frequency and nature of medication errors and adverse drug ... file · web viewlittle is known...
TRANSCRIPT
Frequency and nature of medication errors and adverse drug events in mental health hospitals: a systematic
review
Short version of title: Medication errors and adverse drug events in mental health hospitals
Ghadah H Alshehri MPharm1
Richard N Keers PhD1,2,3
Darren M Ashcroft PhD1,2
1Centre for Pharmacoepidemiology and Drug Safety, Division of Pharmacy and Optometry, School of Health
Sciences, University of Manchester, Manchester Academic Health Sciences Centre (MAHSC), Manchester,
United Kingdom, M13 9PT
2NIHR Greater Manchester Patient Safety Translational Research Centre, Manchester Academic Health
Sciences Centre (MAHSC), University of Manchester, Manchester, United Kingdom M13 9PT.
3Pharmacy Department, Greater Manchester Mental Health NHS Foundation Trust, Manchester, United
Kingdom M8 5RB
Tel: (+44)161 275 2415, Email: [email protected]
Acknowledgements: Ghadah H Alshehri gratefully acknowledges the Princess Nora Bint Abdul Rahman
University for funding her PhD programme at the University of Manchester.
Conflict of interest: All authors declare that they have no conflict of interest.
This article does not contain any studies with human participants or animals performed by any of the authors.
1

Tables and figures
Figure 1: Flow diagram of the systematic process applied in medication error studies.
Table 1: Characteristics of studies examining medication errors and adverse drug events in mental health
hospitals
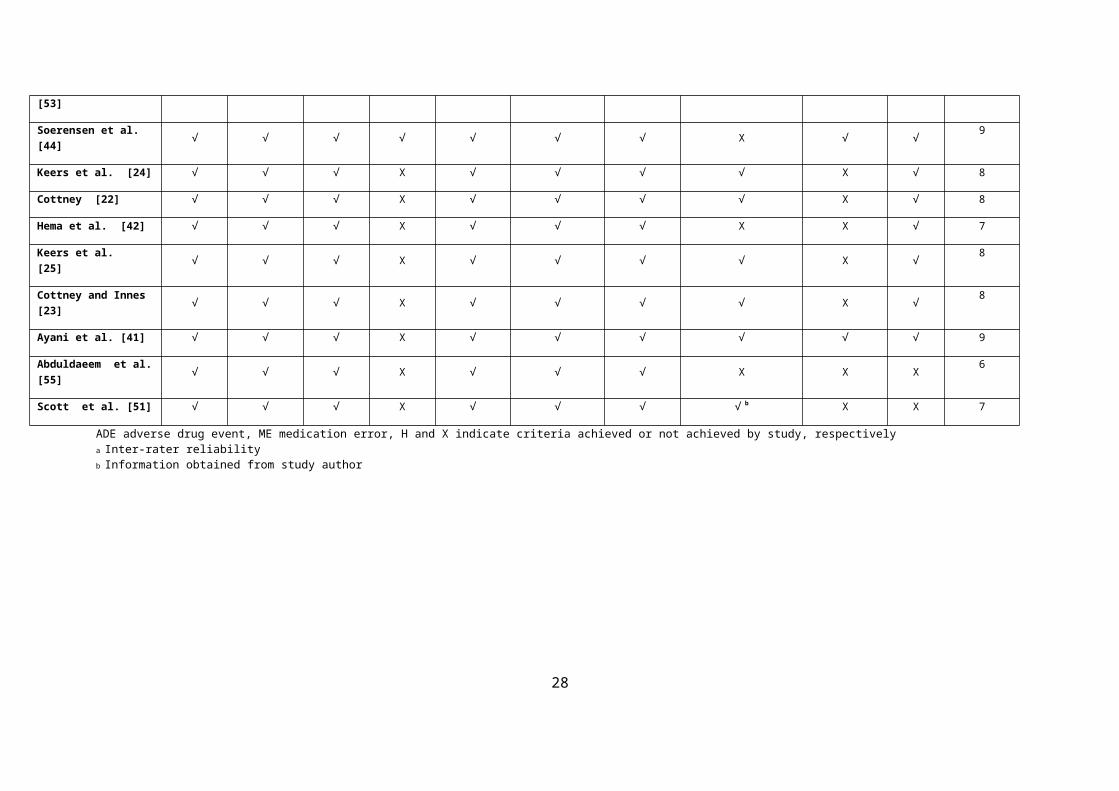
Table 2: Quality assessment criteria applied to the included studies
2

Abstract Background
Little is known about the frequency and nature of medication errors (MEs) and adverse drug events (ADEs) that
occur in mental health hospitals.
Objective:
This systematic review aims to provide an up-to-date and critical appraisal of the epidemiology and nature of
MEs and ADEs in this setting.
Method
Ten electronic databases were searched including: MEDLINE, EMBASE, CINAHL, International
Pharmaceutical Abstracts, PsycINFO, Scopus, British Nursing Index, ASSIA, Web of Science, and Cochrane
Database of Systematic Reviews (1999 to October 2016). Studies that examined the rate of MEs or ADEs in
mental health hospitals were included and quality appraisal of the included studies was conducted.
Result
In total, 20 studies were identified. The rate of MEs ranged from 10.6 to 17.5 per 1000 patient-days (n= 2) and
ADEs from 10.0-42.0 per 1000 patient-days (n=2) with 13.0 -17.3% of ADEs found to be preventable. ADEs
were rated as clinically significant (66.0-71.0%), serious (28.0-31.0%), or life threatening (1.4-2.0%).
Prescribing errors occurred in 4.5-6.3% of newly written or omitted prescription items (n=3); dispensing errors
occurred in 4.6% of opportunities for error (n=1) and in 8.8% of patients (n=1); medication administration errors
in 3.3-48.0% of opportunities for error (n=5). MEs and ADEs frequently associated with psychotropic, with
atypical antipsychotic drugs commonly involved. Variability in study setting and data collection methods
limited direct comparisons between studies.
Conclusion
Medication errors occur frequently in mental health hospitals and are associated with risk of patient harm.
Effective interventions are needed to target these events and improve patient safety.
Key points:
Medication errors (MEs) and adverse drug events (ADEs) are common in mental health hospitals Psychotropic medication was often involved in MEs and accounted for the majority of harm associated with
medication use. Further research is needed to examine the rate of ADEs, dispensing errors and unintentional medication
discrepancies at interface between primary and secondary care mental health settings. Future research is needed to examine the organisational and system context and its influence on medication
safety in mental health settings so that effective interventions can be implemented.
3
1. Introduction
The prevention of medication errors (MEs) and adverse drug events (ADEs) in hospitals is recognised
internationally as an important health care priority [1]. A systematic review of eight studies from the US, UK,
New Zealand, Australia, and Canada found that the median incidence rate of in-hospital adverse events was
9.2% of patients, with ADEs found to be common, accounting for 15.1% of adverse events [2]. Other systematic
reviews have examined the frequency of prescribing errors (PEs), medication administration errors (MAEs) and
dispensing errors (DEs) in hospitals worldwide, with reported median rates of error being 7% (inter-quartile
range (IQR) 2.0–14.0%) of medication orders, 19.0% (IQR 8.6-28.3%) of total opportunities for error, and a
range of 0.1- 2.7% for items dispensed, respectively [3-5]. Whilst these reviews have contributed to our
understanding of the extent and nature of medication-related problems in general hospitals, these estimates
cannot be assumed to represent more specialist settings, such as mental health hospitals, where different patient
population characteristics and ways of working may create distinct medication safety challenges than those seen
in general hospital settings [6-8].
Patients with serious mental illness have a set of vulnerabilities and risks associated with nature of mental
illnesses and pharmacological treatment [6, 7, 9]. For instance, the cognitive impairment associated with mental
illness may be associated with non-adherence with medical treatment and poor reporting of medication related
problems [8, 10, 11]. In addition, mental health care practice also differs with regard to the unique medicines
related legislation, such as the UK Mental Health Act 1983 (amended 2007), that requires strict documentation
of prescribing practice and allows administration of treatment for mental disorders against the patient’s will
[12]. The type of medications used and the way in which these medicines are managed in mental health may
also create unique safety challenges compared to general hospitals. For example, psychotropic medication such
as antipsychotics, antidepressants and benzodiazepines are used frequently in the hospitalised mental health
population, many of which contribute to physical health problems such as impaired glucose tolerance,
dyslipidaemia, sexual dysfunction and extrapyramidal side effects [6, 9, 13, 14]. Polypharmacy [15], high dose
antipsychotic prescribing [16, 17] and drug-drug/disease interactions are also prevalent in the mental health
population [18], which can increase the risk of medication- related problems.
Taking all these issues into account, the need to explore the burden of medicines safety issues in mental health
hospital is therefore warranted. Earlier literature reviews have focussed on MEs and/or ADEs exclusively in
mental health hospitals [8, 19-21] but only three of these were systematic in nature [19-21]. Whilst informative,
these reviews are now outdated as more recent publications relating to ME and ADE in mental health hospitals
have emerged[22-25]. They were also restricted to English language publications [20, 21] or were specific to
elderly patients [21], which limits understanding across wider mental health settings and populations. Some of
these earlier reviews also included studies that reported error rates based on incident report data [26, 27], which
are known to underestimate error rates substantially [28], or focussed exclusively on MEs without consideration
of ADEs [20, 21]. Therefore, the aim of this systematic review was to provide an up-to-date and critical
assessment of the frequency and nature of ME and ADE in mental health hospitals.
4
2. Method
2.1. Definitions
ADEs were defined as: “any injury resulting from medical intervention related to a drug” [29, 30] and those
associated with medication errors classified as preventable adverse drug events (pADEs). Medication errors
were defined according to the National Coordinating Council for Medication Error Reporting and Prevention
(NCCMERP) as: “any preventable event that may cause or lead to inappropriate medication use or patient harm
while the medication is in the control of the health care professional, patient, or consumer. Such events may be
related to professional practice, health care products, procedures, and systems, including prescribing, order
communication, product labelling, packaging, and nomenclature, compounding, dispensing, distribution,
administration, education, monitoring, and use”[31]. Unintentional medication discrepancies were also
examined and defined as “unexplained differences in documented medication regimens at the point of transition
of care”[32].
2.2. Search strategy
We searched ten electronic databases from January 1999 to October 2016: MEDLINE, EMBASE, Cumulative
Index to Nursing and Allied Health Literature (CINHAL), International Pharmaceutical Abstracts (IPA),
PsycINFO, Scopus, British Nursing Index (BNI), Applied Social Science Index and Abstract (ASSIA), Web of
Science, and Cochrane Database of Systematic Reviews. The start date of the search was selected to coincide
with the publication of the landmark report To Err Is Human: Building a Safer Health System [33], which is
generally considered to have instigated extensive patient safety research [34], and to also ensure that the
included studies related to current medication safety practices in mental health hospitals. For each database, the
search keywords used were divided into three groups: error-related terms (including error(s), medication
error(s), medical error, drug error, treatment error, therapeutic error, medication safety, drug safety, drug-related
problem, adverse drug event, preventable adverse drug event, potential adverse drug event, near miss,
medication incident, clinical incident, drug incident, incident report, prescribing error, prescription error,
administration error, dispensing error, transcription error, omission, discrepancy); epidemiology-related terms
(including rate, prevalence, incidence); and setting-related terms (including psychiatry, psychiatric hospital,
mental health hospital, adult psychiatry, child psychiatry, adolescent psychiatry, geriatric psychiatry, and
forensic psychiatry). The reference lists of all included articles and relevant reviews were also examined to
identify any additional studies that could be eligible for inclusion. Any additional studies identified by the
project team were also included as long as they fulfilled the study’s inclusion criteria. Study authors were
contacted when additional information was required.
5
2.3. Inclusion and exclusion criteria
Inclusion criteria: studies published between 1999 to October 2016 that reported the rate of ME/ADE in one or
more stage(s) of the treatment process (prescribing, administration, transcription, dispensing and monitoring) for
patients in mental health hospitals (in-patient and outpatient services). Studies that examined the rate of
unintentional medication discrepancies at the point of transition of care between mental health hospitals and
other settings (such as primary care) were also included. However, studies that failed to differentiate between
intentional and unintentional discrepancies using a robust method (e.g. by contacting the medical team) were not
included. In addition, studies that examined the impact of interventions on ME or ADE rates were only included
if a baseline error rate could be determined. Conference abstracts were also included if they provided sufficient
data that allowed for the rate of ME or ADE to be calculated.
Exclusion criteria: studies that utilised incident reports as the primary source of collecting data were excluded
(as they greatly underestimate the error rate)[28], as were those that used an estimated denominator to calculate
the rate of ME or ADE (as the provided rate may not be reflective of the actual rate) [3]. Studies that reported
ME or ADE rates for a single drug, single drug class or disease were excluded, as were studies that only
examined specific prescribing, administration, transcription or dispensing error subtypes such as wrong dose.
Studies that reported the rate of potentially inappropriate prescribing (PIP) in mental health hospitals were
excluded, as they were not considered to be medication errors [35]. Whilst review articles were excluded, we
screened the reference lists of any identified reviews to identify other relevant studies.
2.4. Data extraction
A standardized data collection form was developed and used to collect information concerning: publication
year; country of origin; study setting; definitions used; study design (retrospective or prospective); and error
detection method. In addition, information related to the main findings of the study, including the rate of ME or
ADE (including the rate of pADEs), type of denominator used, type of errors, class of medication involved, and
severity of reported errors, was also retrieved. For each study, data was extracted by two of the authors
independently, with any disagreements in extraction being resolved by discussion between all authors.
2.5. Quality assessment
The quality of the included studies was assessed on the basis of criteria originally developed by Allan and
Barker [36], which has been used in other systematic reviews of medication safety [37-39], including one in
mental health settings[21]. The criteria require a clear description of the following: aim/objectives of the study;
outcome definition; error categories specified; error categories defined (applicable for general ME studies only);
denominator; data collection method; study setting; validity and reliability measures used; and consideration of
study limitations.
6

