full mouth rehabilitation
TRANSCRIPT
1
FULL MOUTH REHABILITATION
PRESENTED BY : ILA YADAVPG STUDENT DEPT. OF PROSTHODONTICS

2
CONTENTS PART 1 Definition Indications Classification Occlusal approach and schemes Review of occlusal schemes Terminologies Hobo’s philosophy for full mouth rehabilitation Hobo’s Twin table technique Hobo’s Twin stage technique References

3
ACCORDING TO GPT-8
FULL MOUTH REHABILITATION is defined as the restoration of the form and function of the masticatory apparatus to as nearly a normal condition as possible
4
The objective of full mouth rehabilitation is not only thereconstruction and restoration of the worn out dentition,
butalso maintenance of the health of the entire
stomatognathicsystem. Full mouth rehabilitation should re-establish a stateof functional as well as biological efficiency where teethand their periodontal structures, the muscles of
mastication,and the temporomandibular joint (TMJ) mechanisms allfunction together in synchronous harmony

5
Why do we need
to reorga
nize occlusi
on?
REPEATED FRACTURE OR FAILURE OF TEETH
OR RESTORATI
ON
UNACCEPTABLE
FUNCTION AND
AESTHETICS
TRAUMA FROM OCCLUSION
BRUXISM
LACK OF INTEROCC
LUSAL SPACE FOR RESTORATI
ON
before after
6
Classification by Turner and Missirlain (1984)
Category 1 - Excessive wear with loss of vertical dimension.
Category 2 - Excessive wear without loss of vertical dimension of occlusion but with space available.
Category 3 - Excessive wear without loss of vertical dimension of occlusion but with limited space available
Turner KA, Missirlian DM (1984) Restoration of the extremely worn dentition. J Prosthet Dent 52:467–474

7
Category-1: Excessive wear with loss of verticaldimension of occlusion (VDO) The patient closest speaking space is more than 1 mm The interocclusal space is more than 4 mm Some loss of facial contour and drooping of the
corners of the mouth. All teeth of one arch must be prepared in a single
sitting once the final decision is made. This makes the increase in VDO less abrupt and allows better control of esthetics.

8
Category-2: Excessive wear without loss of VDO butwith space available Patients typically have a long history of gradual wear caused by bruxism, oral habits, or environmental
factors The occlusal vertical dimension (OVD) is maintained by
continuous eruption. It might be difficult to achieve retention and
resistance form because of shorter crown length and gingivoplasty may be needed.
Enameloplasty of opposing posterior teeth may provide some space for the restorative material.
9
Category-3: Excessive wear without loss of VDO but with limited space There is excessive wear of anterior teeth over a long period, and there is minimal wear of the posterior
teeth. Centric relation and centric occlusion are coincidental Closest speaking space of 1 mm and an interocclusal distance of 2–3 mm. In such cases vertical space must be obtained for
restorative materials. This can be accomplished by orthodontic movement,
restorative repositioning, surgical repositioning of segments
10
After evaluating and classifying the patient’s existing clinical situation but before beginning the reconstruction procedure, decide upon the OCCLUSAL APPROACH and choose an appropriate OCCLUSAL SCHEME

11
Occlusal Approach
Confirmative
approach
• occlusion is reconstructed according to the patient’s existing intercuspal position.
• It is adopted when small amount of restorative treatment is undertaken.
Reorganized
approach
• New occlusal scheme is established around a suitable condylar position which is the centric relation position.
• The patient’s occlusion may be reorganised if the existing intercuspal position is unacceptable and needs to be changed or when extensive treatment is to be undertaken to optimize patient’s occlusion.

12
Occlusal schemes The occlusal schemes for eccentric
movements are classified according to the contact condition between upper and lower posterior teeth.
Balanced articulation group function and mutually protected articulation.
13
Balanced Occlusion/ Balanced Articulation
The bilateral, simultaneous, anterior and posterior occlusion contact of teeth in centric and eccentric positions.

14
Group function, as established by Schuyler (1959) was intended to distribute occlusal forces uniformly to all the teeth of the working side, also referred to as unilateral balanced articulation, which occurred only in 8% of natural dentition.
So the definition was changed to multiple contact relationships of the posterior teeth of the lateral movements of the working side in 1987

15
D’Amico in 1958 conducted a study and stated that cuspid protected articulation and disocclusion were natural adaptations for preventing destructive occlusion.
Cuspid protected articulation is defined as mutually protected articulation in which the vertical and horizontal overlap of the cuspid teeth dis engages the posterior teeth in excursive movements of the mandible

16
Review of Occlusal Concepts and Philosophies
An early concept of comprehensive dentistry originated from the gnathologic society founded by McCollum in1926.
McCollum together with Stuart published their
classic ‘‘Research Report’’ in 1955 and gave the GNATHOLOGICAL CONCEPT.
Gary M. DeWood. Gnathology and Pankey-Mann-Schuyler : fulfilling the requirements of occlusion in oral rehabilitationThe University of Toledo The University of Toledo Digital Repository 2004
17
They believed that anterior guidance was independent of the condylar path and described condylar path as a fixed entity in adults.
The concept of balanced occlusion which included the idea that the most posterior position of the condyles was the optimal functional position for restoring denture occlusion was applied to restoration of the natural dentition by McCollum, Schuyler and others.
18
STUART AND STALLARD observed that the upper lingual cusps stamp into lower fossae and lower incisors, canines and buccal cusps stamp into the upper fossae.
They observed that canines discluded all other teeth in laterotrusive (working) excursion which was similar to the observation of D’Amico.
In their report in 1960, they adopted the concept of mutually protected occlusion (canine-protected /organic occlusion) which replaced the concept of balanced occlusion.
Stuart CE (1973) The contributions of gnathology to prosthodontics. J Prosthet Dent 30:607–608Stuart CE, Stallard H (1960) Principles involved in restoring occlusion of the natural teeth. J Prosthet Dent 10:304–313
19
SCHUYLER first introduced the Concept Of ‘FREEDOM IN CENTRIC’’ and supported the theory that centric relation was rather a biological area of the TMJ than a point.
In this concept, ‘‘there is a flat area in the central fossae upon which opposing cusps contact which permits a degree of freedom (0.5–1 mm) in eccentric movements uninfluenced by tooth inclines’’.
It relies on cusp-to-surface mechanics. Schuyler suggested that incisal guidance without
freedom of movement from a centric relation occlusion to a more anterior tooth intercuspation will ‘‘lock-in’’ the posterior occlusion
Schuyler CH (1959) An evaluation of incisal guidance and its influence on restorative dentistry. J Prosthet Dent 9:374–378Schuyler CH (1963) The function and importance of incisal guidance in oral rehabilitation. J Prosthet Dent 13:1011–1029

20
An organized approach to oral rehabilitation was introduced by Pankey utilizing the principles of occlusion advocated by Schuyler, known as THE PANKEY–MANN–SCHUYLER (PMS) PHILOSOPHY OF ORAL REHABILITATION
Their philosophy was pertinently based on the Spherical theory of occlusion, The ‘‘wax chew-in’’ technique described by
Meyer and Brenner, and on the importance of cuspid teeth as
discussed by D’Amico.Mann AW, Pankey LD (1960) Oral rehabilitation: part I. Use of the P-M instrument in treatment planning and in restoring lower posterior teeth. J Prosthet Dent 10:135–150Pankey LD, Mann AW (1960) Oral rehabilitation: part II.Reconstruction of the upper teeth using a functionally generated path technique. J Prosthet Dent 10:151–162

21
Early gnathologic concepts focussed primarily on the condylar path and it was believed that anterior guidance was independent of the condylar path.
HOBO AND TAKAYAMA in their study revealed that anterior guidance influenced the working condylar path and concluded that they were dependent factors.
Hobo adopted the concept of posterior disclusion and gave the TWIN-TABLES TECHNIQUE.
Hobo S (1991) Twin-tables technique for occlusal rehabilitation.Part I: mechanism of anterior guidance. J Prosthet Dent 66:299–303Hobo S (1991) Twin-tables technique for occlusal rehabilitation. Part II: clinical procedures. J Prosthet Dent 66:471-477
22
THE TWIN-STAGE Procedure was developed as the advanced version of the Twin-Table technique.
Takayama in their research concluded that cusp angle be considered as the most reliable determinant of occlusion as cusp angle does not deviate and is 4 times more reliable than the condylar and incisal path which show deviation.
Hobo S, Takayama H (1997) Twin-stage procedure. Part 1: a new method to reproduce precise eccentric occlusal relations. Int J Periodontic Restor Dent 17:113–123

23
TERMINOLOGIES (as per GPT – 8)
Condylar Guidance Mandibular guidance generated by the
condyle and the articular disc traversing the contours of the glenoid fossae.
Condylar Guidance : The mechanical form located in the upper posterior region of an articulator that controls the movement of it’s mobile member.

24
Incisal Guidance The influence of the contacting surfaces of
the mandibular and maxillary anterior teeth on mandibular movements.
Incisal Guidance The influences of the contacting surfaces
of the guide pin and the guide table on articular movement.
25
Bennet Angle : The angle formed between the sagittal plane and the average path of the advancing condyle as viewed in the horizontal plane during lateral mandibular movements
Immediate mandibular Lateral Translation The translatory portion of lateral movement
in which the non working side of condyle moves essentially straight and medially as it leaves the centric relation position.
26
Physiologic Rest Position The mandibular position assumed when
the head is in an upright position and the involved muscles, particularly the elevators and the depressor groups, are in tonic contraction and the condyles are in a neutral unstrained position
Laterotrusion Condylar movement on the working side
in the horizontal plane
27
Mandibular Translation The translatory movement ( medio-
lateral) movement of the mandible when viewed in the frontal plane.
Fischer’s Angle The angle formed by the intersection of
the protrusive and non working side condylar path as viewed in sagittal plane.

28
HOBO’S PHILOSOPHY FOR FULL MOUTH REHABILITATION

29
Early gnathologic concepts focused primarily on thecondylar path. The concepts were based on the theory thatthe condylar path does not change during adulthood
andthat the determination of anterior guidance is at thediscretion of the dentist. McCollum and Stuart believed that anterior
guidance was independent of the condylar path.

30
To verify whether condylar guidance and anterior guidance were independent factors, hobo and takayama measured the lateral condylar paths in 10 patients with an electronic mandibular recording device.
The measurements were recorded under two test conditions: tooth-contact / without clutch condition, and nontooth contact / with clutch condition. The results demonstrated that the working-side condylar path
changed remarkably while the nonworking-side condylar path did not reveal noticeable changes.
From this movement, it was observed that the condylar path was affected by anterior guidance and
Condylar guidance and anterior guidance were dependent, not independent, factors.
Hobo S. Takayama H. effect of canine guidance on the working conduler path. Int J Prosthodont 1989;2:73-9

31
Neutral line
Surtrusion Detrusion
Hobo S. A kinematic investigation of mandibular border movement by means of an electronic measuring system. Part III. Rotational center of lateral movement. J PHOSTHET DENT 1984;52:66-72.
32
Importance of Anterior GuidanceInci
sal guidance
Canine guidance
Anterio
r guidanceAlthough anterior guidance only ranges from 2 to 6
mm, it greatly influences occlusion, In healthy patients, anterior guidance is approximately 5 degrees steeper than the condylar path in the sagittal plane.Therefore, when a patient protrudes the mandible, the anterior teeth guide it downward, creating space between the posterior teeth referred to as POSTERIOR DISCLUSION. The same phenomenon occurs during lateral movement.
33
Necessity For Disocclusion 1. “Security insurance” to protect the
teeth from harmful effects due to cuspal interference.
An interference could occur due to a difference between the eccentric and returning condylar path.
2. A redundant need to protect the teeth
from harmful effects due to any cuspal interference since anterior guidance varies among individuals .

34
Determinants of disclusionAngle of
hinge rotation
Cusp shape factor
Measured value(mm)
Angle of hinge rotation(mm)
Cusp shape factor(mm)
Protrusive 1.1 0.2 0.9
Working 0.5 0.5 0
Nonworking 1.0 0.5 0.5
35
Angle of hinge rotation The mandible rotates around the intercondylar axis during eccentric movements when anterior guidance is
steeper than the condylar path (Fig. 2). The factor that compensates for the difference in steepness is the angle of hinge rotation.
Takayama and Hobo analyzed disclusion relative to the angle of hinge rotation by using kinematic formulae.
The results indicated that the angle of hinge rotation contributed to posterior disclusion by approximately 0.2 mm for protrusive movement and 0.5 mm on average for lateral movement on both working and nonworking sides.

36

37
When the right and left condyle moves 3 mm in protrusive movement and the nonworking condyle moves 3 mm in lateral movement, the amounts of disclusion were
1.1 +- 0.6 mm during protrusive movement 0.5 +- 0.3 mm on the working side and 1.0 +- 0.6 mm on the nonworking side during
lateral movement measured at the mesiobuccal cusp tip of the
mandibular first molar.

38
The actual disclusion during protrusive and lateral movements on the nonworking side differ from the angle of hinge rotation.
This leaves residual amounts of disclusion unaccounted for, namely, 0.9 mm in protrusive and 0.5 mm on the nonworking side.
Thus suggesting that the angle of hinge rotation was not solely responsible for disclusion.
The residual amounts can also be attributed to another determinant of disclusion, the CUSP SHAPE FACTOR.

39
Cusp shape factor

40
41

42

43
Buffer space McCollum and Stuart described the condylar path as a
fixed entity in an adult. Repetitive lateral movements compared with the
respective condylar paths, show no movement tracing the same line.
The deviation in the condylar path during eccentric movements was attributed to the shock-absorbing nature of the articular disk. Hobo and Takayama refered to this deviation in condylar path as a “buffer space.”
Molar disclusion should be greater than the buffer space to avoid occlusal interferences during eccentric movements. Buffer space Disclusion
Protrusive 0.8 mm 1.1 mmWorking 0.3 mm 0.5 mmNonworking 0.8 mm 1.0 mm

44
THE ANGLE OF HINGE ROTATION produced by the angular difference between anterior guidance and the condylar path assists posterior disclusion but is not solely responsible.THE CUSP SHAPE FACTOR is created by establishing the appropriate form of the posterior cusps aligned to the condylar path; thus it also contributes to posterior disclusion.The molars must disclude slightly more than the deviation in the condylar path ( BUFFER SPACE ) to avoid occlusal interferences.
The mechanism of anterior guidance was reviewed to provide a basis for understanding THE TWIN-TABLES AND TWIN STAGE TECHNIQUES, which are practical method for establishing anterior guidance and cusp shape from the condylar path.

45
TWIN TABLE TECHNIQUE
Incisal table 1 Without disclusion Cusp shape factor
Incisal table 2 With disclusion Angle of hinge rotation

46
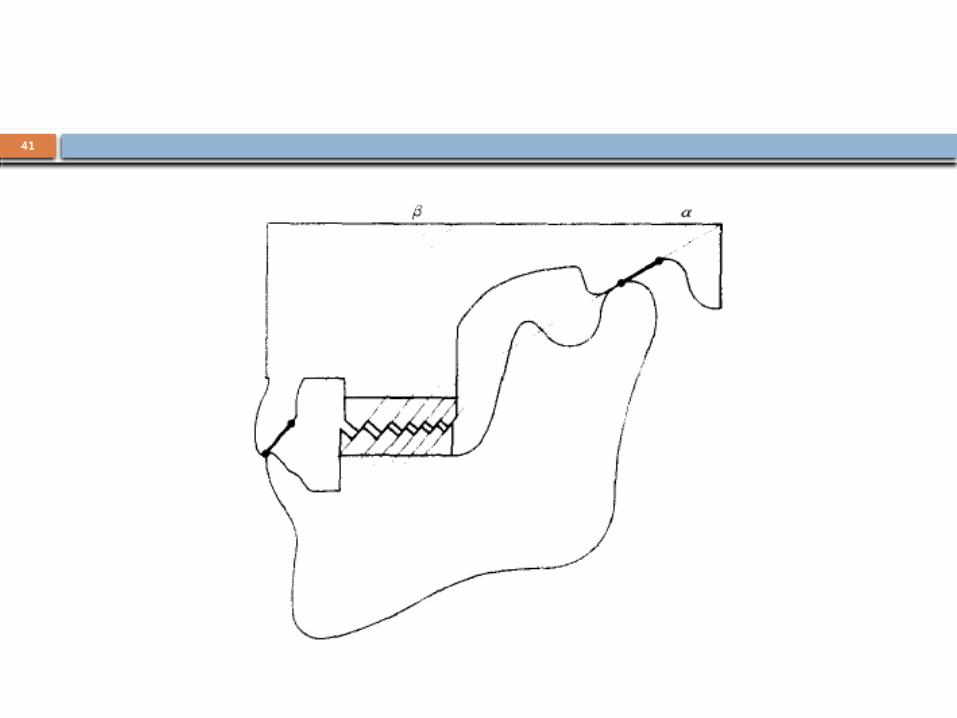
Procedure For the twin-tables technique, the working
condylar path is set on the articulator to move directly outward along the transverse horizontal axis to produce a neutral line.
A semiadjustable arcon-type articulator with a box-shaped fossa element mimics such a working condylar path.
When a fully adjustable articulator is used, the working condylar path is reset to zero both in the frontal and the horizontal planes so that the working condyle moves straight outward.

