full mouth restoration on dental implants utilizing titanium laser
TRANSCRIPT

Full Mouth Restoration on Dental Implants UtilizingTitanium Laser-Welded Frameworksjerd_265 215..226
ROBERT SCHNEIDER, DDS, MS
ABSTRACTIn today’s dental literature, most frequently, esthetics are addressed with fixed restorations.This article will illustrate the opportunity to provide our patients with very good esthetic out-comes with a hopeless dentition utilizing dental implants, laser-welded titanium components,and characterized acrylic resin prostheses. The definitive prostheses provide excellent facialsupport, phonetics, esthetics, smile line, and function. The steps in such a treatment will be pre-sented from the clinical to dental laboratory procedures.
CLINICAL SIGNIFICANCEIncorporating newer technology into our patient treatment plans, which increasingly includesdental implants, may allow more time-efficient, esthetic, predictable, and reliable treatment.Laser-welded titanium frameworks offer many advantages for the patient, clinician, and dentaltechnician, which are illustrated.
(J Esthet Restor Dent 21:215–228, 2009)
I N T R O D U C T I O N
Originally, dental implantswere considered a “last
resort” for treatment of the eden-tulous patient. As implant den-tistry progressed, the originalBrånemark protocol required longhealing periods of several monthsfor osseointegration to take placebefore beginning fabrication ofthe definitive prosthesis.1 Manychanges in restorative and surgicalprotocol, microscopic and macro-scopic implant surface treatmentshave resulted in a significantreduction of healing timeand decreased patienttreatment time.2
With these improvements, however,there are still challenges facing thepatient, practitioner, and labora-tory technologist. These can be butare not limited to: patient expecta-tions, oral anatomy, patientfinances, practitioner knowledgeand clinical skills, laboratoryskills, and available biomaterialsfor fabrication of theplanned prosthesis.3–5
Patient expectations are a majorconcern for implant practitioners.Frequently, there are hard and softtissue compromises in the so called“esthetic zone” that precludeoptimal results with some fixedprosthetic restorations. Many
edentulous maxillas can be treatedwith dental implants and restoredwith over-dentures that result in avery cosmetic restoration. Signifi-cant residual ridge resorption canbe compensated for by the labialflange and tooth positioning toprovide optimal maxillary lipsupport, smile line, and facialsupport. The implants can provideretention and stability to theremovable prosthesis in addition tothe benefit of preserving the alveo-lar bone due to the presence ofdental implants in the area.
Implant overdenture therapy hasbeen utilized successfully for atleast two decades with high success
Professor, University of Iowa Hospitals and Clinics, Hospital Dentistry Institute,Division of Maxillofacial Prosthodontics, Iowa City, IA, USA
© 2 0 0 9 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L AT I O N © 2 0 0 9 , W I L E Y P E R I O D I C A L S , I N C .DOI 10.1111/j.1708-8240.2009.00265.x V O L U M E 2 1 , N U M B E R 4 , 2 0 0 9 215

rates.6 With the development ofnew technologies and use of newmaterials, many overdentures arenow able to be fabricated withouta palate and are very stable andretentive.7–9 This has several advan-tages to the patient such asimproved taste and temperaturesensation and a less bulky prosthe-sis, which may provide improvedspeech patterns for some patients.Multiple implant attachmentoptions have been utilized success-fully over the years.8
Mandibular implant-supportedfixed bridges for the edentulouswere treated by the early Bråne-mark protocol with the placementof 5–6 dental implants and resto-ration with a traditionally waxedand cast gold framework to whichthe dental technician couldprocess either composite or acrylicresin materials.1 These types of
restorations were very successfulbut with the escalation in the costof gold, this may render themsomewhat obsolete. There areseveral methods for utilizingCAD-CAM technology forfabrication of some of theseframeworks.10–12 This article willdescribe patient treatment withdental implants in both the maxil-lary and mandibular arch andrestored with titanium laser-welded prostheses. The maxilla isrestored with a Hader bar-supported palate-less overdentureand the mandible with screw-retained fixed bridges. The advan-tages over the previous lostwax/gold casting techniquesare several. The technician savestime by utilizing prefabricatedtitanium components resultingin improved fit and biocompatibil-ity, a very strong restoration,and use of a current technology
that is well researched andtoday, routinely available,compared with some CAD-CAM (computer aideddesign-computer aidedmanufacturing) systems.13–15
PAT I E N T T R E AT M E N T
A 62-year-old female presented forevaluation of her failing dentition.She was interested in improvedesthetics and function. Her healthhistory was noncontributory. Clini-cal examination revealed general-ized probing depths of 4–8millimeters, mobile dentition, mal-occlusion, and generally a non-restorable dentition (Figure 1A andB). Evaluation of her radiographsshowed significant destruction ofthe supporting osseous structures,many failing restorations, andrecurrent caries. Observationof the mounted diagnostic
A B
Figure 1. A and B, The patient’s pretreatment dental condition, noting defective restorations, periodontal disease, andtooth malposition.
T I TA N I U M L A S E R - W E L D E D F R A M E W O R K S
216© 2 0 0 9 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L AT I O N © 2 0 0 9 , W I L E Y P E R I O D I C A L S , I N C .

