gastrointestinal bleeding. why is gi bleeding important? mortality rates from upper gi bleeding vary...
TRANSCRIPT
Gastrointestinal Bleeding

Why is GI bleeding important? Mortality rates from upper GI
bleeding vary from 3.5% to 7% in the U.S.
Mortality rates for lower GI bleeding is reported at 3.6%
If new GI bleed in hospital, mortality can be 25%
Billions of dollars spent for >300,000 hospitalizations per year

Why is GI bleeding important Complications
Integrilin Heparin, etc.
Iatrogenic causes NSAIDS Aspirin Coumadin

Approach to GI Bleeding Identify the Clinical Setting
ER vs. Ward vs. MICU vs. CCU vs. Clinic Clinical presentation – i.e.
history/assessment Resuscitation Labs Localize Bleed Definitive therapy

Resuscitation Key component to GI Bleed Identify stumbling blocks
Pt with sign comorb. – CHF, valvular hrt dz, etc.
Review setting where res. should occur Access
Should be automatic – 2 large bore IVs

Resuscitation cont. Mention on size:
Poiseuille’s law Triple Lumen: two
18 g, one 16 g with length 20 cm
Central line: 8F with 10 cm length
Short and wide will get the job done

Resuscitation cont. Fluid of choice
Isotonic fluid – Normal Saline or Ringer’s are both good choices
Patients with active bleeding and a coagulopathy (INR>1.5) or thrombocytopenia (<50,000) should be transfused with FFP and platelets, respectively

Resuscitation cont. Frequent vitals checks and gauging
initial status Orthostatics, pulse, hypoxia, symptoms
(agitation, lightheadedness, etc.) Vitals:
Normal BP: minor blood loss <10% of volume + orthostatics: mod blood loss 10-20% of vol. Resting hypotension: SEVERE BLOOD LOSS
>20-25%

HPI Goal is to help identify likely
source and potential etiologies Also to identify those patients
most at risk – i.e. who will crump on the way to the unit
Focus on the details – how much, how long, pain, meds, etc.

HPI – cont. Upper GI bleed commonly presents with
hematemesis (vomiting blood or coffee-ground material) or melena (black, sticky maladorous stool) 5x more likely to be an upper source Defined as bleeding occurring proximal to
the ligament of trietz Melena: at least 50 cc of blood loss –
typically upper source, but cecal bleeds can be melanic
If pt is vomiting BRB – GET NERVOUS!!!

HPI – cont. Bleeding from a lower GI source refers
to blood loss originating from a sight distal to the ligament of Treitz.
Lower GI bleeding typically presents with hematochezia (passage of maroon or bright red blood from the rectum)
Up to 11% of patients with hematochezia may have an upper source
Patient’s historyImportant historical features include:1. Age: elderly are more likely to bleed
from diverticula, ischemic colitis, malignancy and younger patients are more likely bleeding from PUD, esophagitis, varices
2. Prior bleeding3. Known GI disease: diverticulosis, IBD,
PUD, portal hypertension4. Previous surgery
Patient’s history cont.
5.Medications: coumadin, heparin, NSAIDs, aspirin
6.Abdominal pain: PUD, mesenteric ischemia
7.Change in bowel habits, weight loss, anorexia
8.Other comorbid conditions: CKD, coagulation d/o
9.Previous retching: Mallory-Weiss
Lab’s and Rad’s CBC – may be normal LFTs, coags – screening tool and
identifying synthetic dysfunction Chemistry or P2 – watch BUN – will
tend to trend up if upper CXR / AAS – specific clinical
presentations – looking for catastrophe – free air – mediastinum or abdomen

Bedside Studies“Never trust anyone’s lavage” – Todd Sheer
NG Lavage – were the money is made (90% sensitive for UGI) Blood (18% mortality) – GET
NERVOUS Coffee grounds (10% mortality) –
likely not actively bleeding Clear (6% mortality) – could have bled
and stopped Bilious – rules out upper bleed

Bedside Studies cont. Proctoscope
Typically performed by general surgery and for hematochezia
Looking for obvious ulcerations, fissures, etc. - limited exam as only 10-20 cm observed and messy!