47
Diagnostic casts are mounted on semiadjustable articulator.
48
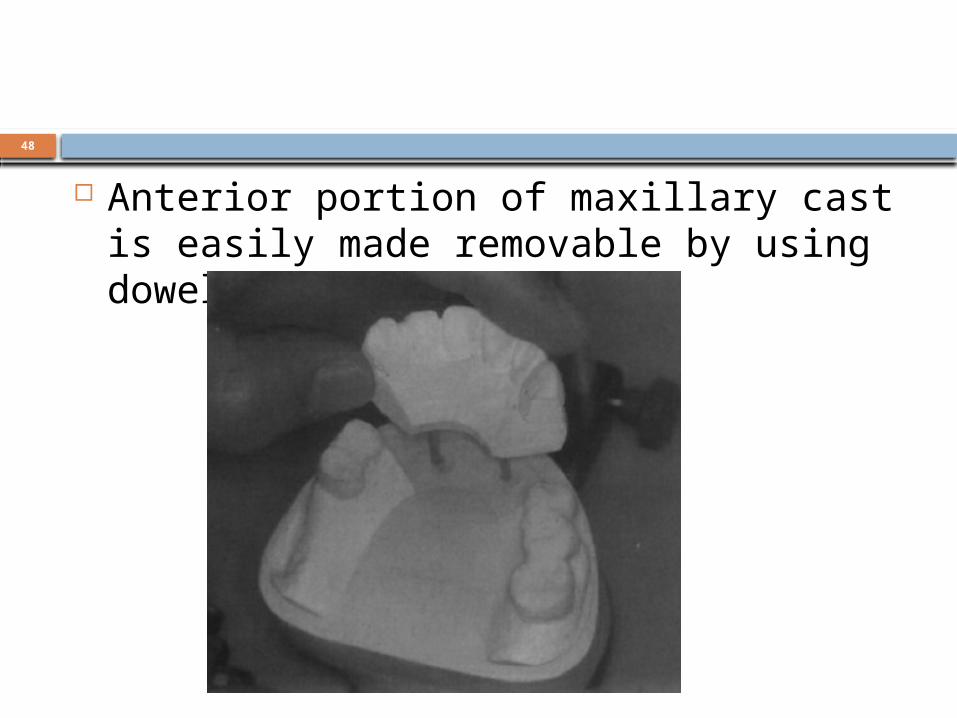
Anterior portion of maxillary cast is easily made removable by using dowel pins.
49
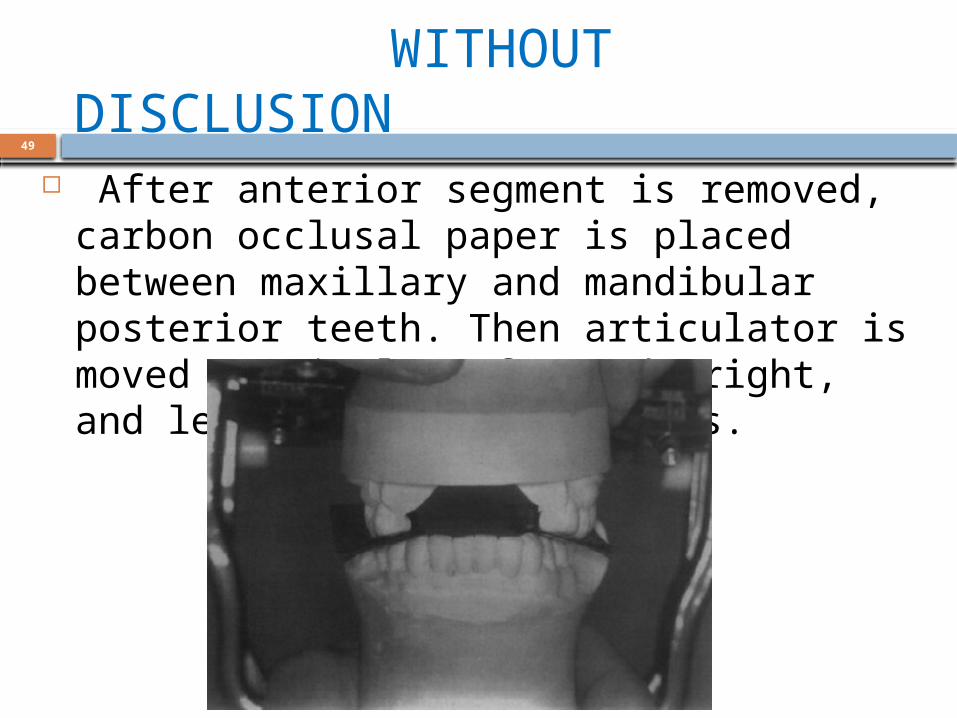
WITHOUT DISCLUSION After anterior segment is removed, carbon
occlusal paper is placed between maxillary and mandibular posterior teeth. Then articulator is moved to simulate forward, right, and left movement directions.
50
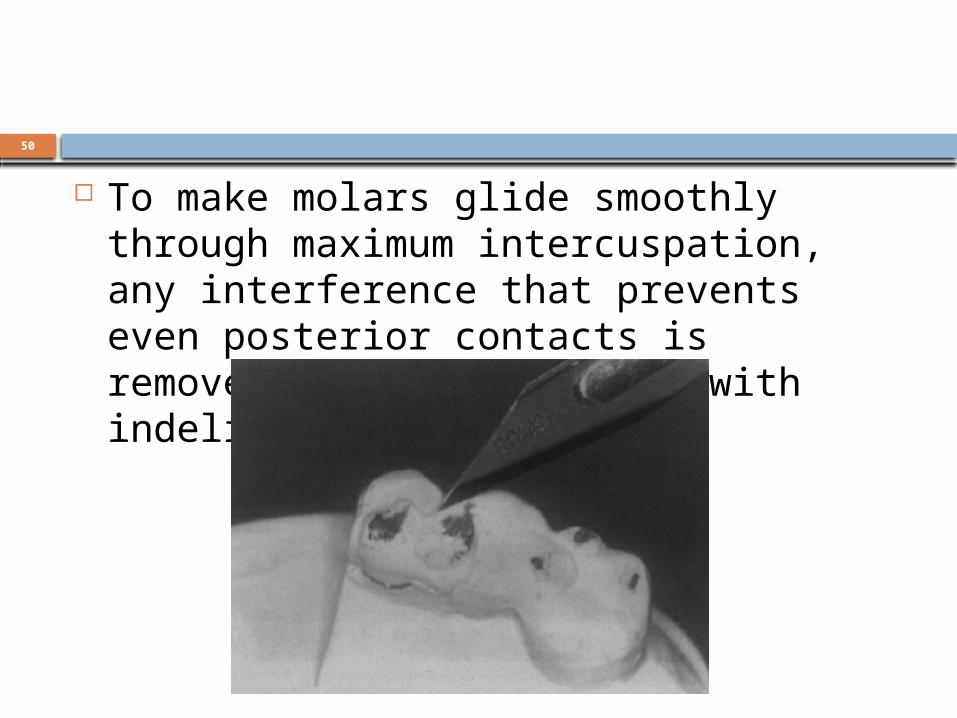
To make molars glide smoothly through maximum intercuspation, any interference that prevents even posterior contacts is removed. Areas are marked with indelible pen.
51
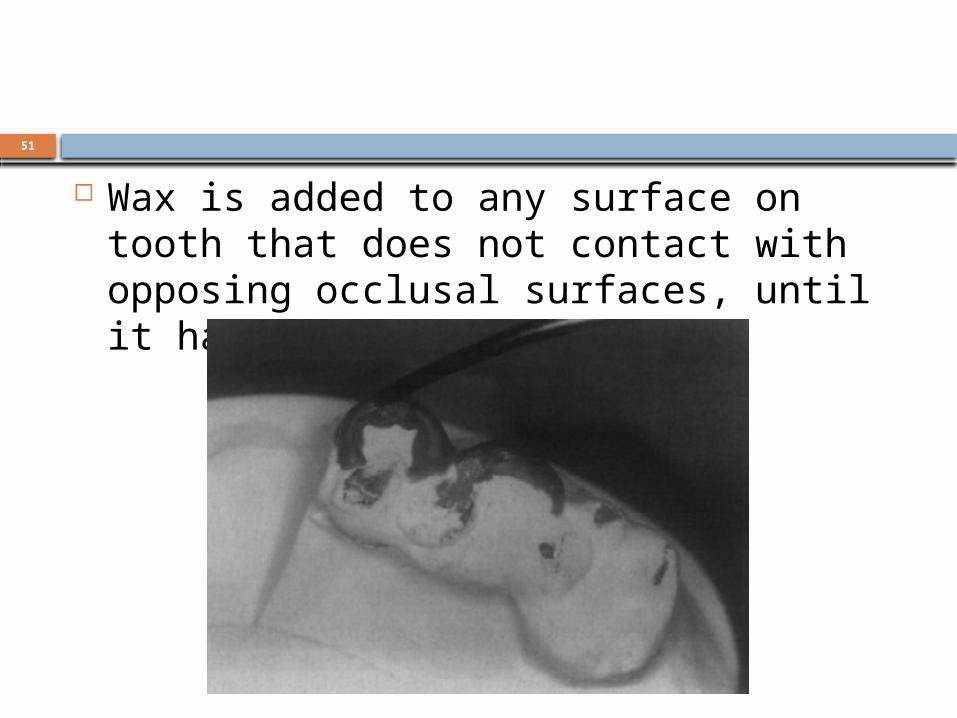
Wax is added to any surface on tooth that does not contact with opposing occlusal surfaces, until it has even contact.
52
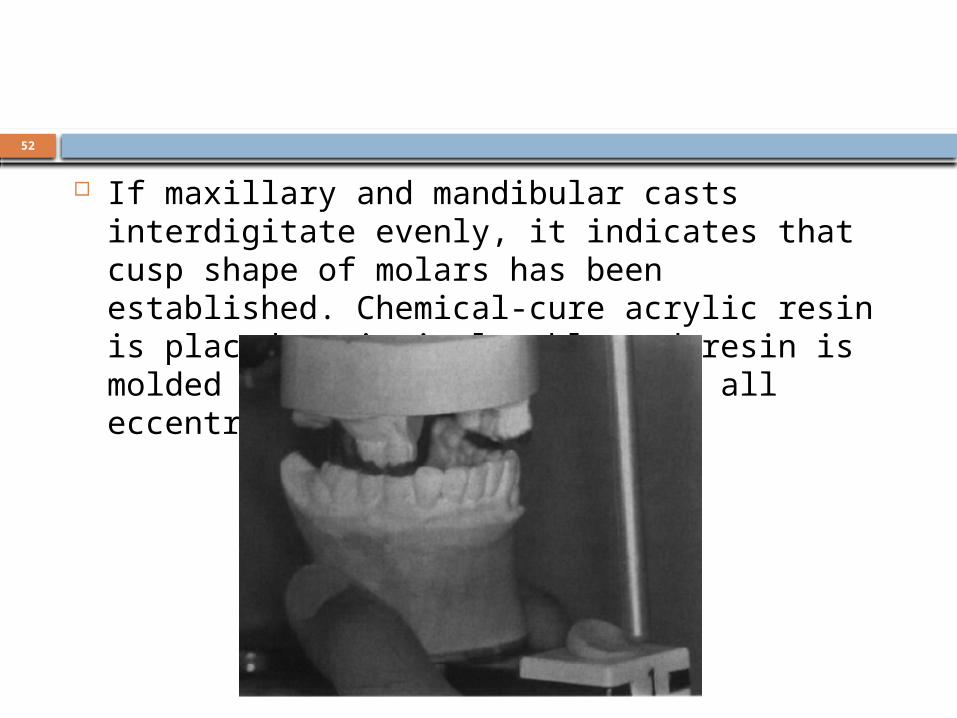
If maxillary and mandibular casts interdigitate
evenly, it indicates that cusp shape of molars has been established. Chemical-cure acrylic resin is placed on incisal table and resin is molded by moving articulator in all eccentric movements.

53
WITH DISCLUSION Three-millimeter thick plastic space is
placed in nonworking-side fossa box to approximate lateral movement

54
Vinyl sheet 1 mm thick is placed on tip of mesiobuccal cusp of mandibular first molar on nonworking side.

55
When articulator is closed, incisal pin is directed laterally and upward. Resin cone is formed to record this position.

56
Mounted maxillary and mandibular working casts and two incisal tables.

57
Anterior portion of maxillary working cast is removed after wax outlines are completed.
58
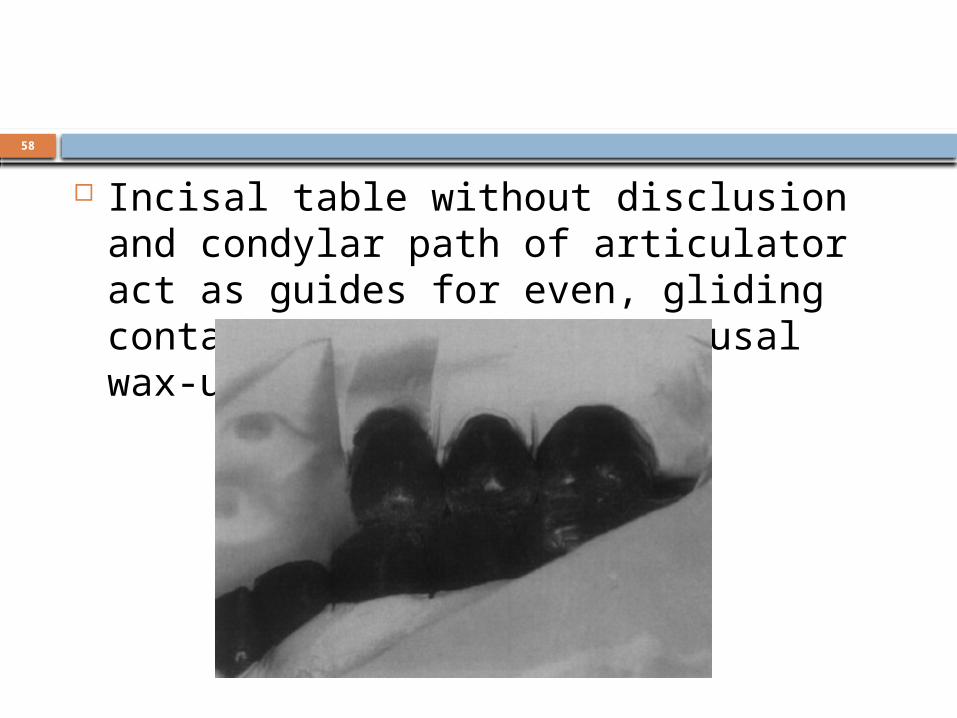
Incisal table without disclusion and condylar path of articulator act as guides for even, gliding contacts in posterior occlusal wax-ups.
59
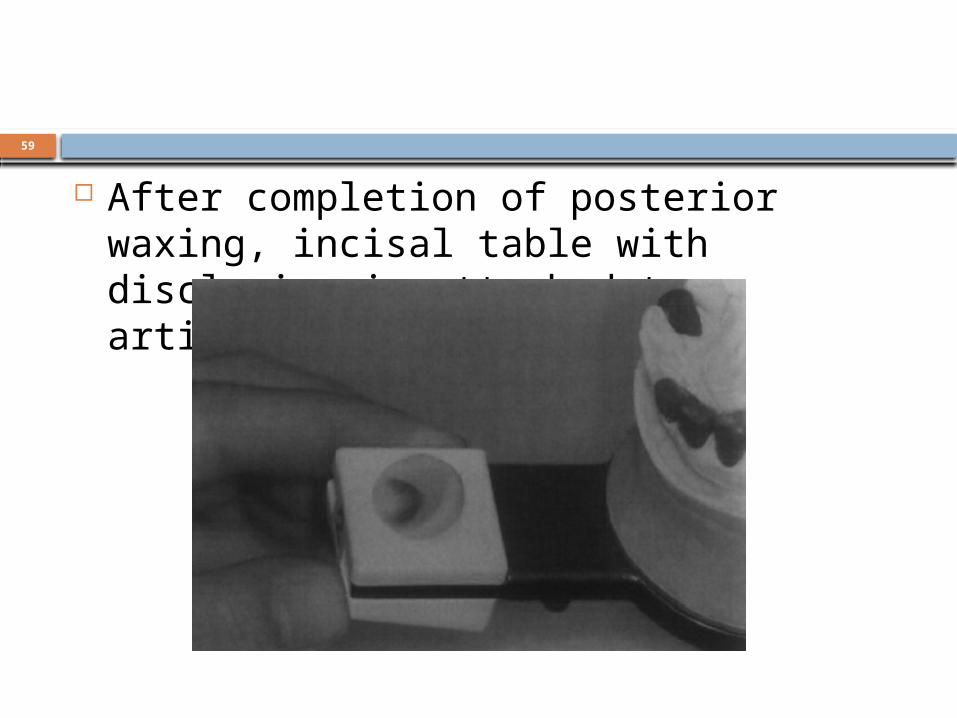
After completion of posterior waxing, incisal table with disclusion is attached to articulator.

