foot & ankle examination workshop - · pdf filetalocrural (ankle) joint ... clinical...
TRANSCRIPT

Foot & Ankle
Examination Workshop Morteza Khodaee, MD, MPH, FACSM, FAAFP
Associate Professor
Department of Family Medicine
University of Colorado School of Medicine
July 4, 2013

Objectives
Participants will be able to:
Select the most effective and evidence based
physical examination tests to establish the
diagnosis.
Demonstrate proficiency in a number of
examination techniques, including inspection,
palpation, range of motion, and special tests
Determine when imaging may be needed for an
ankle injury based on the Ottawa foot and
ankle rules.

Anatomy Hindfoot
Inferior Tibiofibular Joint
Syndesmosis type with minimum movement
Ant. & post. inferior tibiofibular, transverse
tibiofibular, and interosseus ligament

Anatomy Hindfoot
Talocrural (Ankle) Joint
Formed by Talus, Med. & Lat Malleoli
Uniaxial and modified hinged type
Plantar flexion to 50° and dorsiflexion to 20°
ATF & PTF, and calcaneofibular lig. laterally
Deltoid lig. medially

Anatomy Hindfoot
Subtalar (Talocalcanean) Joint
Formed by talus, calcaneus, navicular, and
cuboid
Supination 45°-60° and pronation 15°-30°

Anatomy Lateral View

Anatomy Medial View

Anatomy Anterior View

Anatomy Posterior View

Anatomy
Midfoot
Chopart’s Joint
Midtarsal joints
between the talus-
calcaneus and the
navicular-cuboid
Minimum movement

Anatomy
Forefoot Tarsometatarsal (Lisfranc’s)
Joints
Intermetatarsal Joints
Metatarsophalangeal Joints
Toe extension, lateral four toes
(MTP 40°), big toe (MTP 70°)
Toe flexion, lateral four toes
(MTP 40°), big toe (MTP 45°)
Interphalangeal Joints
Toe extension, lateral four toes
(PIP 0°, DIP 30°), big toe (IP 0°)
Toe flexion, lateral four toes (PIP
35°, DIP 60°), big toe (IP 90°)

Evaluation History
Mechanism of Injury
Presence of transient or fixed deformity
of the foot & ankle at the time of injury
Level of activities after the injury

Evaluation History
Swelling or bruising (ecchymosis)
Pain characters (location, intensity, type,
duration, aggravating and alleviating
factors)
History of previous injury

Physical Examination Observation
Lateral View a. Calcaneal apophysitis
(Sever’s)
b. Achilles tendinosis
c. Achilles rupture
d. Retrocalcaneal
bursitis
e. Post. ankle
impingement
f. Calcaneofibular lig
g. Sinus tarsi
h. Ant. talofibular lig
i. Ant. ankle
impingement
j. Avulsion Fx of 5th MT
c

