gastroenterology - amsa.org.au meded student... · 1 histology of the git ..……………….. 6...
TRANSCRIPT
This document is a student submission made to the Australian Medical Students’ Association Limited (AMSA). All use is subject to our Terms of Service available at https://amsa.org.au/terms-of-service
Student Submitted Resources
Gastroenterology
Gastrointestinal Medicine & Nutrition
Tarren Zimsen
James Cook University
Last Update: December 2012 | File ID: GASTR2017.02

This document is a student submission made to the Australian Medical Students’ Association Limited (AMSA). All use is subject to our Terms of Service available at https://amsa.org.au/terms-of-service
ContentsGastrointestinal Medicine and Nutrition
1 Histology of the GIT ..……………….. 6
2 Abdominal Cavity and Peritoneum ……………….. 10
3 Histology of the Biliary Tree ……………….. 16
4 GI tract motility ……………….. 21
5 Gastrointestinal secretions and absorptions ……………….. 25
6 Digestion and absorption (CHO / Protein) ……………….. 30
7 Liver digestion and absorption (liver function) ……………….. 34
8 Metabolism of the Liver ……………….. 39
9 Nutritional requirements for health ……………….. 45
10 Nutritional status assessment ……………….. 53
11 Control of food intake ……………….. 59
12 Diet and Disease Management ……………….. 66

1 | P a g e
Study Period 2
Summary notes
2012
By Tarren Zimsen

5 | P a g e
Gastrointestinal
Medicine and
Nutrition

6 | P a g e
Gastrointestinal medicine and nutrition week 1 summary
Histology of the GIT
The human digestive system is effectively one long tube that contains many different subsets all
serving different purposes. As the tube is hollow in a sense, with openings in the oral cavity and the
anus, it is classified as the external environment and thus goblet cells are what secrete into it. The 4
basic layers of GI tract are similar in almost all of its organs except for a few differences.
The basic layers of the GI tract:
(i) The mucosa is the most inner layer and it comes into contact with the lumen. The
mucosa itself is further separated into 3 different layers which are the epithelia, lamina
propria and the muscularis mucosae. The epithelial lining typically has simple columnar
cells however it parts that undergo high abrasive forces stratified squamous epithelia is
also found. The epithelia layer is responsible for a lot of the mucous and enzyme
secretion. The lamina propria underlies the epithelia lining and is a layer of connective
tissue. It has the role of absorbing digested nutrience, supplying the epithelia with
nourishment and defends against bacterial attack through direct lymphatic drainage.
The last layer of the mucosa is the muscularis mucosae which controls fine movement
for example if food gets caught onto the epithelium.
(ii) The submucosa is an areolar connective tissue containing a rich supply of blood and
lymphatic vessels, lymphoid follicles and nerve fibres. The elastic fibres within it allow
the muscle to change shape and retain its elasticity.
(iii) The muscularis externa is divided
into two layers of muscle, the
circular and the longitudinal.
These two layers work together to
produce a smooth muscle
contraction that allows peristalsis.
In certain parts of the GI tract the
circular layer becomes larger to
produce a sphincter.
(iv) The serosa is the most outer layer
of the canal.
The statements that are set out in the above paragraph are general and there are sometimes big
differences. For example in the oesophagus the epithelium layer is actually stratified squamous
instead of simple columnar. This is purely due to the amount of abrasive forces that are in play in the
oesophagus. Another factor that must be noted is that in the oesophagus the skeletal, voluntary
muscle, slowly becomes smooth muscle thus meaning that the person has no control over the
digestion.
Once you get to the stomach the epithelium turns back to simple columnar cells. The stomach also
contains a large amount of goblet cells that help to secrete the enzymes into the vessel. It is the
ducts in the sub mucosa that produce the mucous that lines the stomach and ensures that it does
not undergo any self-digestion. The stomach also has three layers of muscularis externa which

7 | P a g e
allows it to contract in varying manners. The mucosa of the stomach is full
of glands and pits, with different types of glands and pits being placed in
different areas. The length of the pits and glands change as you progress
from the cardia to the body and the pylorus. These gastric pits are useful
for secreting a lot of the HCl that is found in the stomach along with the
enzymes (the stomach releases 2L of gastric juices every day). The stomach
is separated from the oesophagus superiorly and the duodenum inferiorly
by sphincters.
In order to get maximum surface area and therefore maximum absorbance of
food the small intestines have a clever mechanism of increasing its surface area.
First the plicae circularis then the villus and finally the enterocytes all fold in on
each other to create a velvet like appearance, but more importantly increasing
the surface area to 200 sq m. The small intestines is split into three sections the
duodenum which is the closest to the stomach then the jejunum and finally the
ilium. The intestines also contain little inversions into the intestinal wall, these are known as crypts
of lieberkuhn and they carry out the task of secreting intestinal juice that can help the movement
down the digestive tract. In the duodenum specific there is a gland known as the brunners gland
which secretes an alkaline solution to help neutralise the acidic solution that is entering from the
stomach. The jejunum contains the tallest villi which allows for the most absorption. The ileum
contains a layer of cells deep to the epithelium known as lymphoid tissue that is the first line of
defence for micro-organisms that enter the body.
The large intestines are the sight of the major water reabsorption. Because of the decrease in the
fluid content large amounts of goblet cells are required to ensure that the bolus is fluid enough to
transport through. The large intestines is split up into 5 parts: the secum, accending colon,
transverse colon, descending colon and the sigmoid. Another factor that is worth noting is that the
longitudinal layer of the muscularis externa changes to become three tinea coli that helps to great
degree with faecal compaction.
Appendix is an organ that has very little use in humans however can cause great risks.
The rectum must have an even higher number of goblet cells to allow
the faeces to be excreted onto the anus. It contains rectal valves which
allow it to decipher between gas and solid in the rectum. This is crucial
for faecal control. The ano rectal junction shows a quite succinct
transition between the two, with the anus the later purely responsible
with holding the stool in, and the rectum still involved in absorption and
separating solid from gas. The anus is voluntary and the rectum
involuntary.
Rectal valves

8 | P a g e
The regions of the abdomen
The abdomen can either be divided by the four quadrant pattern or the
nine region pattern.
The four quadrant pattern takes one section through the median plane and
one through the trans umbilical plane which separates into right upper, left
upper, right lower, and left lower. What must be noted is that it is the left
and right hand side of the patient not you.
The nine region pattern divides the body down the mid clavicular planes
which run through the middle of the clavicles. The horizontal plains run
through the intertubular plane which is roughly the height of the top of
the ilium. And the subcostal plane which is just under the last rib.
The abdominal wall
The anterior abdominal wall consists of multiple layers from the skin all
the way through to the parietal peritoneum. All these layers work
together to maintain the intra-abdominal pressure and make sure that
the organs stay where they are supposed to stay. The obvious outer layer is the skin; deep to this is
more superficial and the scarpas layer which is deeper. The Campers layer is made predominantly
made of connective tissue whereas the scarpas layer is extremely fibrous. Fat layerings are also
found in this region and thickness varies on the health status of the individual being tested. One
more layer deeper is the deep fascia which has a very large connective tissue medium (aponeurotic=
big tendon). The external oblique comes in which runs anteriorly, inferiorly, and medially. The
internal oblique is one more layer in and it runs anteriorly, superiorly and medially. These muscles
help to allow the body to turn. The next layer in is the transverses abdominus where the fibres run
more or less horizontally. The rectus abdominus run down the middle and are what are defined in a
six pack. The line down the centre of the rectus abdominus is the linea alba. Inside all the layers of
muscle there are two layers of membrane that separate the contracting muscle from the abdominal
organs. The more superficial of the two is the transversalis fascia and the deeper one is the parietal
peritoneum. There are also visce
them to be compartmentalised.
The posterior abdominal wall is also crucial in maintaining the intra-abdominal pressure. The
muscles that play a role in the posterior wall are the psoas major, the quadratus lumborum the
transersus abdominis and the iliacus.
The roof of the abdominal cavity is the diaphragm. It is the primary muscle that is involved in
breathing for the human. Its contraction and relaxation helps to create pressure differences that aid
in breathing. It is said to be a musculartendinous partition as the central tendon is surrounded by a
muscle. The tendon stretches and relaxes to allow for the expansion of the lungs. The diaphragm has
three foramens in it. The vena cava goes through one of the foramens through the tendenous part
of the diaphragm at T8. The Oesophagus goes through the muscular portion at T10 and the
diaphragm helps to create a sphincter. The last vessel that comes through the diaphragm is the
abdominal aorta which comes down the back at T12. The abdominal aorta feeds the phemoral artery

9 | P a g e
which feeds the legs along with all other abdominal organs. There are multiple vessels that leave the
abdominal aorta and not all are symmetrical.
The lymphatic drainage of the posterior abdominal wall is described quite simply. The ciliac
mesenteric lymph nodes drain the top, then the superior mesenteric lymph nodes drain the middle
umbilicus region, and the inferior mesenteric lymph nodes drain the bottom.
The nerves that exit the spinal cord must get through the psoas major muscle and both the lumbar
plexus and femoral nerves do this.

10 | P a g e
Gastrointestinal Medicine and Nutrition week 2 summary
Abdominal Cavity and Peritoneum
The peritoneum is a think membrane that lines
the abdominal wall. Other types of peritoneum
also line the organs in the GIT. The peritoneal
cavity which is defined by the diaphragm
superiorly and the pelvic cavity inferiorly is
divided into a greater and lesser sac. The two
sacs are continuous (joined) through the
omental foramen. The abdominal peritoneum
gains its blood supply from the vessels that
support the abdominal wall, whereas the
visceral peritoneum gains their blood supply
from the vessels that supply the individual organs. The visceral peritoneum is developed through
endocytosis like engulfment of the organs during
development. It must be noted that not all parts of the
digestive system have peritoneum and other ligaments
holding it together. Some parts are completely free to
move. The image right highlights the parts that are
attached on the left and the parts that are free moving
on the right.
Mesenteries are peritoneal folds that attach the
viscera to the posterior abdominal wall. The mesentery is associated with the small intestines; it runs
from the ilium and the jejunum junction to the duodenum jejunum junction. It contains 2 layers of
connective tissue with varying amounts of accumulated fat depending on the person. The transverse
mesocolon is associated with the transverse colon and it connects this to the posterior abdominal
wall. The double layered connective tissue leave the posterior abdominal wall near the head and
body of the pancreas and then head down to surround the transverse colon. The sigmoid mesocolon
is associated with the sigmoid colon is an inverted V shape that attaches the sigmoid colon to the
abdominal wall.
On top of these three mesenteries there are also a lot of peritoneal ligaments that attach
the organs to the abdominal wall. All these are in place to ensure that excessive movement of the
organs in the abdominal cavity does not occur. The peritoneum even folds in such a manner
sometimes to create pouches in the abdomen that other aspects cannot get to. The ligament that
runs down the middle of the liver is known as the palistone ligament.
Omenta are a 4 layered piece of
peritoneum that runs like an apron down the front
of the abdominal organs. It runs from the lower
part of the stomach to the jejunum and ilium. The
width of the omenta varies depending on the
amount of body fat stored in the individual.

11 | P a g e
Torsion is when organ spins on an axis. This can be detrimental to the health of the organ
and the individual as the blood vessels that feed into the organ may not allow the organ to stay
alive.
The mouth: is the site of the initial digestion of the food. The digestive system in a human being is
basically a system that is tasked with disassembly. In the mouth mechanical digestion occurs through
the physical nature of the food being grinded by the teeth, and chemical digestion of the enzymes in
the salivary glands working to digest the food.
The salivary glands (p 1044 1047 Grays anatomy)
The salivary glands are important in human food digestions as they allow the chemical
digestion to occur in the mouth. They are mostly small glands in the mucosa and submucosa of the
oral epithelial lining. There are three relatively large glands known as the parotid, which is found
sublingual glands is at the base of the mouth.
Once out of the mouth the food passes through the pharynx and the thoracic oesophagus. The food
is then moved down the oesophagus through a process called peristalsis into the stomach. The
oesophagus is approximately 25 cm long and cuts through the diaphragm at vertebrae T 10. In the
oesophagus there are compressions that are present due to other vessels in the region. One
constriction is due to the presence of the aorta and the other is due to the
left main bronchus.
The stomach is the next organ in the digestive system; the lower
oesophageal sphincter stops the bolus of food from going back up the
oesophagus from the stomach after it has passed. When the sphincter fails
is divided into four parts; the cardia, the fundus, the body, and the pyloric.
The inside of the stomach contains a structure known as rugae which is
present to allow the stomach to be able to expand when large meals are consumed. In the linning of
the stomach you get mucosal folds that secrete the mucous to ensure that the pepsinogen that is
also s -digest and eat away at the stomach lining. It is the goblet cells inside these
glands that secrete the mucous, the parietal cells that secrete the HCl and the chief cells secrete the
enzyme pepsinogen which becomes pepsin in the highly acidic stomach.
The small intestines are the next organ along in the digestive tract. The small intestines have
the chief responsibility for absorption and hence they have large numbers of villi to increase the
surface area. The small intestines are linked to the stomach through the pyloric junction and as soon
as the bolus of food enters the small intestines it must be treated
by an alkaline solution to neutralise. The alkaline is secreted from
es from
mechanisms. The small intestine is split into three sections in total
equalling 6 or 7 metres.
(i) Duodenum is the first part of the small intestines, it is
quite short, and contains the highest number of plica

12 | P a g e
intestines is also where the bile from the gall bladder and the
pancreatic juice enters.
(ii) The jejunum; is next and is often empty it has a larger wall
and more prominent plicae circularis than the ilium. It also
contains a less prominent arterial arcade and longer vasa
recta. The jejunum makes up approximately 2/5 of the small
intestines
(iii) The Ileum is the last part and makes up about 3/5 of the small
intestines. It contains very little plica circularis and this
structure is completely absent towards the end. It contains a
large number of lymphoid tissue to defend against infection. It
also contains a lot more pertinent arcade of arteries with much
shorter vasa recta
The large intestine is the next component in the digestive system. It effectively frames the small
intestines beginning from the iliocecal and ending at anus. The large intestines are around 7 cm in
diameter and plays a crucial role in absorbing water prior to faeces are created. The wall of the large
intestines must contain large amounts of goblet cells to help with the flow of bolus through the
system. The bolus would now be incredibly hard especially after the water has been taken out. There
are three characteristic features of the large intestines. firstly the tinea coli which is a muscle that
runs along it is present instead of the longitudinal layer of the muscularis externa. Secondly the
presence of haustra which are the bumpy external of the large intestines are present. This structure
is not found anywhere else and has a role to play in faecal
compaction and making faeces that particular shape. The third
is the epiploic appendages which are accumulations of a fat that
are attached to the haustra. These three features tell the
examiner whether the piece they are looking at is the small or
large intestines. The sheer fact of determining the difference
through size can sometimes be dangerous, as depending on the
time of the last meal of the deseased different areas may be
larger. The large intestine is made of seven parts: the cecum
and appendix, the ascending colon, the transverse colon, the
descending colon, the sigmoid, the rectum and the anus.
- The cecum (secum) is the first part of the large
intestines; it is joined to the ilium of the small intestines through the iliocecal valve. The
appendix opens into the cecum at the iliocecal junction.
- The role of the appendix is unknown; however it can cause enormous
amounts of discomfort if the patient gets appendicitis. It is narrow
and wormlike, with its own mesentery. It contains tinea coli that
converge at its base. The appendix can be found in varying different
orientations, sometimes even inside the cecum.
- Large Intestines: is a continuation of the cecum, it runs up the body in
the ascending colon, across the top of the small intestines in the