60
Anterior segment is repositioned. Melted wax is added on lingual surfaces of anterior teeth; then articulator is closed and moved through all border movements to form anterior guidance.
61
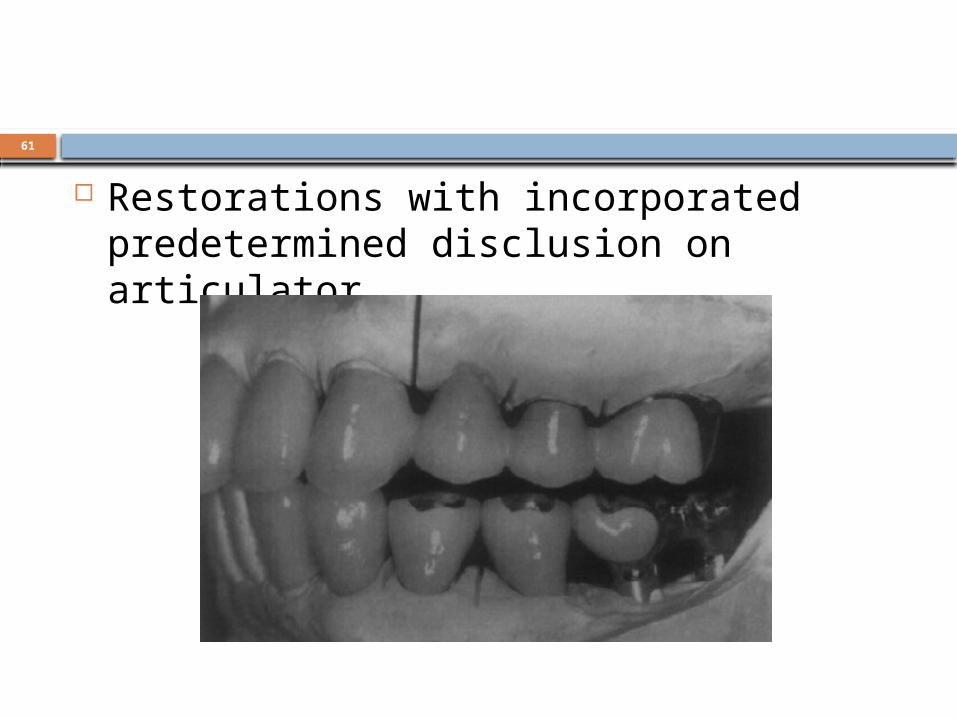
Restorations with incorporated predetermined disclusion on articulator.
62
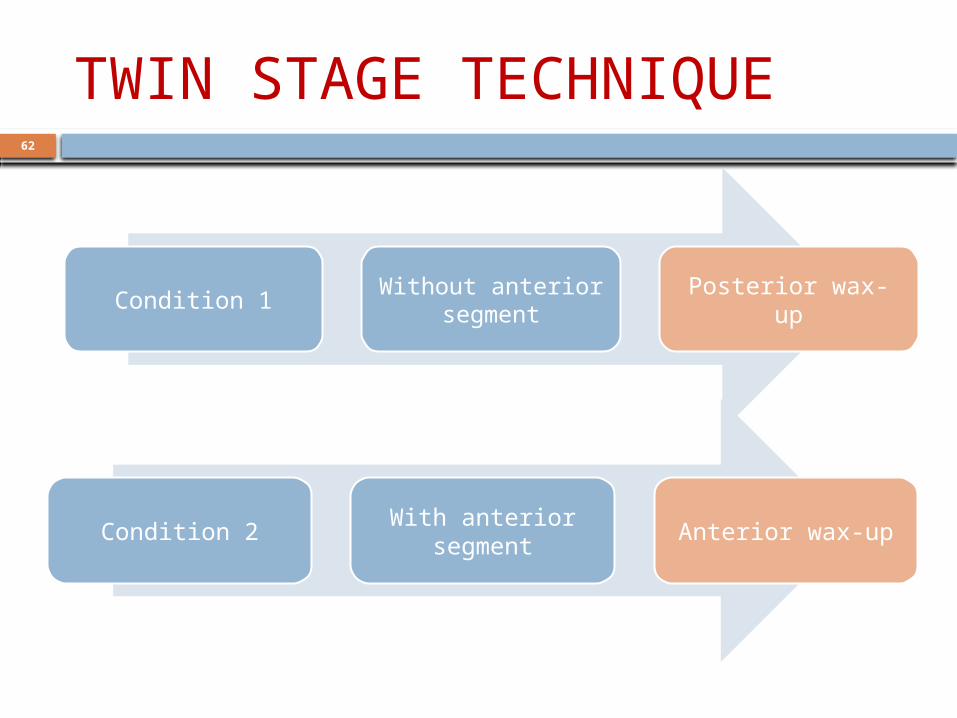
TWIN STAGE TECHNIQUE
Condition 1 Without anterior segment Posterior wax-up
Condition 2 With anterior segment Anterior wax-up

63
64
FABRICATION OF THE CUSP ANGLE According to "Condition 1,“ Adjust an articulator to the following values:
sagittal condylar path inclination =25 degrees, Bennett angle=15 degrees, sagittal inclination of the anterior guide table=25 degrees and lateral wing angle=10 degrees.
Make the anterior segment of the maxillary or mandibular cast removable using dowel pins. Remove the anterior segment. Make the maxillary and mandibular casts on the articulator so that they do not disocclude during eccentric movement
65
Wax the occlusal morphology of the posterior teeth so the maxillary and mandibular cusps contact during eccentric movement. Thus, a balanced articulation is obtained and every cusp will have a standard cusp angle.
66
FABRICATION OF ANTERIOR TEETH According to "Condition 2," adjust an
articulator to the following values: sagittal condylar path inclination=40 degrees, Bennett angle=15 degrees, sagittal inclination of the anterior guide table=45 degrees, and lateral wing angle=20 degrees
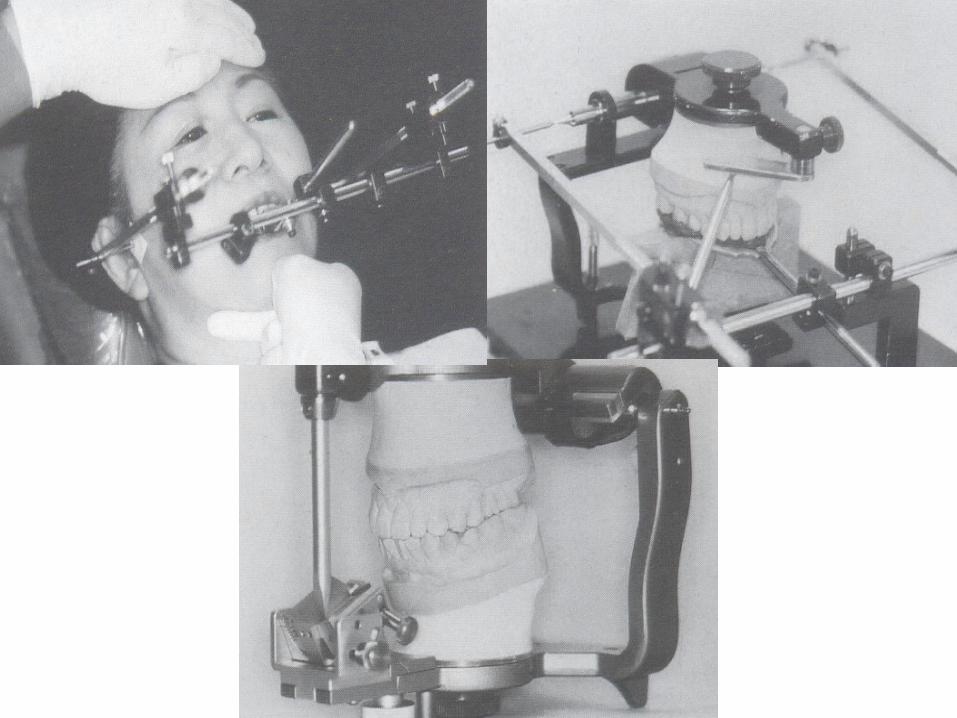
Reassemble the anterior segment of the cast. The maxillary and mandibular casts on the articulator produce the standard amount of disocclusion.
67
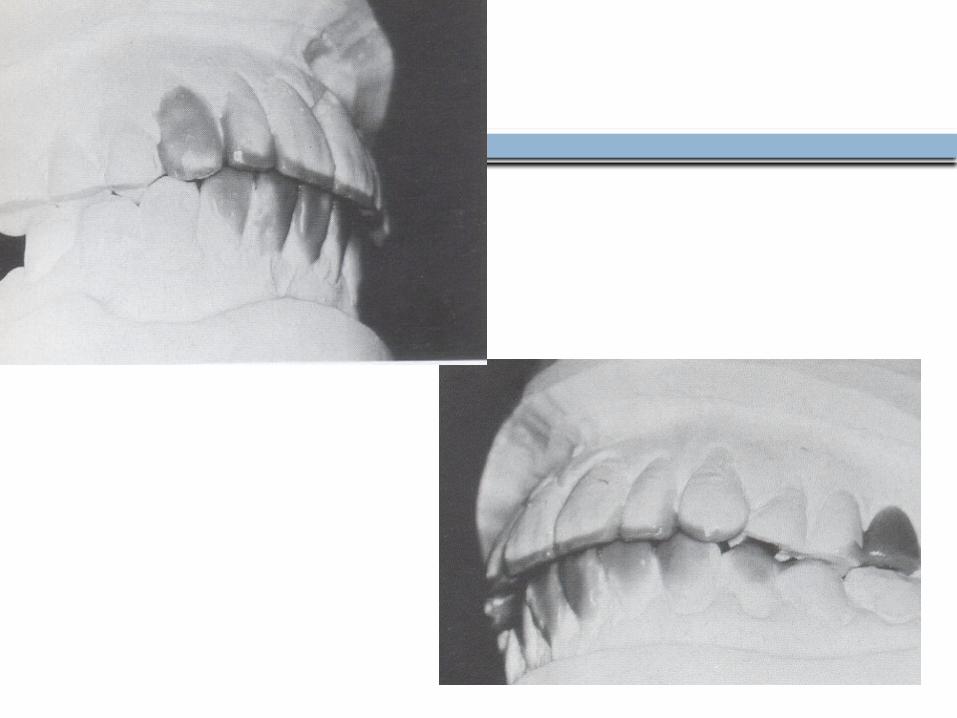
Wax the palatal contours of the maxillary anterior teeth so the maxillary and mandibular incisors contact during protrusive movement, and the maxillary and mandibular canines on the working side contact during lateral movement. Thus, anterior guidance is established and the standard amount of disocclusion will be produced.
68
69

70

71

72

73

74

75
76
77
78

79
Case Report

80
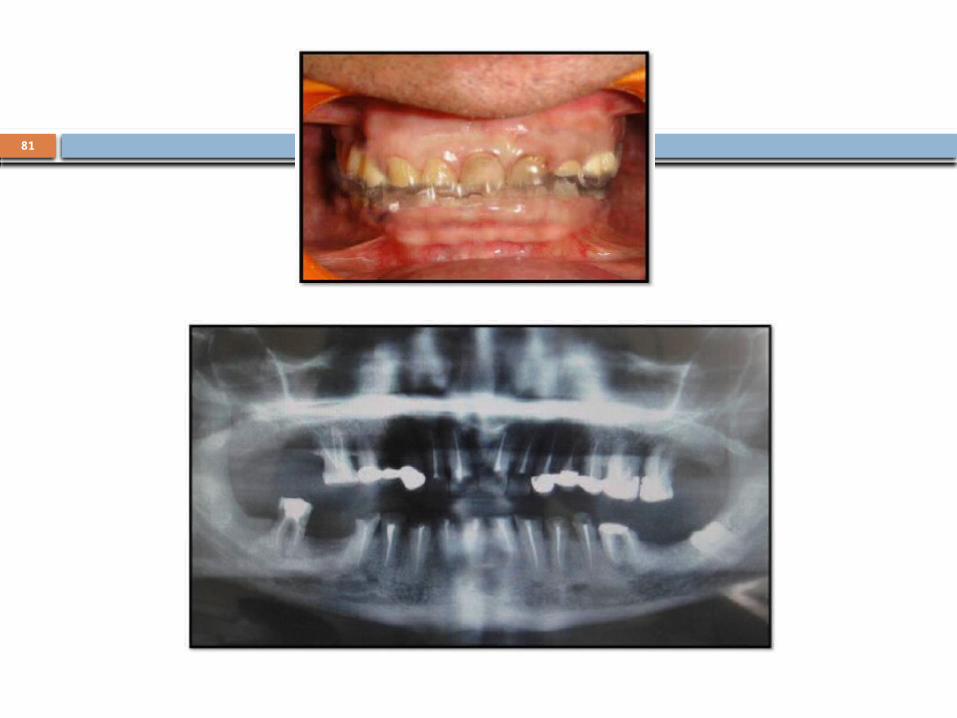
Diagnostic maxillary & mandibular impressions were made with irreversible hydrocolloid impression material and casts were retrieved. Occlusal equilibration was done in the patient’s mouth by removing the occlusal interferences so that centric relation coincided with maximum intercuspal position. Again impressions were made and the casts were articulated using an earpiece face bow (Hanau Springbow) over which maxillary occlusal splint was fabricated at increased vertical dimension. The permissive occlusal splint at centric relation position for 12 weeks was given to determine acceptability of proposed change in occlusal scheme.
81

82
Occlusal plane analysis
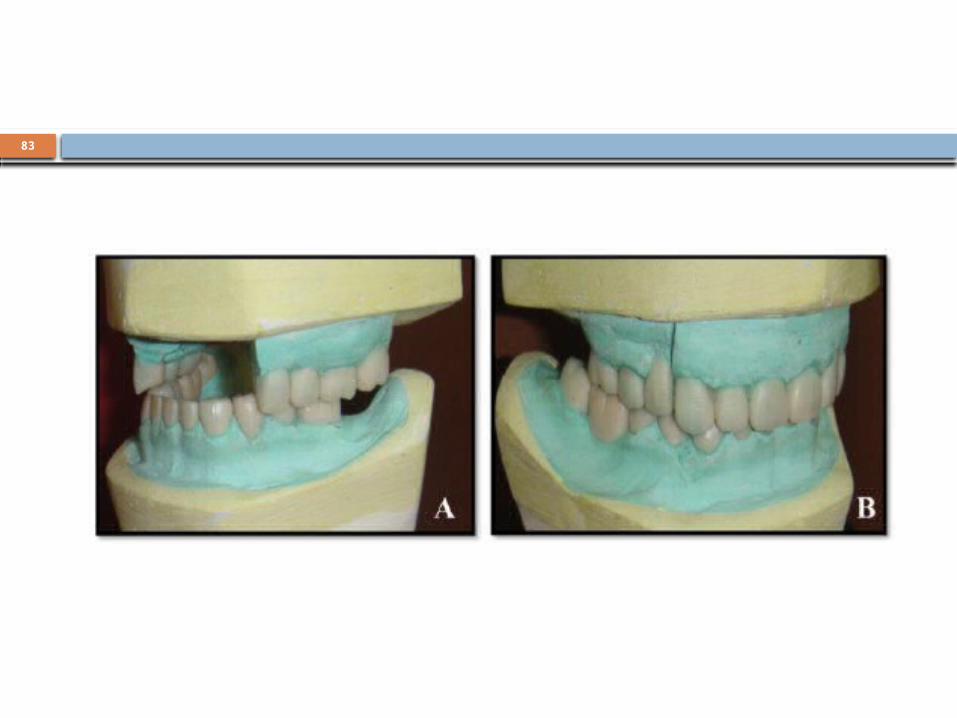
83

84

85

86
87
REFERENCES
Turner KA, Missirlian DM (1984) Restoration of the extremely worn dentition. J Prosthet Dent 52:467–474
Gary M. DeWood. Gnathology and Pankey-Mann-Schuyler : fulfilling the requirements of occlusion in oral rehabilitation
The University of Toledo The University of Toledo Digital Repository 2004 Stuart CE (1973) The contributions of gnathology to prosthodontics. J Prosthet
Dent 30:607–608 Stuart CE, Stallard H (1960) Principles involved in restoring occlusion of the
natural teeth. J Prosthet Dent 10:304–313 Schuyler CH (1959) An evaluation of incisal guidance and its influence on
restorative dentistry. J Prosthet Dent 9:374–378 Schuyler CH (1963) The function and importance of incisal guidance in oral
rehabilitation. J Prosthet Dent 13:1011–1029 Mann AW, Pankey LD (1960) Oral rehabilitation: part I. Use of the P-M
instrument in treatment planning and in restoring lower posterior teeth. J Prosthet Dent 10:135–150
Pankey LD, Mann AW (1960) Oral rehabilitation: part II.Reconstruction of the upper teeth using a functionally generated path technique. J Prosthet Dent 10:151–162

