic antibiotic use give yogurt or lactobacillus supplements bull If patientresident has a compromised gut (intestinal mucosal atrophy or malabsorbtion from malnutrition
10-20 mg of glutamine supplementation should be considered
Note 8 oz Arginaid Extra provides the following 10 g protein 250 calories 20 mg zinc 1000 IU vitamin A 250 mg vitamin C MVI with minerals usually contain the following amounts 15 mg zinc 3500 IU vitamin A 60 mg vitamin C 18 mg iron and 2 mg copper
Document available at wwwprimarisorg MO-08-46-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Selected Characteristics of Support Surfaces
Selected Characteristics for Classes of Support Surfaces Support Devices
Performance characteristics Air-fluidized Low Air-loss Alternating
Air Static Flotation
(air or water) Foam Standard Mattress
Increased support area Yes Yes Yes Yes Yes No
Low moisture retention Yes Yes No No No No
Reduced heat accumulation Yes Yes No No No No
Shear reduction Yes Yes Yes No No
Pressure reduction Yes Yes Yes Yes Yes No
Dynamic Yes Yes Yes No No No
Cost per day High High Moderate Low Low Low
Reference Quick Reference Guide for Clinicians No 15 page 11 Developed by the Agency for Healthcare Research and Quality (AHRQ)
Chair Support Surfaces Support Surface Characteristics Cost Concerns Foam Cushion
Gel Cushion
Air-filled Cushion
bull
bull
bull
bull
bull
bull
Provides some pressure reduction depending upon the thickness of the foam (a thickness of no less than four inches is recommended) Resident still requires repositioning at least every hour
Low Cost
Reduces pressure by spreading pressure across the contact surface Does not replace repositioning
Low to Moderate
Cost
Reduces pressure by evenly distributing weight Cells fill with air and deflate as pressure is applied Does not replace repositioning
High Cost
bull
bull
bull
bull
After laundering this surface is no longer useful for pressure reduction A slip cover that can be separately laundered keeps the cushion clean and dry
Pressure reduction depends on the cushionrsquos condition (watch for breaks in the integrity of the cushion which renders this product ineffective) Do not attempt to mend any breaks in the cushion
Compromised integrity can render this product ineffective An ineffective air-filled cushion should be replaced
Document available at wwwprimarisorg MO-08-51-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

____________________________________________________________________________________________________________
SBAR Skin Care Instructions Situation
S Resident Name ______________________________________________________ Age___________ Admit Date _________________ Admitting physicianconsulting physician ___________________________________________________________________________ Diagnosisreason for admission ____________________________________________________________________________________ Treatment plan _________________________________________________________________________________________________
Background (check all that apply)B Past medical history _____________________________________________________________________________________________ Allergies _______________________________________________________________________________________________________ Diet type ___________________________________________ q NGG-tube feedings q TPNPPN q Ostomydrains q Foley
Medication Medication
Assessment (check all that apply)A q Pressure ulcer present q Precautions___________ q Completely immobile q Limited mobility q Fully mobile q Incontinent q Impaired sensation q Alertoriented q Confused q Lethargicunresponsive q Photos taken
Braden Score_______ q High Risk q Low Risk q No Risk
Decubitus Key Stage I Redskin intact Stage II Superficial breakdown Stage III Skin breakdown Sub Q involved Stage IV Skin breakdown Musclebone exposed Do no stage if base of wound not visible
Site Diagram
Date Site Stage Size (in cm) Description (color drainage odor sloughing eschar undermining)
Recommendation (check all that apply)
Pressure Ulcer Prevention Measures q Keep clean and dry q Avoid diaperbrief use q Apply cleanserbarrier lotions to ________ every ____ hours q Apply Nystatin powder to _____________ every ____ hours q Use special bedmattress (specify type) __________________ q Turn and reposition patient every ______ hours q Use chair cushion (specify type) ________________________ q Elevate heels q Use heel protectorsheel lift q Use elbow protectors q Dietarynutrition consult q Other______________________________________________
Pressure Ulcer Management q Ulcer treatment _____________________________________ q Dressings (specify type and frequency) __________________
___________________________________________________ q Wound vac _________________________________________ q Consider Foley catheter_______________________________ q Odor control________________________________________ q Dietarynutrition consult q Other______________________________________________
___________________________________________________
Front Back
Left Left Right Right
R
Comments _____________________________________________________________________________________________________