13 | P a g e
transverse colon, and descends down the left hand side of the patient. The sigmoid is the
end of the colon and runs from the pelvic brim to the S3, and its S shape helps to store
faeces until defecation.
- The rectum is continuous with the sigmoid. The rectum and the anus play a crucial role in
controlling defecation. They both contain a sphincter that works in opposite ways. The inner
sphincter is involuntary and is contracted until an adequate amount of faeces builds up. At
this point the muscle relaxes letting the faeces through. The outer sphincter which is usually
relaxed must then contract. The outer sphincter is voluntary and hence people have control
of their bowel movements. The two sphincters work in opposing natures to each other.
The digestive system is divided into three distinct portions; a foregut,
midgut and a hindgut. The foregut by name is the most superior of the
three, the midgut is in the middle and the hindgut most inferior. The
foregut is made up of the liver, stomach, spleen, and pancreas, the midgut
is made of the small intestines and the ascending and transverse colon,
while the hindgut contains the descending colon, sigmoid and the rectum
and anus.
Arteries that supply the GIT
The celiac trunk that branches off the abdominal aorta, further branches
off to feed the foregut. It splits into the left gastric artery, the splenic
artery and the common hepatic artery. The other two arteries that extend
away from the abdominal aorta are the superior mesenteric artery which feeds the midgut and the
inferior mesenteric artery which feeds the hindgut.
Other information regarding vessels in the abdomen (add after SS use greys to formulate notes)
- Left Gastric Artery: supplies the abdominal oesophagus
and travels along the lesser curvature of the stomach to
supply the lesser curvature side. The left gastric artery is
the smallest of the three vessels that originate from the
cilia trunk. The left gastric artery anastomoses (joins
together to form a circle) with the right gastric artery. The
advantage of having anastomoses is that it allows the
vessels to get around clots etc.
- Splenic artery: is one of the branches of the celiac trunk. And passes over the margin of the
pancreas. The pancreoduodenal artery from the splenic artery supplies the pancreas. The
splenic artery vessel that actually feeds the spleen must
have a little slack in the vessel as the spleen that is sitting
directly under the diaphragm moves up and down, hence
requiring the slack in the vessel. The splenic artery also
gives rise to the left gastro-omental artery which supplies
the greater curvature of the stomach. It also anastomoses
with the right gastro-omental artery to allow for this. The
splenic artery also gives rise to the short gastric arteries

14 | P a g e
which supply the fundus of the stomach. The end of the splenic artery penetrates the hymen
of the spleen and feeds it with blood supply. Note that
it is important that the pancreas has a sufficient blood
supply as the secretion of insulin and the control of
blood glucose is dependent on it.
- Common Hepatic Artery: it gives rise to the right gastric
artery, the hepatic artery proper which leads to the liver
itself, and the gastro-duodenal artery which feeds the
duodenum. The hepatic artery along with the bile duct
and the carpel vein travel along the free edge of the
lesser omentum.
- Superior mesenteric Artery: supplies the small
intestines after the duodenum, the asceding colon and the first two thirds of the transverse
colon. The meso-appendix artery feeds the
appendix. You have duodenal arteries, iliac arteries,
jejunal artery, middle colic artery and the right colic
artery.
- Inferior mesenteric artery: comes out of the
abdominal aorta at around L3. It covers the last third
of the transverse colon, as well as the descending
colon, rectum and anus.
- Venous Drainage: the inferior mesenteric vein, is
supplied by all the structures that were fed by the
inferior mesenteric artery. The inferior mesenteric
vein however drains into the splenic vein and then
the hepatic portal vein, as all blood coming from the digestive
system with new nourishment must go through the liver first.
The superior mesenteric vein drains all the structures that
were fed by the superior mesenteric artery. They all come
together to form the portal vein. The portal vein sits in the
free margin of the lesser omentum.
- Lymphatics: there are three main lymph nodes that are the
celiac, inferior mesenteric, and superior mesenteric lymph
nodes similar to the vein they all line up. However they all
drain into the
cistern chyli

15 | P a g e
Innervation (nerve input)
The entire gastrointestinal tract is supplied by the
autonomic section of the system. There are afferent neurons that
respond to chemical stimuli, mechanical deformation and radial
stretch. There are heaps of nerves that are intertwined into the
submucosa and the muscularis layer. When the body is in its fight
or flight mechanism the body prioritises away from the digestive
system. It is sympathetic nerves that feed the gastrointestinal
tract. So both enteric (sensory cells) pick up information and
autonomous (motor) neurons provide the changes.
Referred pain: is the fact that sometimes the sensory nerve that
feeds the internal viscera are connected to the brain with an external part of
the skin. This is why a person with appendicitis will present with pain around
the umbilicus region and not where the actual appendix is present. The brain
the appendix gets so swollen that it is moving other viscera triggering other
sensory input. In the same note this is why people with heart attacks
complain of pain under their left arm.
Draw up a flow chart that details the abdominal arteries

16 | P a g e
Gastrointestinal Medicine and Nutrition week 3 summary
Histology of the Biliary Tree
Other than the main gastro intestinal tract that is
effectively one long hollow tube that breaks down
food, there are also many other organs that aid in
digestion known as biliary organs. These organs
include the Liver, pancreas, gall bladder, and spleen,
and they all play a role in aiding the digestive process.
The liver: is the largest organ in the body and it makes
a peritoneum which gives its appearance however does contain a bare area underneath the
coronary ligament is flush against the diaphragm. The liver is connected to the other parts of the
body by various ligaments. Firstly the falcciform ligament that runs
down the front of the liver separating it into left and right attaches
the liver to the anterior abdominal wall. An extension from the
inferior end of the falciform ligament is the ligamentum terres
which runs from the bottom of the falciform ligament to the
umbilicus. Secondly, there are left and right triangular ligaments
that attach the liver to the diaphragm. The liver is not only
separated into left and right sections with a Quadrate and Caudate
lobe being present as well. It is the inferior vena cava that burrows
into the liver that actually separates left and right.
As the liver has the function of cleansing the blood that comes from the gastrointestinal
tract it has two very different supplies of blood. One is the blood from the hepatic portal vein that
comes straight from the GI tract for cleansing, and the second is from the hepatic artery proper
which provides blood that is required for the liver to survive. The
term portal literally means that the vein is in between two beds of
capillaries, in this case the capillaries of the GI tract and the
capillaries of the liver. 70% of the blood that the liver receives is
from the hepatic portal vein, and only 30 % from the hepatic artery
proper. It receives about 1.5 L of blood per minute.
The arterial support comes from the common hepatic, then
the hepatic artery proper and then the left and right hepatic arteries
which go on to feed the left and right parts of the liver. From here
capillaries are formed obviously, and the veins system is very similar
just in reverse. The blood flows into the hepatic veins which then
lead to the inferior vena cava to head towards the heart. The
hepatic portal vein which supplies the liver with blood from the GI
tract has multiple branches that lead into it including the splenic vein, the superior rectal vein, the
superior and inferior mesenteric veins, and the superficial veins of the abdominal wall. The liver has
the 3 main roles in human function: store glycogen, clean blood and create bile. The vessels that

17 | P a g e
feed the body these three things all originate from the part of the liver called the porta hepatis
where the hepatic artery, the hepatic portal vein, and the
hepatic bile duct all leave the liver.
Histology of the Liver: At the most basic level the liver is
composed of lobules, that each have a hexagonal structure.
Each of the lobules contains a central vein with all the
hepatocytes leading in towards it. Where the three
hepatocytes meet you get a portal triad which contains three
vessels; a portal venuole, a bile duct, and a lymphatic arteriole.
At the portal triad you get these structures but it must be noted
that the vein is a lot larger than any of the other vessels due to
the purpose of the liver. The bile duct is made of simple
cuboidal epithelium. The bile in the liver is actually produced in
the hepatocytes however it dlowly drains to larger and larger
canals in the liver until it reaches the bile duct. It must be noted
that bile and blood flow are generally in opposing directions.
The Gall Bladder: is a sac that is found inferior to the liver, at it has the function storing the bile that
the liver produces and concentrating it so that it has a more potent effect on emulsifying the fat. The
gall bladder is divided into the body neck and fundus. The gall bladder is stimulated when a bolus of
food reaches the duodenum; this stimulates the release of cholecystokinin which further stimulates
the release of bile from the gall bladder. The bile enters the duodenum
and emulsifies the fat which makes it a lot easier to digest by the lipase
enzymes secreted from the pancreas.
Histology of the Gall Bladder: the gall bladder histologically consists of a
folded mucosa of simple columnar epithelial cells with underlying fibro
vascular lamina propria, and a deeper muscularis externa with a layer of
external elastic fibres and a serosa. There is no muscularis
mucosa or sub mucosa.
Gallstones can occur when excess cholesterol enters the gall
bladder and it forms crystals. The gall bladder must then be
removed from the patient. High amounts of pain can be created
by the gall stones, and the loss of it through the cholecystectomy
is usually well tolerated in humans.

18 | P a g e
The Pancreas is a vital organ in the human body it is a secretory gland that has two vital roles. It
provides both endocrine and exocrine hormones. The endocrine function of the pancreas is the
insulin and glucagon that it produces that are supplied into the blood stream to help manage the
levels of the blood glucose. The exocrine function is
the plethora of digestive enzymes that it produces
to help breakdown the food that we eat. The
pancreas is divided into a head (surrounded by the
duodenum) a neck a body and a tail, and is also
said to be retroperitoneal. It sits slightly posterior
to the stomach and the
tail All the pancreatic
enzymes that are fed ito the duodenum are transported through small
vessels until it meets the main pancreatic
duct where it is led to the duodenum.
Histologically the pancreas is divided into
two distinct areas based on whether it is
supplying the endocrine or exocrine
function. The islets of langerham which only make up
approximately 1-2% of the pancreas by weight is where
the glucagon and insulin is produced. The other portion of
the pancreas produces the digestive enzymes. Many of
the enzymes that are produced in t
operate in the pancreas. These enzymes are only activated when they reach the basic pH of the
duodenum and this is a clever ploy by the body to stop self-digestion.
The Spleen is the final organ that is discussed it is a large soft vascular lymphoid organ. The spleen
has large immune qualities, and is an organ that is used for a lot of lymphatic
drainage. The spleen is fed by large quantities of blood and hence when it is
ruptured it does bleed profusely. If the spleen is ruptured in a child an
attempt will be made to repair it (due to its immune qualities), however if
the rupture occurs in an adult the spleen will simply be taken out in a
spleenectomy. The spleen is simply fed by the splenic artery and drained by
the splenic vein. An easy way to remember the spleen is that it is 1 inch
thick, 3 inches wide, 5 inches long, 7 ounces, and lies between the 9th and
11th ribs.
Synthesising Session Notes: Development of the GIT and the inguinal region
The very primitive Gut lining is shown right. You are able to identify the
three main blood vessels that supply the abdomen of the individual. The
cloaca is an embryonic derivative that disappears as the individual fetus
matures. By week 8 of the embryonic development all main organ
systems are in place, however in a very unrefined state. The liver of a
fetus is also very much larger than that of an adult.
Islet of
langerham

19 | P a g e
During the development the trachea and the oesophagus are both one tube
that eventually becomes two through the trache-oesophagial folds coming in
on both sides and forming the two pipes (see image right). The respiratory
diverticulum, gives rise to the trachea and the bronchi which lead to the
lungs. Sometimes during development the two
m properly, leaving pathways
between the two. This can be life threatening
and requires immediate attention. By week 7 of
development the relative length of the
oesophagus is formed.
In the stomach development, initially the stomach is facing anteriorly
however it turns during development to form the lesser and greater
curvatures. The posterior portion of the stomach develops faster than
the anterior section, prior to turning. It rotates in a clockwise
direction 90 degrees. This is what explains why the Vegas
nerve serves the stomach. The duodenum develops in the
curved part because it runs out of space. The duodenum is
formed from both the foregut and the midgut, and hence the
proximal portion is fed by the celiac trunk and the distal
portion is fed by the superior mesenteric artery. The common
bile duct penetrates into the duodenum. The duodenum
becomes retro-peritoneal. During the early parts of
pregnancy the cells in the duodenum proliferate so rapidly
that the duodenum actually becomes slightly blocked.
However just prior to the birth it clears up.
The liver and the gall bladder both come about from a
small ventral outgrowth from the foregut, and they are
therefore fed by the celiac artery. The liver is relatively a
lot larger in a developing foetus than an adult. The liver
releases bile from week 12, and therefore must go through
enormous amounts of growth extremely early. At about
week 6 the liver makes up 10% of the weight of the baby.
The image right has the different levels of development,
weeks 5, 6, 7, 8. The pancreas also undergoes extremely
rapid development.
The midgut loop enters the umbilicus region during development because it runs out of space to
develop in the abdomen. It then turns to re-enter the abdominal
cavity. The small intestines go around forming the foiled structure.
The hindgut also develops simultaneously in their own fashion shown
right.

20 | P a g e
The Inguinal region
In a male the testes must migrate from their position high in the abdomen to the extremities for
effective sperm production. While it migrates south it drags with it layers of the abdominal wall that
become part of the scrotum. However by protruding through the abdominal wall potential defects in
the wall form which can later end up in a hernia that requires surgery. The layers of muscle that are
moved through the migration of the testes are the transversalis fascia, the internal oblique muscle
and the external oblique muscle.
The inguinal canal is the pathway that the male spermatic cord takes, as well as the female round
ligament. There are two inguinal canals one on each side of the body. They are formed through a
deficiency in the transersus abdominus muscle.
The spermatic cord contain (look into HB notes) the ductus deferens the testicular artery, the
pampiniform plexus, cremaster artery and vein, nerves, lymphatics, and procesus vaginalis
remnants.
1. Direct Hernia is where the abdominal contents pushes down of the pariental peritoneum,
2. Indirect Hernia is where the abdominal contents gets pushed into the inguinal ring, and the
scrotum. In these cases you can get small intestines in the scrotum.