88
Hobo S (1991) Twin-tables technique for occlusal rehabilitation.Part I: mechanism of anterior guidance. J Prosthet Dent 66:299–303
Hobo S (1991) Twin-tables technique for occlusal rehabilitation. Part II: clinical procedures. J Prosthet Dent 66:471-477
Hobo S, Takayama H (1997) Twin-stage procedure. Part 1: a new method to reproduce precise eccentric occlusal relations. Int J Periodontic Restor Dent 17:113–123
Hobo S. Takayama H. effect of canine guidance on the working conduler path. Int J Prosthodont 1989;2:73-9
Hobo S. A kinematic investigation of mandibular border movement by means of an electronic measuring system. Part III. Rotational center of lateral movement. J PHOSTHET DENT 1984;52:66-72

89

90
FULL MOUTH REHABILITATION
PRESENTED BY : ILA YADAVPG STUDENT DEPT. OF PROSTHODONTICS
91
CONTENTS PART 1 Definition Indications Classification Occlusal approach and schemes Review of occlusal schemes Terminologies Hobo’s philosophy for full mouth rehabilitation Hobo’s Twin table technique Hobo’s Twin stage technique References

92
CONTENTSPART 21) Centric relation2) Vertical dimension3) Neutral zone4) Envelope of function5) Long centric6) PANKEY MANN SCHUYLER CONCEPTRestoring lower anterior teethRestoring upper anterior teeth

93
Restoring lower posteriors- occlusal palne analysisRestoring upper posteriors- functionally generated
path technique7) Solving specific problems Deep over biteAnterior overjetAnterior open biteEnd to end occlusionsSplayed teeth8) Postoperative careReferences

94
PRIMARY REQUIREMENTSFOR SUCCESSFUL OCCLUSAL THERAPY 1. Comfortable and stable TMJs - The jaw joints
must be able to function and accept loading forces with no discomfort. This is always the starting point for any dental treatment that involves the occlusal surfaces of the teeth.
2. Anterior teeth in harmony with the envelope of function and in proper relationship with the lips, the tongue, and the occlusal plane.
3. Non-interfering posterior teeth - Posterior occlusal contacts should not interfere with either the comfortable TMJs in the back or the anterior guidance in the front.

95
FORMULA FOR A PERFECTEDOCCLUSION The first step is to have simultaneous equal
intensity contacts on all teeth when the condyle-disk assemblies are completely seated up in their respective sockets.
The contact on the posterior teeth is on cusp tips (represented by dots.)
The lines on the anterior teeth represent continuous contact from centric relation to incisal edges as the mandible moves forward and laterally.
The formula “dots in back, lines in front”

96
CENTRIC RELATION The maxillomandibular relationship in
which the condyles articulate with the thinnest avascular portion of their respective disks with the complex in the anterior-superior position against the shapes of the articular eminencies. This position is independent of tooth contact. It is restricted to a purely rotary movement about the transverse horizontal axis (GPT-5)

97
2 most important criteria for centric relation are
1.The complete release of the inferior lateral pterygoid muscle
2.Proper alignment of the disk on the condyle
The condyles can freely rotate on a fixed axis in centric relation up to about 20 mm of jaw opening without moving out of the fully seated position in their respective fossa

98
Some common misconceptions Centric relation should not be confused
with centric occlusion, an obsolete term that has been replaced with maximum intercuspation.
Centric relation refers to the fully seated condylar position regardless of how the teeth fit.
Centric relation is not about teeth. It is about the position of the condyles.

99
Ignoring the position of the TMJs when examining the occlusion is not acceptable. Just putting the casts together in maximum intercuspation does not provide the necessary information regarding how the mandibular teeth relate to the maxillary teeth when the condyles are in their completely seated centric relation position, nor does it show what must be done to achieve harmony between the occlusion and the TMJs.

100
If the condyles are in centric relation, they can rotate on a fixed axis. Thus a bite record made at any point of opening on the correct centric relation arc (shown in red) is still in centric relation.
If the casts are mounted on an articulator with the correct condylar axis, the vertical dimension can be increased or decreased without introducing any error.
101
The mandible is in centric relation if five criteria are fulfilled:
1. The disk is properly aligned on both condyles. 2. The condyle-disk assemblies are at the highest
point possible against the posterior slopes of the eminence.
3. The medial pole of each condyle-disk assembly is braced by bone.
4. The inferior lateral pterygoid muscles have released contraction and are passive.
5. The TMJs can accept firm compressive loading with no sign of tenderness or tension.

102
Methods of manipulation for centric relation
ANTERIOR BITE STOPS
Directly Fabricated Anterior Deprogramming Device
The leaf gauge.

103
The Pankey Jig
The Best-bite Appliance
104
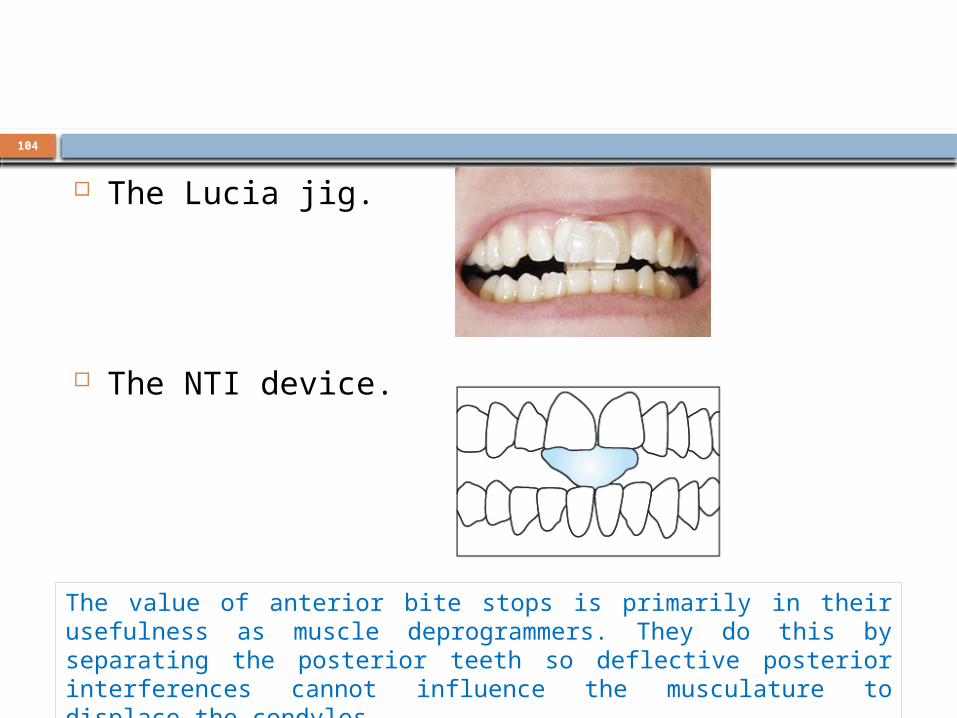
The Lucia jig.
The NTI device.
The value of anterior bite stops is primarily in their usefulness as muscle deprogrammers. They do this by separating the posterior teeth so deflective posterior interferences cannot influence the musculature to displace the condyles.

105
BILATERAL MANIPULATION Recline the patient all the way back. Point the
chin up. A supine patient is more relaxed and in a better
position for the operator to work while seated. Pointing the chin up makes it easier to position the fingers on the mandible and prevents the tendency of some patients to protrude the jaw.

106
Stabilize the head. Lower the patient’s head enough so you can cradle it between your rib cage and forearm
After the head is stabilized, lift the patient’s chin again to slightly stretch the neck.

107
Gently position the four fingers of each hand on the lower border of the mandible. The little finger should be slightly behind the angle of the mandible.
Position the pads of your fingers so they align with the bone, as if you were going to lift the head.
Keep all four fingers tightly together.

108
Bring the thumbs together to form a C with each hand.

109
With a very gentle touch, manipulate the jaw so it slowly hinges open and closed. As it hinges, the mandible will usually slip up into centric relation automatically if no pressure is applied. Any pressure applied before the condyles are completely seated will be resisted by the lateral pterygoid muscles.

110
After the mandible feels like it is hingeing freely and the condyles seem to be fully seated up in their fossae, the mandible is in centric relation.

111
VERTICAL DIMENSION The mandible-to-maxilla relationship,
established by the repetitive contracted length of the elevator muscles, determines the VDO.

112
Measurements from fixed bony landmarks show that the dimension to the cementoenamel junction (A) increases with tooth wear. The dimension from bone landmark to occlusal surface (B) remains even with severe wear

113
Rules for Determining the VDOon Patients with Teeth 1. The VDO that requires the least amount of
dentistry to satisfy esthetic and functional goals is always the VDO of choice. Extensive treatment done solely for the purpose of increasing the vertical dimension to a perceived stereotypical dimension is contraindicated.
2. Maximal intercuspation of the posterior teeth determines the existing VDO. This dimension will be in harmony with the jaw-to-jaw relationship established by the repetitive contracted length of the elevator muscles.
3. The muscle-determined VDO must be measured from origin to insertion of the elevator muscles. This is best measured clinically from the zygoma to the angle of the mandible, the origin to insertion dimension of the masseter muscle.

114
4. The position of the condyles during maximal intercuspation must be considered when evaluating VDO. This is so because any change up or down of the condyles affects muscle length during maximal intercuspation.
5. If the VDO must be changed, it should be determined at the point of anterior teeth contact. If posterior interferences prevent anterior contact in centric relation and occlusal equilibration is determined to be the best choice of treatment, the posterior teeth may be adjusted until anterior contact is achieved in centric relation
115
6. Changing the VDO by either increasing or decreasing it is tolerated well by patients and within reason causes no harm to teeth or supporting structures if tooth contact includes the complete arches and the condyles are completely seated in centric relation during maximal intercuspation.
7. Changes in the true VDO are not permanent. The VDO will return to its original dimension measurable at the masseter muscle. Unnecessary increases in the VDO are contraindicated as they are not maintained.

116
Although there are valid reasons for increasing the vertical dimension, most bite raising has been traditionally done for one of the following invalid reasons:
1. To relieve a TMD. 2. To “unload” the TMJs. 3. To restore “lost” vertical dimension in a
severely worn occlusion. 4. To get rid of facial wrinkles

117
THE NEUTRAL ZONE Teeth are the most movable part of the
masticatory system. If outward horizontal forces from the tongue are greater than inward forces exerted by the buccinator muscle bands and the lips, the teeth will move horizontally until the opposing forces are equal. This zone where the opposing forces are equal is the neutral zone.
118
The neutral zone Considerations 1.The teeth and their alveolar process are the most adaptive
part of the masticatory system .They can be moved horizontally or vertically by light forces
2.There is neutral zone within which muscular pressure against the dentition is equalized from the opposite directions
3. If irregularities of the tooth position, allignment or contour can be corrected within the neutral zone ,the prognosis for the long term stability is good
4. A problem occurs when the neutral zone is not where we want the teeth to be
5.A treatment decision then must allow determination of if and how we can change the neutral zone to orient it where we want the teeth to be

119
Methods for altering the neutral zone 1.Orthodontics –by re aligning the teeth 2. Elimination of the noxious habits 3.Myofunctional therapy 4.Reduction of the tongue size (surgical) 5.Surgical lengthening of the buccinator
band 6.Vestibuloplasty

120
THE ENVELOPE OF FUNCTION Every tooth in the mandible (the only moving
jaw) has an envelope of motion that outlines the outer limits to which each lower tooth can be moved.
More than any other factor, the neutral zone programs the envelope of function. This is so because the neutral zone is the major determinant of how the anterior teeth erupt into the mouth, and it is the position of the anterior teeth that influences the neuromuscular programming of functional jaw movements

121
The envelope of function dictates incisal edge position and consequentially determines the anterior guidance.
Variations in the envelope of function result naturally from how the anterior teeth were guided during eruption into their neutralzone position by the tongue and the lips.
Mechanoreceptors in and around the teeth program the muscles for functional jaw movements. The incisal edge position should be in harmony with the envelope of function.
122
LONG CENTRIC
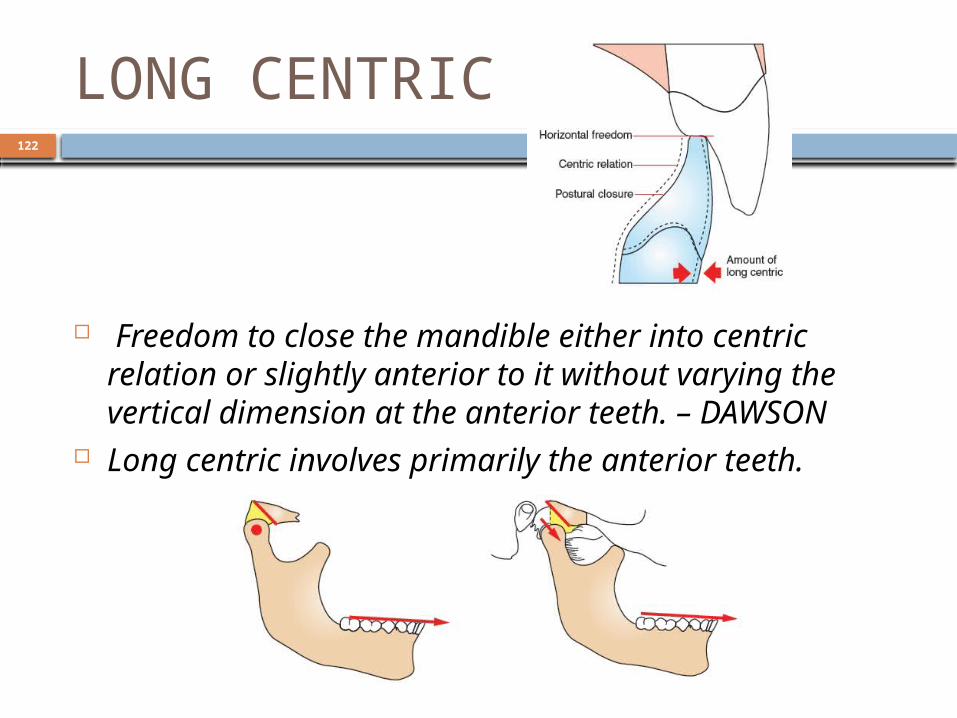
Freedom to close the mandible either into centric relation or slightly anterior to it without varying the vertical dimension at the anterior teeth. – DAWSON
Long centric involves primarily the anterior teeth.

123
How to record long centric Gentle tapping (unguided) on a red marking
ribbon shows interferences to postural closure. Manipulation to centric relation with guided
closure overlays black centric relation contacts on red postural contacts
If red marks appear on inclines forward of centric relation contacts (arrows),it indicates a need to extend the centric relation contact forward.

124
If the incline forward of centric relation marks, it is relieved so the incline does not touch during gentle unguided closure.
The amount of relief required is never more than 0.5 mm.

