from trials evaluating drugs to trials evaluating treatment algorithms – focus on the shiva trial
TRANSCRIPT

From trials evaluating drugs to trialsevaluating treatment algorithms –
Focus on the SHIVA trial
Christophe Le Tourneau, MD, PhD
Institut Curie
Head of the Phase I Program
Department of Medical Oncology
INSERM U900
EACR – Munich – July 7, 2014

Introduction
Chemotherapy
Targeted agent
Chemotherapy
Targeted agent
Chemotherapy
Targeted agent
Chemotherapy
Targeted agent
Chemotherapy
Targeted agent
Chemotherapy
Targeted agent
Chemotherapy
Targeted agent
Chemotherapy
Targeted agent

Introduction
Targets
EGFR
HER-2
mTOR
c-Kit
SMO
VEGF(R)
HDAC
NF-κB
CTLA4
RAF
ALK
RET
Drugs
Erlotinib/GefitinibCetuximab/PanitumumabCetuximab
Trastuzumab/TDM-1Lapatinib/PertuzumabTrastuzumab
Temsirolimus/EverolimusEverolimus
Imatinib
Vismodegib
BevacizumabSunitinibSorafenib
Vorinostat
Bortezomib
Ipilumumab
Vemurafenib
Crizotinib
Vandetanib/Cabozantinib
Tumor types
NSCLCCRCHNSCC
BreastBreastGastric adenocarcinoma
KidneyEndocrine tumors
GIST
Basal cell carcinoma
Breast, kidney, CRC, NSCLCKidney, endocrine tumorsKidney, HCC
Cutaneous lymphoma
Myeloma
Melanoma
Melanoma
NSCLC
Medullary thyroid cancer
Biomarkers
EGFR mutationKRAS mutation
-
HER2 amplificationHER2 amplificationHER2 amplification
--
c-Kit overexpression
-
---
-
-
-
V600E BRAF mutation
ALK translocation
-

Introduction
Ciriello et al. Nature Genet 2013;45:1127-33

IntroductionLUNG ADENOCARCINOMA – HER2 V659E MUTATION – LAPATINIB
Serra et al. Cancer Discov 2013;3:1238-44

IntroductionMELANOMA – KIT MUTATION – IMATINIB
Hodi et al. JCO 2013;31:3182-90

Introduction
Molecularprofile
Molecularalteration
Targeted agentTargeted agentTargeted agentTargeted agent Targeted agent Targeted agent Targeted agent

Introduction
Tsimberidou et al. CCR 2012;18:6373-83
Patients receiving matched targeted therapy Patients receiving no matched targeted therapy

Introduction
Failure-free survival
Patients receiving matched targeted
Overall survival
Patients receiving matched
targeted therapy
therapy
Patients receiving no matched targeted therapy
Tsimberidou et al. CCR 2012;18:6373-83

Outline
• Stratified trials:
- Molecular stratification
- Histologic stratification
• Algorithm-testing trials:
- Non-randomized trials
- Randomized trials
Le Tourneau et al. Chin Clin Oncol 2014;3:13

Outline
• Stratified trials:
- Molecular stratification
- Histologic stratification
• Algorithm-testing trials:
- Non-randomized trials
- Randomized trials

Outline
• Stratified trials:
- Molecular stratification
- Histologic stratification
• Algorithm-testing trials:
- Non-randomized trials
- Randomized trials