2.6. Data analysis
The included studies were heterogeneous in nature, which prevented any meta-analysis of data. Although a
comparable denominator (opportunities for error) was observed among studies reporting medication
administration error rates, differences in study setting and types of administration error being studied meant that
pooled analysis was not appropriate; therefore, the findings were summarised narratively. The percentage rate of
ME was determined by dividing the number of actual errors that occurred or number of patients/prescriptions
affected by MEs by the total number of prescriptions/patients/OE multiplied by 100. The rate of ADE/pADE per
1000 patient days was calculated by dividing number of ADEs/pADEs by the total number of patient days
multiplied by 1000.
3. Literature search results
In all, 20 unique studies were included in this systematic review, as shown in Fig. 1. Six studies examined
overall ME rates[40-45], including two that measured ADEs [40, 41] and some studies also reporting additional
data on PEs [40, 42-45], MAEs[40, 42, 44, 45], transcription errors (TEs) [40, 43, 45] and DEs[42-44]. In total,
14 studies reported data on the rate of PE [24, 25, 40, 42-52] , one on unintentional discrepancies [53], and eight
on MAEs [22, 23, 40, 42, 44, 45, 54, 55]. A summary of the characteristics of the included studies is presented
in Table 1.
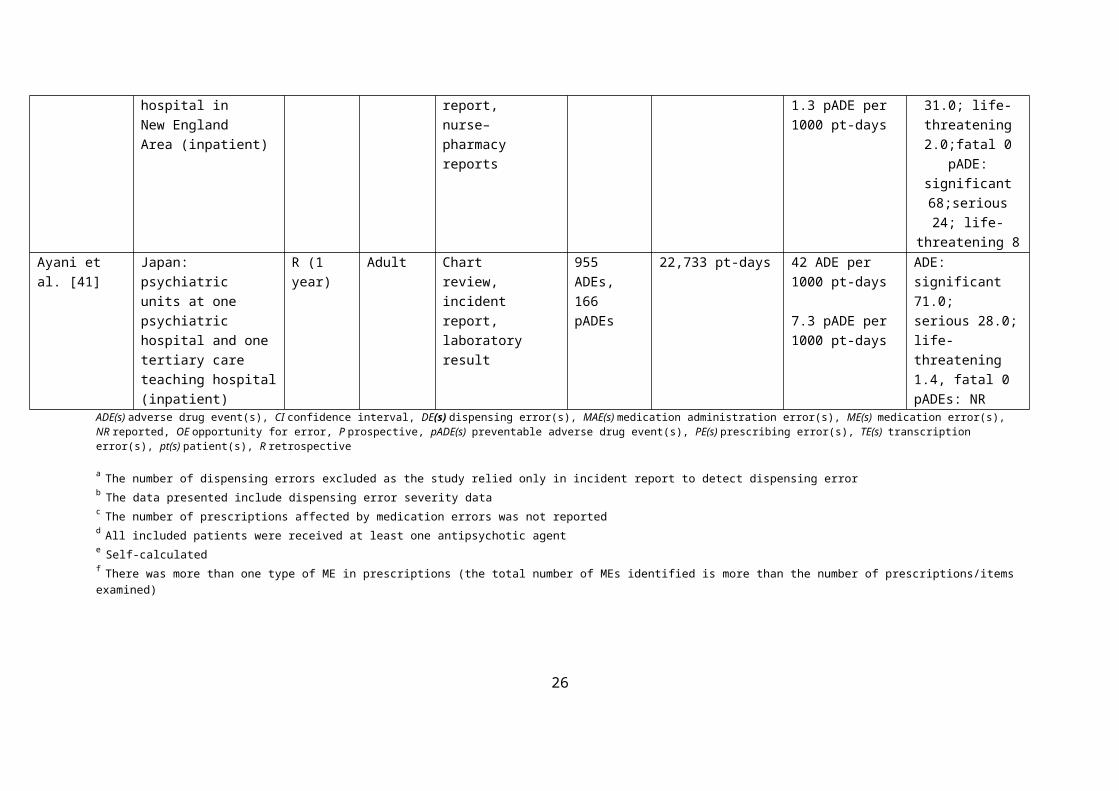
3.1. Quality assessment
The aim and objectives for each study were clearly stated and definitions provided for MEs/ADEs in all (n=16,
80%) but four studies [43, 46, 52, 53] ME categories were specified in all ME studies, and defined in one study
[44]. The denominators were explicitly described in all studies. The data collection method and study setting
were also described clearly in all studies. A process of validation to confirm the error had occurred was applied
in eleven (55%) studies [22-25, 40, 41, 43, 45, 48, 51, 53], all of which used different approaches to error
validation. Reliability measures were applied only in three studies (15%) [40, 41, 44]. In terms of study
limitations, all except five studies did not state key limitation(s) [43, 48, 50, 51, 55]. Three of which were
conference abstracts [43, 51, 55]. Conference abstract made quality assessment of study reporting a challenging
task, as the nature of abstracts precludes sufficient information for such an assessment. A summary of the
quality assessment criteria is shown in Table 2.
7