casts revealed a compromisedocclusal relationship.
The patient was very opposed tothe proposal of complete denturetreatment, as she had previouslyunsuccessfully attempted to weara mandibular removable partialdenture. After further consultationof the patient with the prostho-dontist and an oral surgeon, thepatient was presented with a planthat would include extractions,
fabrication of interim completedentures, healing of 3–6 months,a diagnostic wax up and fabrica-tion of a surgical guide, implantplacement of 6 SPI Element4.5-mm implants (ThommenMedical, Cleveland, OH, USA) ineach the mandible and maxilla.The definitive restorations wouldbe a mandibular-fixed prosthesisand a maxillary bar-supported,palate-less, removablecomplete denture.
A detailed discussion was com-pleted with the patient describingthe advantages and disadvantagesof treating the edentulous maxillawith moderate/severe residualridge resorption of both fixed andremovable prosthodontics. Theadvantages of significantlyincreased stability and retentionwith six maxillary implants and asupporting Hader bar wereaccepted by the patient. Addition-ally, it was felt the patient could
A
C
B
Figure 2. A, B and C, Mounted diagnostic casts and the patient-approved trial wax arrangement following extractionsand healing before implant placement to verify appropriate tooth position, phonetics, and esthetics. The silicone puttyindex assisted in determining the patient would be best treated with an implant supported overdenture due to theamount of alveolar ridge loss and the need for facial support provided from the denture flange.
S C H N E I D E R
V O L U M E 2 1 , N U M B E R 4 , 2 0 0 9 217

more easily complete the requiredhygiene techniques for the maxil-lary bar rather than a fixed pros-thesis with a pontic ridge lapdesign. The maxillary removableprosthesis was selected as thepatient required facial and lipsupport from the completedenture flange for optimal esthet-ics as determined from the edentu-lous wax-up and try-in phaseof treatment.
Maxillary and mandibularimmediate complete dentureswere fabricated prior toextraction of all of the patient’sremaining teeth. The teeth wereextracted uneventfully and theridge contoured for optimalimplant placement following initialhealing. The dentures were deliv-ered, the patient was given routine
instructions, and she was com-fortable with the understandingthat the prostheses wereconsidered interim.
Following a 3-month healingperiod, a diagnostic mountingand wax up was completed fordefinitive evaluation of occlusalvertical dimension, interarch dis-tance, centric relation, and veryclose evaluation of the patient’sesthetics requirements(Figure 2A–C). The patientapproved the esthetic tootharrangement, and surgical guideswere fabricated by duplicatingthe diagnostic esthetic tootharrangement (Figure 3).
A discussion with the surgeonresulted in the surgical guidedesign allowing wide-spread
placement of the implants in anoptimal position for tooth place-ment and spacing for restorativecomponents. Following implantplacement, the immediate dentureswere relieved and a soft tissue con-ditioner was placed in each dentureso the patient could comfortablywear the prostheses during thehealing period. All implants wentto place with an appropriatetorque and no mobility. Thesurgeon determined adequatehealing to begin definitive impres-sions that would be satisfactory 6weeks from initial placement.
The patient healed adequately andat 6 weeks, the restoration processwas begun with preliminaryimpressions from which opendesign custom impression trayswould be fabricated (Figure 4).
Figure 3. Surgical guides fabricated from thediagnostic trial wax arrangement utilized in thedefinitive implant placement in both the maxillary andmandibular aches in the proper predeterminedpositions.
Figure 4. Clinical appearance of the maxillary soft tissuesfollowing a 6-week healing period, illustrating good hygieneand patient compliance to maintain oral health.
T I TA N I U M L A S E R - W E L D E D F R A M E W O R K S
218© 2 0 0 9 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L AT I O N © 2 0 0 9 , W I L E Y P E R I O D I C A L S , I N C .