125
PANKEY-MANN-SCHUYLER CONCEPT
Practical philosophies for occlusal rehabilitation is the rationale or treatment that was originally organized into a workable concept by DR. L.D. PANKEY.Utilizing the "Principles of occlusion" espoused by Dr. Clyde Schuyler, Dr.Pankey integrated different aspects of several treatment approaches into an orderly plan for achieving an optimum occlusal result.
126
The goals of full mouth rehabilitaton are fulfilled by the following these principles :
1. A static coordinated occlusal contact of the maximum number of the teeth when the mandible is in the centric relation
2. An anterior guidance that is in harmony with the function in lateral eccentric positions on the working sides
3. Disclusion by the anterior guidance of all posterior teeth in protrusion
4. Disclusions of the non –working side inclines in lateral excursions
5. Group function of the working side inclines in lateral excursions

127
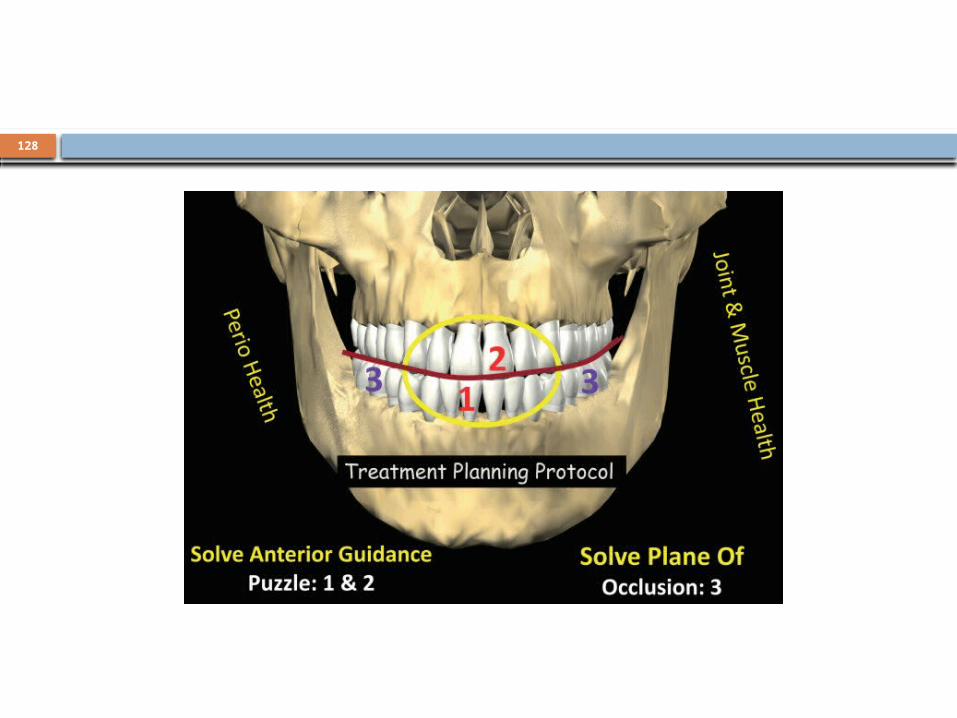
Sequence advocated by the PMS philosophy
Part 1. Examination , diagnosis ,treatment planning ,prognosis
Part 2. Harmonization of the anterior guidance for the best possible 1.Esthetics 2.Function 3.Comfort
Part 3. Selection of an acceptable occlusal plane and restoration of the lower posterior occlusion in harmony with the anterior guidance in a manner that will not interfere with the condylar guidance
Part 4. Restoration of the upper posterior occlusion in harmony with the anterior guidance and condylar guidance. The functionally generated path technique is so closely allied to this reconstruction technique.
128

129
Advantages of the P-M-S technique are 1. Possible to diagnose for entire rehabilitation before a single
tooth is prepared 2. It is well organised logical procedure that progresses
smoothly 3. There is never need to prepare or rebuild more than 8 teeth
at a time 4. It divides the rehabilitation into series of appointments5. There is no danger of losing patients present vertical
dimension 6. All posterior contours are programmed by and are in
harmony with both condylar border movements and perfect anterior guidance

130
RESTORING LOWER ANTERIOR TEETH
The starting point for the occlusal scheme INCISAL EDGE POSITION
The determination of incisal edge position requires
three decisions: 1. The curvature of the incisal plane 2. The height of the incisal plane 3. The horizontal position of the incisal edges
131
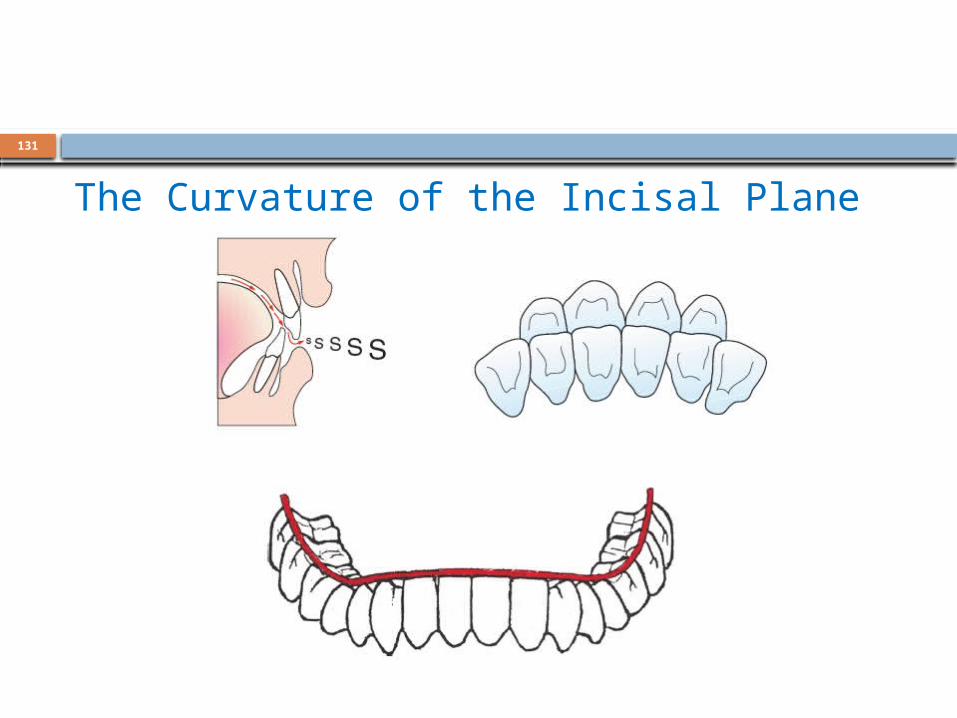
The Curvature of the Incisal Plane
132
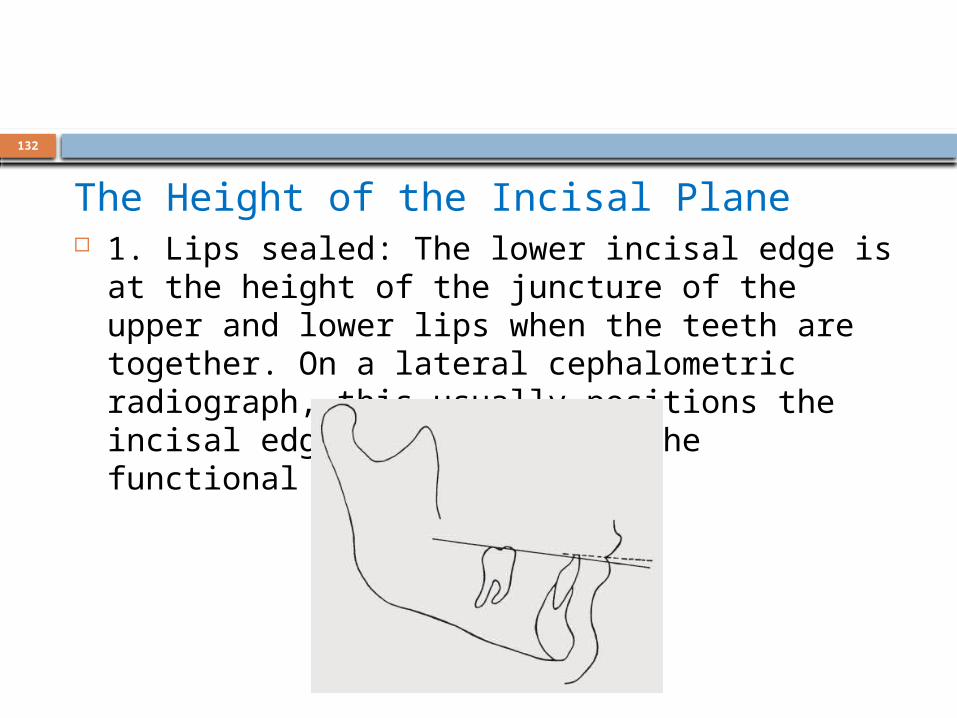
The Height of the Incisal Plane 1. Lips sealed: The lower incisal edge is at the
height of the juncture of the upper and lower lips when the teeth are together. On a lateral cephalometric radiograph, this usually positions the incisal edge slightly above the functional occlusal plane.

133
2. Speaking: “The view” when speaking is of the incisal edges
of the lower anterior teeth. A varying amount of labial contour may also be on display. The upper teeth are usually hidden during speech.

134
3. Smiling: Only the upper anterior teeth are typically on display during smiling. The lower incisors are usually hidden during a big smile.

135
4. Lips slightly parted: When the jaw is at rest and the lips are slightly parted in a half smile, both upper and lower labial surfaces are about equally on display.
136
The horizontal position of the lower incisal edges
The key to determining the horizontal position of lower incisal edges lies in establishing stable holding contacts with the upper anterior teeth.
137
RESTORING UPPER ANTERIOR TEETH
7 factors that determine labial and lingual contours and relate them to the correct incisal edge position as follows :
1.Mandible –to-maxilla relationship at centric relation 2. Lip support 3. Lip closure path 4. Tooth to lip relationship during formation of “f”
and “v” sounds 5. Envelope of function 6.Tooth to tooth relationships during the s sound 7. Neutral zone
138
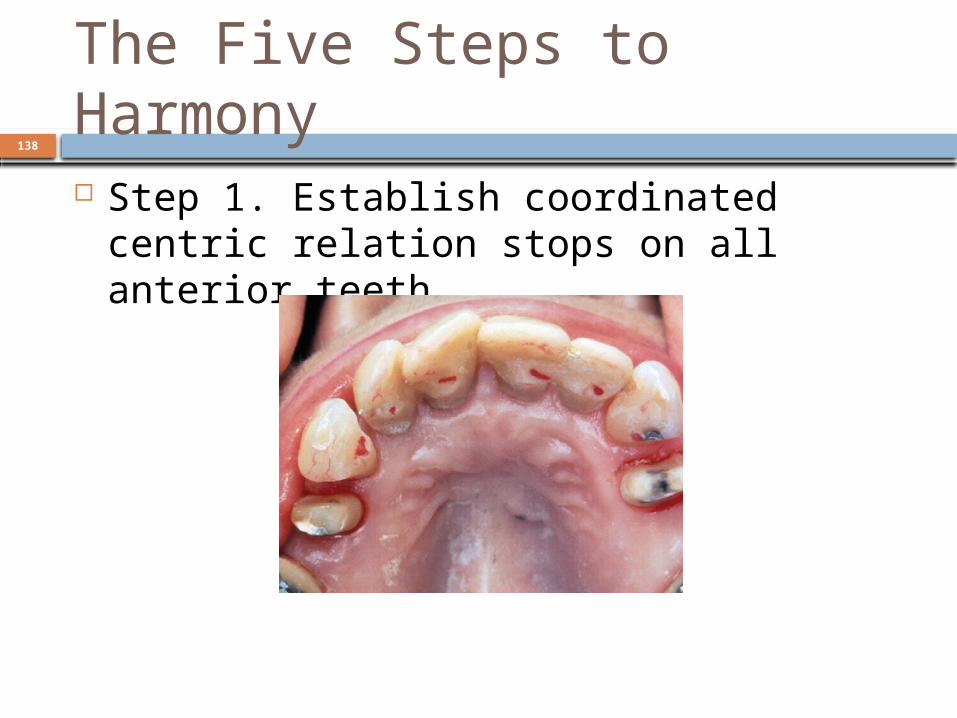
The Five Steps to Harmony Step 1. Establish coordinated centric
relation stops on all anterior teeth
139
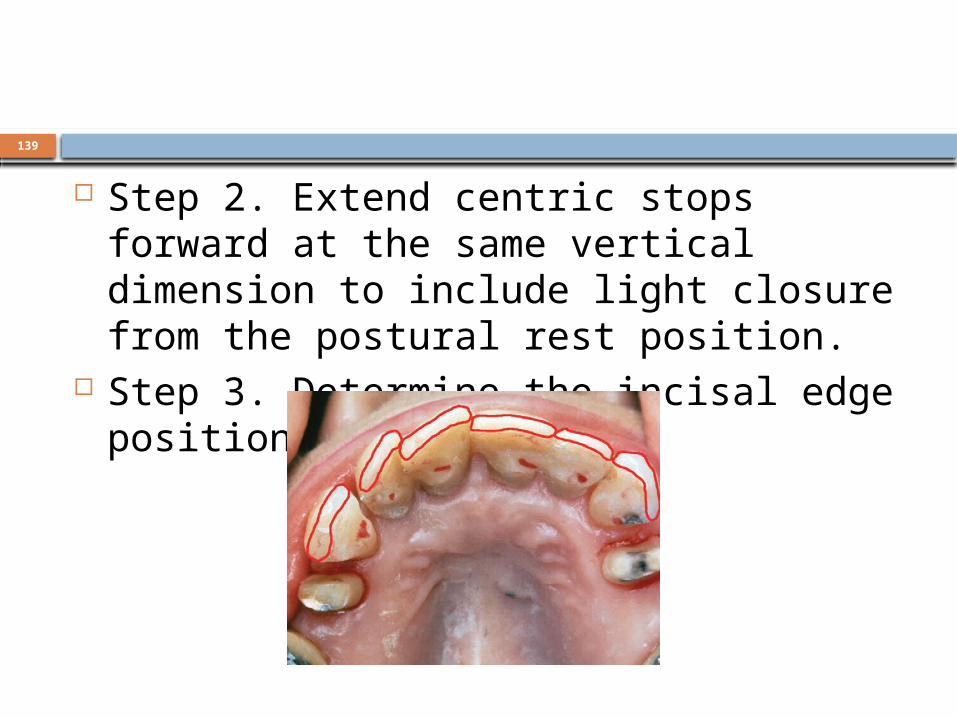
Step 2. Extend centric stops forward at the same vertical dimension to include light closure from the postural rest position.
Step 3. Determine the incisal edge position.

140
Step 4. Establish group function in straight protrusion.

141
Step 5. Establish ideal anterior stress distribution in lateral excursions.

142
The matrix of functionalanatomy
The matrix of functional anatomy describes six specific surfaces of upper anterior teeth that define their contour boundaries.

143
Quick review: Determining anterior tooth position and contour
Step 1: Refine and verify lower incisal edge position, shape, and plane. If upper anterior position has not been determined, it must be done in combination with lower determinations.
144
Step 2: Establish centric holding stops. This is always the first step. The correct anterior guidance cannot be determined until all interferences to centric relation have been eliminated.
145
Step 3: Lip support in line with alveolar contour. The upper half of the labial contour can be determined fairly well on the cast. The upper impression must include the complete contour of the alveolar process.
146
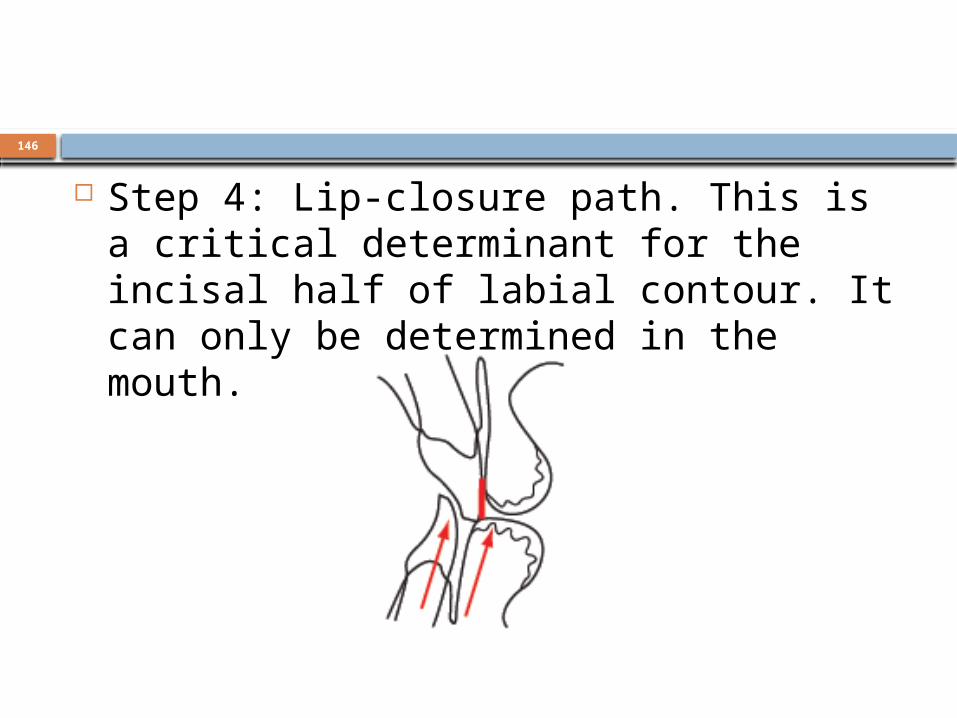
Step 4: Lip-closure path. This is a critical determinant for the incisal half of labial contour. It can only be determined in the mouth.