• FOCUS4 trial
Molecular stratification
Kaplan et al. JCO 2013;31:4592-8

Stratified trials Algorithm-testing trials
Molecularly-stratified
Histology-stratified
Non-randomized
Randomized
Tumor types
MolecularAlterations
Treatments
Test
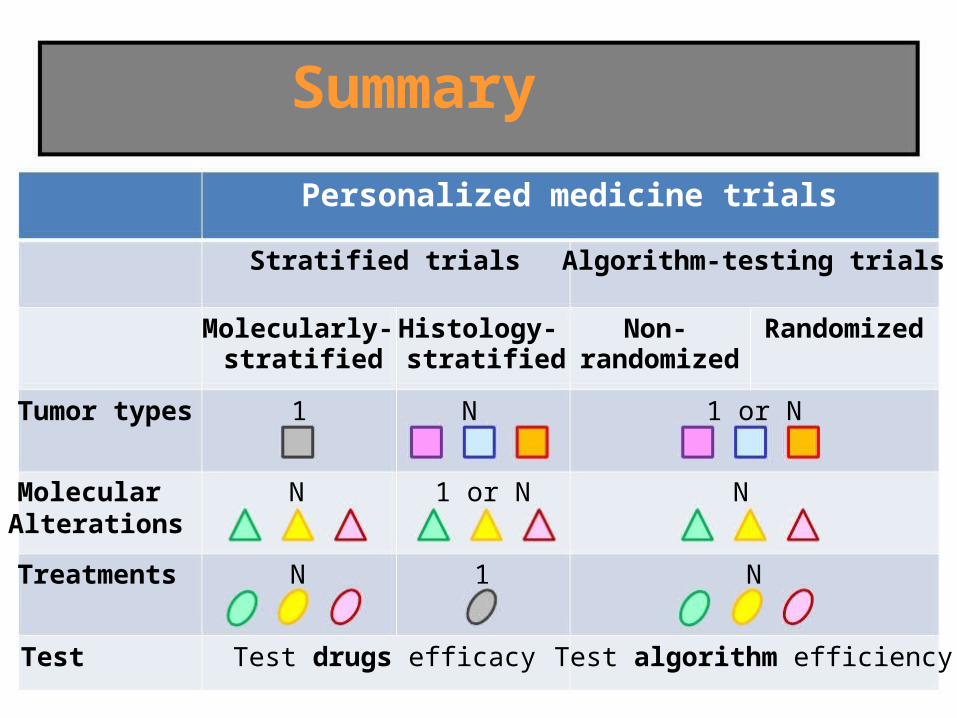
Summary
Personalized medicine trials

Stratified trials Algorithm-testing trials
Histology-stratified
Non-randomized
Randomized
Tumor types
Molecularly-stratified
1
MolecularAlterations
Treatments
Test
Summary
Personalized medicine trials

Stratified trials Algorithm-testing trials
Histology-stratified
Non-randomized
Randomized
Tumor types
Molecular
Molecularly-stratified
1
NAlterations
Treatments
Test
Summary
Personalized medicine trials

Stratified trials Algorithm-testing trials
Histology-stratified
Non-randomized
Randomized
Tumor types
MolecularAlterations
Molecularly-stratified
1
N
NTreatments
Test
Summary
Personalized medicine trials

Outline
• Stratified trials:
- Molecular stratification
- Histologic stratification
• Algorithm-testing trials:
- Non-randomized trials
- Randomized trials
Histologic stratification
• 1 drug
• Multiple tumor types harbouring specificmolecular alterations
• V-BASKET: vemurafenib (V600E BRAF mutation)
• CREATE: crizotinib (ALK/MET alterations)

Stratified trials Algorithm-testing trials
Non-randomized
Randomized
Tumor types
MolecularAlterations
Molecularly-stratified
1
N
Histology-stratified
N
1 or N
N 1Treatments
Test
Summary
Personalized medicine trials

Stratified trials Algorithm-testing trials
Non-randomized
Randomized
Tumor types
MolecularAlterations
Molecularly-stratified
1
N
Histology-stratified
N
1 or N
Treatments N 1
Test Test drugs efficacy
Summary
Personalized medicine trials
Outline
• Stratified trials:
- Molecular stratification
- Histologic stratification
• Algorithm-testing trials:
- Non-randomized trials
- Randomized trials

Outline
• Stratified trials:
- Molecular stratification
- Histologic stratification
• Algorithm-testing trials:
- Non-randomized trials
- Randomized trials

• Pilot study by Von Hoff et al.
Non-randomized trials
von Hoff et al. JCO 2010;28:4877-83

Non-randomized trials
von Hoff et al. JCO 2010;28:4877-83
• 18/66 patients (27%): ratio>1.3

Outline
• Stratified trials:
- Molecular stratification
- Histologic stratification
• Algorithm-testing trials:
- Non-randomized trials
- Randomized trials

• Question:
SHIVA
>?

