fractured fairy tales about fractures! -...
TRANSCRIPT

1
FRACTURED FAIRY TALES ABOUT FRACTURES!
By:
Cynthia Everlith, BSHA, CPC, CMA
Arizona Hand & Wrist Specialists
a division of
OSNA, PLLC
Objectives What is a “fracture”
Different types of “fractures”
l d f Closed “fractures”
Open “fractures”
“Fracture” care
Ethics
Medicare Guides
Modifiers
2
Closed Treatment
l d h Closed Treatment with manipulation
Percutaneous Pin fixation
Open Fracture
Casting/splinting
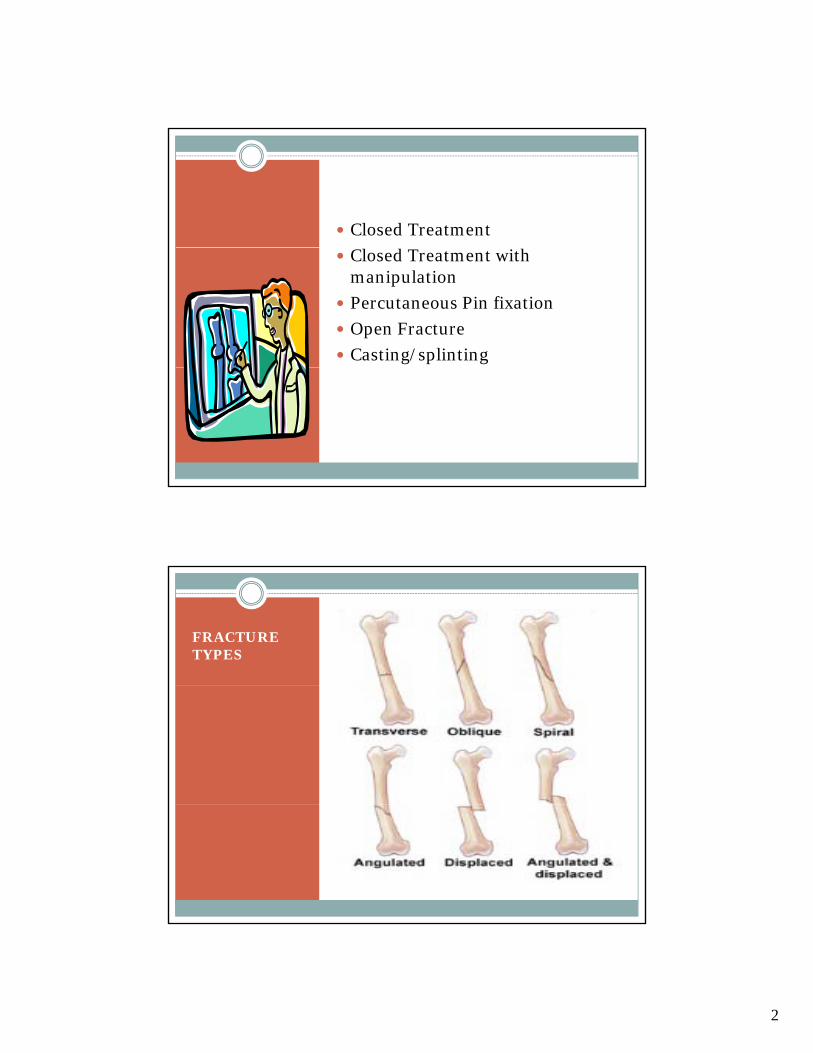
FRACTURETYPES