Diagnostic Studies and Therapeutics EGD Colonoscopy Tagged RBC scan Angiography Surgery

Further Evaluation and Therapy
EGD: Can be performed at the bedside Has high diagnostic accuracy, is
therapeutic and associated with low morbidity
Should be performed early in the course
Patient must be hemodynamically stable
Further Evaluation and Therapy
Colonoscopy: Advantages include precise
localization of bleeding and potential therapeutic intervention.
Early colonoscopy has been associated with reduced length of hospital stay

Further Evaluation and Therapy
Radionuclide Imaging with TRBC scan: Noninvasive modality Detects bleeding that is occurring at a
rate of 0.1 to 0.5 ml/m. Accuracy rates range from 24 to 91% Clinical utility of this test is for
screening before arteriography

Further Evaluation and TherapyAngiography Requires active blood loss of 1 to 1.5 ml/m 100% specific but sensitivity varies from
30-47% If an active lesion is found, intraarterial
vasopressin can be infused causing vasoconstriction and cessation of bleeding
Complications such as intrarterial thrombosis, embolization and renal failure occur in 11% of patients

Further Evaluation and Therapy
Surgery: General indications for surgery are:
Transfusion requirements that exceed 4-6 units over 24 hours or 10 units overall
More than two to three recurrent bleeding episodes from the same source

Upper GI Bleed
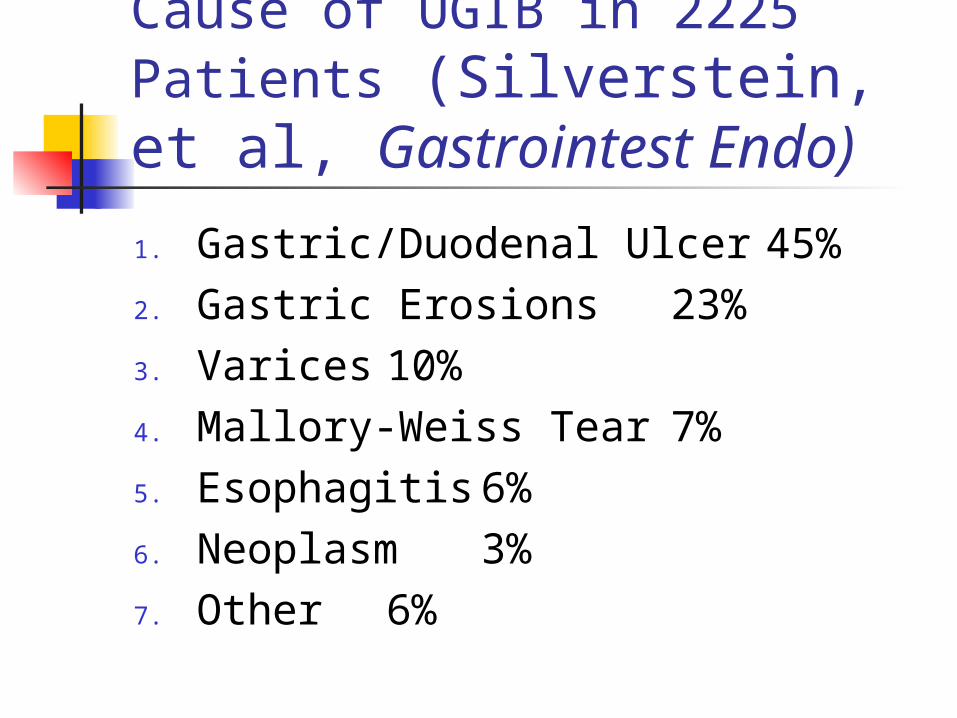
Final Diagnosis of the Cause of UGIB in 2225 Patients (Silverstein, et al, Gastrointest Endo)
1. Gastric/Duodenal Ulcer 45%2. Gastric Erosions 23%3. Varices 10%4. Mallory-Weiss Tear 7%5. Esophagitis 6%6. Neoplasm 3%7. Other 6%
PUD Dr. Robin Warren and Professor
Barry Marshall – fought the battle to prove h. pylori was associated with PUD
Marshall swallowed a culture or h. pylori
Koch would be proud:

PUD cont. Other risk factors: NSAIDS and stress Initial approach: high dose PPI
Capozza: “High dose PPI is as good as endoscopy initially in stopping the bleed”
IV pantoprazole: 80 mg bolus then 8 mg/hr drip
Definitive therapy: endoscopy with injection versus thermal coagulation

Later that night…. Re-bleeding:
Active arterial bleeding 90%
Non-Bleeding visible vessel 50%
Adherent clot 25-30% Oozing without visible
vessel 10-20% Flat Spot 7-10% Clean ulcer base 3-5%