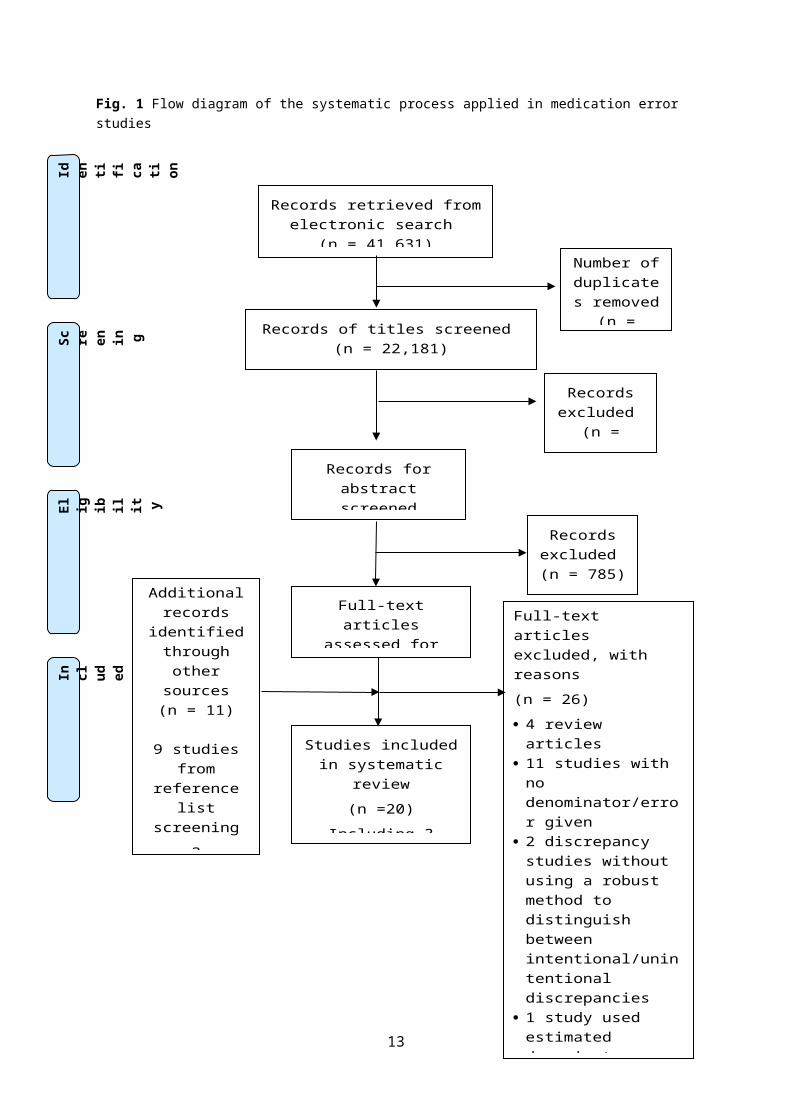
Fig. 1 Flow diagram of the systematic process applied in medication error studies
8
Records retrieved from electronic search
(n = 41,631)
Sc ree
nin g
Inc
lud ed
Eli
gib
ilit y
Ide
nti
fic ati
on
Records of titles screened (n = 22,181)
Records for abstract screened(n = 820)
(n = )
Records excluded
(n = 21,361)
Full-text articles assessed for eligibility
(n =35)
Studies included in systematic review
(n =20)
Including 3 conference abstracts
Records excluded (n = 785)
Additional records
identified through other
sources (n = 11)
9 studies from reference list
screening
2 conference abstract
suggested by project team
Number of duplicates removed
(n = 19,450)
Full-text articles excluded, with reasons
(n = 26)
4 review articles 11 studies with no
denominator/error given 2 discrepancy studies
without using a robust method to distinguish between intentional/unintentional discrepancies
1 study used estimated denominator
3 studies that relied solely on incident report as method for collecting data
1 study on single mental health disease
2 Potential inappropriate prescribing studies
2 abstract that did not provide sufficient data for inclusion
3.2. Frequency of medication errors and adverse drug events
3.2.1. Overall Rates of Medication Errors and Adverse Drug Events
Six studies reported an overall ME rate covering all stages of the medication treatment process from prescribing
through to dispensing (Table 1). Of these, two studies examined both MEs and ADEs [40, 41], and some studies
also reported additional data on the rate of ME categories, including PEs [40, 42-45], MAEs [40, 42, 44, 45],
TEs [40, 43, 45] and DEs [42-44]. Three studies were prospective [40, 42, 43], two studies used both a
retrospective and a prospective design [44, 45] and one study used retrospective chart review [41].
Five studies used different error definitions, including the definition of ME developed by Bates et al. [40, 41],
Reason [44] and the NCCMERP [42, 45]. One study did not provide any error definition [43]. Additional
variability was apparent in the denominators used, the study setting (inpatient or outpatient), the patient
population (child or adult), and data collection methods, which limited our ability to compare the studies
directly. Four studies used different health professions to collect data such as nurses, pharmacists, physicians or
psychiatrists [40, 41, 43, 45]. The remaining two studies did not specify the professional role of the data
collector [42, 44].
Two studies with similar denominators reported an overall ME rate of 10.6–17.5 per 1000 patient-days [40, 41].
Other studies found that MEs occurred in 2.4% of complete prescriptions checked (in a paediatric outpatient
setting) [43], 17.4% of total OE [44] and in 61.4% of patients [42]. MEs commonly occurred during prescribing
[40, 41], transcription [43] and medication administration stages [42, 44, 45] and also occurred due to a lack of
treatment monitoring [41]. Psychotropic therapy was most often associated with error (41.0–68.0%), particularly
involving atypical antipsychotics (19.3–32.0%) [40, 43, 44]. In child outpatient settings, methylphenidate and
trihexyphenidyl were most frequently associated with error [43]. The assessment of potential severity was
carried out either by using the NCCMERP criteria [42] or based on methods used in other published studies [40,
44]. Data on ME severity found that 28.0–50.7% of errors were of significant severity, 42.3–44.8% were of
serious severity and 2.1–4.4% were potentially life threatening [40, 44].
In terms of ADEs, two studies undertaken in the USA and Japan reported rates of 10.0–42.0 per 1000 patient-
days, and 10.8–213.0 per 100 admissions, respectively [40, 41]. Preventable ADE rates accounted for 13.0–
17.3% of all ADEs giving a rate of 1.3–7.3 per 1000 patient-days and 1.3–37.1 per 100 admissions, respectively
[40, 41]. Chart review and incident report were the two methods used to detect ADEs [40, 41]. One study also
used pharmacy and nurse report to detect ADEs [40]. The study from Japan [41] found the incidence rate of
ADEs was higher in medical care units—where psychiatric patients with physical comorbidities are more likely
to be treated—than in acute and nursing units. Psychotropic medicines were commonly involved with ADEs
(79.8–92.0%), including the pADE subset (58.4–68%). Atypical antipsychotic medicines were the most
common psychotropic class associated with ADEs [40, 41]. The severity of ADEs was commonly rated as
significant (66.0–71.0%), serious (28.0–31.0%) or life-threatening (1.4–2.0%) [40, 41]. For pADEs, the
9

corresponding severity ratings were significant 68.0%, serious 24.0 and 8.0% life threatening in the US study
[40].
10
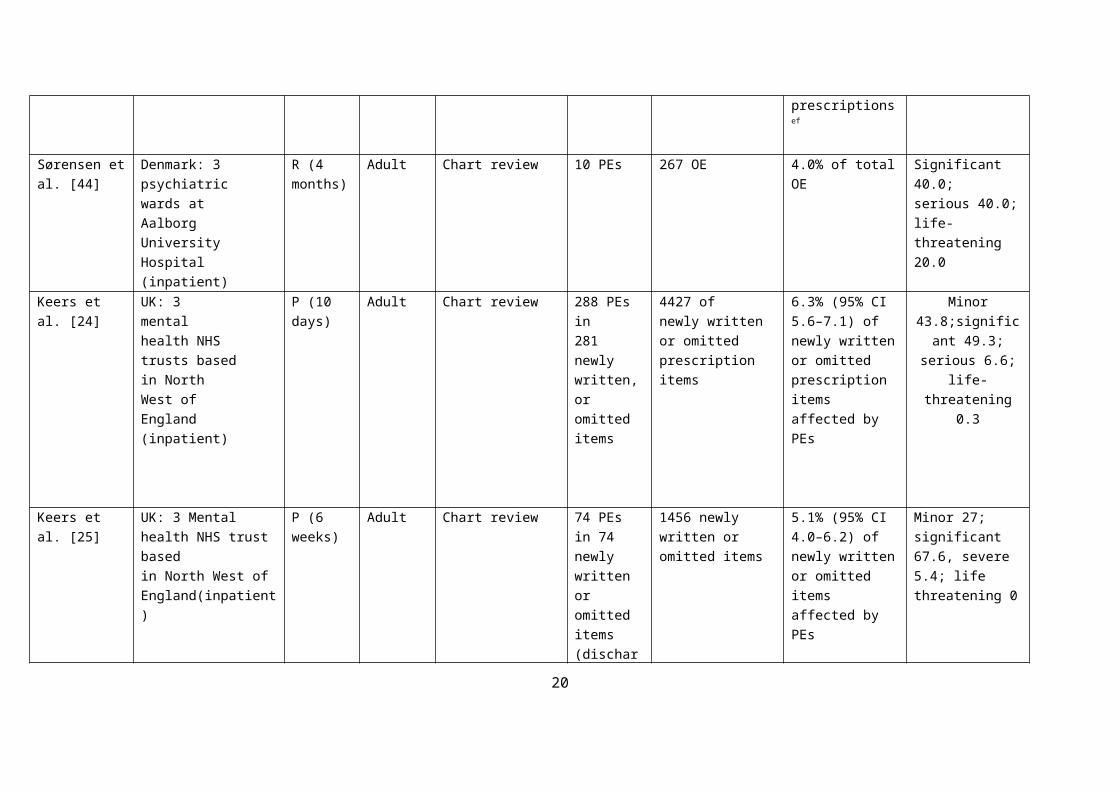
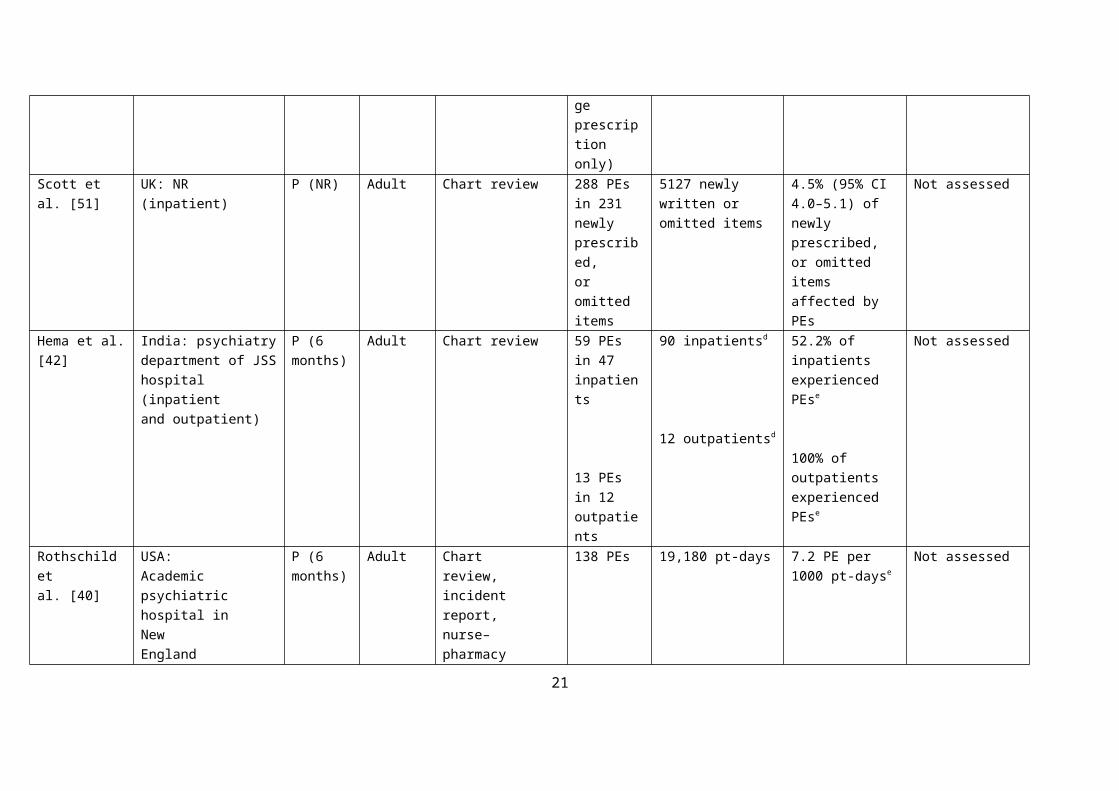
Table 1 Characteristics of studies examining medication errors and adverse drug events in mental health hospitals
Study Country:study site
(studysetting)
Studydesign
(duration)
Patientgroup
Datacollectionmethod
Numerator Denominator Error rate Severity %
Medication error
Rothschild etal. [40]
USA:Academic psychiatrichospital inNewEnglandarea(inpatient)
P (6 months)
Adult Chartreview,incidentreport,nurse–pharmacyreports
203 MEs19,180 pt-days
10.6 per 1000 pt-days
Significant 50.7; serious 44.8; life-threatening 4.4
Grasso et al.[45]
USA:AugustaMentalHealthInstitute, aState psychiatrichospital(inpatient)
R(5Months)
Adult Chart review239 PEs498 TEs 1443MAEsa
1448 pt-days 156 PE per 1000 pt-days344 TE per 1000 pt-days997 MAE per 1000 pt-days
Low 19.0; moderate 23.0; high 58.0b
Sirithongthavonet al. [43]
Thailand:tertiarypsychiatriccarehospital (outpatient)
P(12 months)
Paediatric Chart review 180 MEsc 7444Prescriptions
2.4% of prescription Not assessed
Sørensen et al.[44]
Denmark: 3psychiatricwards atAalborgUniversityHospital(inpatient)
P/R(4 months)
Adult Directobservation,unannouncedcontrolvisits, chartreview
189 MEs 1082 OEs 17.4% of total OEs Non-significant 17.4; Significant 28; serious 42.3;
life-threatening 2.1
11