3
FRACTURES
fracture /frac·ture/
avulsion fracture separation of a small fragment of bone cortex at the site of attachment of a ligament or tendon. axial compression fracture fracture of a vertebra by excessive vertical force so that pieces of it move out in horizontal
directions. Barton's fracture fracture of the distal end of the radius into the wrist joint. Bennett's fracture fracture of the base of the first metacarpal bone running into the carpometacarpal joint, complicated by
subluxation. blow-out fracture fracture of the orbital floor caused by a sudden increase of intraorbital pressure due to traumatic force; the
orbital contents herniate into the maxillary sinus so that the inferior rectus or inferior oblique muscle may become incarcerated in the fracture site, producing diplopia on looking up.
burst fracture axial compression f. capillary fracture one that appears on a radiogram as a fine, hairlike line, the segments of bone not being separated; sometimes
seen in fractures of the skull. closed fracture one that does not produce an open wound in the skin; cf. open f. Colles' fracture fracture of the lower end of the radius, the lower fragment being displaced backward; if the lower fragment is
displaced forward, it is a reverse Colles' fracture. comminuted fracture one in which the bone is splintered or crushed. complete fracture one involving the entire cross section of the bone. compound fracture open f.
(frak´cher) 1. the breaking of a part, especially a bone.
2. a break or rupture in a bone.
depressed fracture , depressed skull fracture fracture of the skull in which a fragment is depressed. de Quervain's fracture fracture of the navicular bone together with a volar luxation of the lunate bone. direct fracture one at the site of injury. dislocation fracture fracture of a bone near an articulation with concomitant dislocation of that joint. Dupuytren's fracture Pott's f. Duverney's fracture fracture of the ilium just below the anterior inferior spine. fissure fracture a crack extending from a surface into, but not through, a long bone. freeze fracture see freeze-fracturing. greenstick fracture one in which one side of a bone is broken, the other being bent. hangman's fracture fracture through the pedicles of the axis (C2) with or without subluxation of the second cervical vertebra or
the third. impacted fracture one in which one fragment is firmly driven into the other. incomplete fracture one which does not entirely destroy the continuity of the bone. insufficiency fracture a stress fracture that occurs during normal stress on a bone of abnormally decreased density. intrauterine fracture fracture of a fetal bone incurred in utero. Jefferson's fracture fracture of the atlas (first cervical vertebra). lead pipe fracture one in which the bone cortex is slightly compressed and bulged on one side with a slight crack on the other
side of the bone. Le Fort fracture bilateral horizontal fracture of the maxilla. Le Fort fractures are classified as follows: Le Fort I f., a horizontal
segmented fracture of the alveolar process of the maxilla, in which the teeth are usually contained in the detached portion of the bone. Le Fort II f., unilateral or bilateral fracture of the maxilla, in which the body of the maxilla is separated from the facial skeleton and the separated portion is pyramidal in shape; the fracture may extend through the body of the maxilla down the midline of the hard palate, through the floor of the orbit, and into the nasal cavity. Le Fort III f., a fracture in which the entire maxilla and of the hard palate, through the floor of the orbit, and into the nasal cavity. Le Fort III f., a fracture in which the entire maxilla and one or more facial bones are completely separated from the craniofacial skelton; such fractures are almost always accompanied by multiple fractures of the facial bones.
Monteggia's fracture one in the proximal half of the shaft of the ulna, with dislocation of the head of the radius. open fracture one in which a wound through the adjacent or overlying soft tissues communicates with the site of the break. parry fracture Monteggia's f. pathologic fracture one due to weakening of the bone structure by pathologic processes, such as neoplasia, osteomalacia, or