Physical Examination Observation
Medial View e. Tarsal tunnel syndrome
f. Med. ankle sprain
g. Entrapment site 1st branch of
lat. plantar n.
h. Entrapment site of med.
plantar n.
a. Calcaneal apophysitis
(Sever’s)
b. Achilles tendinosis
c. Achilles rupture
d. Retrocalcaneal bursitis
a
b
c
d
e f
g
h
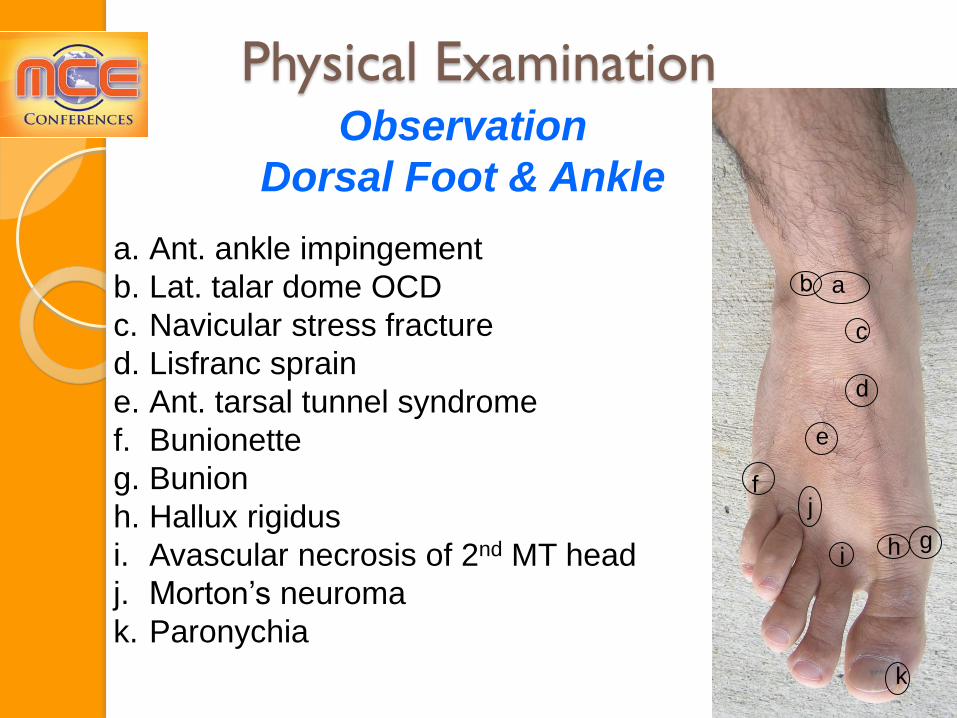
Physical Examination Observation
Dorsal Foot & Ankle
a. Ant. ankle impingement
b. Lat. talar dome OCD
c. Navicular stress fracture
d. Lisfranc sprain
e. Ant. tarsal tunnel syndrome
f. Bunionette
g. Bunion
h. Hallux rigidus
i. Avascular necrosis of 2nd MT head
j. Morton’s neuroma
k. Paronychia
a
e
i
k
j
h
c
f
d
g

Physical Examination Observation
Plantar Foot & Ankle
a.Plantar fat pad
b.Plantar fasciitis
c. Avulsion fracture of the 5th
MT
d.Stress fracture of the 3rd MT
e.Stress fracture of the 2nd MT
f. Sesamoiditis
g.Metatarsalgia
a
f
e d
c
b
g g
g g

Physical
Examination
Observation
Swelling
Ecchymosis

Physical Examination Observation
(Cont’)
Deformities
Ankle Dislocation Ankle ganglion cyst

Physical Examination
Observation
Non-weight-bearing (open-chain)
Weight-bearing (closed-chain)
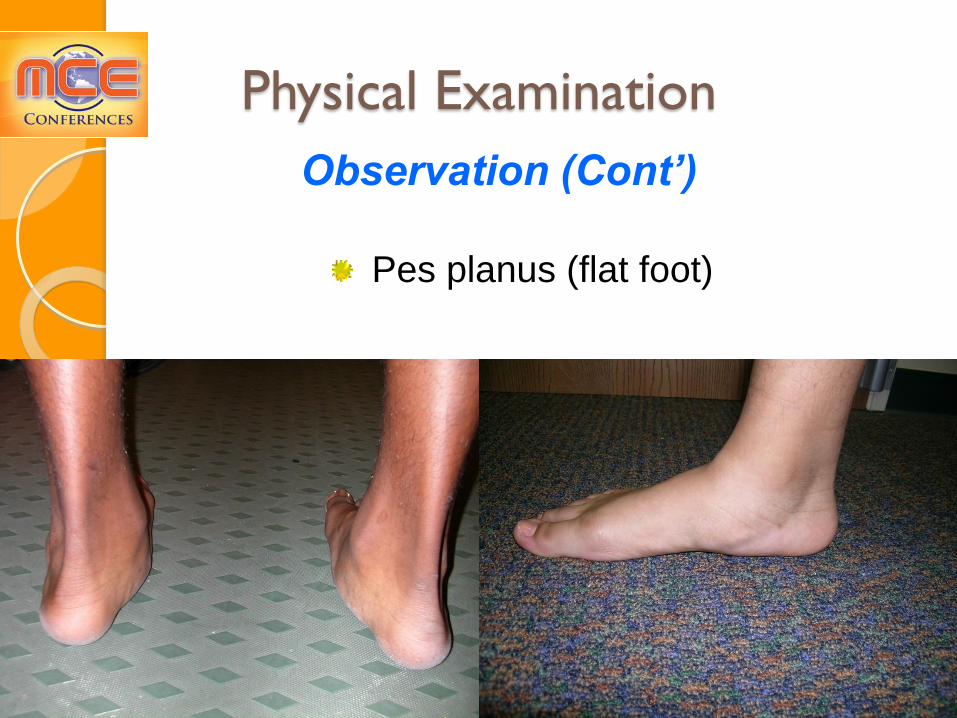
Physical Examination
Observation (Cont’)
Pes planus (flat foot)