Assessment and recommendations completed by (signature)__________________________________ Date __________________Treatment protocol approved by (signature) ________________________________________________ Date __________________
Document available at wwwprimarisorg MO-08-52-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

What happens if I get a pressure ulcer Pressure ulcers are serious problems that can lead to pain slower recovery from health problems and possible complications such as infection By working with your health care team to lower your risk factors most pressure ulcers can be prevented
Ask your health care provider if you are at risk for pressure ulcers and work together to develop a plan to prevent them
MO-08-44-PU June 2008 This material was prepared by Primaris a Medicare Quality Improvement Organization under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
protects your
PPUUPP
ressureressurelcerlcer
reventionrevention
PUP
skin
Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Reduce your risk of getting pressure ulcers Get your family and health care team involved in prevention
What is a pressure ulcer A pressure ulcer also known as a pressure or bed sore is an area of the skin that has damage caused by unrelieved pressure Pressure ulcers begin as reddened areas but can damage skin and muscles if not treated properly
Where are they found on the body Pressure ulcers typically occur in bony areas of the body that sustain pressure when lying or sitting in bed for long periods of time (shoulders elbows hips buttocks and heels)
Who gets pressure ulcers Anyone confined to a bed or chair who is unable to move has loss of sensation bowel or bladder control poor nutrition or has lowered mental awareness is at risk of getting a pressure ulcer
What can I do to prevent pressure ulcers bull Keep moving and change your position frequently If you
are unable to move yourself make sure the staff helps you reposition regularly
bull Look after your skin Keep skin and bedding dry and moisturize dry skin
bull Look for skinrsquos warning signs Let the staff know if your skin stays red longer than thirty minutes feels warm or firm to the touch andor is blistered or broken
bull Reduce friction Donrsquot pull or drag yourself across sheets or push or pull with your heels Avoid repetitive movements such as scratching your foot on the sheets
bull Eat a balanced diet Ask your nurse or health care professional for a proper nutritional plan
Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcer Definition and StagesPressure UlcerPressure Ulcer Definition and StagesDefinition and Stages
PR ESS UR E ULC E R STAGE SDEF IN ITI ON
A pressure ulcer is localized injury to the skin andor underlying tissue usually over a bony prominence as a result of pressure or pressure in combination with shear andor friction
A number of contributing or confounding factors are also associated with pressure ulcers the significance of these factors is yet to be elucidated
Pressure ulcers are staged using the system at right
(SUSPECTED) DEEP TISSUE INJURY Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tisshysue
Further Description Deep tissue injury may be diffishycult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covshyered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
STAGE I Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigshymented skin may not have visible blanching its color may differ from the surrounding area
Further Description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
STAGE II
STAGE IIIFull thickness tissue loss Subcutaneous fat may be visshyible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further Description The depth of a stage III presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bonetendon is not visible or directly palpable
STAGE IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further Description The depth of a stage IV presshysure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subshycutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bonetendon is visible or directly palpable
National Pressure Ulcer Advisory Panel 1255 Twenty-Third Street NW Suite 200 Washington DC 20037 T 202-521-6789 F 202-833-3636 wwwnpuaporg
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further Description Presents as a shiny or dry shalshylow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicated suspected deep tissue injury
UNSTAGEABLEFull thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Further Description Until enough slough andor eschar is removed to expose the base of the wound the true depth and therefore stage cannot be detershymined Stable (dry adherent intact without erythema
removed
This staging system should be used only to describe pressure ulcers Wounds from other causes such as arterial venous diabetic foot skin tears tape burns perineal dermatitis maceration or excoriation should not be staged using this system Other staging systems exist for some of these conditions and should be used instead
or fluctuance) eschar on the heels serves as ldquothe bodyrsquos natural (biological) coverrdquo and should not be
Updated 022007 Copyright copy 2007
Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcer Classifications