The custom trays were utilized forimplant level final impressionsusing a poly-vinyl siloxane impres-sion material (Figures 5A and B,6A and B). The followingappointment, trial bases withocclusion rims were routinelyadjusted for lip support, phonet-ics, esthetics, and determination ofappropriate occlusal verticaldimension and centric relation
(Figure 7). The final shade andmould of the prosthetic teeth wereverified with the patient’s assis-tance along with the shade of thegingival acrylic resin. At thisappointment, a verification indexwas tried in each arch followingremoval of the healing caps(Figure 8A and B). The verifica-tion index will prevent the neces-sity of another appointment for
framework try-in by allowing theclinician to determine that thefinal impression and master castare absolutely accurate. If theverification index does not go toplace accurately, the final impres-sion should be remade. Occasion-ally, if there is a discrepancy thatis minimal, the restorative clini-cian has the option to cut andreadapt the index intraorally and
A B
Figure 5. A and B, Open custom impression trays fabricated for final impressions from the preliminary impressions.This will facilitate direct impressions of the SPI Element implants versus an abutment level impression.
A B
Figure 6. A and B, Resultant master casts poured in a type V improved dental stone.
S C H N E I D E R
V O L U M E 2 1 , N U M B E R 4 , 2 0 0 9 219

correct the master cast by remov-ing the offending laboratoryanalog and replacing it throughthe corrected verification index.
The mounted master casts nowallow the technician to perform
an accurate wax arrangement ofthe prosthetic teeth for the clini-cian and patient evaluation(Figure 9). At this appointment,the clinician should be evaluatingocclusal vertical dimension, centricrelation, facial support, anterior
tooth position for optimal phonet-ics and esthetics, occlusal planeorientation, etc.16 The patient willbe asked to evaluate anteriortooth color, shape, size, and facialsupport. When approved, the waxup can then be returned to the
Figure 7. In the dental laboratory, trial bases withocclusion rims are fabricated directly on the master casts.The author provides the laboratory with duplicate sizehealing caps so the trial base will fit the mouth exactly asit fits the master cast. The maxillo-mandibular relationsare completed in a normal manner along with prosthetictooth selection.
A B
Figure 8. A and B, Verification indices are fabricated on the master casts utilizing the appropriate impression copingsluted together with VLC acrylic resin (Triad, Dentsply, York, PA, USA). The verification indices should go to placepassively and accurately when tried in the patient’s mouth at the try-in appointment.
Figure 9. At the wax try-in appointment, the patient willbe able to verify the esthetic arrangement, tooth display,tooth shade, facial support, phonetics, etc.
T I TA N I U M L A S E R - W E L D E D F R A M E W O R K S
220© 2 0 0 9 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L AT I O N © 2 0 0 9 , W I L E Y P E R I O D I C A L S , I N C .

A
C
B
Figure 11. A, B and C, The dental technician can now select the proper bar supporting abutment (Retain, SPI,Thommen Medical, Cleveland, OH, USA) and titanium coping for the abutment. Milling abutments (ThommenMedical) were selected for the mandibular arch because they are easily milled and welded to titanium stock to retainthe processed acrylic resin prosthesis. The components can then be laser welded with the maxillary titanium Hader barand mandibular fixed prosthesis directly on the master casts resulting in a very accurate fit.
A B
Figure 10. A and B, Following the patient’s approval of the wax set-up, the dental laboratory can fabricate a siliconeindex to aid in the proper contours and design of the definitive prosthesis in relationship to the teeth without distortingthe palatal contours of the maxillary arrangement.
S C H N E I D E R
V O L U M E 2 1 , N U M B E R 4 , 2 0 0 9 221