Physical Examination
Observation (Cont’) Left Achilles tendon rupture

Physical Examination
Observation (Cont’)
Pes cavus (hollow foot)
Splay foot (broadening of the forefoot)
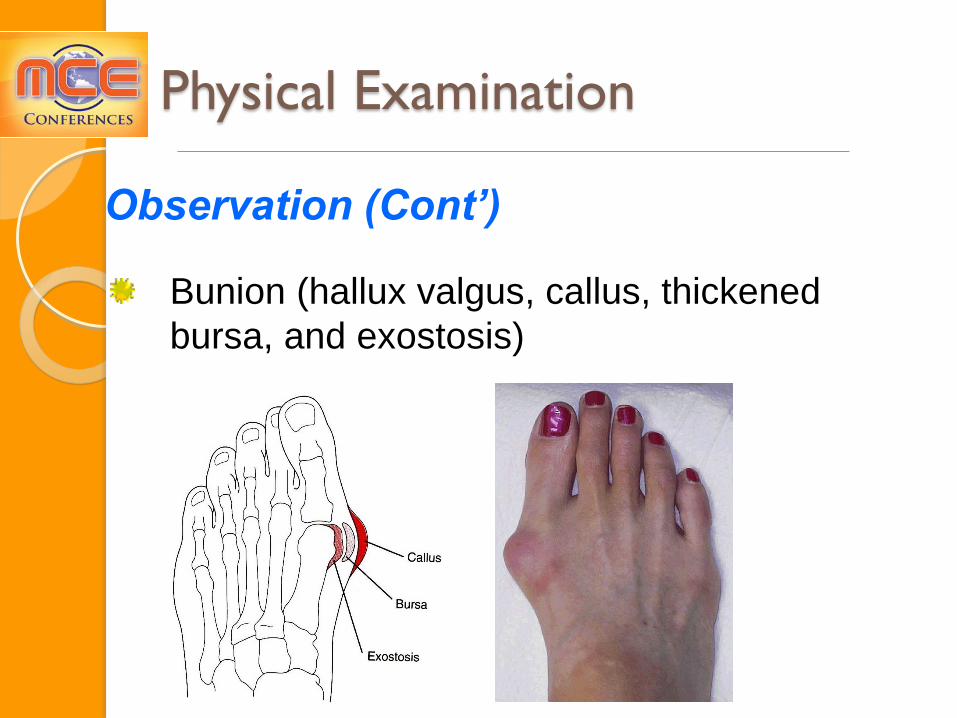
Observation (Cont’)
Bunion (hallux valgus, callus, thickened
bursa, and exostosis)
Physical Examination

Physical Examination
Observation (Cont’)
Bunionette (tailor’s bunion) and Plantar Callus