147
Step 5: Determine incisal edge length (using the smile line). This relationship is important for phonetics of the F and V positions as well as for the best esthetics.

148
Step 6: Refine incisal edge position (using F and V sounds). Determination must be made with gentle, softly spoken sounds. Make sure incisal plane contacts inner vermillion border during gentle speech.

149
Step 7: Adjust for long centric (if needed). Follow the rules for anterior guidance after centric relation and incisal edges have been determined.

150
Step 8: Establish lingual contours (anterior guidance) in harmony with the envelope of function:
a. in straight protrusiveb. in lateral excursions
151
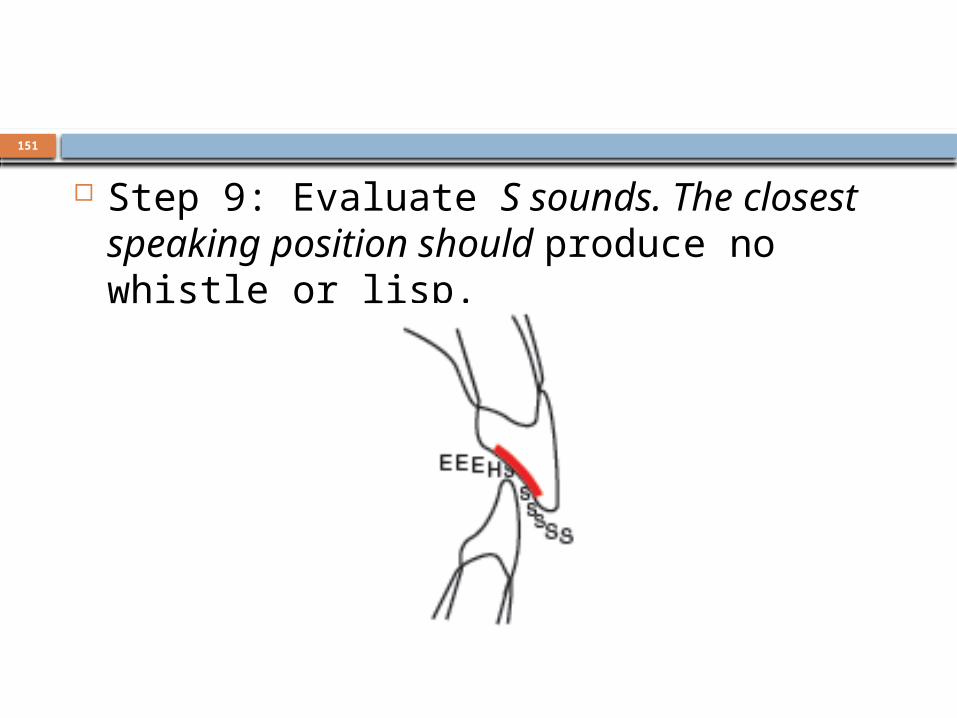
Step 9: Evaluate S sounds. The closest speaking position should produce no whistle or lisp.

152
Step 10: Evaluate cingulum contours (using T and D). Round into centric stops.

153
154
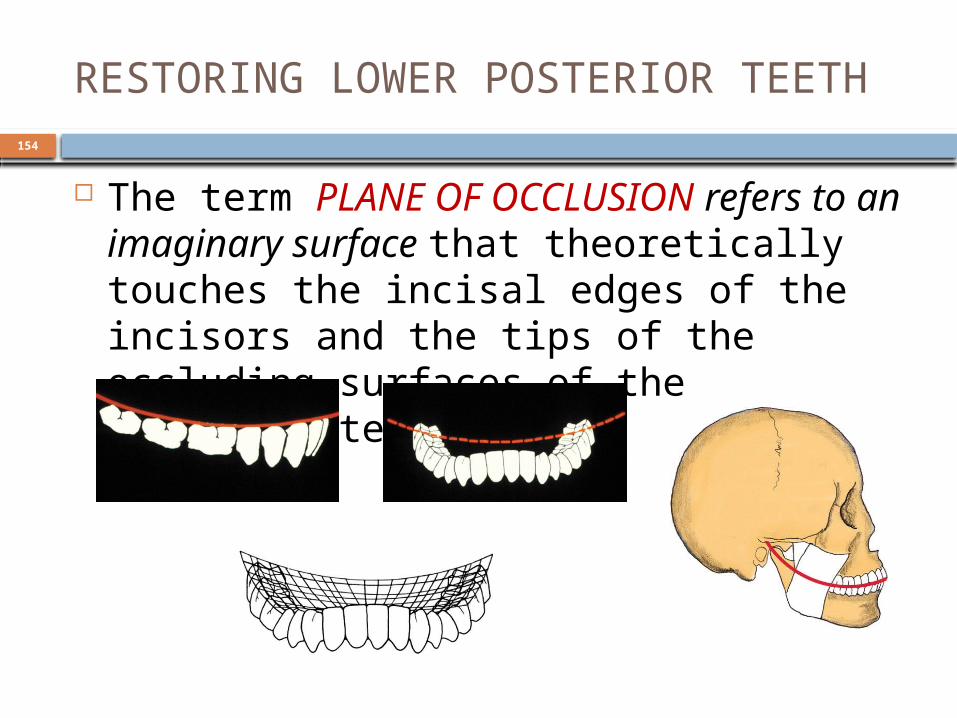
RESTORING LOWER POSTERIOR TEETH
The term PLANE OF OCCLUSION refers to an imaginary surface that theoretically touches the incisal edges of the incisors and the tips of the occluding surfaces of the posterior teeth.
155
Occlusal plane analysis Simplified occlusal plane analyser Broadrick’s occlusal plane analyser A SOPA is preset at 4 inches from the
condylar axis. The SOPA works with DenarR (Teledyne Waterpik™) articulators.
The Broadrick flag accomplishes the same occlusal analysis on almost all types of semiadjustable articulators.
156

157
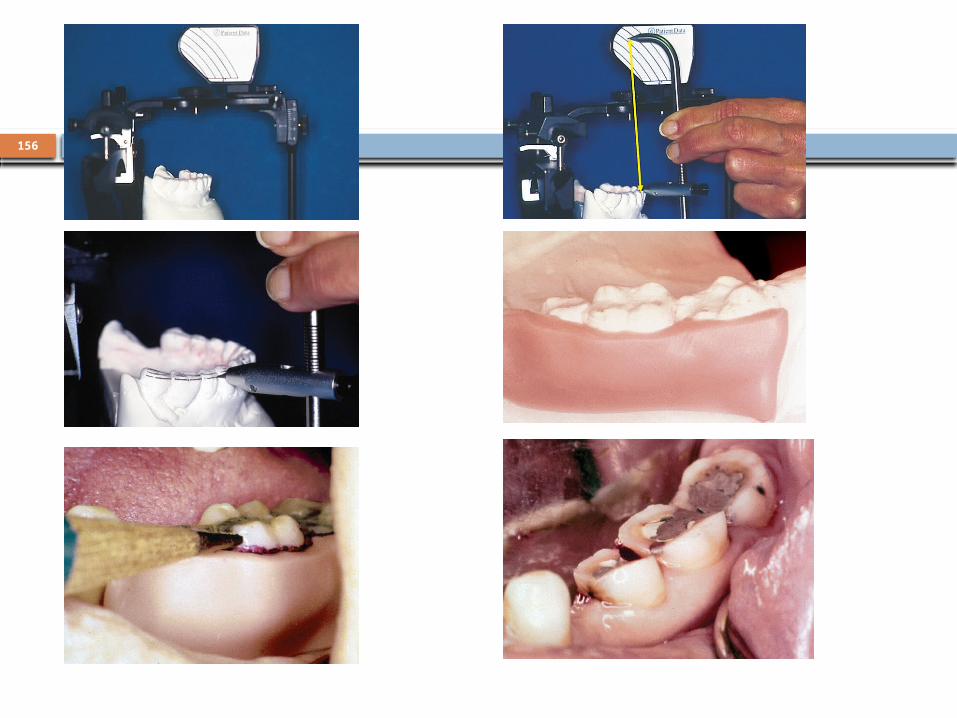
Making the fossa contour guide Step 1: The regular incisal guide pin is removed
and replaced with the special fossa-contour pin. The blade of the pin is indented into a mound of wax on a flat plastic guide table.