laboratory for fabrication of thedefinitive prosthesis frameworkand processing and characteriza-tion of the acrylic resin.17,18
L A B O R AT O RY P R O C E D U R E S F O R
T H E D E F I N I T I V E F R A M E W O R K S
Previous traditional frameworksfor implant-supported prostheticsinclude waxing the prosthesis,investing the wax up, utilizing thelost wax method converting theinvested wax up to a metalliccasting. This can be time consum-ing and extremely technique sensi-tive, as the frameworks haveseveral critical steps dependent ondimensional stability of wax,gypsum investment, oven tempera-tures, and the melting and solidifi-cation of metal alloys commonlyused in dentistry. Occasionally,these frameworks do not accu-rately and passively fit the mastercast following casting and requiresectioning and soldering to providefor an optimal fit to the mastercast.19 Again, this can be time con-suming and costly due to theincrease in time and effort by thedental technician.
Today, the implant companiesmanufacture titanium componentsthat can be utilized with today’simproved laser welding technology.Laser welding is an extremelyaccurate procedure that allows thedental technician to fabricate avery strong and biocompatible
metal prosthesis directly on themaster cast, helping to ensure apassive fit.13
An index is made of the final toothwax up to facilitate optimal designof the framework in relationship tothe appropriate tooth position(Figure 10A and B). The technicianthen can fabricate the frameworksfrom titanium components andassemble them with laser weldingin an inert atmosphere to preventcorrosion and weak joints. Thelaser welds and titanium frame-works are not only biocompatibledue to their titanium compositionbut the laser welds are also fre-quently stronger than their “sol-dered” counterparts in addition tobeing much lighter due to thedecreased specific gravity of tita-nium versus gold alloy. Given thecost of gold today (over $1,000 an
ounce), the titanium frameworkscan also be less expensive.
Because an implant level finalimpression was made, the dentaltechnician was able to select theappropriate abutments for the finalprosthesis (Figure 11A–C): a screwretained Hader bar for the maxillaand a screw retained fixed prosthe-sis in the mandible. The mandibu-lar fixed bridge was fabricated intwo pieces because the most distalimplants were placed in the firstmolar area. There is a consider-ation that mandibular flexurecould be a long-term problem if arigid framework is placed, resultingin possible biomechanical failureof components.20–23
The mandibular frameworksare opaqued and processed inhigh-impact acrylic resin and
Figure 12. The author routinely requests that thetechnician utilize a pink opaque on the mandibularframework to mask the grey color of the metal andprovide a more esthetic restoration.
T I TA N I U M L A S E R - W E L D E D F R A M E W O R K S
222© 2 0 0 9 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L AT I O N © 2 0 0 9 , W I L E Y P E R I O D I C A L S , I N C .
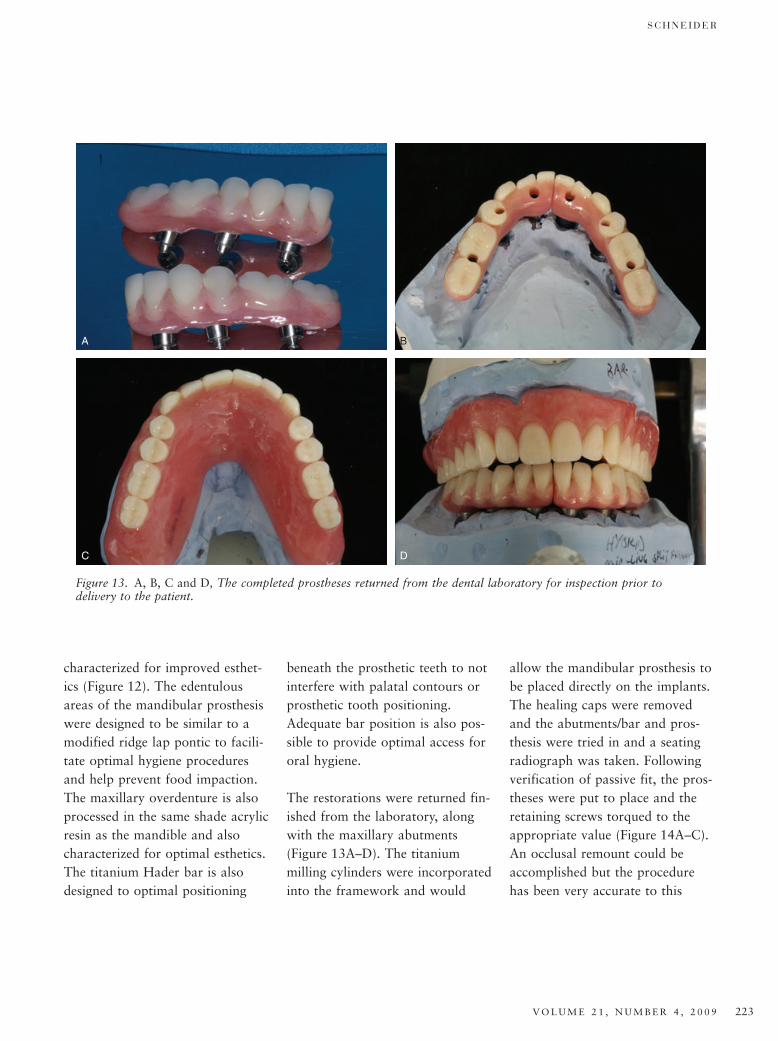
characterized for improved esthet-ics (Figure 12). The edentulousareas of the mandibular prosthesiswere designed to be similar to amodified ridge lap pontic to facili-tate optimal hygiene proceduresand help prevent food impaction.The maxillary overdenture is alsoprocessed in the same shade acrylicresin as the mandible and alsocharacterized for optimal esthetics.The titanium Hader bar is alsodesigned to optimal positioning
beneath the prosthetic teeth to notinterfere with palatal contours orprosthetic tooth positioning.Adequate bar position is also pos-sible to provide optimal access fororal hygiene.
The restorations were returned fin-ished from the laboratory, alongwith the maxillary abutments(Figure 13A–D). The titaniummilling cylinders were incorporatedinto the framework and would
allow the mandibular prosthesis tobe placed directly on the implants.The healing caps were removedand the abutments/bar and pros-thesis were tried in and a seatingradiograph was taken. Followingverification of passive fit, the pros-theses were put to place and theretaining screws torqued to theappropriate value (Figure 14A–C).An occlusal remount could beaccomplished but the procedurehas been very accurate to this
A B
C D
Figure 13. A, B, C and D, The completed prostheses returned from the dental laboratory for inspection prior todelivery to the patient.
S C H N E I D E R
V O L U M E 2 1 , N U M B E R 4 , 2 0 0 9 223