SHIVA
• Promotion: Institut Curie (Paris & Saint-Cloud)
• Other participating centers:
- Centre Léon Bérard (Lyon)
- Centre René Gauducheau (Nantes)
- Institut Claudius Régaud (Toulouse)
- Institut Paoli-Calmettes (Marseille)
- Centre Georges-François Leclerc (Dijon)
- Centre Alexis Vautrin (Nancy)

SHIVA
• Primary objective:- To compare the efficacy of targeted therapy based on
tumor molecular profiling versus conventional therapy inpatients with refractory cancer
• Primary end point:- Progression-free survival
Le Tourneau et al. Target Oncol 2012;7:253-65

SHIVA
• Secondary objectives:- To evaluate overall response rate
- To compare overall survival
- To evaluate tumor growth kinetics*
- To evaluate safety
- To evaluate the ability of circulating tumor DNA to earlypredict treatment efficacy/resistance
- To evaluate the medico-economic impact of theexperimental strategy
*Le Tourneau et al. BJC 2012;106:854-7

SHIVA
• Inclusion criteria:- >18 years old
- patients with any type of cancer that is refractory tostandard of care
- biopsiable & measurable disease
- ECOG PS 0 or 1
- adequate blood counts and organ functions

Informedconsentsigned
Tumor biopsy
Molecularprofile
Patients with refractorycancer (all tumor types)

Molecular profile
• Mutations:
- Ampliseq Cancer Panel
- Ion Torrent / PGM (Life Technologies®)
• Gene copy number alterations:
- Cytoscan HD (Affymetrix®)
• Protein expression:
- IHC (ER, PR, AR)

Molecular profile
• Variants of interest:
- validated hotspots mutations* frequency: >4% for SNVs and >5% for indels
* coverage: >30X for SNVs and >100X for indels
- non targeted variants* outside an hotspot
* frequency >10%
* no synonymous mutations
* no polymorphisms

Molecular profile
• Amplifications:
- Gene copy number* diploid tumor: >6
* tetraploid tumor: >7
- Amplicon size* <1 Mb
* <10 Mb if protein expression is validated in IHC
Servant et al. Frontiers in Genetics 2014;5:e152

Informedconsentsigned
Tumor biopsy
NGS+Cytoscan HD
+IHC
Bioinformatics
Patients with refractorycancer (all tumor types)

Informedconsentsigned
Molecularbiologyboard
Patients with refractorycancer (all tumor types)
Tumor biopsy
NGS+Cytoscan HD
+IHC
Bioinformatics
PathologistsBiologists
Plateforms managers
BioinformaticiansPhysicians

Molecular profile
Le Tourneau et al. BJC [Epub ahead of print April 24, 2014]

Informedconsentsigned
Tumor biopsy
NGS+Cytoscan HD
+IHC
Bioinformatics
Molecularbiologyboard
Specifictherapyavailable
Non eligiblepatient
NO
Eligiblepatient
YES
Patients with refractorycancer (all tumor types)

RConventional therapy atphysicians' discretion
Bioinformatics
Informedconsentsigned
Tumor biopsy
NGS+Cytoscan HD
+IHC
therapyavailable
Molecularbiologyboard
YESNO
Non eligiblepatient
Eligiblepatient
Informedconsentsigned
Patients with refractorycancer (all tumor types)
ImatinibEverolimusSorafenibErlotinibDasatinibLapatinib
TrastuzumabVemurafenibTamoxifenLetrozoleAbiraterone
Targeted therapy based on molecularprofiling
Cross-over
Specific