158
Steps 2 and 3: The upper bow is moved into left and right excursions, allowing the contours of the lateral anterior guidance to determine the path that the guide pin cuts into the wax.
159
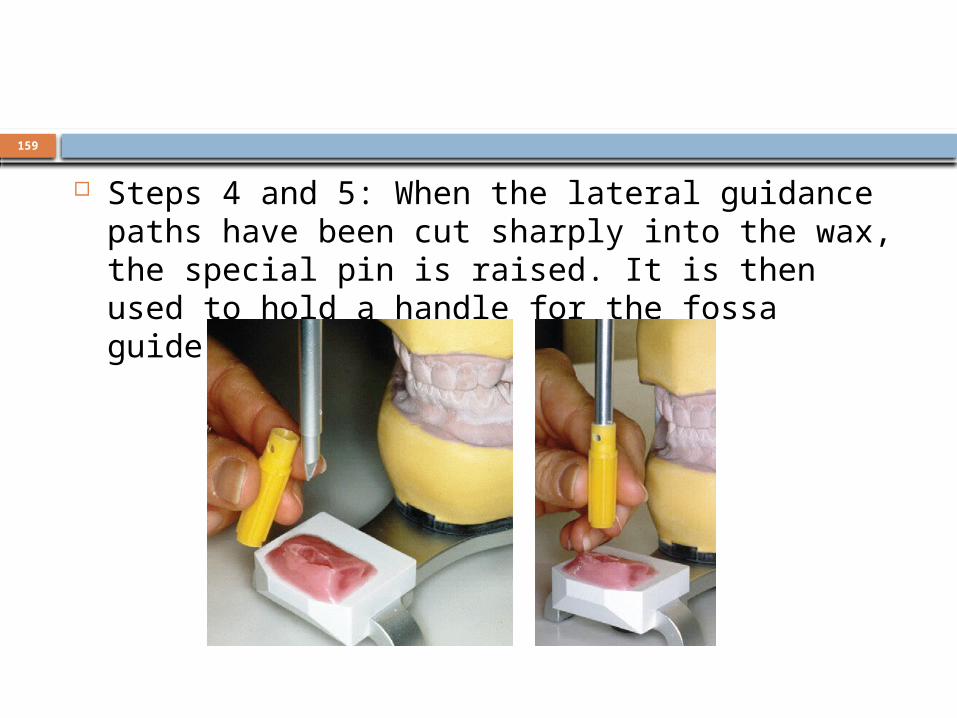
Steps 4 and 5: When the lateral guidance paths have been cut sharply into the wax, the special pin is raised. It is then used to hold a handle for the fossa guide.
160
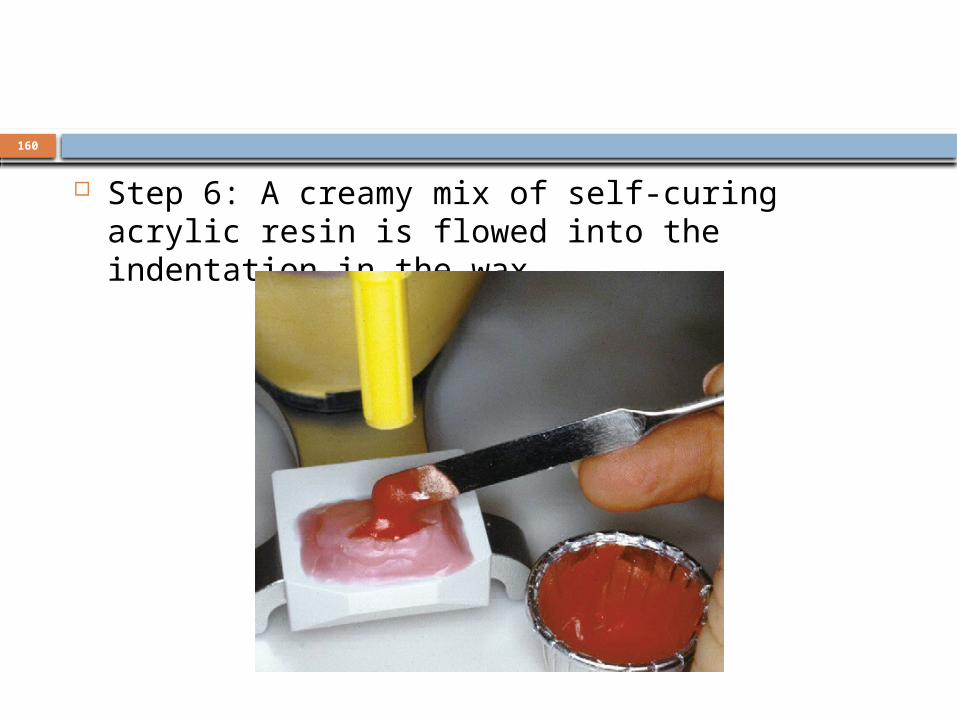
Step 6: A creamy mix of self-curing acrylic resin is flowed into the indentation in the wax.
161
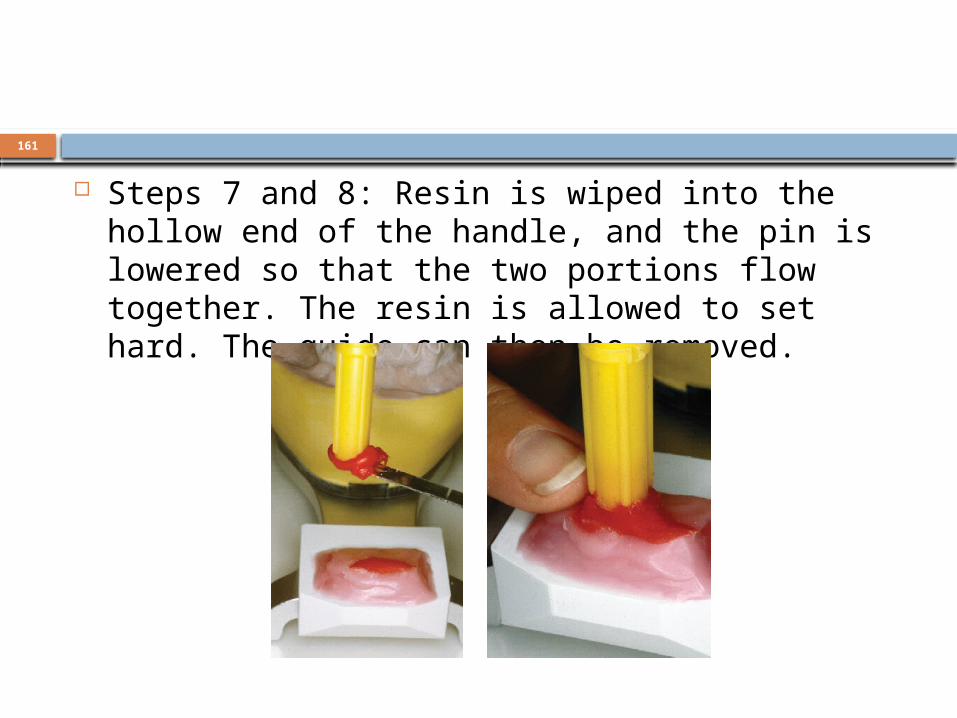
Steps 7 and 8: Resin is wiped into the hollow end of the handle, and the pin is lowered so that the two portions flow together. The resin is allowed to set hard. The guide can then be removed.
162
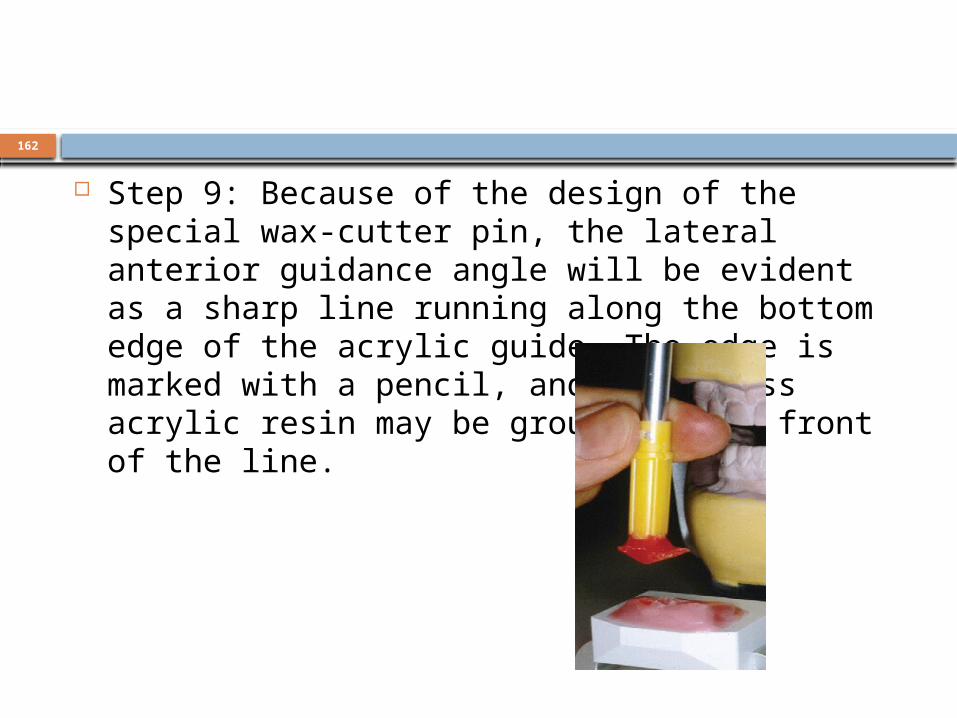
Step 9: Because of the design of the special wax-cutter pin, the lateral anterior guidance angle will be evident as a sharp line running along the bottom edge of the acrylic guide. The edge is marked with a pencil, and any excess acrylic resin may be ground off in front of the line.
163
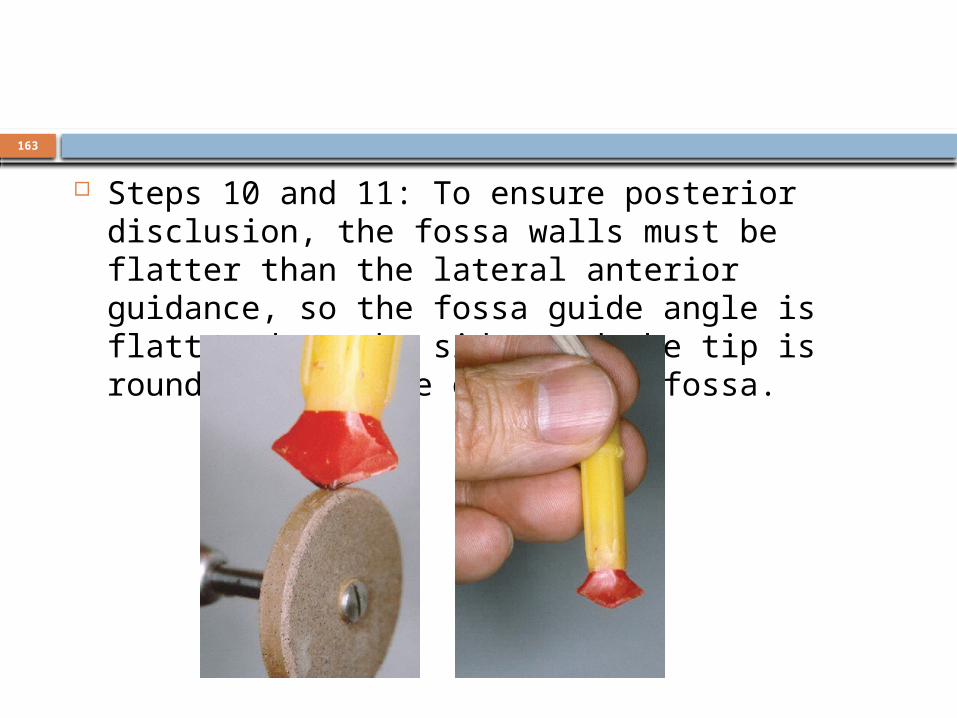
Steps 10 and 11: To ensure posterior disclusion, the fossa walls must be flatter than the lateral anterior guidance, so the fossa guide angle is flattened on the sides and the tip is rounded to a more opened-out fossa.
164
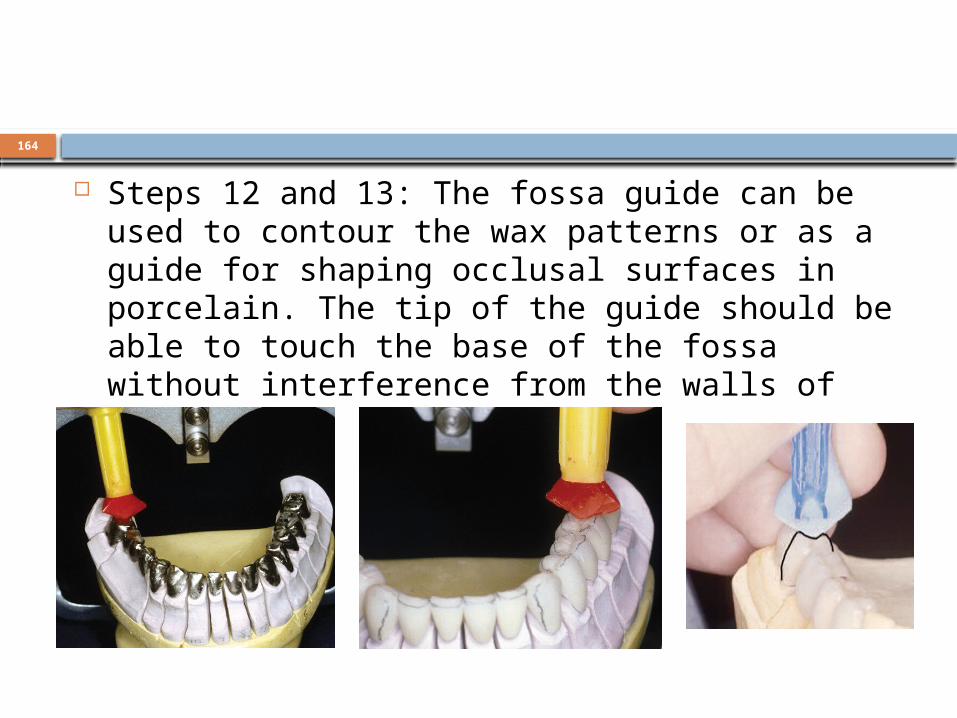
Steps 12 and 13: The fossa guide can be used to contour the wax patterns or as a guide for shaping occlusal surfaces in porcelain. The tip of the guide should be able to touch the base of the fossa without interference from the walls of the fossa.
165
RESTORING UPPER POSTERIOR TEETH
The maxillary posterior teeth are restored with a FUNCTIONALLY GENERATED PATH MODEL that incorporates all movements of the mandiblur
teeth against the maxillary teeth within the patient’s constants (intercondylar distance, terminal hinge axis, interocclusal relationship, and condylar pathways) and the variables (tooth form and position, vertical dimension of occlusion, and anterior guidance) determined and captured in the provisionals and subsequently transferred to the completed restorations in the anterior and mandibular posterior.
166
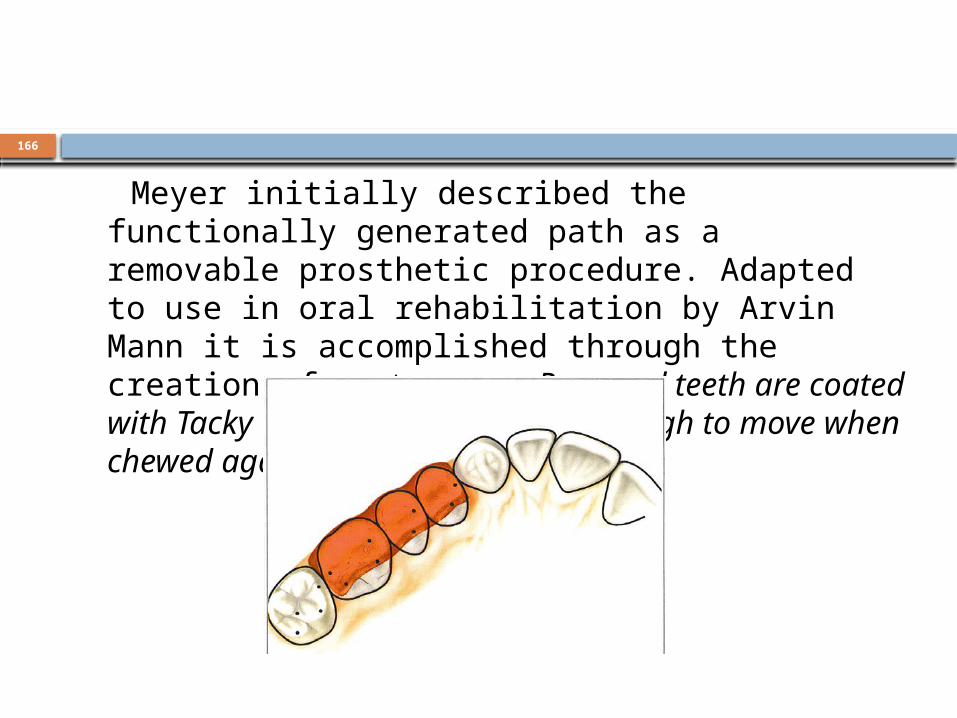
Meyer initially described the functionally generated path as a removable prosthetic procedure. Adapted to use in oral rehabilitation by Arvin Mann it is accomplished through the creation of a stone core. Prepared teeth are coated with Tacky Wax, a wax that is soft enough to move when chewed against.

167
The patient is directed to move through all possible movements and chewing patterns. The wax offers no resistance to the movement and is thus carved into the shape of the movements of the lower teeth against it.

168
The tacky wax shaped by the patient’s movements
169
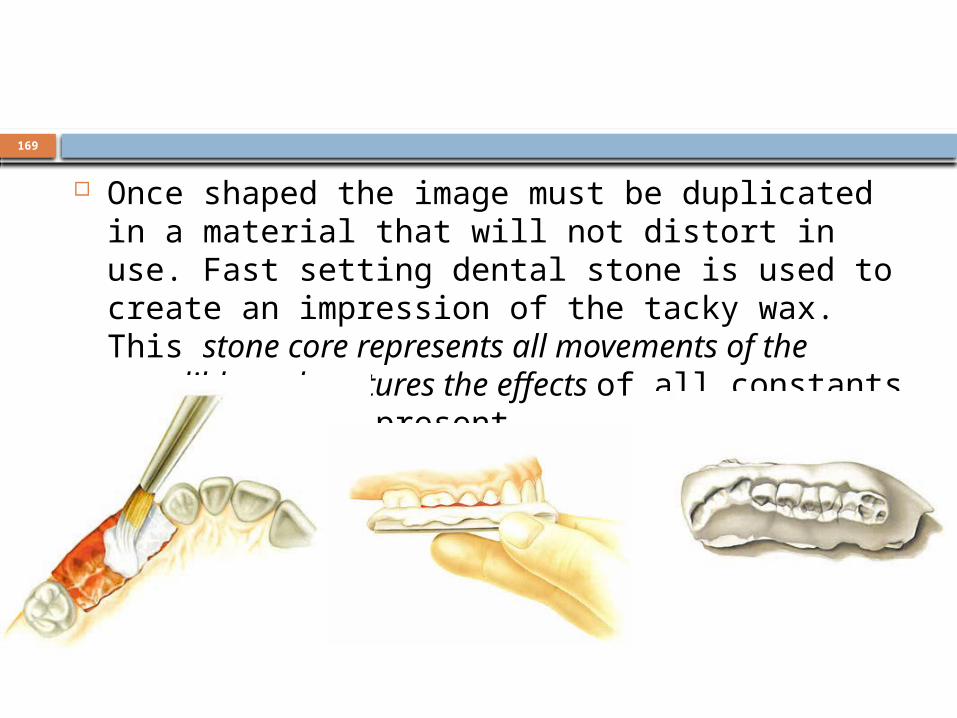
Once shaped the image must be duplicated in a material that will not distort in use. Fast setting dental stone is used to create an impression of the tacky wax. This stone core represents all movements of the mandible and captures the effects of all constants and variables present.
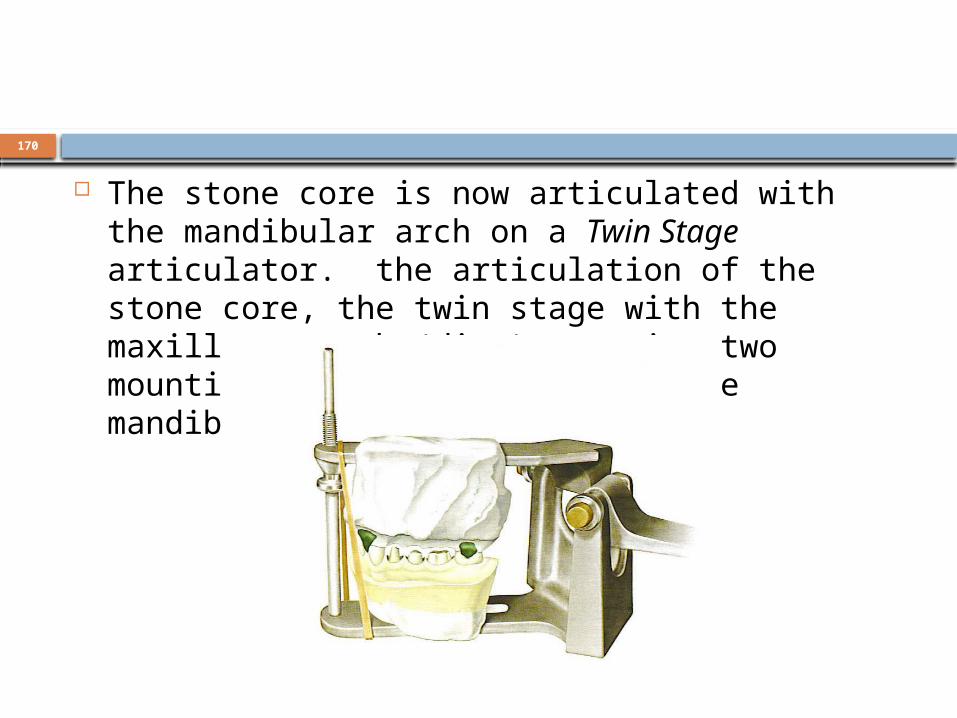
170
The stone core is now articulated with the mandibular arch on a Twin Stage articulator. the articulation of the stone core, the twin stage with the maxillary teeth (dies) opposing two mountings, the stone core and the mandibular model.