Suspected Deep Tissue Injury Purple or maroon localized area of discolored intact skin or blood-filled blister due to damage of underlying soft tissue from pressure andor shear The area may be preceded by tissue that is painful firm mushy boggy warmer or cooler as compared to adjacent tissue
Further description Deep tissue injury may be difficult to detect in individuals with dark skin tones Evolution may include a thin blister over a dark wound bed The wound may further evolve and become covered by thin eschar Evolution may be rapid exposing additional layers of tissue even with optimal treatment
Stage 1 Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching its color may differ from the surrounding area
Further description The area may be painful firm soft warmer or cooler as compared to adjacent tissue Stage I may be difficult to detect in individuals with dark skin tones May indicate ldquoat riskrdquo persons (a heralding sign of risk)
Stage II Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed without slough May also present as an intact or openruptured serum-filled blister
Further description Presents as a shiny or dry shallow ulcer without slough or bruising This stage should not be used to describe skin tears tape burns perineal dermatitis maceration or excoriation
Bruising indicates suspected deep tissue injury
Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcer Classifications
Stage III Full thickness tissue loss Subcutaneous fat may be visible but bone tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling
Further description The depth of a stage III pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and stage III ulcers can be shallow In contrast areas of significant adiposity can develop extremely deep stage III pressure ulcers Bone tendon is not visible or directly palpable
Stage IV Full thickness tissue loss with exposed bone tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling
Further description The depth of a stage IV pressure ulcer varies by anatomical location The bridge of the nose ear occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow Stage IV ulcers can extend into muscle andor supporting structures (eg fascia tendon or joint capsule) making osteomyelitis possible Exposed bone tendon is visible or directly palpable
Unstageable Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow tan gray green or brown) andor eschar (tan brown or black) in the wound bed
Source National Pressure Ulcer Advisory Panel Pressure Ulcer Stages Revised February 2007 Permission to use granted to Primaris the Quality Improvement Organization for Missouri
Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Documentation and Measuring
Measuring Wounds Measure the length ldquohead to toerdquo at the longest point (A) and the width at the widest point (B) Measure the depth (C) at the deepest point of the wound All measures should be in centimeters
A
B
C
Using a clock format describe the location and extent of tunneling (sinus tract) andor undermining
6
12
39
The head of the patient is 1200 the patientrsquos foot is 600
This
rule
r is i
nten
ded
for u
se a
s a re
fere
nce
only
To
prev
ent i
nfec
tion
do
not u
se th
is ru
ler t
o m
easu
re a
n ac
tual
wou
nd
CM1
2 3
4 5
67
89
1011
1213
14
15
sam
ple
TunnelingSinus Tract A narrow channel of passageway extending into healthy tissue
Undermining Tunneling wound which begins directly under the wound edge
If the wound has many landmarks you may want to trace it before measuring
Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure ulcer documentation includes
Wound location Stage
Size bull Length bull Width bull Depth
TunnelingSinus Tract Undermining Necrotic Tissue bull Slough bull Eschar
Granulation
Pain ExudateDrainage bull Amount bull Color bull Odor
Description of Surrounding Tissue Support Surface Wound edges bull Round bull Rolled bull Extended
Note the following skin characteristics
bull Color bull Incisions bull Temperature bull Scars bull Moles bull Intact bull Bruises bull Burns
MO-08-49-PU July 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services and adapted from LHCR The contents presented do not necessarily reflect CMS policy
Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers CNA Knowledge amp Attitude Survey
We are interested in your individual answer Please check the box to indicate ldquoTruerdquo or ldquoFalserdquo for each of the following statements
Position Title _____________________________________________________________________________
Department _______________________________Shift (check one) o Days o Evenings o Nights
Pressure Ulcers CNA Knowledge and Attitude Survey True False 1 Identification and reporting of reddened or open areas of skin are part of my job o o 2 Pressure ulcer prevention is part of my job o o 3 Pressure ulcers should only be documented by RN or LPN staff members o o 4 Immobility is a cause of pressure ulcers o o 5 Incontinence is a cause of pressure ulcers o o 6 Poor dietary intake is a cause of pressure ulcers o o 7 Chronic illness is a cause of pressure ulcers o o 8 Poor circulation is a cause of pressure ulcers o o 9 Pressure ulcers are part of the aging process o o
10 Pressure ulcers can be prevented by proper positioning of residents o o
11 Pressure ulcers begin with a reddened area of the skin that does not disappear after pressure is relieved o o