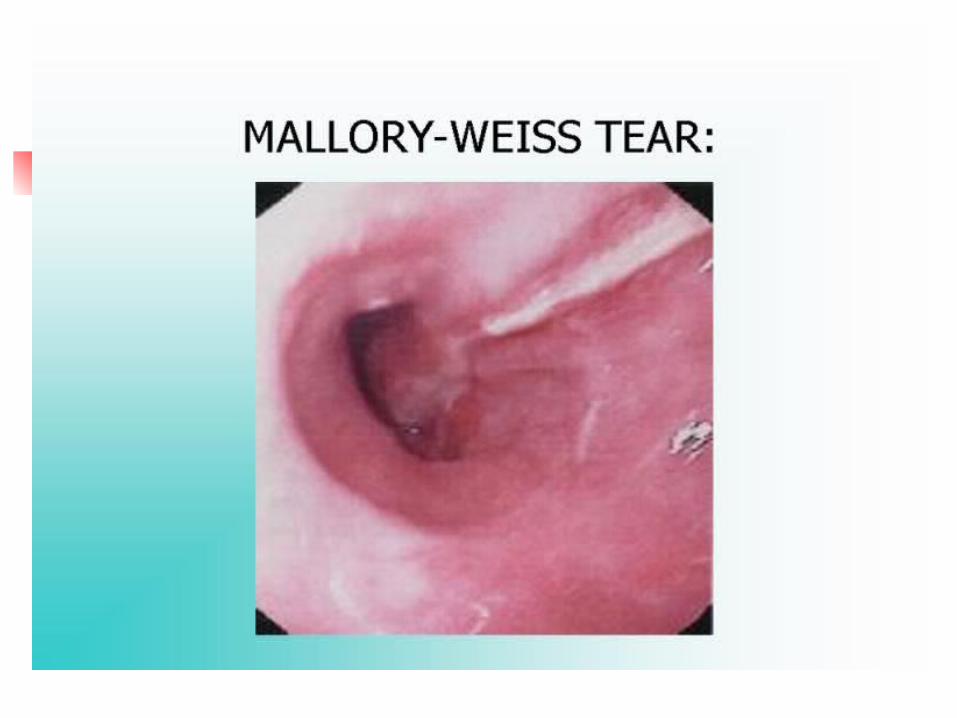
Mallory-Weiss Tear A mucosal tear at
the gastroesophageal junction
Bleeding ceases spontaneously in almost all instances
Consider PPI for 1-2 weeks to promote healing
Mallory-Weiss

Esophageal Varices Variceal hemorrhage requires an ICU
admission Consider endotracheal intubation in
patients who are thought to be actively bleeding for airway protection
Start Octreotide infusion immediately (50 to 100 mcg bolus followed by infusion at 25-50 mcg/hour)
Endoscopy with variceal ligation or banding is the therapy of choice

Esophageal VaricesTIPS (transjugular intrahepatic
portosystemic shunt) A radiologic procedure where a
metal stent is placed between the hepatic veins and portal vein
Indication for TIPS: intractable bleeding unresponsive to variceal ligation or sclerotherapy


Uncommon Causes of Upper GI bleed Gastric antral vascular ectasia Portal hypertensive gastropathy Hemobilia Hemosuccus pancreaticus Aortoenteric Fistulas Upper GI tumors Dieulafoy’s lesion Cameron lesions

Final Diagnosis in Major Lower GI Bleeding
Diverticulosis 43%Angiodysplasia 20%Undetermined 12%Neoplasia 9%Colitis 9%Other 7%


Management of Lower GI Bleed
Acute Hematochezia
Eval and Res.
NGT aspiration
Bile and NO BLOOD
All other
EGD UGI source
Treat as appropriate
negativecolonoscopy

Source identified Negative Exam Not possible due to severity of bleeding
Treat as appropriateHas hematochezia ceased?
no
YES
Small bowel studies
Arteriography versus nuc med scan
Surgical consultation

Diverticular Bleeding Occurs in only 3% of patients with
diverticulosis 75% of diverticula occur in the left side of
the colon Source of diverticular bleed is right sided
50-90% of the time Acute, painless hematochezia Self-limited 70-80% of the time Colonoscopy is diagnostic and
therapeutic
Angiodysplasia Dilated, tortuous submucosal vessels May be the most frequent cause of
acute lower GI bleed in patients over 65
Painless hematochezia Self limited Colonoscopy is diagnostic and
therapeutic

Ischemic Colitis Common entity in the elderly Usually caused by low flow states and
small vessel disease rather than large vessel occlusion
Most commonly occurs at splenic flexure, descending or sigmoid colon
Typically presents with mild, crampy abdominal pain localized to LLQ
May see “thumb printing” on plain films Most cases resolve with supportive care
References Shields, W. “GI Bleed (what I learned from
Patrick)” July, 2003. Uptodate, of course Zuccaro, G. Management of the Adult Patient
with Acute Lower Gastrointestinal Bleeding. Am J Gastro 1998;93:1202-08.
Barkun, A. et al. Consensus Recommendations for Managing Patients with Nonvariceal Upper Gastrointestinal Bleeding. Ann Internal Med. 2003;139:843-857.