Observation
(Cont’)
Hallux Rigidus
(stiff big toe)
Mostly due to
osteoarthritis of
1st MTP
Physical Examination
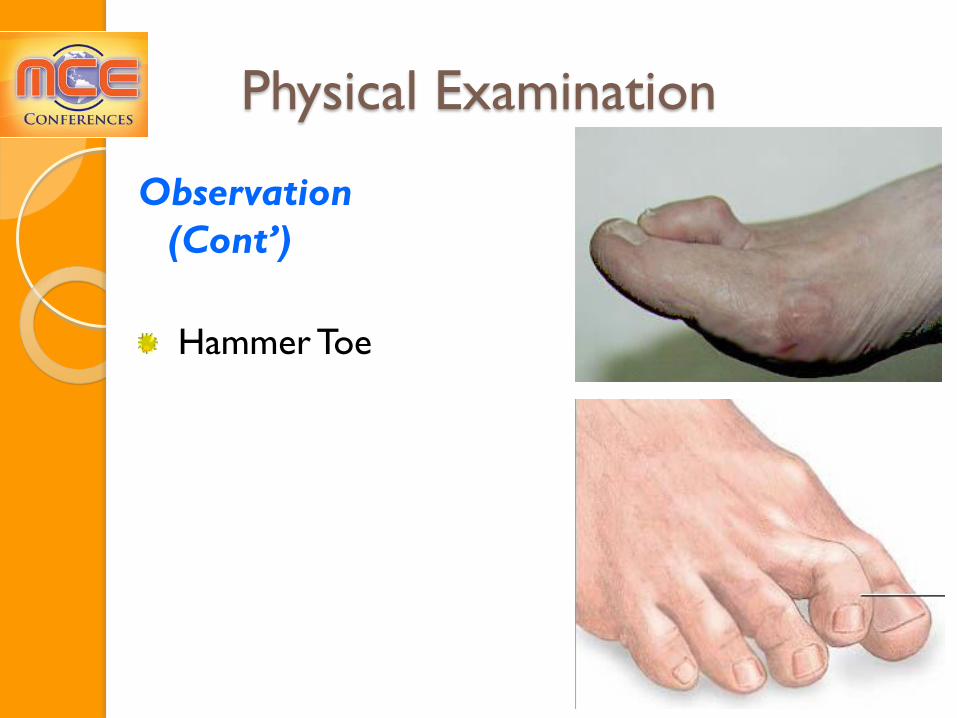
Observation
(Cont’)
Hammer Toe
Physical Examination

Physical Examination Range of Motion (active & passive)
Ankle plantar flexion 50°
Ankle dorsiflexion 20°
Supination 45°-60° (inversion, adduction,
and plantar flexion)
Pronation 15°-30° (eversion, abduction,
and dorsiflexion)
Resisted Isometric Movements
Supination Pronation
Physical Examination Palpation
Medial & lateral malleoli
Medial & lateral ligament complexes
Base of 5th metatarsal
Distal tibiofibuar joint
Talus, calcaneus, navicular, cuneiform,
and cuboid bones
Achilles tendon
Peroneal tendons
Metatersal bones
MTP, PIP, and DIP joints
Neurovascular exam (DP & PT pulses,
cap refill, sensation)