21 | P a g e
Gastrointestinal Medicine and Nutrition week 4 summary
Gastrointestinal (GI) tract motility
As detailed in previous the Gastrointestinal Tract is a single long tube that extends from the oral
cavity all the way down to the anus. It has the primary function to supply nutrience to the body and
excrete waste products. The GI tract works at around an efficiency of around 90%. The primary role
of the nutrience that the body consumes is for looking after the basal metabolic rate, the second
priority is towards growth and finally fat accumulation.
The principle function of the gastrointestinal tract is achieved through motility and
secretion. These two aspects must be controlled carefully, to ensure that the body is able to take in
the full amount of nutrience from the body. Homeostasis must be maintained in the lumen of the GI
tract, and homeostasis for different parts of the GI tact is obviously different. Maintenance of the GI
tract integrity is also crucial due to the very unsavoury environments that are included in it. The
maintenance of the GI tract is hard. The GI structures are orchestrated by both neuronal and
hormonal signals.
The pH value of the mouth is between 6.4 and 7.3; the stomach has a pH of around 1.5 to
4.0, whereas the duodenum has a pH value between 7 and 8. And these pH values are crucial for the
maintenance of certain enzymes as they only work at certain pH.
The transit time for certain portions of the GI
tract is as follows. The oesophagus is between 5 and 10
seconds, the stomach 1-3 hours, the small intestines 7-9
hours and the large intestines 25-30 hours. These
numbers can change however; the fattier in the food
the longer that it is in the small intestines. The word
chime refers to the mixture of food and digestive
enzymes and mucous in the bolus of food. Other factors
can change these values, such as stress, illness, and
diet.
The sphincters in the body are as follows
- The upper oesophageal sphincter is between the pharynx and the proximal part of the
oesophagus.
- The lower oesophageal sphincter is between the oesophagus and the stomach
- The pyloric sphincter is from the stomach to the duodenum
- Iliocecal valve is the junction between the ileum and the cecum (or the small and large
intestines)
- On top of this there are two sphincters in the rectum: the internal anal sphincter and the
external anal sphincter. The internal anal sphincter is smooth muscle and the external one is
skeletal muscle (allowing for conscious control).
Pace maker zones:
1. In the stomach it is found in the fundus sets the peristalsis: 3 per minute

22 | P a g e
2. In the duodenum: sets the rate of segmentation: 12 per minute
3. Transvers colon: one every 30 minutes
There are three temporary storage zones in the GI tract: the stomach, the proximal colon and the
rectum. There are no other temporary storage zones.
Motility in the GI tract, is necessary for many reasons. The muscle both relaxes and
contracts, to help with these factors. The following are resons for GI motility:
- Mixing the digested food
- Contact between digest and cells
- Propulsion of digesta
- Restriction or propultion in a region of the GI tract
- Restrict back flow
- Facilitate adaptive reflex
The stomach has a great ability to stretch with the about of food
that is within it. It can increase is size for a certain extent without
the pressure of the stomach going up, and then after that the
pressure goes up drastically. This is detailed in the graph right.
Tonic contraction is the continued parcel contraction of
the muscles, this can be found in the oesophagus, which is
continually toned and after the bolus of food goes through it
loses tone and then goes back to normal. It must be noted from
this that the GI tract elongates greatly after death due to the
lack of tone. The sphincters are also termed through a tonic
contraction. A difference between a toned and an untoned
sphincter can be seen.
Segmentation is the contraction of your circular
muscles in the muscularis externa layer. The main function of
segmentation is mixing the food as the food gets pushed together
more effectively. It is also involved in slow food propulsion. These
segmentation contractions are only known as segmentation in the
small intestines, in the large intestines it is known as haustral
contractions.
Pendula is the contraction of the longitudinal muscles and
peristalsis is the coordination of segmentation and pendula.
Peristalsis has three different names for the three
different regions: in the oesophagus and the stomach it is known
as peristalsis. In the small intestines it is referred to as the migrating motor complex. IN the large
intestines it is known as mass movement (MM). in the rectum it is the defecation reflex.
The reflexes that are found in the digestive system those are present to ensure that
feedback of the position of the digestive tract is under control. The reflexes are split into receptive

23 | P a g e
and adaptive reflexes. There is a receptor in the mouth that detects increase in contents, which
sends a message through the Vagus nerve to the medulla oblongata for processing. Which then
sends out a motor response to the lower oesophageal sphincter to relax and open, a very little
accommodation reflex is also stimulated in the stomach. The neuro transmitter for these processes
is acetylcholine. Next stretch receptors in the lower oesophageal sphincter detect that again send a
message through the vagus nerve to the brain and back
to open the sphincter. Once it is past the stomach the
enteric nervous system takes over to control the digestive
system.
The stomach does not release all the contents
that it contains at once as the acidic properties if it will
have very big consequences in the duodenum. A very
little is allowed into the duodenum at each of the
contraction (3 per min). Small ejaculations from the
stomach are created to allow for appropriate
neutralisation time is necessary to maintain the integrity of the duodenum. Another factor that must
be considered is that the duodenum cannot hold that much food, that is so hypertonic that would
has entered the duodenum to neutralise the pH and get it to duodenal enzyme friendly levels.
Add in the images of the pacemaker zones. It must be noted that you sometimes get food
moving backwards due to segmentation.
Notes from the GLS
The functions of oesophageal motility is to ensure that the food is propelled in a downward direction
and stop upward flow more commonly known as reflux or heart burn. The digestive system must be
controlled carefully through the Vagus nerve to ensure that the sphincters open and close at the
right time. You can have a receptive response like the one to open a sphincter or an accommodation
response to allow the food to sit. Once food reaches the end of the oesophagus proprioceptors in
the smooth muscle layer detect pressure and send a message to the brain and back to open the
sphincter. A similar concept occurs in the stomach once food enters it and the proprioceptors detect
an increase in pressure messages are sent for the stomach to enlarge to accommodate more food.
The stomach has many features
including the action of peristalsis. Only small
quantities of food are ever injected from the
stomach to the duodenum, as the extreme
acidic environment of the stomach would be
harmful to the duodenum. The wave that is
created in the fundus migrates down the
stomach and ends in the pylorus. The Pyloric
valve in this motion plays a vital part as to not let through food, but to also ensure that the contents
of the stomach get thoroughly mixed. When a person vomits it is usually due to the contents of the
stomach creating too high a pressure, this stimulates the gastro-oesophageal sphincter to relax and
the soft palate to cover the nasal cavity. It is usually due to excessive pressure in the stomach,

24 | P a g e
bacterial toxins, excessive alcohol or spicy foods. After vomiting since a lot of the stomach HCl is lost
the blood of the individual becomes alkaline in an attempt to compensate. It must be noted that it is
the three layers of the stomach that allow for it to create peristalsis in such an oddly shaped organ. If
gastric emptying is not well regulated it can create issues of self-digestion of the duodenum and
osmotic problems in the duodenum.
The control of the release of food into the small
intestines from the stomach has both hormonal and neural
input. The diagram right highlights these inputs in a well-
constructed out diagram. But basically what happens is: when
the presence of hypertonic chime in the duodenum is detected
two simultaneous pathways are stimulated. Firstly entero
endocrine cells secrete enterogastrones which decrease the rate
of emptying in the stomach. Simultaneously, chemoreceptors
and stretch receptors target via the enteric nervous system as
well as the CNS centres to decrease the contractile emptying.
Gastro Oesophageal Reflux: or GOR is a condition where gastric
contents flow up through the oesophagus through the lower oesophageal sphincter. GOR is usually
prevented by many factors including: gravity, Lower oesophageal
sphincter pressure, oblique course of the gastro-oesophageal
junction, and gastric emptying. The sphincter can become
unhealthy due to many factors including smoking and bad diets. If
the regulation of the sphincter and the gastric contraction does not
occur simultaneously there can be a reflux situation created. A
hiatus Hernia can also occur if the sphincter is not operating
appropriately.
GOR is something that is elevated when extra intra-
abdominal pressure created. Intra-abdominal pressure can be created by eating a larger meal, or
being pregnant, or by even undergoing strenuous resistance exercise. GOR is commonly referred to
heart and severe chest pain. The complications those are
associated with GOR if it is remains untreated for a long
period of time, is stricture and Barrett oesophagus. These
are both occurring when the cells tissue of the oesophagus
in the lower oesophagus sphincter die and the new tissue
that forms is scar tissue. This creates really painful GOR
from then onwards.

25 | P a g e
Gastrointestinal Medicine and Nutrition week 5 summary
Gastrointestinal secretions and absorption
Functions of secretion are divided into three different categories, proteins ions and water. One of
the major functions of GI secretions is to maintain the homeostasis in the GI tract and ensure that
osmotic pressure is attained. Proteins functions include digestive enzymes, protection and
lubrication of the mucin and the immune-globulins. The ions are present to maintain osmotic
pressure. Acid and Base
properties are important for
different parts of the GI tract for
the function of the enzymes.
Water is the third type of
secretion that is required to help
with absorption of the different
substances.
Some secretory structures
that are present in the GI tract
include: Goblet cells, secretory
crypts such as the crypt of
glands, and finally organs such as the liver and the gall bladder. The goblet cell is obviously
unicellular and it secretes directly into the GIT. You get
multiple different types of duct complexes.
The basic structures of the cells that are
designed to do exportable proteins are extremely
asymmetrical. This is highlighted by the cell below. The
nutrience or anything that needs to be secreted can
come in through the capillary, come through the cell,
into the endoplasmic reticulum and the golgi apparatus,
and then finally the secretion.
The mucous layer in a cell is of vital importance;
it protects the GI tract from self-digestion. Some of the
environments that are found in the GI tract are capable of self-digestion. The mucous is divided into
two layers. The more inner, loosely adhered mucous, and the closer to the epithelium mucous layer
known as the firmly adhered mucous. The loosely adhered mucous can come off and mix with the
food if need be. However the firmly adhered mucous is a lot more important in the protection of the
stomach. It must be maintained to protect from acid burn. Other factors that are present to protect
the lumen include: cell type, compacted cells, quick cell turnover, alkaline mucous, and blood supply.
The destructive forces of the acid secretion mixed together with pepsin. The other harmful
-steroidal anti-inflammatory drug) these are aspirin or neurofen. What
factor that thins the mucous layer is the helicobacter pylori, which is the bacterium that forms peptic

26 | P a g e
ulcers. It is able to spiral through the
mucous layer and is spread through
the sharing of fluids. The bacteria
works by the following manner shown
right. It does not actually eat through
the epithelium however it can eat
away the glue between epithelium
cells. It secretes ammonia which hide
it from the acid in the stomach. This
also has alkaline properties. Stress
and smoking cause extra acid
production as well.
To treat the bacterial infection what can be given are antibiotics to treat the infection.
Neutralising factors will decrease
the acidity of the stomach, and pain
relief for the patient. However a
careful pain reliever must be
chosen because many will have
negative effects in this situation.
Duct cells are found in the
pancreas and they secrete
bicarbonate juice that helps
maintain pH by acting as a buffer.
Membrane transport can be either active or passive. There are detailed notes on this
covered in MTC. Passive Transport includes; osmosis, and facilitated diffusion whereas active
transport is stuff such as the sodium potassium pump.
- Primary Active Transporter: is what creates a gradient and requires ATP
- Secondary transporter: then uses the gradient that has been set up by the primary
transporter for bodily functions.
- Symporter is a protein channel that carries two molecules from one side of the membrane
to the other side. It has the ability of using the energy of transporting one molecule down a
concentration gradient to bring another up the concentration gradient simultaneously. An
example of this is a glucose and sodium Symporter, that bring sodium downs its gradient
whilst at the same time bringing glucose up its gradient.
- Anti-porter in a protein transporter in the cell membrane that takes two or more items in
different directions. The sodium potassium ATPase pump is the primary example.

27 | P a g e
The reasons that we as students are so interested in GI
secretions, is because there is so much of it. There are
enormous amounts of secretions and absorption in the GI
tract and it remains in balance.
Water also plays an important role in maintaining body
functions with roughly 60% of the body weight being
attributed to water. This is why it is so important that the
water gets reabsorbed in the large intestines.
The principle sites of water absorption are the
jejunum, ileum, proximal colon and gall bladder. The bile
that enters the gall bladder is concentrated up to 20 times
and this means that
The principle secretions in the gastric juices are
pepsinogen from the chief cells, acid from the parietal cells,
and intrinsic factor also from the parietal cells. Mucin is also
secreted from the goblet cells to help protect the stomach
from self-digestion. The stomach is protected against acid
by the mucosal barrier and the effect of prostaglandins
which stimulate the secretion of mucin.
GLS-Gastric acid secretion
There are three agonists for acid secretion in the body. Each one plays a different role in the process
and can be manipulated at different levels to get the desired result for the person. Gastrin which is
an endocrine agent acts on the gastrin receptors found on the basement membrane of the cells. It
has the effect of stimulating the release of the hormone Histamine which is a paracrine hormone
that acts on the local area cells. Histamine attaches to the H2 receptor which stimulates a chain of
events inside the cell using cAMP pathway to secrete HCl into the stomach. The third mechanism
that can be used to increase stomach acidity levels is through the nervous system using the
neurotransmitter acetylcholine pathway. Acetylcholine is released from the Vagus nerve and it acts
on the acetylcholine receptors to utilise the CAM pathway to release HCl into the stomach.
There are also a variety of drugs that can be taken to reduce acid secretion. These are useful to be
taken when a person has a stomach ulcer or is secreting to much HCl naturally. Ranitidine is a drug
that blocks the histamine from binding to its H2 receptor. This will stop the pathway through the
cAMP that is used through the histamine. Acid secreation will not come to a halt however when this
drug is being used, as the acetylcholine pathways is not affected at all. If you want to stop both
pathways the drug omeprazole must be used as it has the ability to block HCl from being secreted.
Substances that enhance acid secretion include pentagastrin that is simply a synthetic form of
gastrin that works in the exact same manner. Caffeine also has the effect of increasing acid secretion
as the it inhibits the phosphodiester enzyme in the cAMP pathway which creates twice the amount
of acid from the gastrin / histamine system that would be usually created.