12 Residents who have had a pressure ulcer in the past are more likely to develop one in the future o o
13 A bed ridden resident will not fully recover from a pressure ulcer without surgery o o
14 Pressure ulcers are often viewed as a sign of poor care being provided by the nursing staff o o
15 Pressure ulcers lower a residentrsquos self-esteem o o 16 Pressure ulcers can occur on any area of the body o o
Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers CNA Knowledge amp Attitude Survey page 2
CNA Knowledge and Attitude Survey Results A Guide to Action Ask staff to complete the CNA Pressure Ulcer Knowledge and Attitude Survey Then use the following as an answer key and a guide to action Yoursquoll notice that particular answers may be ldquoTruerdquo for some staff and ldquoFalserdquo for others This sheet will show how you might revise overall nursing home practices to improve staff knowledge and residentsrsquo care
Questions 1 amp 2 All nursing home clinical staff should have identification assessment prevention care and documentation of pressure ulcers identified as a part of their job duties If your staff felt this statement was ldquoFalserdquo this may be an area you could focus on for additional training Non-clinical staffrsquos answers may vary between ldquoTruerdquo and ldquoFalserdquo If you have nonndashclinical staff who feel that prevention is not part of their job consider additional training It is important for all staff to recognize ways they can identify potential problems and inform appropriate clinical staff Ideas for improvement bull Explain how and why yoursquore committed to pressure ulcer prevention and treatment bull Describe you homersquos overall pressure ulcer plan bull Describe each team member and family memberrsquos role in pressure ulcer prevention assessment and treatment
Question 3 This question addresses pressure ulcer documentation All staff is responsible for noting information as a part of the general pressure ulcer plan of care Leaders must instruct how and where that information will be documented on the residentrsquos record Non-clinical staff may answer ldquoFalserdquo but you need a process for non-clinicians to report their observations as well ensuring this information is documented Ideas for improvement bull Define pressure ulcer documentation guidelines for all disciplines bull Offer training on sharing work responsibilities among disciplines For example activities staff must
reposition resident while attending activities and document this for staff sharing dietary staff must know the resident with a pressure ulcer cannot sit up to eat
bull Identify pressure ulcer tools to increase documentation consistency throughout the facility and within clinical staff For example ulcer measurement guide bedside turning schedule staging guidelines or exudate documentation
Questions 4 5 6 7 8 and 12 These question reference risk factors for pressure ulcer formation Immobility poor nutrition incontinence and circulatory conditions are all risk factors If your facilityrsquos surveyed staff felt any of these statements were ldquoFalserdquo it may indicate that the pressure ulcer risk factors are not well known or their importance is not well understood You may want to identify if one group of employees or employees in general need information regarding risk factors and the role they play in pressure ulcer formation Questions to ask staff bull What are the identified pressure ulcer risk factors bull How do risk factors contribute to the formation of pressure ulcers bull When are residents assessed for risk factors in your facility bull What effect do risk factors have on residentsrsquo plan of care
Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers CNA Knowledge amp Attitude Survey page 3
Who is responsible for identification and care planning for residents with identified risk factors bull bull Why is this important
Question 9 This question addresses a common misconception Pressure ulcers are not part of the normal aging process Although loss of skin elasticity and thinning of the skin are normal with aging pressure ulcer formation is not If most of your staff answered ldquoTruerdquo to this survey question you need to provide them with information about the normal aging process including bull How the factors of the normal aging process contribute to the risk for pressure ulcer formation bull What your facility is doing to address the care associated with the elderly For example nutritional and
activity programs support groups association with community support group bull Your facilityrsquos efforts to communicate with other health care facilities that you have direct interaction with
ie referring hospitals senior citizen groups physicianrsquos offices home health agencies
Question 10 This question addresses the role of proper positioning in pressure ulcer prevention If the lower extremity were positioned with proper support to keep pressure off the heel an ulcer due to pressure on the heel would be prevented If staff felt positioning did not contribute to pressure ulcer prevention as noted with a ldquoFalserdquo answer consider bull Instruction on and demonstration of basic positioning techniques bull Reviewing your homersquos resident care plans to address proper positioning and repositioning ie turning