Physical Examination
Special Tests Thompson test for Achilles tendon rupture
Negative
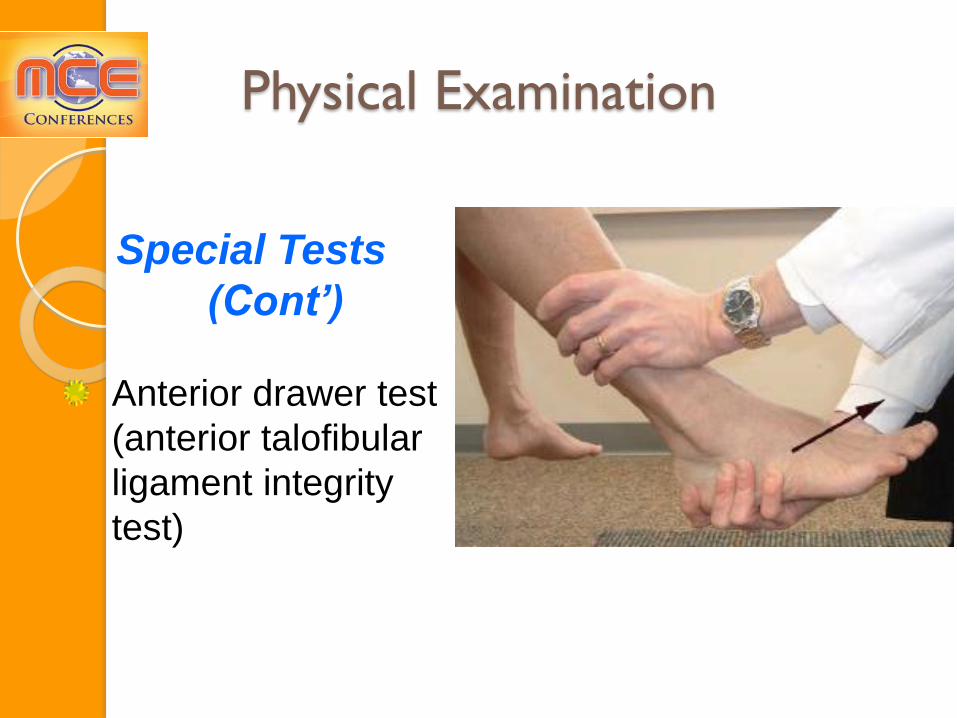
Physical Examination
Special Tests
(Cont’)
Anterior drawer test
(anterior talofibular
ligament integrity
test)
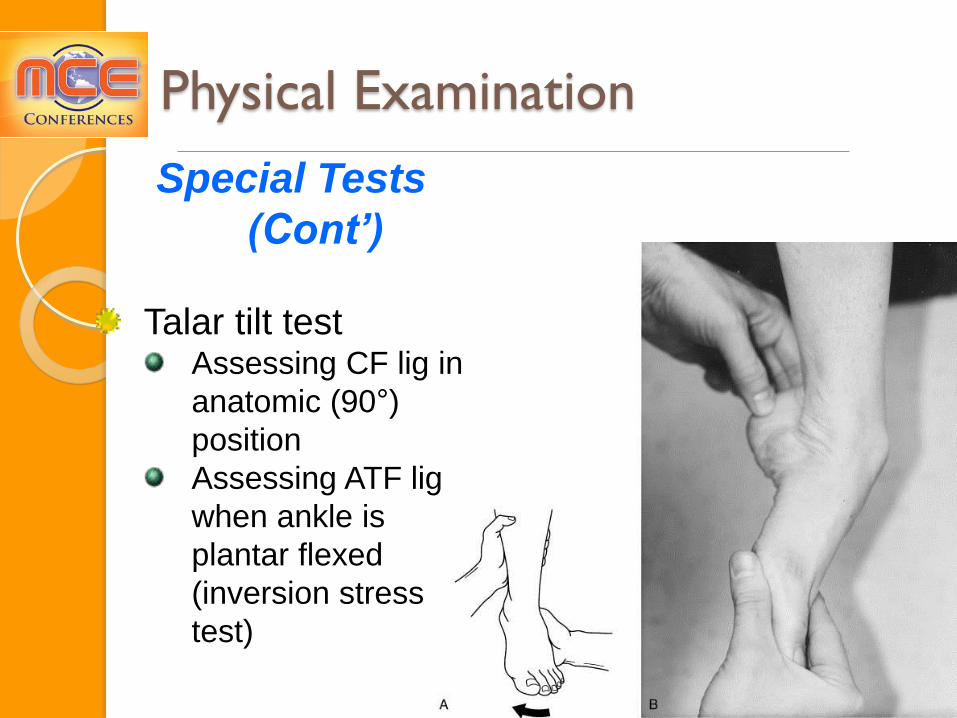
Physical Examination
Special Tests
(Cont’)
Talar tilt test Assessing CF lig in
anatomic (90°)
position
Assessing ATF lig
when ankle is
plantar flexed
(inversion stress
test)