28 | P a g e
Blood that is leaving the stomach during the stimulation of acid secretion would be slightly basic as
the acidic ions will be stolen from the blood stream to be put into the stomach.
GLS - Control of secretion in the salivary glands, pancreas, gall bladder and intestines
The sublingual glands are found in the mouth and are one of the salivary glands. It secretes mostly
mucous into the mouth. The parotid glands are also a salivary gland in the mouth and it secretes
amylose and amylopectin.
There are three types of cells that are found in the gastric glands.
- Chief cells: secrete pepsinogen and lipases
- Parietal cells secrete hydrochloric acid
- Entero-endocrine cells secrete histamine, serotonin and gastrin
the duodenum is what secretes an alkaline solution in the
duodenum to help neutralise the stomach acid that is entering. In the small intestines you will also
find the crypts of lieberkuhn that secrete intestinal juices to help the chime travel down the
intestinal tract. The crypts of lieberkuhn contain cells deep in the crypts that have the role of
microbial defence. If a bacterium is able to get through the acidic stomach and the basic intestines it
will be attacked by lysozymes and antibacterial enzymes from here.
The gall bladder serves the function to concentrate and store bile. Bile which is a yellow alkaline
solution contains salts, pigments, cholesterol, triglycerides, phospholipids and electrolytes. The bile
plays the role to help emulsify the fats that come through to the duodenum. After the injestion of a
big fatty meal the bile salts return, secretin is then releases which the bile into the duodenum. When
there is little food in the duodenum the bile salts are able to be reabsorbed by the ilium and then
used again. This phenomenon is known as entero-hepatic circulation and is a mechanism that is
useful to conserve energy. In the absence of bile the faeces of the individual will be grey-white in
colour and would have fat streaks through it.
When bile stones accumulate and block the duct, stopping bile from being secreted into the gut, bile
salts are secreted into the blood and deposited on the skin. This deposition creates a disease known
as jaundice where the skin appears yellow. It must be noted that jaundice can also be attributed to
liver problems.
The pancreas is another crucial organ in the digestive system. It secretes pancreatic juice that
contains many vital enzymes in digestion and the maintenance of an effective pH for the duodenum.
Pancreatic juice release is controlled by the enzymes secretin and cholecystokinin. Secrete which is
released due to high amounts of HCl in the duodenum causes the pancreatic ducts to secrete
bicarbonate solution. Cholecystokinin is released in response to excess proteins and fats in the
chime and stimulates the release of pancreatic juice. The entero-endocrine cells that are found in
the duodenum secrete both cholecystokinin and secretin.
Synthesising Session discussion questions (a week overview)
The stomach and duodenum have many to stop it from self-digestion:
the rapid proliferating and tightly packed together epithelium, the mucous layers that protect it he

29 | P a g e
Brunner s gland secreting alkaline solution. Of the three the mucous lining will probably be most
important.
As in the case study if a person has helicobacter pylori and stomach ulcers the treatment plan
bicarbonate to neutralise the stomach and take antibiotics to treat the bacterial infection. Some
factors that increase the chance of stomach ulcers other than the bacterial infection are the
decrease
the amount of stress in the lifestyle. Increased stress levels in a lifestyle create glucorticosteroids
that increases the acid production and in turn can lead to the dereas e of the mucous lining and
therefore stomach ulcers.

30 | P a g e
Gastrointestinal Medicine and Nutrition week 6 summary
Digestion and Absorption (CHO / Proteins)
For a person to survive they must get adequate food from all three sources. Carbohydrates, Proteins
and Fats must all be broken down in the GI tract prior to them being absorbed and then used for
their necessary purposes. It is recommended for people to have a diet that pertains of 45-65%
carbohydrates, 15-25% protein and 20-35% fats.
Carbohydrates are sugar units that come in various different sizes. The term saccharide is the basic
sugar unit, with monosaccharide being a single unit, disaccharide being a double unit,
oligosaccharide being a unit between 2-10 molecules long and a polysaccharide being longer than 10
units. Polysaccharides can further be divided into two groups starch polysaccharides and Non starch
polysaccharides. The non-starch polysaccharides are crucial in wheat and fruit and help with
digestion as they are not digested in the small intestines. There are three monosaccharides: glucose,
fructose and galactose. There are also three disaccharides; maltose,
lactose and sucrose. The major form of glucose that the body receives is
starch. Starch is easy for the body to breakdown as it contains many ends
that are able to be oxidised. The glycaemic index is very closely
associated with this factor of the amount of oxidisable ends. Once the
carbohydrates are broken down they are then stored in the muscle tissue
and the liver, with excess being stored as fats.
When carbohydrates are being digested; there are numerous places that facilitate the
breakdown. The digestion of carbohydrates begins in the mouth; the salivary amylase that is
secreted from the serous cells helps to break down the starch. The pH of the mouth is between 6.3
and 7.3, to enable the salivary amylase to work effectively. There is surprisingly no breakdown of
carbohydrates in the stomach. When the chyme enters the small intestine, the release of pancreatic
enzymes such as alpha amylase acts to breakdown the starch into oligosaccharides and
disaccharides. The trigger for the release of the pancreatic enzymes is in the duodenum.
message travels to endocrine hormones to act on the pancreas that produces the enzymes.
The brush border is the next phase of digestion: the brush border is attached to the mucosa,
they are membrane bound, and this is
why segmentation to produce a
thorough mixing, to allow for the
most amount of absorption. At the
brush border is where the
disaccharides are broken down. The
brush border is highlighted by the
following diagram. In the end you get
the three monosaccharides from the
large starch molecules. You get multi-
functional brush border enzymes that
contain two active sites.

31 | P a g e
Non-starch polysaccharides, as shown in the diagram, do not get digested in the small intestines but
must be digested by micro-organisms in the large intestines. There are bacteria that are found in the
large intestines that help with this
acetate, propionate, and butyrate are formed to be used in the body. There is a lot of gas that is
created in the large intestines every day (some comes out as
flatulents but the majority is absorbed and breathed out).
Carbohydrate Absorption: occurs in both the small and the large
intestines. In the jejunum there are Symporter that are being used
to bring an ion and a glucose molecule at the same time. Glucose
is absorbed straight into the bloodstream, and the levels of
glucose in the blood are controlled by the amounts of insulin and
glucagon that are created. People that are unable to control the
amount of glucose that they have in their blood are termed diabetics. These people either lack the
ability to produce insulin or have lost the ability, hence are susceptible to hyperglycaemia. Diebetics
faint due to either abnormally high or abnormally low glucose levels. Blood glucose levels between
4mM and 8mM are normal levels.
Obviously not all carbohydrates are absorbed by the body at the same rate. The rate at which
carbohydrates are absorbed into the blood is compared on a scale known as the glycaemic index.
Foods that are absorbed quickly have a high glycaemic index and vice versa.
Guided Learning Session
Protein breakdown occurs in 3
main steps; shown right. The pH
sensitive pepsin breaks down
the large proteins into large
polypeptides. Pepsin has the
ability to cleave bonds that are
attached to phenylalanine and
tyrosine, but none of the other
bonds. Pepsin hydrolyses about
15% of the protein.
The pancreatic enzymes
which further break down the
protein are trypsin and
chymotrypsin; cleave the polypeptides to even smaller molecules for the brush border enzymes to
further degrade. The brush border enzymes include: aminopeptidse and dipeptidase facilitate the
final break down of the proteins to the individual amino acid level. Brush border enzymes are
attached to the membranes of the plicae circularis in the small intestines, as they are not free
moving proper gastrointestinal tract motility is important to allow for adequate segmentation and
thus thorough absorption. Since proteins are everywhere in the body as a part of the cell structures
it is vital that they are produced in an inactive state and become active in the GIT. All stomach and
pancreatic enzymes possess this ability and it is crucial to stop auto-digestion.

32 | P a g e
The recommended daily intake for protein is 125 g per day. In this serving it is important
that the individual gets the essential amino acids as the non-essential amino acids can be
manufactured in the body. Animal products are the major source of protein in a human diet and
hence those that are vegetarians must carefully watch their diets to ensure that they get the
adequate foods.
The absorption of protein is through several types of carriers that transport specific amino
acids across the small intestines order. Small chain dipeptides and tripeptides are able to be co-
transported into the epithelium cells with H+ ions. In certain situations small proteins can be
absorbed intact through endocytosis; however this is rare as the entire could be seen as non-self and
hence an immune action may be triggered in the blood. In newborn babies however it is common for
complete adsorption of proteins across the epithelium. This is a mechanism to get the IgA antibodies
ve they some passive
immune ability. As young babies have this ability it is extremely important to keep them sheltered
during the first few days of life as this is when they are susceptible to build up allergic reactions to
proteins that do cross the epithelium and are recognised as non-self.
Synthesising Session: Maintaining GI balance and integrity
Coeliac disease: is where a person is unable to absorb gluten properly. If the person eats too much
gluten the protein (gluten) causes damage to the villi of the small intestines which become inflamed
and atrophy. Digestion and absorption are affected a fair bit by this disease if the person continues
to consume the gluten as the small intestines will not be able to absorb the other foods as
effectively due to the damaged microvilli. People that are coeliac can avoid gluten in their diet and
live a normal life.
Pancreatitis: is a disease for the inflammation of the pancreas, it is caused when the digestive
enzymes which the pancreas secretes get activated in the pancreas itself instead of the GIT. This
causes auto-digestion of the pancreas. Pancreatitis can be caused through severe alcohol
consumption, and other infectious disease. High blood calcium concentration is an indication that
pancreatitis is present, so is raised serum amylase concentration.
Lactose intolerance: is a condition where a person lacks the lactase enzyme in their brush border.
This causes lactose to be not absorbed effectively, and hence it slips through the digestive tract and
causes diarrhoea. People with
lactose intolerance have to avoid
milky products.
Shown right is the varying types of
stool that are created by people;
normal stool in in between 3 and 4.

33 | P a g e
Week 6 Integrative
Treatment of peptic ulcer disease
- Antibiotics are administered to treat the helicobacter pylori infection
- Acid channel inhibitors are also administered to stop the secretion of stomach acid into the
stomach
- Over the counter medication that contains salts as well can make the environment more
basic and less harmful for the patient
- The consumption of smaller more regular meals is advised as well as meals that contain less
fat.
Terminology:
Diarrhoea: an increase in the frequency and fluidity of bowel
movements due to mal-absorption of water. This is tied in with loss of
fluids over time and is usually the first sign of a GI tract disorder.
Constipation: is small, difficult and infrequent bowel movement (less
than 3 stools per week)
Zymogen (pro-enzyme): is an inactive enzyme precursor (such as
pepsinogen is to pepsin)
You can test the efficiency of somebody with poor bile secretion
through the amount of fat that is coming through their stool. Increased fat entering the intestines is
linked to increased chance of colon cancer since their would be greater amounts of abrasion in the
intestines leading to greater amounts of proliferation, and a greater chance of a cancer mutation
occurring.
34 | P a g e
Gastrointestinal Medicine and Nutrition week 7 summary
Liver digestion and Absorption; Liver function
The liver is the largest internal organ in the human body; it weighs on average 1.4 kg in an adult and
has the crucial role of creating bile for fat emulsification, CHO, lipid and AA metabolism, waste
removal, vitamin and mineral storage, and dismantling of RBC.
Bile which is formed in the gall bladder gets stored and concentrated in the gall bladder. The gall
bladder is a non-essential organ as people that have gall stones quite regularly have it removed in a
cholecystectomy. Bile Acids and Salts are derivatives of cholesterol synthesised in the hepatocytes.
Cholesterol is converted into bile salts however when excess cholesterol is present the gall stones
can be formed due to their crystallisation in the wrong place. Bile is secreted in the hepatocytes of
the liver and makes its way through the canaliculi into larger and larger bile channels and to the gall
bladder for storage. When there is fat in the duodenum there is a
chemoreceptor (CCK in the I cells and Secretin in the S cells) that
picks it up this situation and stimulates the gall bladder to
contract, and to relax the sphincter of Oddi, causing bile to be
secreted into the duodenum.
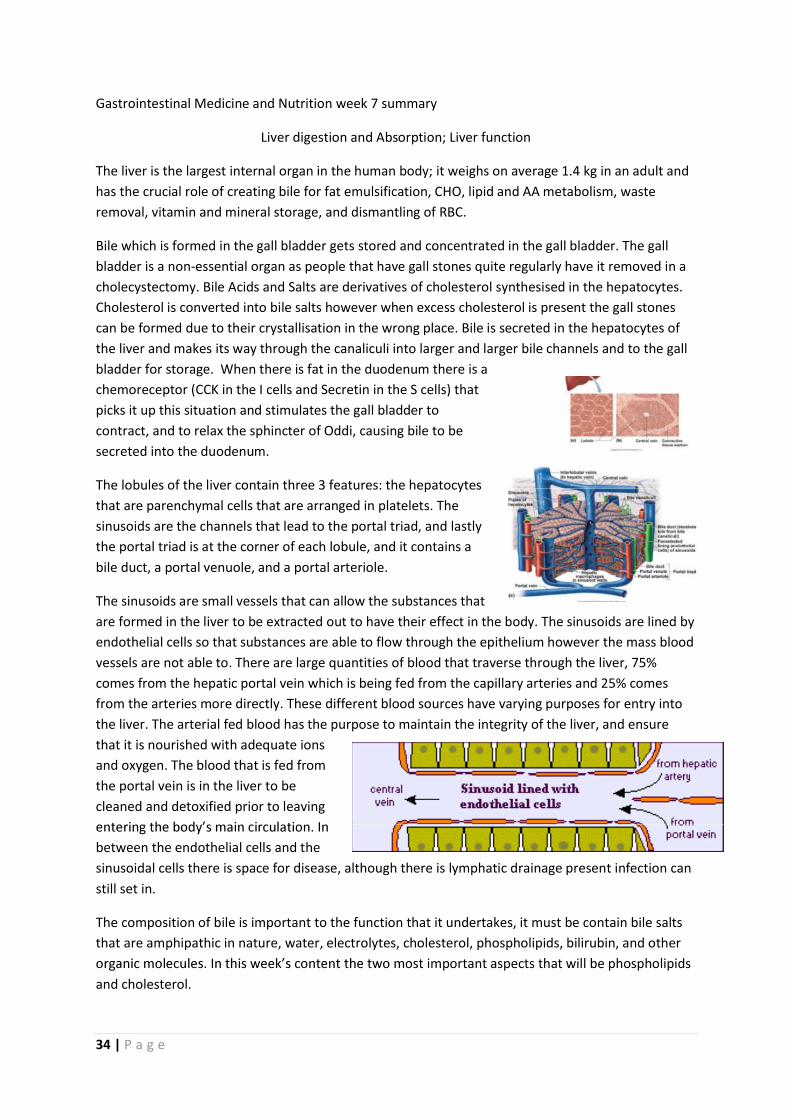
The lobules of the liver contain three 3 features: the hepatocytes
that are parenchymal cells that are arranged in platelets. The
sinusoids are the channels that lead to the portal triad, and lastly
the portal triad is at the corner of each lobule, and it contains a
bile duct, a portal venuole, and a portal arteriole.
The sinusoids are small vessels that can allow the substances that
are formed in the liver to be extracted out to have their effect in the body. The sinusoids are lined by
endothelial cells so that substances are able to flow through the epithelium however the mass blood
vessels are not able to. There are large quantities of blood that traverse through the liver, 75%
comes from the hepatic portal vein which is being fed from the capillary arteries and 25% comes
from the arteries more directly. These different blood sources have varying purposes for entry into
the liver. The arterial fed blood has the purpose to maintain the integrity of the liver, and ensure
that it is nourished with adequate ions
and oxygen. The blood that is fed from
the portal vein is in the liver to be
cleaned and detoxified prior to leaving
between the endothelial cells and the
sinusoidal cells there is space for disease, although there is lymphatic drainage present infection can
still set in.
The composition of bile is important to the function that it undertakes, it must be contain bile salts
that are amphipathic in nature, water, electrolytes, cholesterol, phospholipids, bilirubin, and other
t important aspects that will be phospholipids
and cholesterol.