schedule pressure reduction techniques devices available at your facility to reduce pressure load bull Reviewing of the etiology of pressure ulcer formation with staff such as prolonged pressure reducing the
blood flow to the capillaries causing tissue damage
Question 11 This question addresses pressure ulcer development Pressure ulcers begin with a reddened area of the skin that does not disappear after the pressure is relieved This is identified as a Stage I pressure ulcer A response of ldquoFalserdquo to this question indicates your staff doesnrsquot have a good understanding of pressure ulcer formation Consider the following actions bull Provide all staff with common consistent definitions of pressure ulcer stages such as guidelines from the
National Pressure Ulcer Advisory Panel bull Adopt standard facility procedures for describing measuring and evaluating pressure ulcers bull Provide consistent tools ndash such as measurement guides and an assessment scale ndash throughout the home for
staff to use consistently bull Review and adapt your pressure ulcer plan of care
Question 13 This question identifies the misconception that a bed-ridden residentrsquos pressure ulcer requires surgery to heal Improved wound care products and pressure reduction devices have greatly increased the healing of pressure ulcers without surgical interventions If staff responded ldquoTruerdquo to this statement consider bull Demonstrating and discussing newer pressure-reduction products available to assist with wound healing and
discussing clinical indications
Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-

Pressure Ulcers CNA Knowledge amp Attitude Survey page 4
Question 14 If clinical staff answered ldquoTruerdquo to this question they may need further education and information about why pressure ulcers occur Consider offering training on bull Non-compliancewithpressureulcerplanofcare bull Diseaseprogression
bull Poornutritionalintake bull Otherpressureulcerriskfactors For non-clinical staff additional information may include bull Trainingontheetiologyofpressureulcerformation
bull Reviewingtheroleofnon-clinicalstaffinpressureulcerpreventionandtreatment bull Reviewingriskfactors bull Informationontheirspecificroleinthecareprocessasitrelatestopressureulcers
Question 15 If staff answered ldquoTruerdquo to this statement it indicates they understand the emotional impact a physical condition can have on residentsrsquo self-esteem Pressure ulcers may limit the independence of the resident They may also contribute to a resident feeling lsquosickrsquo and dependent on others for care Additionally many pressure ulcers occur in areas of the body that are emotionally uncomfortable for people to deal with such as the buttocks Dignity may be compromised if the resident feels embarrassed or ashamed over having a pressure ulcer Family members may be angry at the facility or the resident This could add to feelings of inadequacy the resident may already be experiencing If anybody answered ldquoFalserdquo offer education to all staff families and volunteers about pressure ulcers effect on residentsrsquo psychosocial well-being as well as their physical discomfort
Question 16 Pressure ulcers may occur on any part of the body exposed to unrelieved pressure that decreased the flow of blood a sufficient length of time to cause underlying tissue damage A ldquoFalserdquo answer to this question may indicate that your staff does not understand the etiology of a pressure ulcer Although pressure ulcers generally are noted over boney prominences of the body they can occur at any location where unrelieved pressure is noted Educational intervention may include bull Pressure ulcer definition and staging guidelines bull Proper positioning and repositioning techniques bull Proper use of pressure reduction devices bull Frequent reinforcement that pressure ulcer prevention and treatment is everybodyrsquos responsibility
Document available at wwwprimarisorg MO-08-15-PU May 2008 This material was prepared by Primaris the Medicare Quality Improvement Organization for Missouri under contract with the Centers for Medicare amp Medicaid Services (CMS) an agency of the US Department of Health and Human Services The contents presented do not necessarily reflect CMS policy
- pressure ulcer toolkit NH intro
- F314 summary handout_2008
- PU_MDS skin condition coding tip sheet_2008
- facility assessment checklist_2008
- Sample Protocol
- braden scale_2008
- skin tear risk assessment_2008
- LTC dehydration risk assessment_2008
- comprehensive admission skin assessment_2008
- licensed nurse weekly skin assessment_2008
- CNA shower assessment_2008
- daily skin monitoring tool_2008
- systems investigative audit_2008
- prediction prevention treatment pathway_2008
- tissue tolerance and turning schedule_2008
- managing tissue loads_2008
- PU_support surface characteristics_2008
- PU_treatment product categories_2008
- nutritional wound healing guidelines_2008
- selected characteristics of support surfaces_2008
- SBAR NH skin care_2008
- blank page
- PUP brochure
- blank page
- PU_Definition_Stages_NPUAP
- blank page
- pu_pocket cards
- blank page
- CNA knowledge and attitude survey_2008
-