point and the occlusal adjustmentwas extremely minimal.
Oral hygiene was demonstrated forthe patient and she was able toperform the required proceduresquite well. Routine postdeliveryinstructions were given and thepatient was appointed forfollow-up (Figure 15A and B). Thepatient has been problem free forover 3 years with no soft/hard
tissue problems or concerns withthe titanium laser-welded frame-work (Figure 16).
C O N C L U S I O N
Use of current techniques andmaterials allow improved patienttreatment with dental implants.The lost wax method has beenthe basis for the majority ofindirect dental restorationfabrication procedures for
well over a hundred years.Improved technology canprovide the treating practitioner ameans to delivery superior pros-thetics in a timely manner thatmay be superior to that whichwe have all become accustomed.Utilization of new technologywill allow improved and predict-able treatment for our patients.Esthetics, function, andcomfort for the patient have
A
C
B
Figure 14. A, B and C, The maxillary healing caps are removed, maxillary abutments placed along with the Hader barand torqued to place. The mandibular healing caps are removed and the mandibular split midline prosthesis is torquedto place. Before torquing the prostheses to place, the author will verify the occlusal relationship and make anynecessary adjustments and repolish the prosthesis where necessary. Right and left lateral views and frontal view withlips retracted.
T I TA N I U M L A S E R - W E L D E D F R A M E W O R K S
224© 2 0 0 9 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L AT I O N © 2 0 0 9 , W I L E Y P E R I O D I C A L S , I N C .