35 | P a g e
When cholesterol is discussed as of metabolism and creation it is considered as a fat. Cholesterol is
normally created in the liver, and hence people that have cholesterol problems are usually
predisposed to it. However when people have cholesterol issues, a low cholesterol diet is still
advised along with the drugs that have an affect lowering the blood cholesterol.
The gall bladder will concentrate the bile up to 5 times by taking away water from there as
the solution. The bile is modified as they flow through the ducts of the gall bladder in a similar
mechanism to the pancreatic juice. There is an addition of watery bicarbonate secretions as the bile
continues. Adult humans produce on average 500
mL of bile each day.
Enterohepatic circulation is the
reabsorption of the bile through the ileum. Bile can
be recycled 18-20 times this is to ensure that high
blood stream. This is a clever mechanism the body
utilises to decrease the amount of waste bile that is
being excreted in the faeces.
Bile has a vital function in two different roles:
- Bile salts are required for critical digestion and absorption
- Waste products are often removed from the body using bile. They eventually head out through
the faeces. Drugs, Alcohol and a lot of other substances are removed from the body in with the
use of bile. Some compounds that are reabsorbed in the small intestines ultimately eliminated
by the kidney through urine. Bile is also the main way for the body to eradicate excess levels of
cholesterol, as excess levels of galls stones lead to gallstones through the crystallisation of the
gall stones.
Digestion and Absorption of Lipids:
Lipids are a crucial par
supply of dietary fat means that the individual may be at risk of
absorbing the necessary minerals to survive which could be fatal.
or triacylglycerol they usually house the vitamins A, D, E, and K. The
other 5% of the fats that are consumed by the body are the
(triacylglycerols). As fats are insoluble in water they will always stay
together in the watery environment of the small intestines. This is
where bile comes in to play the role to split the fat into millions of
small pieces. The individual units that are covered by the bile salts
are known as micells. This increases the surface area to volume ratio and makes it easier for the
pancreatic enzymes to break down the smaller fat molecules into their respective fatty acids and
glycerols. If the enzymes were eating around one big fat globule then the fat digestion would be a lot
slower. There is a very small amount of stomach, gastric lipase, in the stomach however it is very
minor. The chime is homogenised and released into the duodenum, then the bile is secreted that

36 | P a g e
emulsifies the fat which then allows the pancreatic enzymes to work efficiently. The break down
products is fatty acids and 2 monoacylglycerol. At this stage the molecules are still in a micell stage.
After this when the fatty acids and the 2 monoacylglycerol are actually absorbed by the absorptive
cells or the enterocytes of the small intestines. Once in the enterocytes the endoplasmic reticulum
then simply put the triacylglycerol back together the Golgi body in the cell then adds a protein to be
packaged as chylomicrons. A chylomicron is basically a triacylglycerol with a skin of proteins around
it to get it into the basal membrane of the cell to go into the lymph tissue as the capillaries are too
large. The chylomicrons then enter the blood stream through the left
sub-clavian vein, where it will head to the liver to be processed. The
steps are: emulsification, breakdown, absorption, putting together,
chylomicron, and into the lymph vessel. The process seems very
counter-productive as the triglycerides are simply molecules simply
get smaller and then bigger again, however, the reason for this is to
ensure that they are able to cross membranes with ease.
The crucial differences between lipid breakdown and the
breakdown of CHO and proteins is that there is no brush border enzyme
breakdown of lipids as the lipids would simply be able to slip straight
through the membrane. The enzymes that breakdown lipids are never
membrane bound.
The large molecules of fats are the only ones that get through the
chylomicrons, the smaller fatty acids are able to get into the bloodstream,
and go to the liver. In the liver, you get the triacylglycerols that broken
down into glycerols and fatty acids again. These go into the bloodstream and are transported to the
adipose or the muscle cells where they are required. The remnants of the chylomicrons get broken
down and reused in the liver, they are packaged to produce VLDL (very low density lipoproteins)
which are a lot of triacylglycerols, phospholipids and cholesterol packaged together.
A high density lipid is pretty much a protein shell that does not have any fat; they have the
purpose of going into the bloodstream and collecting cholesterol. The low density lipids are said to
be the bad cholesterol as they can clog the arteries. HDL is good, LDL is bad. There are drugs that can
be placed to stop the digestion of the fats being digested and absorbed. This will lead to greater
amounts being excreted in faeces.
Olestra is a synthetic lipid that makes
food fatty like, however it does not get
digested. This allows people to have
the tasty fatty foods that fill the
stomach for longer; however, the food
goes straight through the system.
The final thing that needs to be
considered is the breakdown of Red
blood cells. It basically happens as per
the following diagram.

37 | P a g e
Notes from GLS:
- Bilirubin must be carried on a albumin molecule in the blood stream as it is not very water
soluble.
- The enzyme in the liver that processes bilirubin is UDP-glucobonate transcarboxylase, it
produces conjugated bilirubin
- The iron in the red blood cell is stored as ferritin and is released back into the blood stream as
required with new RBC
- Jaundice is the yellowing of the skin and is formed by excess levels of bilirubin being found in
the blood. Bilirubin is yellow in appearance and that is why the skin turns that colour.
When there is a hepato-cellular inflammation of the liver, there signs in a blood test for damage are
increased levels of blood albumin, increased levels of bilirubin, and increased levels of lactate
dehydrogenase.
Synthesising Session Biliary Disorders
The term biliary means of or relating to the bile duct, hence a biliary disorder is one where the bile
duct is impeded or damaged is some manner. The major cause of blockage is gall stones which are
cholesterol crystallisations. Other forms of biliary disorders are cancers, autoimmune, and
congenital diseases. Different people are obviously at different risks of getting gall stones, however
the 5 key features that have been attributed to gall stones are: fat, fair, fertile, female and forty.
Obesity and rapid weight loss have been associated with the onset of gall stones, so have increasing
age, pregnancy, and some drugs. It must be noted that in most people gall stones are asymptomatic,
and hence show no signs of pain, only when the stones impede into the pathway of the bile duct do
people require a cholecystectomy.
Gall stones are constantly kept in check by the bile acids, lecithan and the cholesterol.
However when there is super-saturation of cholesterol either by genetic or dietary input the stones
can become too large and out of control. Gall Stones can be divided into separate categories,
cholesterol gall stones contain greater than 80% cholesterol, bile pigment
stones contain less than 20% cholesterol, and mixed stones contain between
20 and 80% cholesterol.
Acute Cholecystitis is infection or inflammation of the gall bladder.
The patient would present with abdominal pain (most commonly right upper
quadrant) that may radiate to the right shoulder or back. The pain is steady
and severe, with associated complaints including nausea, vomiting and
this test you ask the patient to inspire as must as they can and they using
your hands to palpate under the rib cage. People with gall bladder
inflammation would usually have heightened levels of pain or suffering
through this movement. By telling the person to breath in you are exposing the gall bladder the most
since the liver will rise with the diaphragm. When the patient presents they
will usually be voluntarily and involuntarily be guarding the area with their
limbs, they may also often have tachycardia. Once the person is tested

38 | P a g e
thicker gall bladder wall. Fluids and pain relief are administered to comfort the patient as much as
possible antibiotics are administered to treat the potential bacterial infection and once they have
been settled a cholecystectomy is undertaken.
Bile Duct stones (choledocholithiasis) is a slightly different situation where the patient would present
of manners; firstly ERCP can be used to get a thorough understanding of the situation, and then a
cholecystectomy could be used. A
cholecystectomy is simply an intra
operative cholangiogram that leads to
stone removal. ERCP is shown in the
diagram right, the main function of ERCP
is to inject a die that colours the gall
stones so that you can get a very clear X-
ray showing what is in the abdomen. A
small incision must be made to pierce the gall bladder duodenal sphincter, the sphincter of Oddi.
If there are gall stones that are present but they do not obstruct the biliary the patient will still be in
pain however, there will be no liver obstruction thus no inflammation of the liver and in turn normal
blood tests. People that have biliary problems would get greater amounts of pain 3 or 4 hours after
eating heavily fatty meals because the duodenum would be calling for more bile creating the pain.

39 | P a g e
Gastrointestinal Medicine and Nutrition week 8 summary
Metabolism in the liver
The liver has many crucial roles in the human body. It plays as essential role in the management of
glucose concentrations, and maintains homeostasis in the body through periods of starvation and
excess food availability. The liver also has a crucial role in the management of drugs that people take
and when the liver suffers the entire body suffers the consequences. The liver has a very varied role
and that is why people require liver transplants when their liver fails. The liver serves so many
functional purposes with:
- Carbohydrates: as it both stores and secretes glucose into the blood stream as required,
through the processes of glycolysis and gluconeogenesis
- Proteins: synthesis and catabolism, along with amino acid metabolism and urea synthesis
- Lipids: it is involved in lipoprotein and cholesterol synthesis along with fatty acid metabolism
and bile acid synthesis
- Excretion and detoxification: bile acid and bilirubin excretion, drug detoxification, steroid
hormone inactivation and excretion, alcohol metabolism (more than one unit every hour)
- It is also involved in iron storage and Vitamin A, D, E and B12 storage and metabolism.
- Drugs: any type of drug (over the counter, prescription
and illicit) that you put into your system are put
controlled and detoxified by your liver.
The liver is the major controller of food substrates in famine
and in feast conditions. The amounts of glycogen,
triacylglycerols and proteins are all controlled by the liver, and
then are either synthesised or degraded during times of feast
or famine respectively. The liver is able to create glucose
through gluconeogenesis, from pyruvic acid. This pathway can go either way, in famine it will secrete
glucose into the blood to keep you alive, however in times of feast it does not require the glucose in
the blood stream and the glucose 6 phosphates is converted into glycogen.
Drugs: the majority of drugs that are taken are lipophilic so that they can cross the cell
membrane and be active where we want them to be. Because of their lipophilic trait they are unable
to be processed by the kidneys and end up being processed by the liver in a two phase manner. The
first stage is where they go through a
catabolic stage where a hydroxyl or a
methyl group are added in order to
detoxify the drug, this usually occurs
in the smooth intestines catalised by
cytochrome P450 mono-oxygenases.
Stage II occurs in the hepatocytes to
produce an inactive soluble product.
The basic processes of drug
metabolism are detoxification and
then make it soluble to be excreted
by the kidneys. Non polar drugs will

40 | P a g e
simply accumulate in one part of the body. This is why drugs must be taken in the correct
moderation, so that the pathway does not get overloaded, as the particles will build up too much
and the free radicals that are created are not able to be excreted in time creating issues.
Carbohydrate Metabolism: in times of feast we store the glucose, and in times of famine we
obviously use it for energy. 60% of the carbohydrates that we eat are absorbed by the liver to be
placed in to storage pathways. The remainder goes into the blood
stream, which allows glucokinase to phosphorylate glucose,
increased glycogen synthase, increased glycolysis and decreased
gluconeogenesis. When glucose gets absorbed it is almost always
converted to glucose 6 phosphates, and then there are four
pathways that can go from here, detailed right.
Protein Metabolism: the liver is responsible for making a lot of the
proteins in the body, things like albumin and coagulation factor are made in the liver. The amino
acids can be converted to TCA cycle intermediates; however can only be stored in the muscles. The
muscles are sometimes broken down to create energy but
this is only in times of absolute starvation. As amino acids
can only be stored as proteins increased level of protein
uptake is useless unless you are getting muscle damage to
help to get bigger otherwise you are just creating expensive
urine. The proteins that are secreted by the liver include the
ones shown in the table right. There is a difference between
glycogenic and ketogenic amino acids that break down into
glucose intermediates or ketone bodies. These are both able
to be used for energy supply.
Fat metabolism. The liver is responsible for synthesis of
triacylglycerols, synthesis lipoproteins, and synthesis of
cholesterol. Cholesterol is used in the body to help the
fluidity of the cell membrane and a precursor to both
steroid hormones and bile salts. One of the important aspects about fatty acids is that it cannot be
converted into glucose; it must become a ketone body. The liver synthesises ketone bodies to be
used by the body for energy. In human the majority of energy is generated from lipid breakdown.
Lipids are stored as triacylglycerols in the adipose tissue and then they are broken down by lipases to
be used to create energy. They used in
the mitochondrion to create energy. It
is important that lipid levels stay
normal, otherwise the body could use
muscle and to create energy.
Summary of Liver Metabolism: there
are basically three levels that the body
can be functioning under, high energy
substrate levels (straight after meals),
low energy substrate levels (between
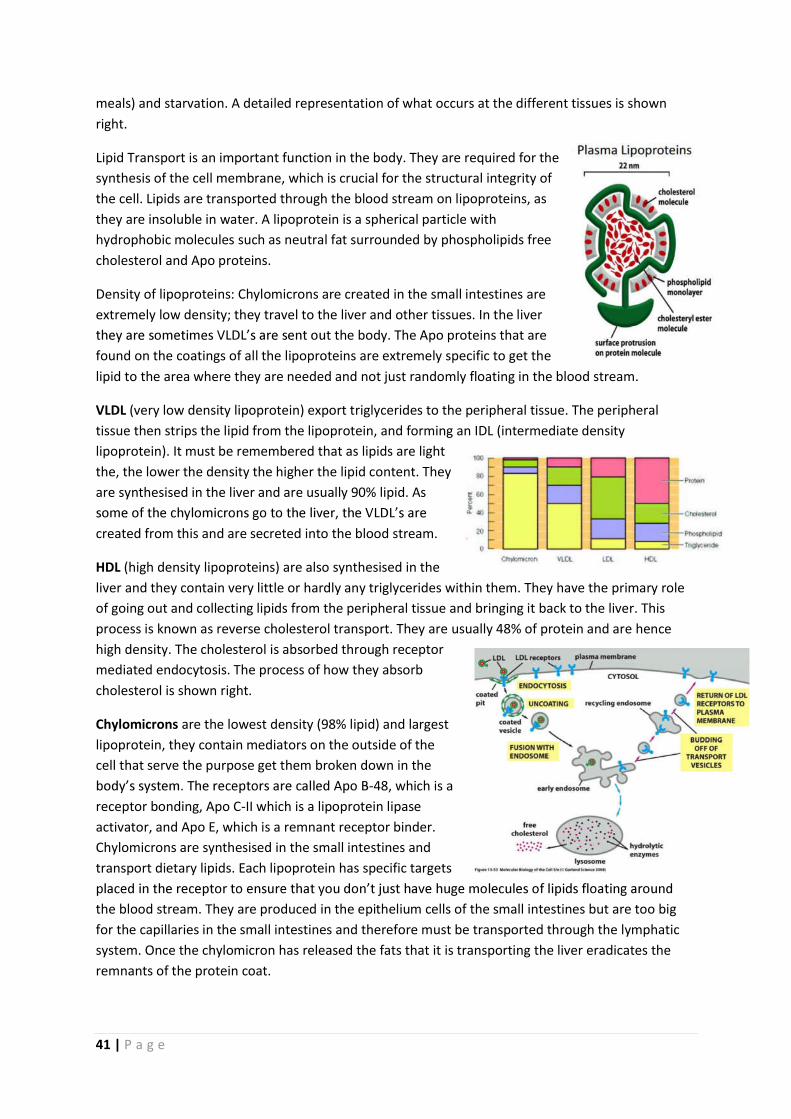
41 | P a g e
meals) and starvation. A detailed representation of what occurs at the different tissues is shown
right.
Lipid Transport is an important function in the body. They are required for the
synthesis of the cell membrane, which is crucial for the structural integrity of
the cell. Lipids are transported through the blood stream on lipoproteins, as
they are insoluble in water. A lipoprotein is a spherical particle with
hydrophobic molecules such as neutral fat surrounded by phospholipids free
cholesterol and Apo proteins.
Density of lipoproteins: Chylomicrons are created in the small intestines are
extremely low density; they travel to the liver and other tissues. In the liver
t the body. The Apo proteins that are
found on the coatings of all the lipoproteins are extremely specific to get the
lipid to the area where they are needed and not just randomly floating in the blood stream.
VLDL (very low density lipoprotein) export triglycerides to the peripheral tissue. The peripheral
tissue then strips the lipid from the lipoprotein, and forming an IDL (intermediate density
lipoprotein). It must be remembered that as lipids are light
the, the lower the density the higher the lipid content. They
are synthesised in the liver and are usually 90% lipid. As
created from this and are secreted into the blood stream.
HDL (high density lipoproteins) are also synthesised in the
liver and they contain very little or hardly any triglycerides within them. They have the primary role
of going out and collecting lipids from the peripheral tissue and bringing it back to the liver. This
process is known as reverse cholesterol transport. They are usually 48% of protein and are hence
high density. The cholesterol is absorbed through receptor
mediated endocytosis. The process of how they absorb
cholesterol is shown right.
Chylomicrons are the lowest density (98% lipid) and largest
lipoprotein, they contain mediators on the outside of the
cell that serve the purpose get them broken down in the
-48, which is a
receptor bonding, Apo C-II which is a lipoprotein lipase
activator, and Apo E, which is a remnant receptor binder.
Chylomicrons are synthesised in the small intestines and
transport dietary lipids. Each lipoprotein has specific targets
the blood stream. They are produced in the epithelium cells of the small intestines but are too big
for the capillaries in the small intestines and therefore must be transported through the lymphatic
system. Once the chylomicron has released the fats that it is transporting the liver eradicates the
remnants of the protein coat.