Physical Examination
Special Tests (Cont’)
Squeeze test of the leg (distal
tibiofibular compression test)
for syndesmosis injury positive, if elicits pain over the
distal anterior syndesmosis

Physical Examination
Special Tests (Cont’)
Coronal (side-to-side)
drawer or Cotton test for
syndesmosis injury
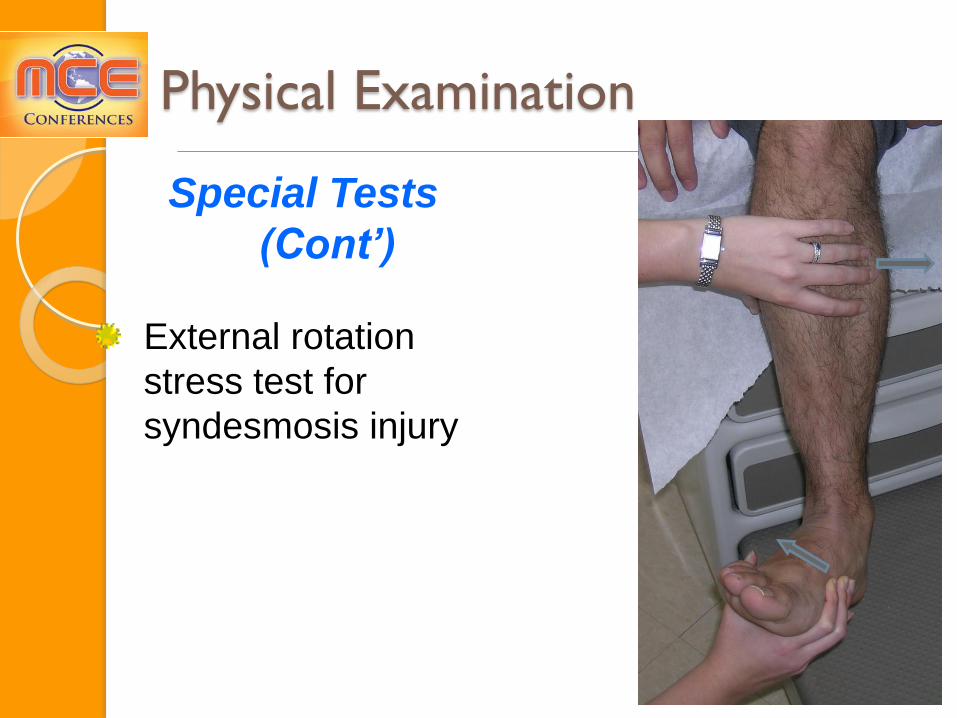
Physical Examination
Special Tests
(Cont’)
External rotation
stress test for
syndesmosis injury
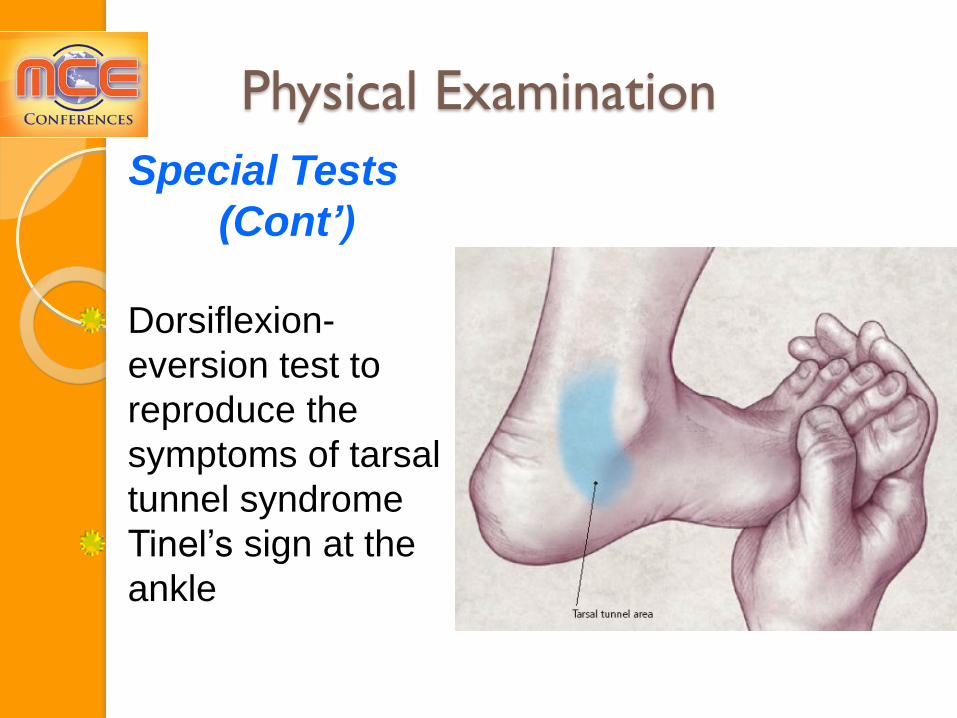
Physical Examination
Special Tests
(Cont’)
Dorsiflexion-
eversion test to
reproduce the
symptoms of tarsal