Hema et al.[42]
India:psychiatrydepartmentof JSSHospital(inpatientandoutpatient)
P (6 months)
Adult Chart review 215 MEs in 102pts
166 ptsd 61.4% of pts experienced MEs
Category A 0Category B 19.0Category C 80.0Category D 0.9
Ayani et al.[41]
Japan: 1Psychiatric hospital and 1 tertiaryCare teachinghospital(inpatient)
R (1 year)
Adult Chartreview,incidentreport,laboratoryresult
398 MEs 22,733 pt-days 17.5 per 1000 pt-days
Not assessed
Prescribing errorNirodi andMitchell [46]
UK: 2psychiatricinpatientunits (inpatient)
R (7 years) Elderly Chart review 92 pts experienced PEs
112 pts 82.1% of pts experienced PEse
Not assessed
Grasso et al.[52]
USA: Augusta Mental Health Institute, astate psychiatrichospital (inpatient)
R (4 months)
Adult Chart review 20 medication lists affected by PEs
110 dischargemedicationlists
18.0% of discharge medication lists affected by PEs
Not assessed
Haw andStubbs [48]
UK: StAndrew’shospital(inpatient)
P (1 month)
Adult Chart review 311 PEs in 50 prescription items
2274prescriptionitems
2.2% of prescription items affected by PEs
55.6 minimal clinical significance: 35.7 clinically significant, 8.7 could cause potential harm; 0 potentially life-threatening
12
Grasso et al.[45]
USA: Augusta Mental Health Institute, aState psychiatricHospital (inpatient)
R(5Months)
Adult Chart review 239 PEs 1448 pt-days 165.5 PE per 1000 pt-days
Not assessed
Stubbs et al.[47]
UK: 9centres (8acute ormentalhealthtrusts andoneindependentpsychiatrichospital)(inpatient)
P (1 week) Adult Chart review 523 PEs in 523 prescription items
22,036prescriptionitems
2.4% of prescription items affected by PEs
47.8 negligible 45.9 minor; 3.3 serious; 1.0 fatal
Shawahna andUr-Rahman [50]
Pakistan:psychiatrydepartmentin ahospital inLahore(inpatient)
P (15 days) Adult Chart review 33 PEs in 77 prescription items
84prescriptionitems
91.6% of prescription items affected by PEse
Not assessed
Jhanjee et al.[49]
India: psychiatryoutpatientdepartmentof GuruTeghBahadurhospital inDelhi(outpatient)
P (Mar 2009to Nov2011)
Adult Chart review 1131 PEsc
899 PEsc
648Prescriptions
464antipsychoticonlyprescriptions
175.0 per 100 prescription ef
193.7 per 100 antipsychotic only prescriptions ef
Not assessed
13
Sørensen et al. [44]
Denmark: 3psychiatricwards atAalborgUniversityHospital(inpatient)
R (4 months)
Adult Chart review 10 PEs 267 OE 4.0% of total OE Significant 40.0; serious 40.0; life-threatening 20.0
Keers et al. [24] UK: 3mentalhealth NHStrusts basedin NorthWest ofEngland(inpatient)
P (10 days) Adult Chart review 288 PEs in281 newlywritten,or omitteditems
4427 ofnewly writtenor omittedprescriptionitems
6.3% (95% CI5.6–7.1) ofnewly writtenor omittedprescriptionitems affected by PEs
Minor 43.8;significant
49.3; serious 6.6; life-threatening 0.3
Keers et al. [25] UK: 3 Mental health NHS trust basedin North West ofEngland(inpatient)
P (6 weeks)
Adult Chart review 74 PEs in 74 newly written or omitted items(dischargeprescriptiononly)
1456 newlywritten oromitted items
5.1% (95% CI4.0–6.2) of newly written or omitted items affected by PEs
Minor 27; significant 67.6, severe 5.4; life threatening 0
Scott et al. [51] UK: NR(inpatient)
P (NR) Adult Chart review 288 PEs in 231newlyprescribed,or omitteditems
5127 newlywritten oromitted items
4.5% (95% CI4.0–5.1) ofnewlyprescribed,or omitteditems affected by PEs
Not assessed
Hema et al. [42] India: psychiatrydepartment of JSShospital (inpatientand outpatient)
P (6 months)
Adult Chart review 59 PEs in 47 inpatients
90 inpatientsd 52.2% of inpatients experienced PEse
Not assessed
14

13 PEs in 12 outpatients
12 outpatientsd100% of outpatients experienced PEse
Rothschild etal. [40]
USA:Academic psychiatrichospital inNewEnglandarea(inpatient)
P (6 months)
Adult Chartreview,incidentreport,nurse–pharmacyreports
138 PEs 19,180 pt-days 7.2 PE per 1000 pt-dayse
Not assessed
Sirithongthavonet al. [43]
Thailand:tertiarypsychiatriccarehospital (outpatient)
P (12 months)
Paediatric Chart review 68 PEsc 7444Prescriptions
0.9% of prescriptionse
Not assessed
Transcription errorGrasso et al.[45]
USA: Augusta Mental Health Institute, aState psychiatricHospital (inpatient)
R(5Months)
Adult Chart review 498 TEs 1448 pt-days 344 TE per 1000 pt-days
Not assessed
Rothschild etal. [40]
USA:Academic psychiatrichospital inNewEnglandarea(inpatient)
P (6 months)
Adult Chartreview,incidentreport,nurse–pharmacyreports
40 TEs 19,180 pt-days 2.1 TE per 1000 pt-dayse
Not assessed
15