171
The twin stage articulator

172
The final wax-up for castings can now be completed against the opposing arch for proper shape and form and against the functionally generated path for proper occlusion.
If immediate posterior disclusion is wanted point contacts are created with the functionally generated path at the desired place.
For group function contact is created for all or part of the functionally generated path representing the movement in which contact is desired.
Final castings created using the functionally generated path and twin stage articulator)
The final castings are tried in, adjusted as necessary to create precise fit and occlusion, and cemented.
Occlusal adjustment is usually limited to adjustment with a rubber wheel or point, even in full group function contact cases.
173
Requirements for occlusal stability5 requirements 1.Stable centric stops on all the teeth 2. An anterior guidance that is in harmony with
the border movements of the envelope of function
3. Disclusion of all posterior teeth in protrusive movements
4. Disclusions of all posterior teeth on the non working side
5. Non interferences of all posterior teeth on the working side

174
DEEP OVERBITE
The first treatment option: Reshape

175
The second treatment option: Reposition

176

177
The third treatment option: Restore

178
ANTERIOR OVERJET

179

180

181
182
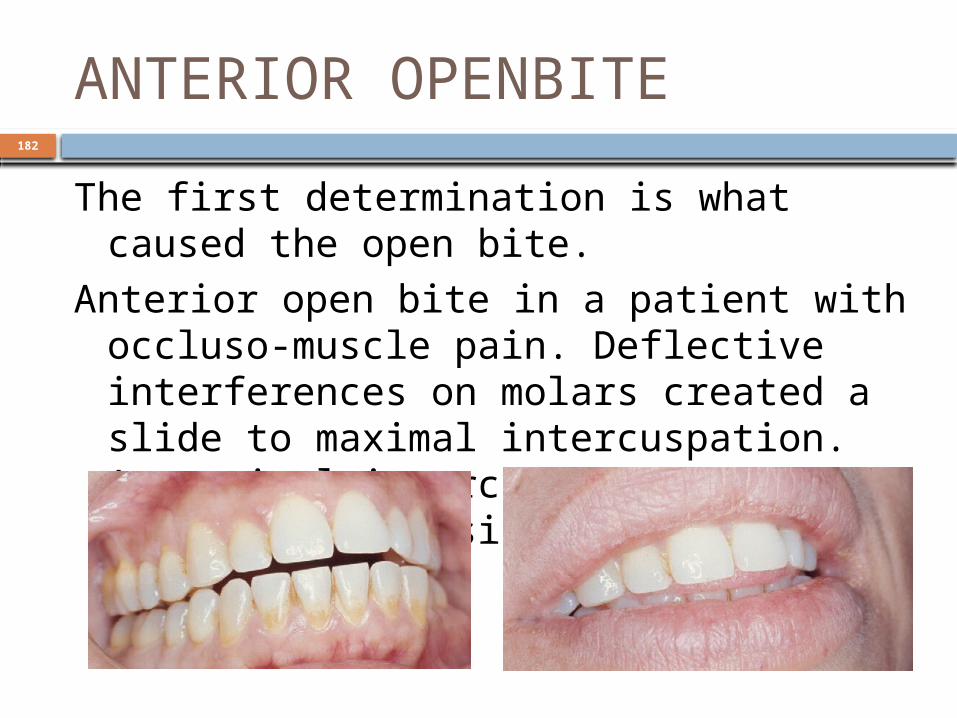
ANTERIOR OPENBITEThe first determination is what caused the
open bite.Anterior open bite in a patient with
occluso-muscle pain. Deflective interferences on molars created a slide to maximal intercuspation. At maximal intercuspation, no contact was possible for the anterior teeth.

183
Maximal intercuspation after occlusal correction by equilibration. Anterior teeth still could not contact opposing teeth

184
Position of teeth after 10 months. No orthodontic treatment or any other attempt was made to close the anterior open bite. The teeth erupted to contact because the tongue no longer maintained a posture to cushion the bite for protection of the deflective premature contact.
SURGICAL OPTION

185
END TO END OCCLUSION An end-to-end occlusion is very often treated as a
malocclusion simply because it does not conform to the requirements of a Class I relationship.
That is not an acceptable reason for altering any occlusion. Instead, the decision to alter the occlusal relationship should be based on a careful evaluation of the following factors.
STABILITY FUNCTION ESTHETICS NEUTRAL ZONE
186
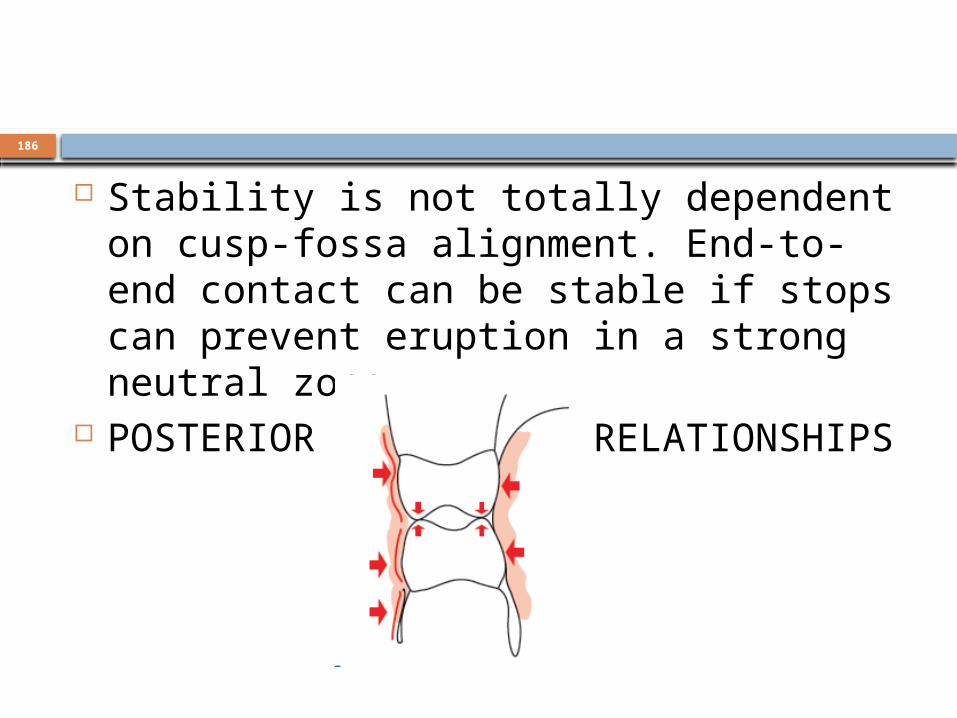
Stability is not totally dependent on cusp-fossa alignment. End-to-end contact can be stable if stops can prevent eruption in a strong neutral zone.
POSTERIOR END-TO-END RELATIONSHIPS

187
A lower-cusp-tip–to–upper-flat-surface relationship. This type of end-to-end relationship can provide good stability as long as lateral function contact is not needed.

188
The centralized lower cusps can contact in working excursion to disclude the balancing side. Contours can be made to look quite natural.

189
SPLAYED TEETH Splayed teeth are almost always
positioned within a strong neutral zone corridor.
190
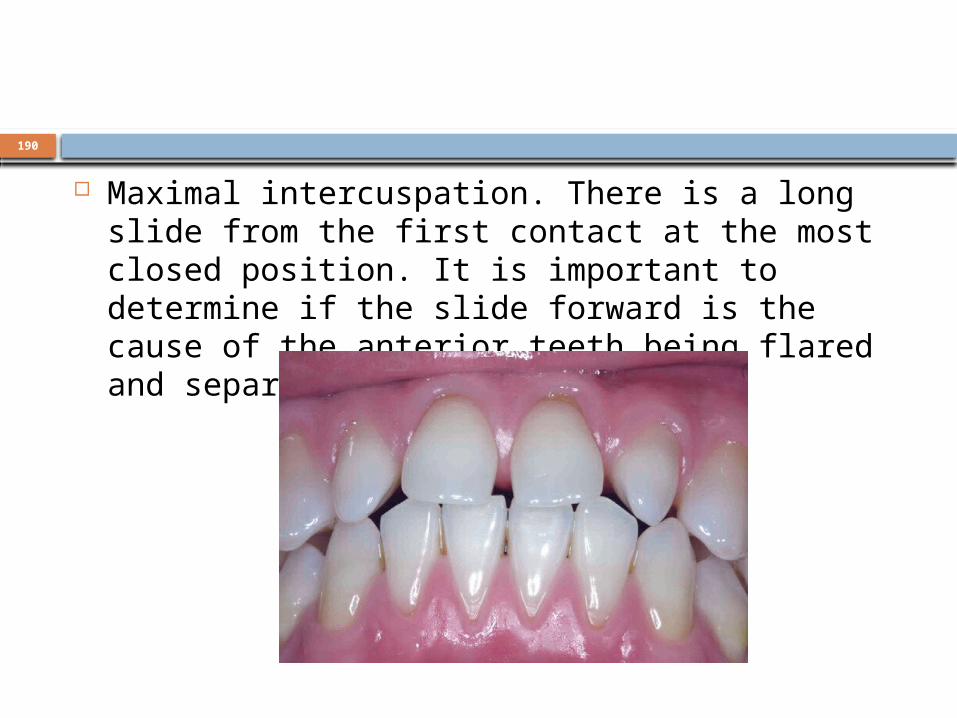
Maximal intercuspation. There is a long slide from the first contact at the most closed position. It is important to determine if the slide forward is the cause of the anterior teeth being flared and separated.
191
If the anterior teeth can contact after a deflective slide to maximal intercuspation, it is okay to achieve contact in centric relation.
If anterior contact cannot be achieved at the most closed position, it indicates that there is a tongue- or lip-biting habit that is responsible for the separation.
Before deciding on anterior contact in centric relation, it is necessary to eliminate a habit pattern that is a primary cause of the splaying and open bite.

192
Equilibration of casts.

193
Anterior guidance
Now it is apparent that an acceptable anterior guidance can be maintained on the central incisors and canines,
So laminate restorations will be the ideal restorations. It will be necessary to restore the lateral incisors with full coverage to achieve contact in centric relation.
194
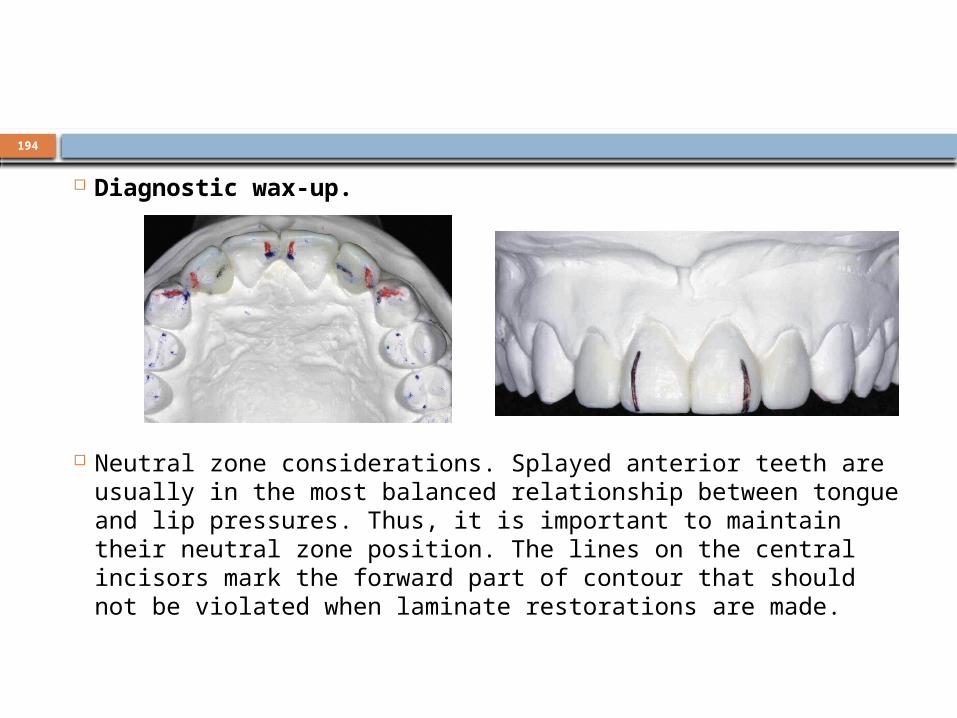
Diagnostic wax-up.
Neutral zone considerations. Splayed anterior teeth are usually in the most balanced relationship between tongue and lip pressures. Thus, it is important to maintain their neutral zone position. The lines on the central incisors mark the forward part of contour that should not be violated when laminate restorations are made.
195
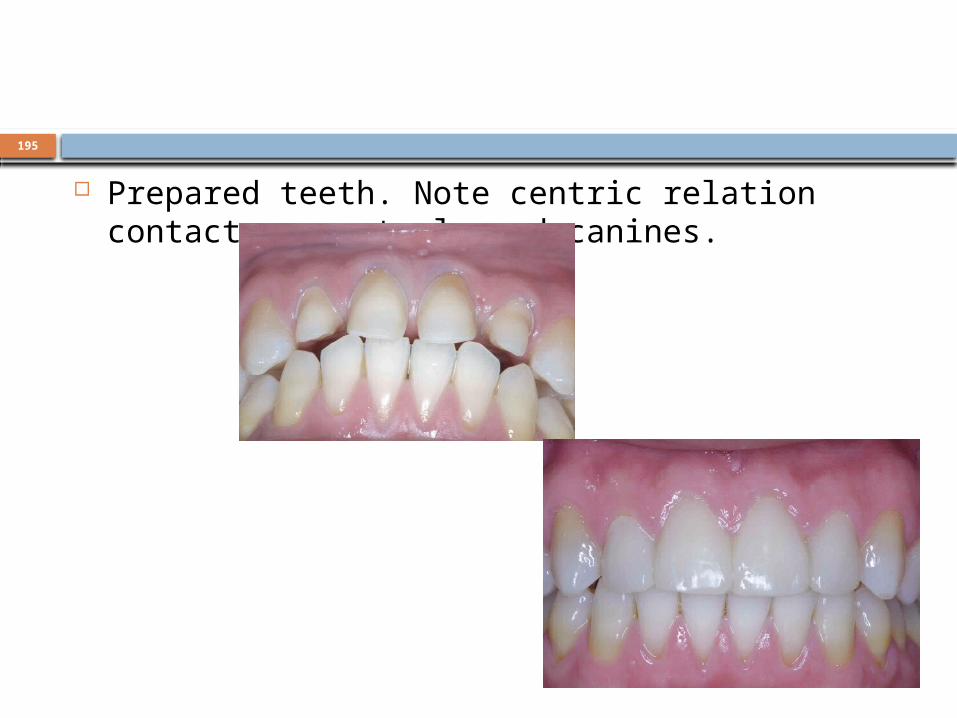
Prepared teeth. Note centric relation contact on centrals and canines.

196
POST-OPERATIVE CARE Dr. Keith begins his instructions to the patient with three
“no’s”: 1. No smoking. He points out the restrictive effect of smoking
on the capillary blood supply to the periodontal tissues and explains why it is so difficult to achieve long-term health of the necessary supporting structures unless the patient agrees to stop. He also clarifies smoking’s other risks to general health.
2. No hard candy. A habit of sucking on hard candies can be devastating to the teeth, especially at the cementoenamel junction where decay can cause so many problems.
3. No more than two soda drinks per week. The corrosive effect of high-acid carbonated drinks is too well documented to be ignored.
197
Patients should be told to report any of the following indications of occlusal disharmony:
1. Any discomfort in the teeth when chewing 2. Any indication of a “high” tooth or any sign
that one or more teeth contact before the rest when closing; any tooth that can be made to hurt by biting on it
3. Any sign of tooth hypermobility 4. Any discomfort in the TMJ area 5. Any limitation of function

198
Night time occlusal appliance use is indicated whenever the envelope of function must be restricted to achieve an improved esthetic result. This is often necessary when a longterm bruxing habit has flattened the anterior guidance.
Patient is recalled after 1 month, 3 month, 6 month, 1 year and then annually.

199
200
References Dawson PE. Evaluation ,diagnosis, and treatment of occlusal problems. 1989 2nd ed.
Cv Mosby Company, toronto. Jeffrey P okeson . Management of temporomandibular disorders and occlusion 5th
edition Mosby company toronto. Mann AW, Pankey LD (1960) Oral rehabilitation: part I. Use of the P-M instrument in
treatment planning and in restoring lower posterior teeth. J Prosthet Dent 10:135–150
Pankey LD, Mann AW (1960) Oral rehabilitation: part II.Reconstruction of the upper teeth using a functionally generated path technique. J Prosthet Dent 10:151–162
Gary M. DeWood. Gnathology and Pankey-Mann-Schuyler : fulfilling the requirements of occlusion in oral rehabilitation The University of Toledo The University of Toledo Digital Repository 2004
Stuart CE (1973) The contributions of gnathology to prosthodontics. J Prosthet Dent 30:607–608
Stuart CE, Stallard H (1960) Principles involved in restoring occlusion of the natural teeth. J Prosthet Dent 10:304–313
Schuyler CH (1959) An evaluation of incisal guidance and its influence on restorative dentistry. J Prosthet Dent 9:374–378
Schuyler CH (1963) The function and importance of incisal guidance in oral rehabilitation. J Prosthet Dent 13:1011–1029

201