osteomyelitis. ping-pong fracture a type of depressed skull fracture usually seen in young children, resembling the indentation that can be
produced with the finger in a ping-pong ball; when elevated it resumes and retains its normal position. Pott's fracture fracture of the lower part of the fibula, with serious injury of the lower tibial articulation, usually a chipping off of a
portion of the medial malleolus, or rupture of the medial ligament. pyramidal fracture (of maxilla) Le Fort II f. sagittal slice fracture fracture of a vertebra breaking it in an oblong direction; the spinal column above is displaced horizontally,
usually causing paraplegia. silver fork fracture Colles' f. simple fracture closed f. Smith's fracture reverse Colles' f. spiral fracture one in which the bone has been twisted apart. spontaneous fracture pathologic f. sprain fracture the separation of a tendon from its insertion, taking with it a piece of bone. Stieda's fracture fracture of the internal condyle of the femur. stress fracture that caused by unusual or repeated stress on a bone.
t f i l f t L F t III f
closed reduction the
The restoration of a body part to its original position after displacement, such as the reduction of a fractured bone by b i i d f b k manipulative reduction
of a fracture without incision.
open reduction reduction of a fracture after incision into the fracture site.
bringing ends or fragments back into original alignment. The use of local or general anesthesia usually accompanies a fracture reduction. If performed by outside manipulation only, the reduction is described as closed; if reduction is described as closed; if surgery is necessary, it is described as open.
4
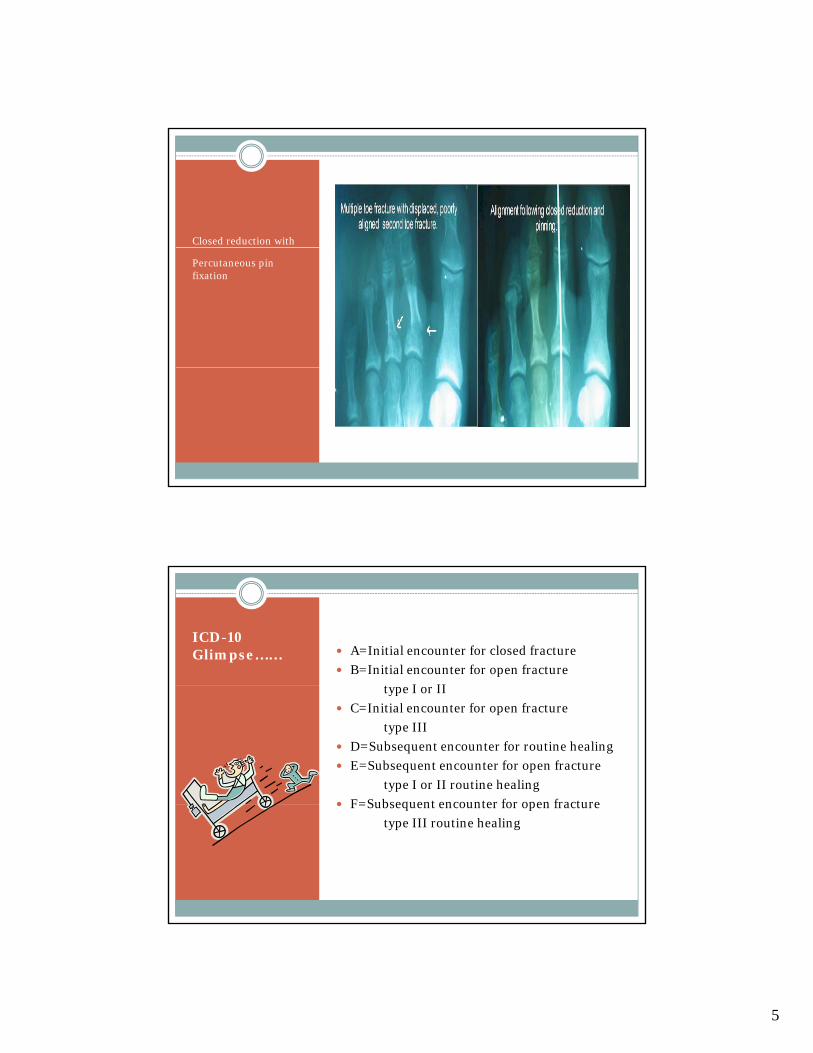
Toe Fracture
Intra-articular
5
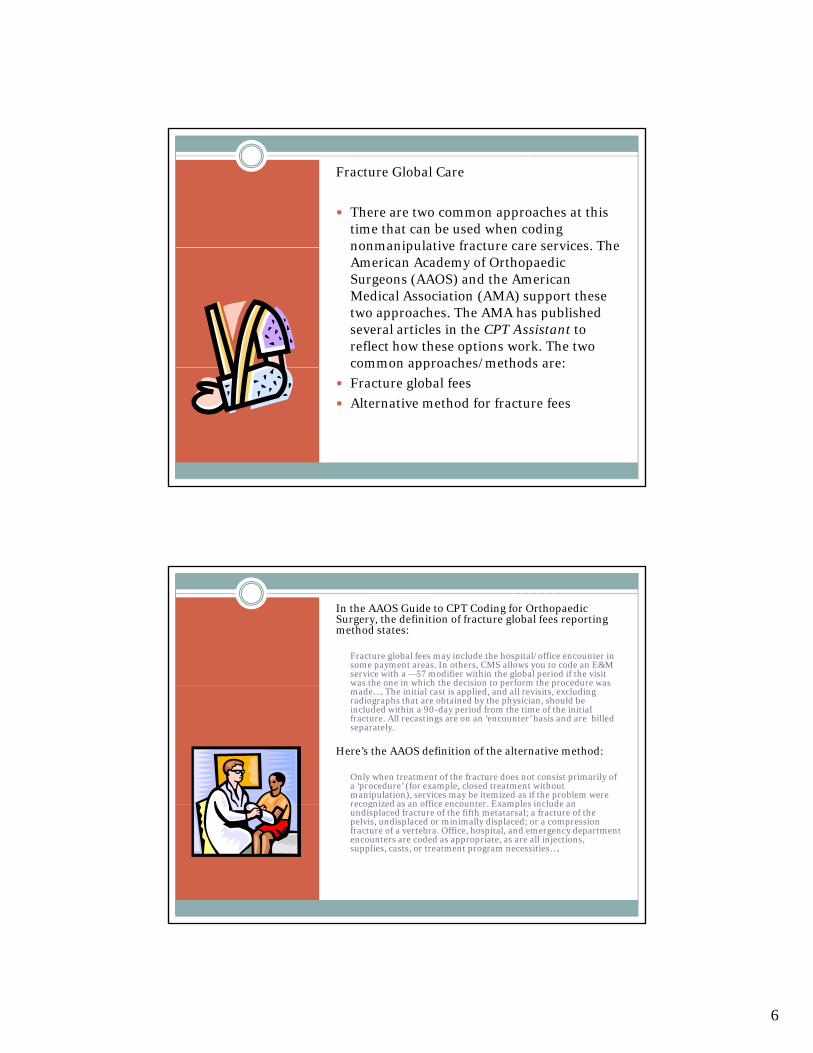
Closed reduction with
Percutaneous pin fixation
ICD-10Glimpse…… A=Initial encounter for closed fracture
B=Initial encounter for open fracture
t I IItype I or II
C=Initial encounter for open fracture
type III
D=Subsequent encounter for routine healing
E=Subsequent encounter for open fracture
type I or II routine healing
F=Subsequent encounter for open fracture F=Subsequent encounter for open fracture
type III routine healing
6
Fracture Global Care
There are two common approaches at this time that can be used when coding nonmanipulative fracture care services The nonmanipulative fracture care services. The American Academy of OrthopaedicSurgeons (AAOS) and the American Medical Association (AMA) support these two approaches. The AMA has published several articles in the CPT Assistant to reflect how these options work. The two common approaches/methods are:common approaches/methods are:
Fracture global fees
Alternative method for fracture fees
In the AAOS Guide to CPT Coding for OrthopaedicSurgery, the definition of fracture global fees reporting method states:
Fracture global fees may include the hospital/office encounter in some payment areas. In others, CMS allows you to code an E&M service with a —57 modifier within the global period if the visit was the one in which the decision to perform the procedure was was the one in which the decision to perform the procedure was made…. The initial cast is applied, and all revisits, excluding radiographs that are obtained by the physician, should be included within a 90-day period from the time of the initial fracture. All recastings are on an ‘encounter’ basis and are billed separately.
Here’s the AAOS definition of the alternative method:
Only when treatment of the fracture does not consist primarily of a ‘procedure’ (for example, closed treatment without manipulation), services may be itemized as if the problem were recognized as an office encounter Examples include an recognized as an office encounter. Examples include an undisplaced fracture of the fifth metatarsal; a fracture of the pelvis, undisplaced or minimally displaced; or a compression fracture of a vertebra. Office, hospital, and emergency department encounters are coded as appropriate, as are all injections, supplies, casts, or treatment program necessities….