Sirithongthavonet al. [43]
Thailand:tertiarypsychiatriccarehospital (outpatient)
P (12 months)
Paediatric Chart review 86 TEsc 7444Prescriptions
1.1% of prescriptionse
Not assessed
Unintentional medication discrepancyBrownlie et al.[53]
UK: SouthEssexPartnershipUniversity NHSFoundationTrustAssessmentUnit(inpatient)
P (3 months)
Adult Chart review 601unintentionaldiscrepancies in 212 admissions
377 ptadmissions
56.0% of admissions affected by unintentional medication discrepancies
If error corrected:62.3 minor; 37.7
moderate.If discrepancy continued to primary care: 23 minor; 76.3 moderate
Medication administration error
Grasso et al.[45]
USA:Augusta MentalHealth Institute, aState psychiatricHospital (inpatient)
R(5months)
Adult Chart review 1443 MAEs 1448 pt-days997 MAE per 1000 pt-days
Not assessed
Haw et al. [54] UK: 2 long staywards at St. Andrew’sHospital(inpatient)
P (4 weeks)
Elderly Directobservation,chart review,incidentreport
369 MAEs 1423 OE 25.9% of total OE Doubtful importance 69.0; minor 7.3, serious 0.3; could not be rated 23.3
Sørensen et al. [44]
Denmark: 3 psychiatricwards at AalborgUniversity Hospital(inpatient)
R(4 months)
Adult Directobservation
142 MAEs 340 OE 42.0% of total OE Non-significant 20.0; significant 27.0; serious 51.0; life-threatening 1.0
Cottney[22]
UK: 21-bed acuteMental health ward
P (3 weeks)
Adult Directobservation
138 MAEs 1542 OE 8.9% of total OE Negligible 40.0; 60.0 minor
16

at East LondonNHS FoundationTrust (inpatient)
Cottney andInnes [23]
UK: 43 wards in East London NationalHealth Trust (inpatient)
P (NR) Adult Directobservation
139 MAEs 4177 OE 3.3% of total OE Negligible 19.0, minor 71.0, serious 11.0; fatal 0
Abduldaeem etal. [55]
UK: 2 acuteMental health wards inPharmacy BerkshireHealthcare NHSfoundation trust(inpatient)
P (NR) Adult Directobservation
153 MAEs 317 OE 48.0% of total OE Not assessed
Hema et al.[42]
India: psychiatry department of JSS Hospital (inpatient)
P (6 months)
Adult Chart review 133 MAEs in 88 pts
90 patientsd 97.7% of inpatients experienced MAEse Not assessed
Rothschild etal. [40]
USA:Academic psychiatrichospital inNew England area(inpatient)
P (6 months)
Adult Chartreview,incidentreport,nurse–pharmacyreports
20 MAEs 19,180 pt-days 1.0 MAE per 1000 pt-dayse
Not assessed
Dispensing errorSørensen et al. [44]
Denmark: 3 psychiatricwards at AalborgUniversity Hospital (inpatient)
P (4 months)
Adult Directobservation,unannouncedcontrol visit
18 DEs 391 OE 4.6% of total OE Non-significant 22.2; significant 61.0; serious 33.0; life-threatening 0
Hema et al.[42]
India: Psychiatry department of JSSHospital (inpatient)
P (6 months)
Adult Chart review 10 DEs in 8 pts
90 patientsd 8.8% of pts experienced DEse
Not assessed
Sirithongthavonet al. [43]
Thailand: tertiaryPsychiatric care hospital (outpatient)
P (12 months)
Paediatric Chart review 17 DEsc 7444Prescriptions
0.2% of prescriptionse
Not assessed
Adverse drug events
17

Rothschild etal. [40]
USA: 172-Bed academicpsychiatrichospital inNew EnglandArea (inpatient)
P (6 months)
Adult Chartreview,incidentreport,nurse–pharmacyreports
191 ADEs,25 pADEs
19,180 pt-days 10 ADEs per 1000 pt-days;
1.3 pADE per 1000 pt-days
ADE: significant 66.0; serious 31.0;
life-threatening 2.0;fatal 0
pADE: significant 68;serious 24; life-
threatening 8Ayani et al. [41] Japan: psychiatric
units at one psychiatrichospital and one tertiary care teaching hospital (inpatient)
R (1 year) Adult Chartreview,incidentreport,laboratoryresult
955 ADEs,166 pADEs
22,733 pt-days 42 ADE per 1000 pt-days
7.3 pADE per 1000 pt-days
ADE: significant 71.0; serious 28.0; life-threatening 1.4, fatal 0pADEs: NR
ADE(s) adverse drug event(s), CI confidence interval, DE(s) dispensing error(s), MAE(s) medication administration error(s), ME(s) medication error(s), NR reported, OE opportunity for error, P prospective, pADE(s) preventable adverse drug event(s), PE(s) prescribing error(s), TE(s) transcription error(s), pt(s) patient(s), R retrospective
a The number of dispensing errors excluded as the study relied only in incident report to detect dispensing errorb The data presented include dispensing error severity datac The number of prescriptions affected by medication errors was not reportedd All included patients were received at least one antipsychotic agente Self-calculatedf There was more than one type of ME in prescriptions (the total number of MEs identified is more than the number of prescriptions/items examined)
18

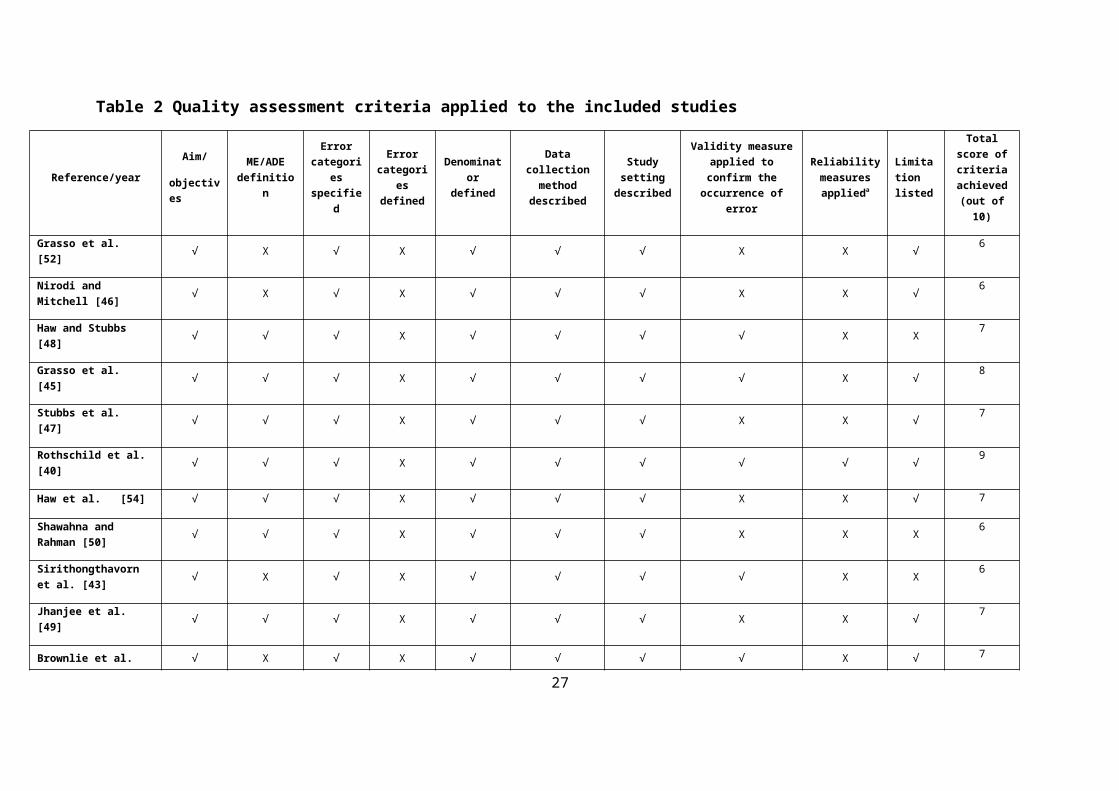
Table 2 Quality assessment criteria applied to the included studies
Reference/yearAim/
objectives
ME/ADE definition
Error categories specified
Error categories
defined
Denominator defined
Data collection method
described
Study setting described
Validity measure applied to confirm the
occurrence of error
Reliability measures applieda
Limitation listed
Total score of criteria achieved
(out of 10)
Grasso et al. [52] √ X √ X √ √ √ X X √ 6
Nirodi and Mitchell [46] √ X √ X √ √ √ X X √ 6
Haw and Stubbs [48] √ √ √ X √ √ √ √ X X 7
Grasso et al. [45] √ √ √ X √ √ √ √ X √ 8
Stubbs et al. [47] √ √ √ X √ √ √ X X √ 7
Rothschild et al. [40] √ √ √ X √ √ √ √ √ √ 9
Haw et al. [54] √ √ √ X √ √ √ X X √ 7
Shawahna and Rahman [50] √ √ √ X √ √ √ X X X 6
Sirithongthavorn et al. [43] √ X √ X √ √ √ √ X X 6
Jhanjee et al. [49] √ √ √ X √ √ √ X X √ 7
Brownlie et al. [53] √ X √ X √ √ √ √ X √ 7
Soerensen et al. [44] √ √ √ √ √ √ √ X √ √ 9
Keers et al. [24] √ √ √ X √ √ √ √ X √ 8
Cottney [22] √ √ √ X √ √ √ √ X √ 8
Hema et al. [42] √ √ √ X √ √ √ X X √ 7
Keers et al. [25] √ √ √ X √ √ √ √ X √ 8
Cottney and Innes [23] √ √ √ X √ √ √ √ X √ 8
Ayani et al. [41] √ √ √ X √ √ √ √ √ √ 9
19
Abduldaeem et al. [55] √ √ √ X √ √ √ X X X 6
Scott et al. [51] √ √ √ X √ √ √ √ b X X 7
ADE adverse drug event, ME medication error, H and X indicate criteria achieved or not achieved by study, respectivelya Inter-rater reliabilityb Information obtained from study author
20
3.2.2. Prescribing errors
In total, 14 studies reported data concerning the frequency of PEs, making it the most frequent error type studied
[24, 25, 40, 42-52]. A total of 50.0% of studies [24, 25, 47-51] used the PE definition proposed by Dean et al.
[56], namely ‘‘a clinically meaningful prescribing error occurs when, as a result of a prescribing decision or
prescription writing process, there is an unintentional significant (1) reduction in the probability of treatment
being timely and effective or (2) increase in the risk of harm when compared with generally accepted practice’’.
However, in the mental health setting, several additional clinical scenarios were added to adapt this definition,
including prescribing a drug without registering a patient with the drug company and performing the necessary
monitoring (e.g. for clozapine) or prescribing a drug to mental health patients without a Mental Health Act form
authorization. One study [44] used the definition of a PE by Lisby et al. [57], and the remaining six studies
(42.8%) did not state any definition at all [40, 42, 43, 45, 46, 52]. The majority of studies (n = 10 [71.4%]) were
conducted prospectively [24, 25, 40, 42, 43, 47-51] except for four studies that used a retrospective design [44-
46, 52]. All studies were conducted in inpatient settings except two studies that took place in an outpatient
setting [43, 49] and another which took place across both inpatients and outpatients [42]. Chart review was the
method used for detecting PEs by all studies except one study which also used incident reports and
nurse/pharmacy staff reports [40].
Pharmacists collected the data in six studies [24, 25, 47, 48, 51, 52], combinations of health care professionals
were used in three studies [40, 43, 45] and physicians in one study [46]. Four studies did not specify the
professional status of the data collectors [42, 44, 49, 50]. The presence of PE was confirmed either by using one
reviewer (medical director) in one study [45] or a panel of healthcare professionals in four studies [24, 25, 40,
48, 51]; the rest did not report any process of error validation [42-44, 46, 47, 49, 50, 52]. Across the studies,
there were differences in the types of denominator used to determine PE rates. Three studies (one focused on
PEs on hospital discharge) [25] provided the PE rate per newly written or omitted item checked, the rate of
which ranged from 4.5 to 6.3% [24, 25, 51]. A further three PE studies reported a rate of errors for all
prescription items affected by PEs, with a rate range of 2.2–91.6% [47, 48, 50]. A range of 52.2–82.1% of
patients [42, 46], 7.2–165 per 1000 patient-days [44] (see Table 1). In paediatric outpatient setting, the rate of
PE was 0.9% of complete prescriptions checked [43].
Two studies from the UK found that senior physicians were more likely than more junior physicians to make
PEs [24, 25]. In addition, the use of an electronic prescription pro forma and the number of medication items
prescribed were found to increase the risk of PEs on discharge prescriptions [25]. The most frequent PEs
reported involved the omission of regularly prescribed medication (12.5%) [24], missing or incorrect dose
(23.3%) [51] and writing incomplete prescriptions [47, 48]. Three studies found that psychotropic therapies
were more commonly associated with PEs [25, 44, 47], in contrast to two studies that found that non-
psychotropic therapy was commonly involved, particularly antimicrobial medication [48, 51]. The severity of
harm classified for most PEs was potentially significant (9.0–49.3%) or minor (27.0–44.0%). Some PEs were
21