Treatment algorithm
Targets
KIT, ABL1/2, RET
PI3KCA, AKT1AKT2/3, mTOR, RICTOR, RAPTORPTEN
STK11
INPP4B
BRAF
PDGFRA/B, FLT3
EGFR
HER-2
SRCEPHA2, LCK, YES1
ER, PR
AR
Molecular alterations
Mutation/Amplification
Mutation/AmplificationAmplificationHomozygous deletionHeterozygous deletion + mutation or IHCHomozygous deletionHeterozygous deletion + mutationHomozygous deletion
Mutation/Amplification
Mutation/Amplification
Mutation/Amplification
Mutation/Amplification
Mutation/AmplificationAmplification
Protein expression >10% IHC
Protein expression >10% IHC
Targeted therapies
Imatinib
Everolimus
Vemurafenib
Sorafenib
Erlotinib
Lapatinib + Trastuzumab
Dasatinib
Tamoxifen or Letrozole
Abiraterone
Le Tourneau et al. BJC [Epub ahead of print April 24, 2014]

Treatment algorithm
• Multiple molecular alterations:- DNA alterations are considered of a higher impact than
hormone receptors expression
- If AR and ER/PR are both overexpressed, the hormonereceptor with the highest expression level is taken intoaccount
- If >2 DNA alterations are identified, clinically validatedalterations prevail (i.e. HER-2 amplification)
- Erlotinib is not given in case of KRAS mutation

SHIVA
• Randomization:
- 1:1
- stratification on the Royal MarsdenPrognostic score for oncology phase Icancer patients
- stratification on the signalling pathway(PI3K/AKT/mTOR, Hormone receptors, MAPK pathway)
Arkenau et al. JCO 2009;27:2692-6

SHIVA
• Sample size:- 6 months PFS = 15% in phase I cancer patients treated
with cytotoxic agents
- Hypothesis: 6 months PFS = 30% in the experimentalarm (HR = 0.625)
142 events with a type 1 error of 5% and a power of80% in the bilateral setting
200 patients should be randomized
up to 1,000 patients might have to be included
Hortsmann et al. NEJM 2005;352:895-904

Accrual
Included
Planned
740

Randomization
Randomized
Planned
170
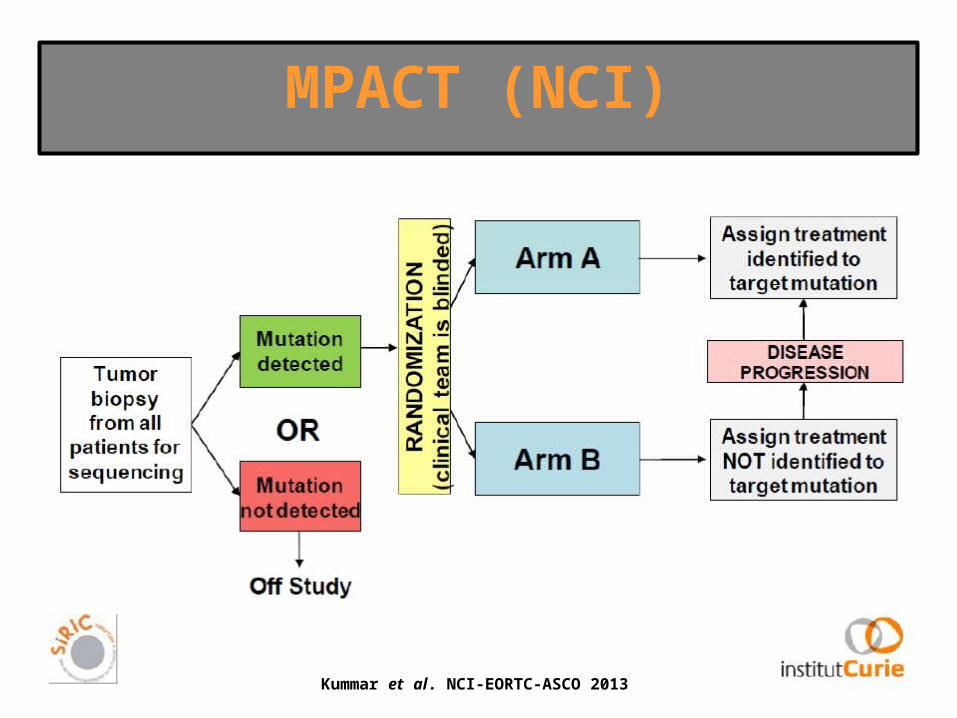
MPACT (NCI)
Kummar et al. NCI-EORTC-ASCO 2013