42 | P a g e
IDL
precursor to low density lipoproteins. They have the same Apo proteins as the VLDL
LDL
here is a Apo B-100, the Apo
proteins keep getting taken off as
the process goes on. The LDL is the
bad cholesterol, because it has a
high level of cholesterol in it, we do
not want too much of it floating
around our boy. HDL are also known
as good cholesterol because they
contain a very low amount of
cholesterol, and they have the role
of going out and collecting
cholesterol and bringing it back into
liver. The receptors that help to
bring the cholesterol in are receptor
mediated, and hence when the cell is full of cholesterol they cut off the receptors and then no other
cholesterol is taken up.
In a healthy cell the level of cholesterol formation and degradation is at a relatively equal level,
however people can have genetic faults or develop problems through life where they lost this
balance causing excess levels of cholesterol to be released into the blood stream. This can cause
major problems. One of these problems are atherosclerosis; where they are unable to uptake the
cholesterol as the receptor is defective. This means that greater amount of cholesterol accumulate
of the outside of the cell, that cannot be digested. This then creates larger and larger lipid balls. This
is shown in the diagram right, with normal on top and
atherosclerosis on the bottom.
Overview of the lecture was the general function of the liver in
the control of homeostasis and the manner in which lipids are
controlled in the blood stream.
Guided Learning Session Notes
- Cholesterol is able to become hydrophilic if it becomes
a cholesterol ester as there will be an OH group on the cholesterol.
- Triacylglycerols are always converted back into glycerol and three fatty acids before they can
be up taken by the cells.
- The liver is described as the major source of both triacylglycerols and cholesterol as although
it does not actively store either of the molecules it is involved in the packaging of lipids into
triacylglycerols and the creation and organisation of cholesterol.
- Excessive Alcohol consumption causes loss of homeostasis leading to insulin resistance of
the cells and inflammation of the liver leading to steatosis. The lipase enzyme is activated by
insulin hence when the cell becomes insulin resistant the lipase can no longer be activated

43 | P a g e
leading to an accumulation of fat in the cell. Cirrhosis (replacement of the liver tissue by
fibres scar tissue) which leads to loss of funciton is often the outcome of chronic alcohol
consumption.
- Free Fatty Acids are transported through the blood on the protein serum albumin.
- The five different lipoproteins in order of size are: chylomicrons, VLDL, LDL, IDL, HDL. When
considering density the order is simply reversed.
Cholesterol is synthesised from the starting material acetyl-CoA, along with all lipids. Two acetyl-
-hydroxy-3-methyl-glutaryl, this reaction is catalysed by the enzyme,
HMG-CoA reductase. This enzyme is controlled in three manners to ensure that too much
three mechanisms are:
- Cholesterol feedback actually inhibits the HMG-CoA reductase gene from being activated
- Cholesterol also is a destructive force against the enzyme
- It is inactivated from phosphorylation. It is of importance to the health community to inhibit this enzyme because then you could treat people that are having high cholesterol levels.
Synthesising Session: Inflammatory Liver Disease
When the liver becomes inflamed due to a variety of reasons the end result is scarring
through collagen fibrosis. A patient that is presenting with liver problems a history is vital since the
lifestyle that somebody lives has a big impact on the health of their liver. Signs of chronic liver
problems include jaundice which can be
first identified in the eyes. Blood Tests
are looking for raised levels of hepatitis
antibodies, as well as liver enzymes in
the blood stream, as that could indicate a
leak. Inflammation of the liver can be
caused by a plethora of reasons that are
highlighted in the figure right. The main
causes are: infection, autoimmune,
metabolic, heredity, and drug or toxin
induced causes.
If when seen under a CT scan the liver is
bumpy the person probably has sclerosis
or scarring of the liver. Hepatitis B could
be the cause however it must be quickly
identified if the person is chronic or acute. If antibody E is found in the blood then it means the
person has chronic problem (particular antibody takes 6 months to appear).
Hereditary Problems with the liver may be related to iron levels, or copper amounts in the
body. Both of this elements need to be maintained carefully.

44 | P a g e
As the liver is the site for a lot of the drug mobilisation, it can be affected by drugs easily.
This includes over the counter medication, herbal remedies and illict drugs. Anti-biotics is the
number one cause of the drug related liver failure.
Interesting Side note:
- Any activity that increase abrasion on a surface increases the chance of cancer. This includes
sun burn, abrasive foods in the gastrointestinal tract, or smoking. The increased amount of
abrasion or cell damage means that increased levels of proliferation are required leading to
a greater chance of a spontaneous mutation occurring that causes cancer.
- Metabolic syndrome: is a combination of medical disorders that when occur together
increase the risk of heart problems and diabetes. The requirements for someone to have
metabolic syndrome are the presence of one of: diabetes, impaired glucose tolerance,
impaired fasting glucose, insulin resistance as well as, blood pressure greater than 140 / 90,
increased blood triglyceride concentration, central obesity (BMI greater than 30) and
increased amounts of urinary albumin.

45 | P a g e
Gastrointestinal Medicine and Nutrition week 9 summary
Nutrition Requirements for Health
Every person that is living requires a certain amount of nutrition to survive. The human body
requires food for three broad functions. The nutrition is used for structural and functional purposes
such as maintenance of the BMR. Secondly any excess is used for performance that can be used for
aspects such as growth and pregnancy. The final purpose that
the food is used for when there is excess is being placed into
reserves, this outcome obviously has some major side effects.
We get nutrition into out body through eating and using the GI
tract to digest the food. Sometimes a person may be
incapacitated and food is then fed intravenous, or a tube is
passed through the mouth directly into the oesophagus. When
you are intravenously injecting somebody with nutrition you
must be careful that the osmolality of the vein as the increased
solutes may be harmful to the health of the vein.
The guidelines and the nutrient reference values are based on many different sources of
information including: dietary intakes for the population, observation of the population, animal and
human experimentation, other countries values, and many other sources. The 2003 NHMRC dietary
guidelines are split into adults and children. For adults the 4 guidelines are:
1. Enjoy a wide variety of nutritious foods
2. Prevent weight gain: be physically active and eat accordingly to your energy needs
3. Care for your food: prepare and store safely
4. Encourage and support breastfeeding
For the children and adolescents the guidelines differ slightly different:
1. Enjoy a wide variety of nutritious foods
2. Children and adolescents need sufficient nutritious foods to grow and develop normally
- Growth should be closely checked regularly for young children
- Physical activity is important in all children and adolescents
3.
4. Encourage and support breastfeeding.
Under each of these guidelines there are more specific rules that are set out to make them clearer.
For example under the first guideline for both the children and adults has:
- Eat plenty of vegetables, legumes, and fruits
- Eat plenty of cereals preferably wholegrain
- Include lean meat, fish, poultry,
- Include milks, yoghurts, cheeses and alternatives, (reduced fat milk for adolescents not
children as their energy needs are too high)
- Drink plenty of water
- Limit saturated fats and moderate fat intake
- Choose foods low in salt
- Consume only moderate amounts of sugar.

46 | P a g e
There are currently new guidelines that are being worked on, however they are un-examinable. The
graphic educational tool that is being used to teach young children the correct quantities of food
that they are to consume has also changed recently. The previously popular pyramid has been taken
over by a plate to highlight the amount of each
item of food
they should
have on their
plate.
Dietary Energy
Basal Metabolic Rate: is the energy expenditure of a person who is lying down, completely at rest
both physically and mentally, in a thermo neutral environment with a person that has been fasting
for 12 hours. The person undertaking the test must be careful of the mental status of the patient
because people that are not mentally relaxed will be burning more energy. The resting metabolic
rate is a similar test however the qualifications are not as tight.
The energy unit that is used is the Joule (J) which is the energy expended to move 1kg, 1 meter by 1
newton force. The older unit that was used was the calorie; to convert from calories to J you simply
multiply by 4.184, normally in humans we are discussing in KJ for food consumption and MJ for daily
energy expenditure. The rate of energy
expenditure is in Watts (W) which is a measure
of J / sec.
The diagram right highlights the fact that there
is a lot of food that we are not able to gain
nourishment out of. The DM refers to dry
matter, the OM stands for organic matter. The
diagram below shows the amounts of food that
are usually absorbed by the body. It is shown in
the diagram that a small portion is always lost
in faeces, urine and heat. The Net energy is the
energy that is available to be used by the body for
maintenance, performance and if there are left overs
reserves. This shows us that about 90% of the food
that we eat being captured.
A typical male Australian diet has 40% protein and 30
% fat and the remainder being carbohydrate. With
fats saturated and unsaturated fat levels must be
watched.

47 | P a g e
Fatty Acids: with fatty acids are the polyunsaturated fatty acids being omega 3 and omega 6. Omega
6 is the fatty acid linoleic acid and contains 18:2 formations. Omega 3 on the other hand is the
linolenic acid and contains the 18:3 formations. Vitamins also regularly come in through lipids; hence
the lipid is important as it is the only way that the vitamin can get across the membrane.
Known as Formation Digested to
Omega 6 Linoleic 18:2 Arachidoric acid (cell membrane)
Omega 3 linolenic 18:3 EPA (nervous tissue) and DHA (hormones)
Amino Acids: traditionally there are 9 essential amino acids, however histadine and arginine cannot
be created fast enough in a baby and hence needs to be ingested.
Reasons for malnutrition in a population include: poor education about nutrition, famine, illness
such as irritable bowel syndrome, abnormal diet (synthesising session), poverty, child neglect and
the elderly. These lead to deficiencies in the Amino Acid levels, and could be detrimental to the
health of the individual.
Minerals are potent organic compounds that are not used as a fuel source. For growth and health in
the human species they are essential however only minute amounts are required in the body. They
assist in many functional systems. There are two classifications of minerals:
- Minerals (moderate amounts needed): are Ca, P, Mg (all bone minerals), Cl, K, S Na
- Trace Minerals (trace amounts that are required: Cu, Al,
Sr (bone minerals, Co, Cr, Mn, Se, Fe, Zn
consume enough dairy products. Australians are also deficient in
Iodine, selenium iron and zinc. The table right highlights the amount
of each mineral there is present in a 60kg person. Below are
descriptions of the role of each of the minerals in the human body.
Iodine is essential for thyroid gland development

48 | P a g e
Vitamins are also potent organic compounds that function as co-enzymes, and are not used as an
energy source ever. They must all be consumed except for vitamin D (from sunlight) and K (intestinal
bacteria produce it). Vitamins are divided into fat soluble and water soluble.
- Fat soluble vitamins include vitamins A, D, E and K. They are stored in the body except
for K. Vitamin A is generally associated with vision, D is from the sunlight and a
deficiency creates rickets, E is important for membranes, K is a bone regulator and a
blood clotting mechanism
- Water soluble vitamins: Vitamin B and C. Decreased levels of Vitamin C will create
scurvy, and the majority of vitamin C is found in the adrenal glands and the pituitary
gland.
Folate is very important for women that are pregnant as the folate is necessary for successful
development of the neural tube of the foetus.
- some final images of carbohydrates and the effect on the glycaemic index
Note:
The importance of appropriate nutrition and exercise will only get greater and greater as time goes
on. Currently 50% of Australians are considered overweight, and as a future medical practitioner it is
amount of chronic health problems in the future.
Scurvy is a disease that is caused from a lack of vitamin C it is very common in sailors where the
amounts of perishable fruits are low. It results is lethargy and malaise, then the formation of spots
on the skin, spongy gums and bleeding of the mucous membranes. When it advances there is a
risk of: wounds, loss of teeth, jaundice, fever, neuropathy and death. It is prevented and treated by
simply eating a diet that contains citrus fruits and vitamin C.