assessed as having the potential to cause serious harm (3.3–40%) or even death (0.3–20%) if not prevented [24,
25, 44, 47].
3.2.3. Unintentional Medication Discrepancy
One study investigated the rate of unintentional discrepancy at the time of hospital admission for 382 patients
[53]. Medication chart review was conducted prospectively by pharmacy technician to detect discrepancies. The
medication discrepancies were validated by approaching the clinical team involved with each identified
discrepancy. Fifty six percent of hospital admissions were associated with unintentional medication
discrepancies. Increasing age and polypharmacy found to increase the risk of unintentional medication
discrepancy at hospital admission. Drug omission was the most frequent type of discrepancy reported (77.2%)
followed by wrong/unclear dose prescribed (7.0%). The potential severity of unintentional medication
discrepancies was rated as moderate in 37.7% and minor in 62.3% of cases [53].
3.2.4. Transcription errors
Three studies investigated the rate of transcription errors with two studies conducted in the US [40, 45] and one
study conducted in Thailand [43]. Two studies used chart review to detect TEs [43, 45], whereas the other used
a combination of chart review, incident report review and pharmacy and nurse staff reports [40]. All studies
were conducted in inpatient settings [40, 45] except one study that took place in an outpatient paediatric setting
[43]. None of these studies provided a definition of transcription error. However, two studies specified
transcription error categories [43, 45]. Two studies used nurse, pharmacist, and physician data collectors [40,
43] and the other used nurse and pharmacist data collectors [45]. The reported rate of TE was between 1.1–344
per 1000 patient-days [40, 43, 45]. Situations in which the medication order was not transcribed [45] or
transcribed incorrectly [43, 45] were found to be the most common TE subtypes reported.
3.2.5. Medication Administration Errors
Eight studies assessed the rate of MAEs. All studies [22, 23, 54, 55] used the MAE definition developed by
Baker et al. [58] except two studies, one of which [44] used the definition proposed by Lisby et al. [57], and the
other three studies did not state any definition [40, 42, 45]. Six studies used a prospective design [22, 23, 40, 42,
44, 55], and one was conducted retrospectively [45]. One study used both a retrospective and a prospective
design to detect MAE [54]. Direct observation was the most common method for detecting MAEs, representing
the sole data collection method in four studies [22, 23, 44, 55]. Two studies relied only on chart review to detect
error [42, 45], while the other two studies used a combination of the above methods in addition to incident
reports [54] and nurse and pharmacy reports [40]. Pharmacists collected the data in four studies [22, 23, 54, 55],
a pharmacy director and nurse in two studies [40, 45], whereas the remaining studies did not specify the
professional status of the data collector [42, 44]. In three studies, MAEs were validated independently either by
senior pharmacists [22, 23] or by a medical director [45], and the remaining two studies used a consensus
meeting of the research team [44, 54].
22

The total OE was used as the error denominator by most MAE studies [22, 23, 44, 54, 55], except for three that
used patient-days [40, 45] or number of patients [42] as the denominator. The Barker et al. definition of OE was
used by three studies [22, 23, 55], and the remaining studies either developed their own definition [44] or did
not state any [54]. The rate of MAEs reported in studies using similar denominators ranged from 3.3 to 48.0%
of total OE [22, 23, 44, 54, 55], 1.0–997.0 per 1000 patient-days [40, 45] or 97.7% of patients [42]. One study
found that greater numbers of interruptions, patients on the ward, doses administered, and medication doses due
significantly increased the rate of MAEs [23]. Other factors, such as non-oral route of medication
administration, presence of organic brain disease (e.g. dementia), swallowing difficulties or patients who
regularly refused to take their medication were associated with MAEs in elderly patients [54]. Wrong time
errors (1.9–39.2%) and drug omissions (7.5–57%) were reported to be the two most common MAE types
identified across the studies [22, 23, 42, 44, 54, 55]. Only two studies examined whether psychotropic or non-
psychotropic drugs were more likely to be related to MAEs; their conclusions were conflicting [44, 54]. Severity
ratings varied across the studies, with 7.3–71.0% classified as minor severity and 0.3–5.0% as potentially
serious [22, 23, 44, 54].
3.2.6. Dispensing Errors
The rate of DEs was assessed by three studies [42-44]. Two studies were conducted in an adult inpatient setting
[42, 44] and one took place in an outpatient paediatric setting [43]. Dispensing errors were detected by direct
observation and unannounced control visits in one study [44] and by chart review in two studies [42, 43]. In
adult inpatient settings, DE reported rates were 4.6% of total OE [44] and 8.8% of patients [42], while the
reported rate in paediatric outpatient setting was 0.2% of complete prescriptions checked [43]. The most
common types of DE were wrong medication brand (87.5%), dose omission (50.0%), and incorrect labelling of
medication (22.0%) [42, 44]. The potential severity was assessed in one study using two senior clinical
pharmacologists; 61.1% of DE were assessed as having potentially clinically significant effects, with the
remainder classed as potentially serious [44].
4. Discussion
Our systematic review found that MEs in mental health hospitals are common and do cause harm to psychiatric
patients. Such risks affect multiple stages of the medication use process (prescribing, dispensing and
administration) and are common at points of care transfer and outpatient hospital settings. Of the 20 studies
identified, only two examined actual harm due to medication use. The reported ranges of ME and ADE rates in
mental health hospitals appear to overlap with reported IQRs of MEs and ADEs in general hospitals [3-5].
However, the risk associated with these errors differed according to the type of medication involved.
Psychotropic medication was found to be more frequently associated with MEs and ADEs than were non-
psychotropic medicines. Atypical antipsychotics were the most common class of psychotropic medication
involved with ADEs and MEs [40, 41]. In general hospitals, analgesics [29], anti-infective agents [59, 60] and
cardiovascular medications were commonly associated with ADEs [61], whereas anti-infectives [3] and
cardiovascular and gastrointestinal medications [4] were found to be more often associated with PEs and MAEs,
respectively. Therefore, understanding the risks associated with psychotropic medicines is crucial for improving
23

safety in mental health hospitals. Drug omission, incorrect dose and wrong time errors were by far the most
commonly observed ME subtypes in mental health hospitals. This is similar to results reported in systematic
reviews of PE and MAE in general hospitals [3, 4, 39]. Other evidence from the US also found that wrong time
error, drug omission, and incorrect dose were the three most common types of MEs in 36 healthcare facilities
[58]. Future research should target these types of MEs to improve medication safety in mental health hospitals.
The majority of studies assessed the severity of MEs and ADEs. However, variations in the scales used to assess
severity precluded direct comparisons. This variability has also been recognised as a limitation in other reviews
of MEs [3, 4]. For studies that used a similar assessment scale, the majority of MEs that caused actual patient
harm were of significant severity [40, 41]. Future research should seek standardization between severity
assessment scales to allow for direct comparison. We found that around 65.0% of the included studies were
conducted after 2006, highlighting that research examining MEs and ADEs in mental health settings is a
developing area. In addition, the majority of ME studies were conducted in the UK, [22-25, 46-48, 51, 53-55],
whereas only a few were published in other Western (Denmark, USA) [40, 44] and Asian (Japan, Thailand,
Pakistan and India) regions [41-43, 49, 50]. To gain deeper insight into the scale of MEs in mental health
hospitals, it is important to obtain additional epidemiological evidence from other countries, which would be
important in understanding the differences in healthcare practices within mental health hospitals from a global
perspective. In terms of ADEs, only two studies from the USA and Japan have investigated the frequency of
ADEs [40, 41]; as no information is available from other countries, this should be considered an important target
for future research. Overall, whilst the included studies varied in terms of outcome definitions and research
methods, it is important to highlight the emerging consistency in study design that has been achieved in studies
investigating ADE, PE and MAE emerging recently. For instance, in MAE studies based in the UK, consistency
was achieved in terms of the data collection method (direct observation, a recognised gold standard) [62] and
denominator used (OE, the most common in the wider literature) [4]. PE studies (also based in the UK) used
similar PE definitions [56], denominators (newly omitted and written items [n = 3 studies]) [24, 25, 51] and data
collection methods (chart review) [24, 25, 44-52]. Such homogeneity could be used as a benchmark for ongoing
research projects in the field as well as to facilitate comparisons of ME rates in mental health hospitals. Greater
standardisation in study methodology is needed, not only to support direct comparisons between different
studies but also to address deficits in the global knowledge on medication safety in mental health settings. This
review showed that MEs at the mental healthcare interface between secondary and primary care frequently
present a risk of causing harm to patients [24, 52, 53]. However, the majority of these data were from secondary
care, and little is known about the frequency of such errors after hospital discharge back to the community [63-
65]. Evidence from the UK found that a ME occurs in 69.0% and 43.0% of medications at the time of admission
to and discharge from mental health hospitals, respectively [66]. Other recent evidence from the USA suggests
that 23.3% of psychiatric patients had at least one unintentional discrepancy at the time of hospital discharge
[67]. These estimates clearly highlight the importance of medication reconciliation at care interfaces in mental
health settings to improve safe care transfer [68, 69]. This is supported by recent studies reporting on the clinical
benefit of medication reconciliation at the mental healthcare interface [66, 67, 70, 71]. Accordingly, a recent
national UK survey [72] found that medication reconciliation is now common practice in the majority of mental
health services in the UK. Further research is required to identify the burden of MEs at interfaces between
24