7

8
Open Reduction pInternal Fixation with plates and screws
Billing
OV, X-ray, cast application, lisupplies
vs
Global package, 90 day follow-up
No initial cast application.
Good, bad, indifferent?????

9
Business Decision
You need to decide if the RVU value f it i d billi t i h th for itemized billing outweighs the global package.
What if a patient comes into your office with a fractured clavicle. It is not displaced and has good position. The patient is given a position. The patient is given a sling and told to follow up PRN.
What should be charged? Can the office bill fracture care? Why and why not?y

10
Fracture care
S P L I T T I N G F E E S
W H E N S H O U L D I T B E D O N E ?
D O E S I T H A P P E N ?
Physician Reimbursement
Approximately
17% pre-operative
63% operative
20% post-operative

11
Fractured Femur

12
Femoral rod fixation
Question
So what should be done?
The patient was injured on the slopes of Aspen and lives in New Jersey. Has surgery in Aspen, but then goes home. Who should get the $$$$?
What questions on this situation arise? What is the What questions on this situation arise? What is the right thing?
13
ModifiersIf the surgeon knows that the patient is not staying for post-op care. They should apply modifier -54 (surgical care only)
There should be a phone call and or written documentation from the performing surgeon to the orthopedist in a transfer of care
The orthopedist accepting care should bill same surgery code with modifier -55 (post-operative)
CMS 1500
If you are the treating physician and you are billing for pre and intra-operative care you must put the DOS on pre and intra operative care you must put the DOS on the from/to date service line.
If you are billing for transfer of care for fracture care the physician accepting the transfer must put the care…the physician accepting the transfer must put the date seen.

14
Left-Intramedullary rod
Right-plate and screw fixation
15
What if the patient is seen by another physician in your practice during a global period…
Or…
If it was a closed reduction without manipulation, which fee alternative did you use?did you use?
16
References
AAOS Complete Global Service Data for Orthopaedic Surgery 2011
CPT changes 2011 AMA
AMA Category III codes
Video clip “Fractured Fairy Tales, retrieved from youtube
Video clip “Skiing Montague”, retrieved from youtube