tunnel syndrome
Tinel’s sign at the
ankle
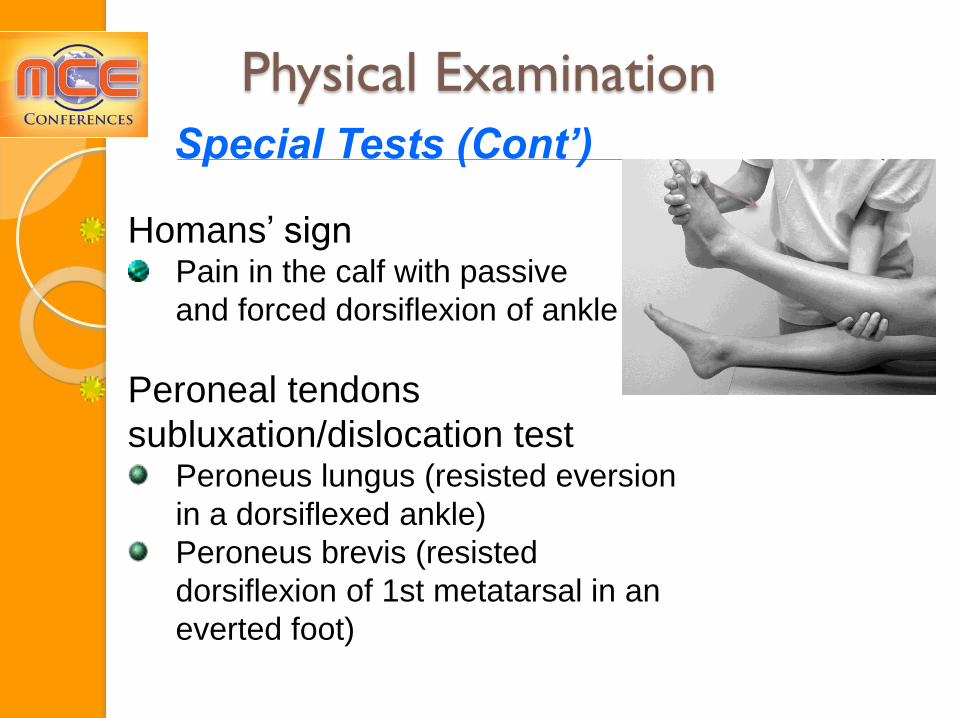
Physical Examination
Special Tests (Cont’)
Homans’ sign Pain in the calf with passive
and forced dorsiflexion of ankle
Peroneal tendons
subluxation/dislocation test Peroneus lungus (resisted eversion
in a dorsiflexed ankle)
Peroneus brevis (resisted
dorsiflexion of 1st metatarsal in an
everted foot)

Diagnostic
Imaging Plain Film
Radiography
Anteroposterior view
Medial tibiofibular clear
space (between the
fibula and the peroneal
incisura of the tibia)
normally <4 mm
Tibiofibular overlap <6
mm is abnormal