mental healthcare settings. Few studies have been published that evaluate interventions to reduce the number of
MEs in mental health hospitals [22, 52, 73]. A study based in a US psychiatric hospital found that using a
personal digital assistant (PDA) reduced the rate of MEs in discharge lists from 18.0 to 8.0% [52]. Another
study investigated the effectiveness of implementing a provider order entry (POE) programme to reduce error in
mental health hospitals [73]. However, none of these studies described the type of MEs involved or their
potential to cause harm to patients. Another UK-based study examined the impact on the rate of MAEs of
implementing an automated dispensing cabinet in a mental health hospital; it found the cabinet to be associated
with a reduction in MAE rate from 8.9 to 7.2% as well as a reduction in the time spent by nurses administering
medication from 2.9 to 2.3 min per dose [22]. However, implementing a successful intervention to reduce the
number of MEs in a hospital is largely based on understanding the causes and risk factors associated with their
occurrence [74-76]. Although this is beyond the scope of this study, some of the included studies highlighted
some of the risk factors associated with the occurrence of MEs in mental health hospitals [23-25], and the first
in-depth qualitative study of the causes of MAEs in this setting has emerged [77]. Future qualitative studies are
needed to identify the root causes and risk factors associated with MEs and ADEs in mental health hospitals to
help design effective remedial interventions. To our knowledge, this is the most up-to-date systematic appraisal
of the evidence examining the frequency, nature and severity of MEs and ADEs in mental health hospitals. A
comprehensive search strategy was used to identify eligible studies from a wide range of databases without
language restriction, and the reference lists of included studies and relevant review papers were manually
searched. Moreover, our inclusion criteria with respect to study designs were stricter than previously published
systematic reviews [20, 21], as we excluded studies based only on incident reports as the sole method of data
collection. However, we were faced with a number of limitations in the studies identified—heterogeneity in the
denominator used, the population involved, and the outcome definition—which limited the opportunity for
direct comparisons between different studies. In addition, studies differed in the way they presented the
classification of drugs involved in MEs/ADEs, with some not reporting any at all. Likewise, different schemes
were used to classify error subtypes. This can be seen, for example, in some MAE studies that considered
nurses’ behaviour, such as unauthorized tablet crushing or failure to report patient identity, as an MAE whereas
other studies did not—all of which eventually affected the reported MAE frequency. With this in mind, these
specific study limitations should be considered when drawing conclusions from the findings of this review.
5. Conclusion
MEs and ADEs are common in mental health hospitals. Medication safety interventions should target risks
associated with psychotropic medicines, especially at the prescribing and administration stages of the medicine
use process. Further research is required to investigate the rate of DEs, unintentional discrepancies and ADEs in
mental health hospitals. Future research should examine the underlying causes of MEs and ADEs so theory-
based interventions can be developed and evaluated to improve patient safety in this specialist healthcare
setting.
25
6. References
1. World Health Organization. World alliance for patient safety.Geneva: WHO; 2005. http://www.who.int/patientsafety/en/brochure_final.pdf. Accessed 15 April 2016.2. de Vries EN, Ramrattan MA, Smorenburg SM, Gouma DJ, Boermeester MA. The incidence and nature of in-hospital adverse events: a systematic review. Quality and Safety in Health Care. 2008;17(3):216-23.3. Lewis PJ, Dornan T, Taylor D, Tully MP, Wass V, Ashcroft DM. Prevalence, incidence and nature of prescribing errors in hospital inpatients. Drug Safety. 2009;32(5):379-89.4. Keers RN, Williams SD, Cooke J, Ashcroft DM. Prevalence and nature of medication administration errors in health care settings: a systematic review of direct observational evidence. Annals of Pharmacotherapy. 2013;47(2):237-56.5. James KL, Barlow D, McArtney R, Hiom S, Roberts D, Whittlesea C. Incidence, type and causes of dispensing errors: a review of the literature. International journal of pharmacy practice. 2009;17(1):9-30.6. Hert M, Correll CU, Bobes J, Cetkovich Bakmas M, Cohen D, Asai I, et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World psychiatry. 2011;10(1):52-77.7. Hert M, Cohen D, Bobes J, Cetkovich Bakmas M, Leucht S, Ndetei DM, et al. Physical illness in patients with severe mental disorders. II. Barriers to care, monitoring and treatment guidelines, plus recommendations at the system and individual level. World psychiatry. 2011;10(2):138-51.8. Procyshyn RM, Barr AM, Brickell T, Honer WG. Medication errors in psychiatry: A comprehensive review. CNS Drugs. 2010;24(7):595-609.9. Latoo J, Mistry M, Dunne FJ. Physical morbidity and mortality in people with mental illness. British Journal of Medical Practitioners. 2013;6(3):621-3.10. Kane JM, Kishimoto T, Correll CU. Non-adherence to medication in patients with psychotic disorders: epidemiology, contributing factors and management strategies. World Psychiatry. 2013;12(3):216-26.11. Chapman SC, Horne R. Medication nonadherence and psychiatry. Current Opinion in Psychiatry. 2013;26(5):446-52.12. The National Archives.Mental Health Act 2007. http://www.legislation.gov.uk/ukpga/2007/12/contents. Accessed 1 feb 2017.13. Newcomer JW. Metabolic considerations in the use of antipsychotic medications: a review of recent evidence. The Journal of Clinical Psychiatry. 2007.14. Teixeira PJR, Rocha FL. The prevalence of metabolic syndrome among psychiatric inpatients in Brazil. Revista brasileira de psiquiatria. 2007;29(4):330-6.15. Kukreja S, Kalra G, Shah N, Shrivastava A. Polypharmacy In Psychiatry: A Review. Mens Sana Monographs. 2013;11(1):82-99.16. Centorrino F, Goren JL, Hennen J, Salvatore P, Kelleher JP, Baldessarini RJ. Multiple versus single antipsychotic agents for hospitalized psychiatric patients: case-control study of risks versus benefits. American Journal of Psychiatry. 2004;161(4):700-6.17. Lelliott P, Paton C, Harrington M, Konsolaki M, Sensky T, Okocha C. The influence of patient variables on polypharmacy and combined high dose of antipsychotic drugs prescribed for in-patients. The Psychiatrist. 2002;26(11):411-4.18. Sinclair LI, Davies SJ, Parton G, Potokar JP. Drug–drug interactions in general hospital and psychiatric hospital in-patients prescribed psychotropic medications. Int J Psychiatry Clin Pract. 2010;14(3):212-9.19. Grasso BC, Rothschild JM, Genest R, Bates DW. What do we know about medication errors in inpatient psychiatry? Joint Commission journal on quality and safety. 2003;29(8):391-400.20. Maidment ID, Lelliott P, Paton C. Medication errors in mental healthcare: A systematic review. Quality and Safety in Health Care. 2006;15(6):409-13.21. Maidment ID, Haw C, Stubbs J, Fox C, Katona C, Franklin BD. Medication errors in older people with mental health problems: a review. International journal of geriatric psychiatry. 2008;23(6):564-73.22. Cottney A. Improving the safety and efficiency of nurse medication rounds through the introduction of an automated dispensing cabinet. BMJ quality improvement reports. 2014;3(1):u204237. w1843.23. Cottney A, Innes J. Medication-administration errors in an urban mental health hospital: A direct observation study. International Journal of Mental Health Nursing. 2015;24(1):65-74.24. Keers RN, Williams SD, Vattakatuchery JJ, Brown P, Miller J, Prescott L, et al. Prevalence, nature and predictors of prescribing errors in mental health hospitals: a prospective multicentre study. BMJ open. 2014;4(9):e006084.
26