been addressed in a predictableand reliable manner due toadaptation and utilizationof newer componentsand technologies.
D I S C L O S U R E A N D
A C K N O W L E D G M E N T
Dr. Schneider has occasionallylectured for Thommen Medical,for which he received honoraria.
The author thanks Kirk Fridrich,DDS, MS, for his surgical expertise
in the treatment of this patientwith extractions and implant place-ment, and Dan Roberts, CDT, forhis skills in the laboratory pre-paration of the abutments, laserwelding, and processing ofthe definitive prostheses forthe patient.
R E F E R E N C E S
1. Adell R, Ericksson B, Lekholn U,et al. Long-term follow-up study ofosseointegrated implants in the treatmentof totally edentulous jaws. Int J OralMaxillofac Implants 1990;5:347–59.
2. Weber HP, Crohin CC, Fiorellini JP.A 5-year prospective clinical and radio-graphic study of non-submerged dentalimplants. Clin Oral Implants Res2000;11:144–53.
3. Moy PK, Medina D, Shetty V, AghalooTL. Dental implant failure rates and asso-ciated risk factors. Int J Oral MaxillofacImplants 2005;20:569–77.
4. Goodacre CJ, Vernal G, RungcharassaengK, Kan JY. Clinical complicationswith implants and implant prostheses.J Prosthet Dent 2003;90:121–32.
5. Mojon P, Thomason JM, Walls AW.The impact of falling rates of edentulism.Int J Prosthodont 2004;17:434–40.
6. Sadowsky SJ. Treatment considerationsfor maxillary implant overdentures:a systematic review. J Prosthet Dent2007;97:340–8.
7. Kramer A, Weber H, Benzing U. Implantand prosthetic treatment of the edentu-lous maxilla using a bar-supported pros-thesis. Int Oral Maxillofac Implants1992;7:251–5.
8. Trakas T, Michalakis K, Kang K,Hirayama H. Attachment systems forimplant retained overdentures: a litera-ture review. Implant Dent 2006;15:24–34.
9. Zitzmann NU, Marinello CP. Implant-supported removable overdentures in the
A B
Figure 15. A and B, The patient’s smile with the wax trial denture and with the definitive prostheses in place. Note nonoticeable changes in development of smile line or lip and facial support.
Figure 16. Panoramic radiograph taken 3 yearspostdelivery illustrating stable bone levels around therestored implants.
S C H N E I D E R
V O L U M E 2 1 , N U M B E R 4 , 2 0 0 9 225

edentulous maxilla: clinical and technicalaspects. Int J Prosthodont 1999;12:385–90.
10. Riedy SJ, Lang BR, Lang BE. Fit ofimplant framework fabricated by differ-ent techniques. J Prosthet Dent1997;7:353–9.
11. Jemt T, Lie A. Accuracy of implant-supported prostheses in the edentulousjaw. Analysis of precision of fit betweencast gold-alloy frameworks and mastercasts by means of a three-dimensionalphotogrammetric technique. Clin OralImpalnts Res 1995;6:172–80.
12. Jemt T, Back T, Peterson A. Precision ofCNC-milled titanium frameworks forimplant treatment in the edentulous jaw.Int J Prosthodont 1999;12:209–15.
13. Jemt T, Henry P, Linden B, et al. A com-parison of laser-welded titanium and con-ventional cast frameworks supported byimplants in the partially edentulous jaw:a 3-year prospective multicenter study.Int J Prosthodont 2000;13:282–8.
14. Johansson LA, Ekfeldt A. Implantsupported fixed partial prostheses:a retrospective study. Int J Prosthodont2003;16:172–6.
15. Hellden LB, Derand T. Description andevaluation of a simplified method toachieve passive fit between cast titaniumframeworks and implants. Int J OralMaxillofac Implants 1998;13:190–6.
16. Desjardins RP. Clinical evaluation of thewax trial denture. JADA 1982;104:184–90.
17. Nash JC, Reisburg DJ. Color character-ization of denture base material. TrendsTech 1995;12:33–7.
18. Crace K. An updated guide to character-izing injected dentures. J Dent Tech1996;9:1–6.
19. Wee AG, Aquilino SA, Schneider RL.Strategies to achieve fit in implant pro-sthodontics: a review of the literature.Int J Prosthodont 1999;12:167–78.
20. Paez CY, Barco T, Roushdy A, Andres C.Split-frame implant prosthesis designed
to compensate for mandibular flexure:a clinical report. J Prosthet Dent2003;89:341–3.
21. Regli CP, Kelly EK. The phenomenon ofdecreased mandibular arch width inopening movements. J Prosthet Dent1967;17:49–53.
22. Goodkind RJ, Heringlake CB. Mandibu-lar flexure in opening and closing move-ments. J Prosthet Dent 1973;30:134–8.
23. Lindquist LW, Rockler B, Carlsson GE.Bone resorption around fixtures in eden-tulous patients treated with mandibularfixed tissue-integrated prostheses.J Prosthet Dent 1988;59:59–63.
Reprint requests: Robert Schneider,University of Iowa Hospitals and Clinics,Hospital Dentistry Institute, Division ofMaxillofacial Prosthodontics, 200 HawkinsDrive, Iowa City, IA, USA 52242-1049;email: [email protected]
T I TA N I U M L A S E R - W E L D E D F R A M E W O R K S
226© 2 0 0 9 , C O P Y R I G H T T H E A U T H O RJ O U R N A L C O M P I L AT I O N © 2 0 0 9 , W I L E Y P E R I O D I C A L S , I N C .