49 | P a g e
Guided Learning Session:
Activity 1: Nutritional requirements for pregnancy, lactation and Infancy
Listeria Monocytogenes is a problem in pregnant women and not usually other individuals.
The bacterium is in abundance in nature and affects pregnant women more because they are under
very different life circumstances. The bacterium is an infection that presents with influenza like
symptoms. The ultimate outcome for the patient is an early onset of labour, and reduced foetal
movements. Cooking food to above 70o C is wha
survive. Foods that are to be avoided include soft cheeses such as brie, camembert, feta, and queso
blanco fresco as they can be contaminated and permit the growth of the bacterium.
During pregnancy there are normal birth ranges in weight that a mother should put on.
For an individual with an ideal BMI an increase of body weight of about 25-25 pounds is the ideal
weight gain. For mothers that are starting overweight they are expected to increase less weight.
Individuals that are obviously underweight should put on a greater amount of mass. It seems odd
that although the baby only weighs 2.5 kg on average the mother puts on that much weight,
however, the amniotic fluid and the remainder of maternal modifications all add on weight. Mothers
of twins are supposed to increase weight in the 16 20 kg range.
Overweight and obese mothers place themselves and their children at risk of many
diseases. The mother is at risk of gestational hypertension, gestational diabetes. The newborn is at
risk of being overweight on delivery, being preterm and thus not being adequately mature for the
external environment, being a stillbirth, or having neonatal birth issues. Women that are obese and
are having children need to be careful and be in constant contact with their doctors.
Constipation may occur during pregnancy due to the decreased levels of physical activity
and a change in the diet that the mother undergoes. In order to overcome constipation, an increase
in the amount of non-starch polysaccharides should increase as those are what get broken down in
the large intestines.
Heartburn is caused due to an increase in the intra-abdominal pressure leading to the
stomach pressure also being increased through the decrease in size of the stomach space. The
uterus particularly in the later stages of pregnancy takes up a large space in the abdomen and the
stomach certainly becomes smaller. An increase in stomach pressure would obviously place pressure
on the upper oesophageal sphincter and this will result in heartburn. The consumption of smaller
regular meals can be advised to the patient to help the food be digested completely.
Preconception the parents should limit the consumption of apples, take .8mg folate
tablets, and follow the recommended food servings for every day. The avoidance of seafood is also
advised pre conception as seafood has the potential to be high in mercury which will in turn affect
the foetuses central nervous system development. The mother has no real need to worry about
allergen desensitisation for a newborn as there is no data to support it.
The consumption of solid foods from the infant should not be encouraged until 4 6
months after the baby is born. Until this time fluids and breastfeeding is the most important manner
for the Breastfeeding should be encouraged from the mother for a variety of reasons including:

50 | P a g e
- The breast milk being a great energy source for the infant
- The act of breast-feeding is a great bonding experience to be shared between the infant
and the mother
- Breast milk contains IgA antibodies that are able to be passed to the body of the infant
through the bulk absorption in the small intestines
- Breast milk has a lot of the essential vitamins and minerals and amino acids in the correct
proportions for the newborn.
Activity 2: Nutritional Requirements for Infants, Children, Adolescents, and adults in Australia
An infant is defined as someone that is under the age of 12months. Child and Adolescent are in the
age groups 12 months to 18 years, and adults are over the age of 18. There are different nutritional
requirements for different age groups due to the different energy requirements of each. For
example adults require nutrition just for maintenance of their bodies, when children require it for
this function and the growth and development that they undergo. The table below highlights the
required percentages of each food intake for an adult. For children (up to a certain extent) food
intake should not be restricted due to the energy requirements for growth.
Lower Upper
Carbohydrates 45% 65%
Fats 20% 35%
Proteins 15% 25%
On top of this it is crucial that individuals get adequate vitamins and minerals so that the bodily
functions can continue. The typical Australian diet has some insufficiencies in vitamins and minerals:
calcium, sodium, selenium and iron are usually insufficient.
Dietary Guidelines for Adults
1. Eat a wide range of foods
2. Limit intake of foods and drinks containing saturate and trans fats, added salt, added sugar,
and alcohol
3. Achieve and maintain a healthy weight choose nutritious foods over that suit for energy
requirements
4. Encourage and support breastfeeding
5. Care for your food; store and prepare carefully
Gastritis: the inflammation of the lining of the stomach. Gastric Atrophy: is the end of chronic
gastritis, mucosal glands eventually losing function. Both of these increase in prevalence with
increasing age. A blocking of the stomach glands to would mean that the stomach and the remainder
of the gastrointestinal tract will be a lot less efficient at absorbing food.
National Physical Activity Guidelines:
- Think of movement as an opportunity not an inconvenience
- Be active every day in as many ways as you can
- Put together at least 30mins of moderate to vigorous intensity physical activity on most
days
- If possible enjoy some regular vigorous physical activity.

51 | P a g e
Important diseases that is associated with obesity
- Coronary Heart disease
- Type 2 diabetes
- Hypertension
- Stroke
- Low back pain
- Gout
- Venous insufficiency
- Gestational diabetes
Synthesising Session: Evaluation of selected Dietary plans
Are vegetarian diets healthier? What about Vegan Diets?
A properly planned vegetarian diet is by and large a lot healthier for the individual.
disease. Protein inadequacies is the biggest concern to a vegetarian however with appropriate
planning it is able to get all the essential amino acids that you require through the diet.
Veganism is the abstaining from the use of any animal product. Vegans do not only stop
consuming meat and fish but do not consume any animal product including dairy products, eggs and
often honey. In general Vegans have a lot lower chance of chronic disease, however this can be
attributed to psychosocial factors as well as their diet. A well planned Vegan diet is able to produce
adequate amounts of all nutrition required.
Dr Atkins Diet plan
The atkins diet is based on the core principle of reducing the amount of carbohydrates and
slightly increasing fat quantities that are consumed to ensure that the body becomes more efficient
as burning fats for fuel. The process of fat breakdown known as ketosis, is at its highest when blood
insulin levels are low, and insulin levels are low when blood glucose levels are low.
There are four phases in the Atkins diet:
1. Induction phase is the most restrictive phase of the Atkins diet. For a period of two weeks
nearly all carbohydrates are cut with the purpose being to get the body used to processing
fats for energy. During this stage the most rapid weight loss is seen.
2. Ongoing weight loss: involves an increase in the amount of carbohydrates that are
consumed however, not to an extent where weight gain ceases. This phase of the Atkins diet
is continued until the individual is 10 pounds away from the target weight. This stage of the
diet has a weekly rung system where you slowly introduce certain things that you would
want to be in your normal diet, on a weekly intervals. The rungs in order are: induction of
acceptable fruit and vegetable, fresh cheese, nuts and seeds, berries, alcohol, legumes,
other fruits, starchy vegetables, and whole grains. A rung on the ladder can be missed if you
3. Pre-maintenance: carbohydrates are increased by another 10 grams per day, and the weight
loss is extremely slow

52 | P a g e
4. Maintenance: is where all the habits that have been accumulated over time know have to
set in and you individual should attempt to maintain the health weight goal that they set out
to achieve.
High protein diet: is a special diet that is used by bodybuilders often in an attempt to build up
muscle and reduce fat simultaneously. The diet may include protein supplementation to ensure that
the appropriate amount of amino acids into the diet to assist muscle repair. Excess amounts of
protein associated with low carbs, particularly non starch polysaccharides, is very harmful for the
body.
Mediterranean Diet: is a diet that is based on the apparent paradox that is present between the high
level of fat consumption of some European countries and the lower rates of cardiovascular problems
in these countries. What the Mediterranean diet is based on is high consumption of fruits and
vegetables along with slightly higher fat consumption.

53 | P a g e
Gastrointestinal Medicine and Nutrition week 10 summary
Nutritional Status Assessment
When you are discussing the Nutritional Status Assessment you are considering malnutrition.
Malnutrition can be considered for both an excess and deficit of energy, nutrience, and imbalance in
the requirements that are required for survival. Under nutrition is the deficit in energy and nutrition.
Over nutrition is the excess energy or nutrience. There are 4 methods of Nutritional Assessment:
1. Historical Information: using a nutritional diary
2. Physical Examination: skin folds, waist measurements
3. Anthropometric Data: is a non-invasive measurement of body parameters (BMI height and
weight)
4. Laboratory Test: look into other parameters (blood, urine, faeces)
Have to remember that there are limitations to the measurements of skin folds and BMI. Firstly the
people that are undertaking the measurements are not trained, the BMI is good for normal
individuals however, people that have larger muscle mass will wrongly represent a person health.
A primary nutritional deficiency is when there is inadequate nutritional
being ingested, whereas a secondary nutritional deficiency is when you
issue than lifestyle related issue for the primary nutritional
deficiencies. Through either of these issues you get a decline in
nutritional stores, leading to decreased body function and eventually
physical signs and symptoms. A physical examination is able to pick up
on the changing signs that the person is showing however the declining
nutrient stores and the decreased body function requires
laboratory test usually.
Anthropometric Data: include things such as growth charts
(refer Centre of Disease control as well as WHO growth
chart). The age : weight growth charts are useful for
understanding how well somebody is growing. The BMI for
boys aged five to nineteen is shown right, with the
percentiles on the right hand side of the graph.
Laboratory Test are most commonly blood and urine, and
they have the advantage over the other means of testing as you can gain the nutritional status
directly. They tell the physician information regarding electrolyte balance, acid base balance, organ
function, and problems with nutritional implications. However laboratory tests do have certain
limitations, the data is open for interpretation, with a single test being insufficient. With blood tests
the effects of the short term can have large implications on the results of the test. An example of a
laboratory test is the: protein-energy malnutrition (PEM). PEM works on the assumption that the
liver secretes certain enzymes that are found in the blood, and then by the levels of these proteins
that are present you are able to determine whether the liver is functioning appropriately. Protein
levels can also be checked through the urine, where the nitrogen balance can be tested through
urinary urea. Some different proteins that are found in the body are shown right with the half-life of

54 | P a g e
each also shown. The half-life of a protein is the duration of
time that the protein remains is the body before it is broken
down.
Fats are the next nutrient that can be tested. Excess
levels of body fat have been associated with a lot of different issues in the body such as
cardiovascular disease and type 2 diabetes. It is important to note the distribution and the amount
of fat that is present on the body. Fats that are stored in and around the vital organs are a lot more
dangerous to the person than fat that is stored on the extremities. Lipid transport proteins such as
chylomicrons, VLDL, LDL, and HDL also can tell the physician the health of the individual in regards to
fat transport through a simple blood test.
Glucose Test are used to test for type 2 diabetes, and other glucose related absorption issue.
A normal blood test should show glucose concentration in between 4 and 8 mM. High levels of blood
glucose could simply be an instantaneous situation such as after a big meal. Urinary glucose diseases
such as glycosuria, then you cannot get rid of glucose out of blood stream meaning that you either
have a receptor problem or an insulin problem. With glucose testing, fasting blood glucose test is the
test that should be used twice to make sure. People that have glucose maintenance issues, generally
carry their own gluco-metres, and that is what tells them whether they should be consuming extra
foods or if their blood glucose is in a healthy realm. The HbA1c is a test that measures the long term
glucose levels (over a couple of months) so that people
cannot fix their results before blood tests. With the
HbA1c measurement; 6% is good, 8% is a warning, 10%
is bad, and 13% is dangerous, however recently to
decrease confusion; an mg / 100 mL level.
Vitamin and Mineral deficiencies are also an issue in Australian families, as many pe
fruit or vegetables. The other reasons for mineral deficiencies are poor absorption and abnormal
metabolism.
Non Nutritional related anaemia include: massive blood loss, infections, hereditary blood
disorders such as sickle cell anaemia, and chronic liver disease. Iron deficiency Anaemia is the other
type of anaemia. To test for this you get a blood count of: haemoglobin, haematocrit, serum ferritin
er than
normal, and serum folate is decreased and increased mean corpuscular volume or simply the mal-
absorption of the vitamins that can be checked through the schilling test.
GLS additions
Body Mass Index (BMI): is a method that is used to gauge the average health of a person of normal
build. The BMI is a measurement of your weight divided by your height squared, and it therefore in
the unit kg / m2. BMI is something that is inaccurate for people that are muscular build as the weight
factor in the calculation does not decipher between body fat and body muscle.
Skin Folds measurement: is another method that is utilised to determine the body fat percentage of
there is a manner to decipher between the muscle weight and the fat weight. A limitation to the skin

55 | P a g e
folds measurement is that the measurements are only as accurate as the person that is taking the
measurements is trained. Another inadequacy in the testing of skin folds is that the test assumes
that the ratio of subcutaneous fat and deep fat stores is the same.
Waist to Hip Ratio: also assesses fat distribution. A high waist to hip ratio indicates high intra-
abdominal fat, which is considered to be associated with greater health risks.
Normal values for all three of the following tests is found in the GLS document and added in below.
BMI and waist/hip
Body Mass Index Values
Waist / Hip ratio
Underweight < 18.5 Female
Accepted weight 18.5 -24.9 Healthy < .8
Overweight 25 29.9 Male
Obese >30 Healthy < .9
Body Fat Percentage Averages
To calculate Body Fat percentage there
is an extremely complicated formula
that is shown right:

56 | P a g e
GLS lecture: Dietary Records
Some of the methods that can be employed to record diet in a
population or on an individual level include:
- Weighed food record
- 24 hour diet recall
- Diet History
- Food Frequency Questionnaire (example shown right)
- Food Diary
Each of them has different respective advantages and disadvantages.
Advantages Disadvantages
Weighed food record
- Increased accuracy with portions
- Increased client burden - May alter the consumption
24 hour diet recall
- Low client burden - Avoids record keeping bias - More objective than Diet
history - Low cost
- Single recall may be different from usual diet
- Interviewer must be trained - Limited by client memory
(cognitive limitations of extremely young and the aged)
- Items are often forgotten
Diet History - Provides complete and detailed history
- Accounts for variations in diet - Representative of usual diet
- Requires a dietician to perform - Dependant on clients memory - Time consuming
Food Frequency Questionnaire
- Does not alter usual diet - Helpful for quick estimates - Helpful for describing food
intake patterns
- Foods may not be specific enough
- Does not provide enough information on total consumption
- High frequency of under and over estimation
Food Diary - Record of food intake at time of consumption
- Errors in recall are less than retrospective methods
- Food intake can be altered during reporting periods
- Under reporting is common (social desirability bias)
- Client burden is high - Portion size is difficult to
estimate - Number of days is required to
represent usual intake.
Some instructions that should be followed when you are keeping a food diary include.
- Record at time of consumption
- Include all beverages and snacks
- Provide as much detail as possible (include brand names)
- For composite dishes include the amount of each dish
- Keep food diary for 3 days with one being a weekend
- Try not to let it alter your normal diet