25. Keers RN, Williams SD, Vattakatuchery JJ, Brown P, Miller J, Prescott L, et al. Medication safety at the interface: Evaluating risks associated with discharge prescriptions from mental health hospitals. Journal of Clinical Pharmacy and Therapeutics. 2015;40(6):645-54.26. Ito H, Yamazumi S. Common types of medication errors on long-term psychiatric care units. International Journal for Quality in Health Care. 2003;15(3):207-12.27. Haw CM, Dickens G, Stubbs J. A review of medication administration errors reported in a large psychiatric hospital in the United kingdom. Psychiatric Services. 2005;56(12):1610-3.28. Meyer-Massetti C, Cheng CM, Schwappach DL, Paulsen L, Ide B, Meier CR, et al. Systematic review of medication safety assessment methods. Am J Health Syst Pharm. 2011;68(3):227-40.29. Bates DW, Cullen DJ, Laird N, Petersen LA, Small SD, Servi D, et al. Incidence of adverse drug events and potential adverse drug events: implications for prevention. Jama. 1995;274(1):29-34.30. Bates DW, Miller EB, Cullen DJ, Burdick L, Williams L, Laird N, et al. Patient risk factors for adverse drug events in hospitalized patients. Archives of internal medicine. 1999;159(21):2553-60.31. National Coordinating Council for Medication Error Reporting and Prevention. About Medication Errors: What is a Medication Error.2015. http://www.nccmerp.org/aboutMedErrors. Accessed 2 Feb 2016.32. Mueller SK, Sponsler KC, Kripalani S, Schnipper JL. Hospital-based medication reconciliation practices: a systematic review. Arch Intern Med. 2012;172(14):1057-69.33. Kohn LT, Corrigan JM, Donaldson MS. To err is human: building a safer health system. Washington, D.C: National Academies Press; 1999.34. Stelfox HT, Palmisani S, Scurlock C, Orav EJ, Bates DW. The “To Err is Human” report and the patient safety literature. Quality and Safety in Health Care. 2006;15(3):174-8.35. Buetow SA, Sibbald B, Cantrill JA, Halliwell S. Prevalence of potentially inappropriate long term prescribing in general practice in the United Kingdom, 1980–95: systematic literature review. BMJ. 1996 1996-11-30 08:00:00;313(7069):1371-4.36. Allan E, Barker K. Fundamentals of medication error research. American Journal of Health-System Pharmacy. 1990;47(3):555-71.37. Ghaleb MA, Barber N, Franklin BD, Yeung VW, Khaki ZF, Wong IC. Systematic Review of Medication Errors in Pediatric Patients. Annals of Pharmacotherapy. 2006;40(10):1766-76.38. Alsulami Z, Conroy S, Choonara I. Medication errors in the Middle East countries: a systematic review of the literature. European Journal of Clinical Pharmacology. 2013;69(4):995-1008.39. McLeod MC, Barber N, Franklin BD. Methodological variations and their effects on reported medication administration error rates. BMJ quality & safety. 2013;22(4):278-89.40. Rothschild JM, Mann K, Keohane CA, Williams DH, Foskett C, Rosen SL, et al. Medication safety in a psychiatric hospital. General Hospital Psychiatry. 2007;29(2):156-62.41. Ayani N, Sakuma M, Morimoto T, Kikuchi T, Watanabe K, Narumoto J, et al. The epidemiology of adverse drug events and medication errors among psychiatric inpatients in Japan: the JADE study. BMC Psychiatry. 2016;16(1):303.42. Hema Sahithi K, Mohammad I, Manoranjani Reddy J, Nandha Kishore G, Ramesh M, Sebastian J. Assessment of medication errors in psychiatry practice in a tertiary care hospital. International Journal of Pharmaceutical Sciences and Research. 2015;6(1):226-32.43. Sirithongthavorn S, Narkpongphun A, Kamduang N, Isarapongs P, Kanjanarat P. Common types of medication errors of outpatient service in pediatric psychiatry care. Pharmacoepidemiology and Drug Safety (PDS). 2009 August;18 (S1):S245-S6.44. Sørensen AL, Lisby M, Nielsen LP, Poulsen BK, Mainz J. The medication process in a psychiatric hospital: are errors a potential threat to patient safety? Risk management and healthcare policy. 2013;2013(6):23-31.45. Grasso BC, Genest R, Jordan CW, Bates DW. Use of chart and record reviews to detect medication errors in a state psychiatric hospital. Psychiatric Services. 2003 01 May;54(5):677-81.46. Nirodi P, Mitchell A. The quality of psychotropic drug prescribing in patients in psychiatric units for the elderly. Aging & mental health. 2002;6(2):191-6.47. Stubbs J, Haw C, Taylor D. Prescription errors in psychiatry - a multi-centre study. Journal of Psychopharmacology. 2006;20(4):553-61.48. Haw C, Stubbs J. Prescribing errors at a psychiatric hospital. Pharmacy in Practice. 2003;13(2):64-6.49. Jhanjee A, Bhatia M, Oberoi A, Srivastava S. Medication errors in psychiatric practice—A Cross-sectional Study. 2012.50. Shawahna R. Prescribing errors in psychiatry department: An audit from a hospital in Lahore. Journal of Pakistan Psychiatric Society. 2008;5(1):31.51. Scott H, Brown D, Herreraa H.Prevalence and nature of prescribing errors in a mental health setting: analysis of preliminary data from a prospective study. International Journal of Pharmacy Practice. 2016:3:8–13.
27
52. Grasso BC, Genest R, Yung K, Arnold C. Reducing errors in discharge medication lists by using personal digital assistants. Psychiatric Services. 2002;53(10):1325-6.53. Brownlie K, Schneider C, Culliford R, Fox C, Boukouvalas A, Willan C, et al. Medication reconciliation by a pharmacy technician in a mental health assessment unit. International journal of clinical pharmacy. 2014;36(2):303-9.54. Haw C, Stubbs J, Dickens G. An observational study of medication administration errors in old-age psychiatric inpatients. International Journal for Quality in Health Care. 2007;19(4):210-6.55. Abduldaeem H,Masters K, Patel N, Donyai P. A direct observation study of medication administration errors in a mental health inpatient setting. International Journal of Pharmacy Practice 2016; 24(1):4–15.56. Dean B, Barber N, Schachter M. What is a prescribing error? Quality in Health Care. 2000;9(4):232-7.57. Lisby M, Nielsen LP, Mainz J. Errors in the medication process: frequency, type, and potential clinical consequences. International Journal for Quality in Health Care. 2005;17(1):15-22.58. Barker KN, Flynn EA, Pepper GA, Bates DW, Mikeal RL. Medication errors observed in 36 health care facilities. Archives of internal medicine. 2002;162(16):1897-903.59. Morimoto T, Sakuma M, Matsui K, Kuramoto N, Toshiro J, Murakami J, et al. Incidence of Adverse Drug Events and Medication Errors in Japan: the JADE Study. Journal of general internal medicine. 2011;26(2):148-53.60. Aljadhey H, Mahmoud MA, Ahmed Y, Sultana R, Zouein S, Alshanawani S, et al. Incidence of adverse drug events in public and private hospitals in Riyadh, Saudi Arabia: the (ADESA) prospective cohort study. BMJ open. 2016;6(7):e010831.61. Hug BL, Witkowski DJ, Sox CM, Keohane CA, Seger DL, Yoon C, et al. Adverse drug event rates in six community hospitals and the potential impact of computerized physician order entry for prevention. Journal of general internal medicine. 2010;25(1):31-8.62. Dean B, Barber N. Validity and reliability of observational methods for studying medication administration errors. American Journal of Health-System Pharmacy. 2001;58(1):54-9.63. Bourgeois FT, Shannon MW, Valim C, Mandl KD. Adverse drug events in the outpatient setting: an 11‐year national analysis. Pharmacoepidemiology and drug safety. 2010;19(9):901-10.64. Thomsen LA, Winterstein AG, Sondergaard B, Haugbolle LS, Melander A. Systematic review of the incidence and characteristics of preventable adverse drug events in ambulatory care. Annals of Pharmacotherapy. 2007;41(9):1411-26.65. Taché SV, Sönnichsen A, Ashcroft DM. Prevalence of adverse drug events in ambulatory care: a systematic review. Annals of Pharmacotherapy. 2011;45(7-8):977-89.66. Morcos S, Francis S-A, Duggan C. Where are the weakest links? A descriptive study of discrepancies in prescribing between primary and secondary sectors of mental health service provision. The Psychiatrist. 2002;26(10):371-4.67. Nelson LA, Graham MR, Schaefer MG. Characterization of medication discrepancies occurring at the time of discharge from a state psychiatric inpatient facility. Journal of Pharmacy Practice. 2010 April;23 (2):153-4.68. National Mental Health Development Unit. Getting the medicines right 2: medicines management in mental health crisis resolution and home treatment teams. 2010. http://www.crisiscareconcordat.org.uk/wp-content/uploads/2015/07/Getting-the-Medicines-Right-2.pdf Accessed 10 Sept 2016.69. The Joint Commission . National patient safety goals. 2015. http://www.jointcommission.org/assets/1/6/2015_NPSG_HAP.pdf. Accessed 10 Sept 2016.70. Lizer MH, Brackbill ML. Medication history reconciliation by pharmacists in an inpatient behavioral health unit. American journal of health-system pharmacy. 2007;64(10).71. Paton C, McIntyre S, Bhatti SF, Shingleton-Smith A, Gray R, Gerrett D, et al. Medicines reconciliation on admission to inpatient psychiatric care: findings from a UK quality improvement programme. Therapeutic advances in psychopharmacology. 2011;1(4):101-10.72. Kothari M, Maidment I, Lyon R, Haygarth L. Medicines reconciliation in comparison with NICE guidelines across secondary care mental health organisations. International journal of clinical pharmacy. 2016;38(2):289-95.73. Jayaram G, Doyle D, Steinwachs D, Samuels J. Identifying and reducing medication errors in psychiatry: creating a culture of safety through the use of an adverse event reporting mechanism. Journal of Psychiatric Practice. 2011;17(2):81-8.74. Keers RN, Williams SD, Cooke J, Ashcroft DM. Causes of medication administration errors in hospitals: a systematic review of quantitative and qualitative evidence. Drug safety. 2013;36(11):1045-67.75. Tully MP, Ashcroft DM, Dornan T, Lewis PJ, Taylor D, Wass V. The causes of and factors associated with prescribing errors in hospital inpatients. Drug safety. 2009;32(10):819-36.
28

76. Neale G, Woloshynowych M, Vincent C. Exploring the causes of adverse events in NHS hospital practice. Journal of the Royal Society of Medicine. 2001;94(7):322-30.77. Keers R, Placido M, Bennett K, Clayton K, Brown P, Ashcroft D. Understanding the Causes of Medication Administration Errors in a Mental Health Hospital Using Qualitative Interviews with the Critical Incident Technique. Pharmacoepidemiology and Drug Safety. 2016;25:3-23.
29