Stratified trials Algorithm-testing trials
Molecularly-stratified
Histology-stratified
Non-randomized
Randomized
1 or NTumor types
MolecularAlterations
1
N
N
1 or N
Treatments N 1
Test Test drugs efficacy
Summary
Personalized medicine trials

Stratified trials Algorithm-testing trials
Molecularly-stratified
Histology-stratified
Non-randomized
Randomized
Tumor types
MolecularAlterations
1
N
N
1 or N
1 or N
N
Treatments N 1
Test Test drugs efficacy
Summary
Personalized medicine trials

Stratified trials Algorithm-testing trials
Molecularly-stratified
Histology-stratified
Non-randomized
Randomized
Tumor types
MolecularAlterations
1
N
N
1 or N
1 or N
N
Treatments N 1 N
Test Test drugs efficacy
Summary
Personalized medicine trials
Stratified trials Algorithm-testing trials
Molecularly-stratified
Histology-stratified
Non-randomized
Randomized
Tumor types
MolecularAlterations
1
N
N
1 or N
1 or N
N
Treatments N 1 N
Test Test drugs efficacy Test algorithm efficiency
Summary
Personalized medicine trials

Conclusions
• High-throughput technologies haveentered the clinic
• Emergence of personalized medicineclinical trials
• Multiples challenges
• It remains to be demonstrated that the useof high throughput technologies improvespatients outcome

Acknowledgments• Direction
Thierry Philip
Claude Huriet
Pierre Teillac
Daniel Louvard
• ICGEXOlivier Delattre
Thomas Rio Frio
Quentin Leroy
Virginie Bernard
• UGECPatricia Tresca
Sebastien Armanet
Fabrice Mulot
• BiostatisticsXavier Paoletti
Corine Plancher
Cécile Mauborgne
• PathologyAnne Salomon
Odette Mariani
Frédérique Hammel
Xavier Sastre
Didier Meseure
• Translational researchMaud Kamal
David Gentien
Sergio Roman-Roman
• RadiologyVincent Servois
Daniel Szwarc
• BioinformaticsPhilippe Huppé
Nicolas Servant
Julien Romejon
Emmanuel Barillot
Philippe La Rosa
Alexandre Hamburger
Pierre Gestraud
Fanny Coffin
Séverine Lair
Bruno Zeitouni
Alban Lermine
Camille Barette
• ComunicationCéline Giustranti
Catherine Goupillon-Senghor
Cécile Charre
• GeneticsIvan Bièche
Gaëlle Pierron
Etienne Rouleau
Céline Callens
Marc-Henri Stern
• SurgeryThomas Jouffroy
José Rodriguez
Angélique Girod
Pascale Mariani
Virginie Fourchotte
Fabien Reyal
• FoundationHélène Bongrain- Meng
Ifrah El-Alia
Véronique Masson
Agnès Hubert
• Clinical researchMalika Medjbahri
• SamplingSolène Padiglione
• PharmacyLaurence Escalup
• OncologyAlain Livartowski
Suzy Scholl
Laurent Mignot
Philippe Beuzeboc
Paul Cottu
Jean-Yves Pierga
Véronique Diéras
Valérie Laurence
Sophie Piperno-Neumann
Catherine Daniel
Wulfran Cacheux
Bruno Buecher
Emmanuel Mitry
Astrid Lièvre
Coraline Dubot
Etienne Brain
Barbara Dieumegard
Frédérique Cvitkovic