57 | P a g e
In order to calculate the amount of nutrient that you are in-taking you can
utilise the values that are shown right.
1. Step one is to work out the amount of each of the individual food
groups you are consuming. You do this through the recording
mechanisms that are discussed above.
2. Step two, is to figure out the about of energy that you are in-
taking
3. Add the energy intakes together and then you have a baseline for total energy consumption
4. If you want to figure out % of energy intake you are getting from each food group you then
simply divide the individual food group by total and multiply by 100.
Other things that are recommended and should be noted
- Each person should intake 30 grams of fibre each day
- 1000 mg of calcium is advised daily
- Iron is advised in the diet: 18mg for women and 8 mg for men every day
In order to control your weight your energy intake should be equal to the energy expenditure. The
daily recommended energy demands are about
8700 Ki, and if you consume 2000-4000 K j per day
less than that you should lose about .5 1 kg.
- A big mac takes about 55 minutes of
continuous swimming to work off
Some examples of different foods and the energy
that is gained from them are highlighted below.
Synthesising Session: Assessing nutrition in day to day practice
As doctors we are always assessing the nutrition of the patients that we see, doctors assess
their patients in numerous different manners including those that are listed above and even some
things as simple as looking at the patient.
Monitoring Growth in Children:
Growth charts are to be used when you are assessing the efficiency of growth in children.
Growth charts are a great way to pick up issues such as protein-energy malnutrition, obesity or
overweight, and is incredibly good indicator for the doctor since different children grow at different
speeds. Growth charts are used in 5 different situations:
1.
Aiming to identify growh faltering which may indicate underlying physical ill health,
deprivation or neglect and allow early intervention

58 | P a g e
2. As a surveillance tool for individual children in order to identify the onset of obesity early.
3. As a screening test at a single point in time to indicate abnormalities such as short stature,
or turners syndrome
4. As an eligibility criteria for growth hormone replacement
5. For analysis of population growth and trends.
When you are looking at certain case studies of individual that stop growing you need to take into
consideration their nutrition. There are three basic ways in which a person may be malnourished,
reduced intake of food, reduced absorption, or increased losses of energy / fuel.
Osteoporosis is a degenerative bone disease where increased activity of the thyroid gland
leads to hyperthyroidism and thus less calcium being deposited onto the bones. The lower levels of
calcium that is found on the bones then leads to the bones
becoming more brittle and in turn are a lot easier to
break. Vitamin D is an important factor in osteoporosis, as
vitamin D is crucial to help absorb calcium into the bones.
The risk factors for osteoporosis are shown on the right.
When a patient present with lethargy and a lack of
energy a potential reason could be some sort of anaemia.
In order to diagnose successfully the doctor must do a
blood count to test the amount of haemoglobin that is present and iron studies. Iron is transported
around the body with the molecule transferrin however multiple blood tests are required to gain an
accurate gauge of transferrin as it is also an acute phase reactant. So the main cause of anaemia
would be a lack of the consumption of Iron in the diet or an inability to absorb in efficiently.
are also at risk of getting these symptoms particularly straight after giving birth due to the large
amount of blood loss.
In summary when looking at the clinical assessment of nutrition you must take a
multifaceted view to ensure that nothing is missed. The issue is usually targeted to the person /
problem, and is often followed as a trend rather than a point reading.
-

59 | P a g e
Gastrointestinal Medicine and Nutrition week 11 summary
Control of Food intake
The human body has numerous mechanisms within it that
ensures that the amount of food stores that are present stay
within a normal level. The body is either in a state of seeking
picture is highlighted in the image right, where food intake
control fits in. The control of food intake can be divided into three broad categories, psychosocial,
physiological and social or environmental. The diagram below
in the right highlights the numerous different factors that
religion and food availability must also be included in this very
broad umbrella. Here are some definitions for terms that are
- Hunger: to seek food with craving for food and
physiological effects such as restlessness and stomach
contractions
- Satiety: is the feeling of satisfaction after eating food,
to some extent a conditioned reflex
- Appetite: desire for food. Powerful and poorly
controlled stimulus to eat.
The control of appetite is numerous circulating peptides and steroids that have a powerful action on
the hypothalamus. The main sources of these controlling factors are the: fat cells, the
gastrointestinal tract and the pancreas. Inside the hypothalamus there are neuronal centres that
participate in the control of food intake. The lateral nuclei are stimulated to increase feeding, the
ventromedial is your satiety centre and is therefore stimulated when your body wants to quench its
desire to feed. The paraventricular nuclei
are inhibitory and the dorsomedial nuclei
are stimulatory, with the arcuate nucleus
being the pivotal component that ensures
that everything works around it.
Arcuate Nucleus: receives signals
from multiple GI and adipose hormones. It
regulates the food intake as well as energy
expenditure, and is accessible from
circulating signals in the bloodstream. There
are two primary populations of neurons that
have either have a inhibitory or stimulatory
effect on food intake. POMC/CART
hormones inhibit food intake and increase Energy expenditure while ARGP/NPY hormones stimulate
food intake and therefore inhibit energy expenditure. These hormones act as targets for several
other appetite regulating hormones such as leptin, insulin, CCK, and ghrelin. On top of these

60 | P a g e
hormones there are a plethora of other
hormones that also have an impact on
the feeding and satiety levels of a
person.
Short Term control: preventing overeating at each meal
GI system will be unable to digest food at an optimal rate. Eat
smaller portions to allow GI tract to allow passage at steady rate
to digest and absorb at an optimal rate. By eating the correctly
sized portions you also decrease the risk of getting too much
metabolic storage, through the over consumption of food.
Systems that are at work to limit short term control include:
- Distension of the stomach and the duodenum; stretch
receptors send inhibitory signals through the vagus nerve
to suppress feeding.
- Oral factors are also present: where when you chew food
the body has a counter on the amount of food that is
coming through.
With these control mechanism some people they do not work as well and then they are genetically
more associated to gain weight.
Gastrointestinal Hormones: there are hormones that are present in the body that act to both
suppress and stimulate feeding. Hormones that suppress feeding include:
- CCK (responses to fat/protein in the duodenum): sensory receptors in duodenum send
messages through the Vagus nerve to the brain that satiety has been reached
- Peptide YY: secreted from the entire GI system (mainly the ileum and the colon) is
stimulated by the food intake and influenced by calories and food composition. The higher
levels of calories the greater the secretion of the peptide YY
- Glucagon like peptides are secreted due to a food in the intestines they stimulate glucose
dependant insulin to be secreted which suppresses appetite
Hormones that increase the need to feed include
- Ghrelin: which is released by the parietal cells (small amounts by the intestines) in response
to fasting it stimulates body to want to eat more food by increasing its appetite. The exact
method that it uses is unclear.

61 | P a g e
Long term control: maintenance of energy stores
When the body is looking at long term control of the energy stores there are basically two
situations that it can be in. Firstly it could be in a state where energy stores are below normal and in
this state the body will increase its feeding. Or it could be in a
state of high energy stores when feeding is decreased. The
long term control also has a lot to do with the past situation
the body was in. After starvation the body is more likely to
have the desire to eat large quantities of food, and after
times of high feed levels, the body will generally eat less. The
concentration of blood metabolites play a crucial role in this mechanism with glucostatic amino
factor that the body takes into account, when in a cold climate people generally eat a lot more in
order to maintain a higher standard of body warmth.
The feedback mechanism that is in place involves the hormone leptin. Leptin is a hormone
that is secreted from the adiposities of the body, when the levels are high. Basically when adipose
tissue levels are high there are high levels of leptin that is secreted which in turn decreases hunger
and then decreases fat storage. Leptin is also related to the onset of puberty in women, as when
adequate leptin is present the person has adequate fuel storages to undergo the changes that are
undertaken during puberty. There are mutations that cause a defect in leptin receptors, and
mutations that cause you to be unable to produce leptin. When this occurs the person wants to eat
a lot, as there is no feedback to stop people from being aware of the amount of adipose tissue that
they have. This can lead to morbid obesity or hyperphagia (abnormal amount of eating).
All these mechanism are present in normal people when they are in a healthy body weight
range. However with people that are not in a healthy body weight, then they may lose the ability to
control their weight. In obesity situations these mechanisms are overcome. One of the largest issues
with people that are obese is the pleasure system in the brain. Dopamine is a drug that gets
released from the body after pleasurable experiences; it makes you feel good and makes you want
to undertake the experience again. Dopamine is generally secreted from the body after things such
as sexual intercourse, exercise, and in some people eating.
When eating becomes a pleasurable experience the quantity
of food that is consumed by that person will obviously
increase, increasing their body weight. This is how people get
addicted to foods or most activities in that manner.
Peripheral Signalling: at the level of the
Gastrointestinal system feedback is created through the
vagal reflexes and the GI peptide hormones. At a peripheral
level the feedback mechanism is based around the presence
or absence of energy stores.

62 | P a g e
Mouse Models looking at obesity and diabetes
Using parabyosis experimentation they joined multiple mice together so that they share the same
blood system, and genetically modified them to be an obese mouse, a diabetic obese mouse or a
normal mouse. The results of the parabyosis experiment are shown right the explanation was gained
that:
- The db gene coded for
the leptin receptor
- The ob gene coded for
leptin
Using these assumptions that
are listed above, it is easy to
understand the results. When
leptin was given to the mouse
that was unable to produce leptin, the weight went back to normal, however in the mouse that
lacked the leptin receptor nothing could have been done.
GLS additions
The control of food intake can be physiological as it is described above, however it can also be
psychological or behavioural. When individuals undergo extreme periods of dieting they are often
cognitively impaired, and develop different behavioural traits. There were two diets that were
looked at in the GLS: firstly the women from Antibes and their extreme diet; take note of the
outcome of the crash dieting, the second was of a group of young healthy men and their highly
restrictive diet that they had to undergo. The specifics of the diets include:

63 | P a g e
The women of Antibes:
The starvation of the men: 36 young strong psychologically strong men were put on extremely
restrictive diets for 6 months. For three months the individuals are normally, while their lifestyles
were studied carefully. After this 3 month period the candidates went through 6 months of a diet
where their calorie intake was approximately halved. The body weights of the individuals dropped
by on average 25%. After the 6 month diet the men went through a 3 month rehabilitation phase.
There were many physical, psychological and social changes during the diet period, and some were
even maintained during the recovery and even after recovery. There were changes in:
- Attitudes and Behaviour towards food: food becomes the primary topic of conversation, and
dreams. There was decreased desire for sexual activity during semi-starvation. Men began to
eat different concoctions of food, and collect items that were related with food such as cook
books and cooking utensils. They were torn between gulping their food down rapidly and
making it last a long time.
- Binge Eating: several of the volunteers were unable to stick to the guidelines and went off
and had copious amounts of food. There was incredible complaints of hunger from nearly all
the men. During the rehabilitation phase a lot of the men could not control their urges, and
would eat amounts of food that were so large that they would fall ill. Others would have to
geographically isolate themselves from the food, otherwise they would not be able to stop
themselves from eating.
- Social and Sexual changes: the men became slowly more withdrawn and isolated.
- Cognitive and physical changes
The experiment proved that many of the previous symptoms that were associated with anorexia
nervosa, were actually associated with starvation and not anorexia. Giving people with eating
disorders may find the results of this experiment useful, as they are able to understand the
reasoning behind the feelings that they are experiencing.
(Read through the readings and summarise the diets and the results, look through GLS answers).
Synthesising Session Adolescent Eating Disorders
Adolescent eating disorders are not limited to adolescent people, adults are able to contract
the illness as well, however adolescence is the usual time for these behaviours to occur, as during
your teenage years you are normally under educated in the decisions that you make in regards to
their diet. An eating disorder is a severe illness causing more illness (time away from study / work)
and death than most other illnesses that affect young people. It was large tolls on not just the
physical nature of the affected, but the emotional state of themselves and those that are around
them. Eating disorders are not simply an alternate way of life, or a bad behaviour, people seem to
use the word loosely when in reality it is a very serious issue.
There are many eating disorders that effect adolescents, they effect at both ends of the
eating scale. Firstly there are Binge Eating disorders, that effects 5:100 people. The other end of the
scale involves disorders such as Anorexia Nervosa and Bulimia Nervosa where the body is incredibly
underweight. The most common eating disorder is EDNOS (eating disorders not otherwise specified)
as they have not been specified.

64 | P a g e
Anorexia Nervosa: is the relentless self-starvation and severe loss of weight, with mental
attributes as well such as denial of the severity of the situation and the fear of weight gain.
Individuals with anorexia nervosa have weight and shape concerns that are severely more acute
than normal, and they view a distorted body shape as ideal. They commonly indulge in other
methods to lose weight such as: laxatives, self-induced vomiting, and excessive exercise. There are
sometimes episodes of binge eating, and severe levels of mood changes with depression and anxiety
risk high. A person with anorexia nervosa is less than 85% of their expected body weight, whereas a
person with anorexia bulimia is normally within 10% of their weight range. People with anorexia
nervosa have large amounts of what is the appropriate body image, they are able to look at healthy
people and know that they are healthy, yet still think that they are very overweight. 5% of people
with anorexia nervosa pass away within the first 10 years, it is one of the hardest diseases to treat as
there is a physical as well as a psychological issue that has to be faced by the allied heath team.
With anorexia bulimia the person may even be overweight as they go through binge eating
that is followed by vomiting.
A lot of people believe that the disease of anorexia is new, however there is well
documented evidence of people that are anorexic many years ago, however the 20th century
be noted that only 1 in 10 individuals that suffer from anorexia are males.
Since the turn of the industrial revolution and definitely in recent times rates of obesity and
overweight individuals has been going higher and higher. In Australia alone 56% of adults are
considered obese and 20% of children. The issue with obesity is a lot more prevalent than that of
too much of a change.
People that are at the highest risk of getting obesity are city dwellers, women that were
expose
people with low self-esteem however are driven to achieve. The media plays a role as it promotes
Once a person is affected by anorexia nervosa a team including
nutritionists, doctors, psycho-therapists, nurses and supportive family
members are crucial to ensure that the individual survives. There are 4
steps that must be overcome highlighted in the image right.
Binge eating is another eating disorder that is a lot more common in
men. Some lifestyle characteristics that influences the binge eating include: low self-esteem,
depression, body image concerns, and poorly controlled diabetes. If somebody is binge eating you
must put them on a moderat
they would then be at a much higher chance of relapsing.
Another issue with people that suffer from eating disorders is that they are very rarely able
to self-diagnose. The majority of the time that they present is because they have been told to by a
family member or have been forced to by a family member.
65 | P a g e
The difference between bulimia and anorexia is that in bulimia there is the constant cycle of binge
eating and then vomittng, whereas in anorexia there is simply a mass restriction in the amout of
food that is consumed.
It must be remembered that not all people that diet have an eating disorder.

66 | P a g e
Gastrointestinal Medicine and Nutrition week 12 summary
Diet and Disease Management
GIMN week 12 intro lecture is un-examinable
There is a strong correlation between diet and disease in life. Diet and nutrition play an important
role in promoting good health, growth and development during life. It must be noted that both
under-nutrition and over-nutrition have negative impacts on the effects of chronic disease. Diseases
that present the greatest public health issue due to poor diet and nutrition include: obesity,
diabetes, Cardio vascular disease, cancer (colon), osteoporosis, and dental disease. Chronic disease
accounts for an enormous amount of deaths (75% by 2020) in the community and more than half of
chronic disease deaths are related to poor nutrition. Chronic diseases are largely preventable in the
community if people make different lifestyle choices, such that diets that contain 5-9 serves of fruit
per day decrease the risk of all chronic diseases.

67 | P a g e
Ecology of
Health