Diagnostic Imaging
Plain Film Radiography
Mortise (internal oblique
15°-30°) view
Tibiofibular overlap <1
mm is abnormal
Uniform 3–4 mm space
around the talus (space
between the talar
margin and medial and
lateral malleolus)

Diagnostic
Imaging
Plain Film
Radiography
Lateral View
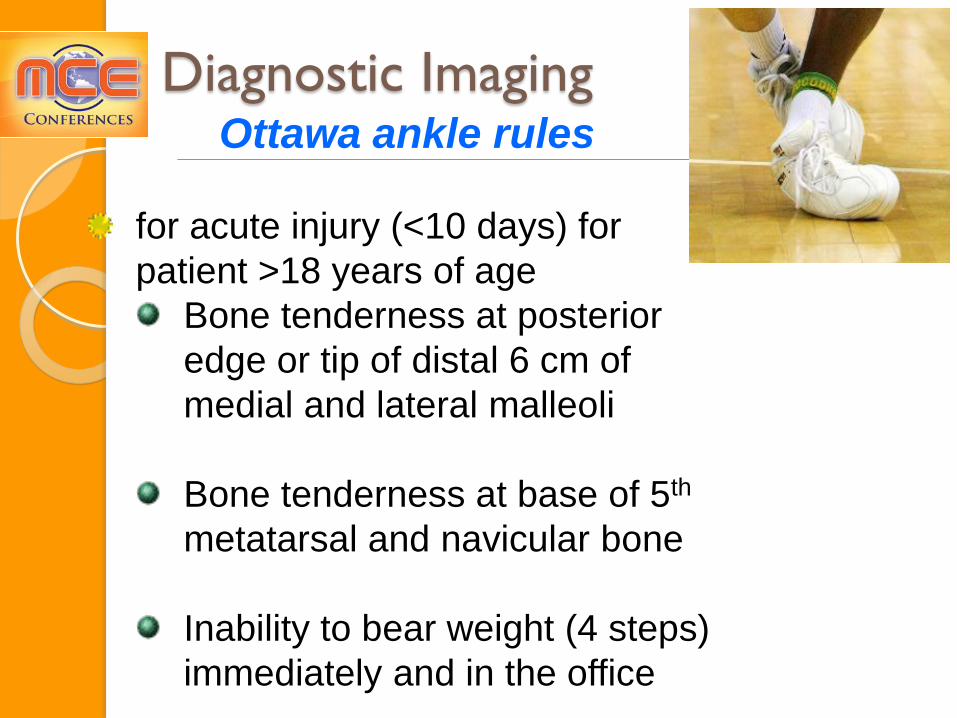
Diagnostic Imaging Ottawa ankle rules
for acute injury (<10 days) for
patient >18 years of age
Bone tenderness at posterior
edge or tip of distal 6 cm of
medial and lateral malleoli
Bone tenderness at base of 5th
metatarsal and navicular bone
Inability to bear weight (4 steps)
immediately and in the office

Case # 1
HPI:
A 33 yo ♀ presents for a 5 year Hx of L 4th toe pain. Pain has been getting worse in the last few ms. S/P NSVD 4 ms ago. She started 4-5 miles/wk running since 3wks ago. Pain radiates up to her metatarsal and down to her 3rd-4th toes. She has numbness and tingling which goes away 10 minutes after running. Tennis shoes makes the symptoms worse. Barefoot walking does not aggravate the symptoms.
42

Case # 1 Con’t
PSH: R partial meniscectomy 1997
ØPMH, ØSH, ØFH, ØMeds
PE: Mild B genu varum. Mild tenderness in
the head of L 4th metatarsal and the area
between the 3rd and 4th metatarsal. Normal
ROM. Squeeze test cause tingling and
numbness in her 4th toe.
43

Case # 1 Con’t
44
Imaging:
– X-ray (AP, obl)
Os Peroneum
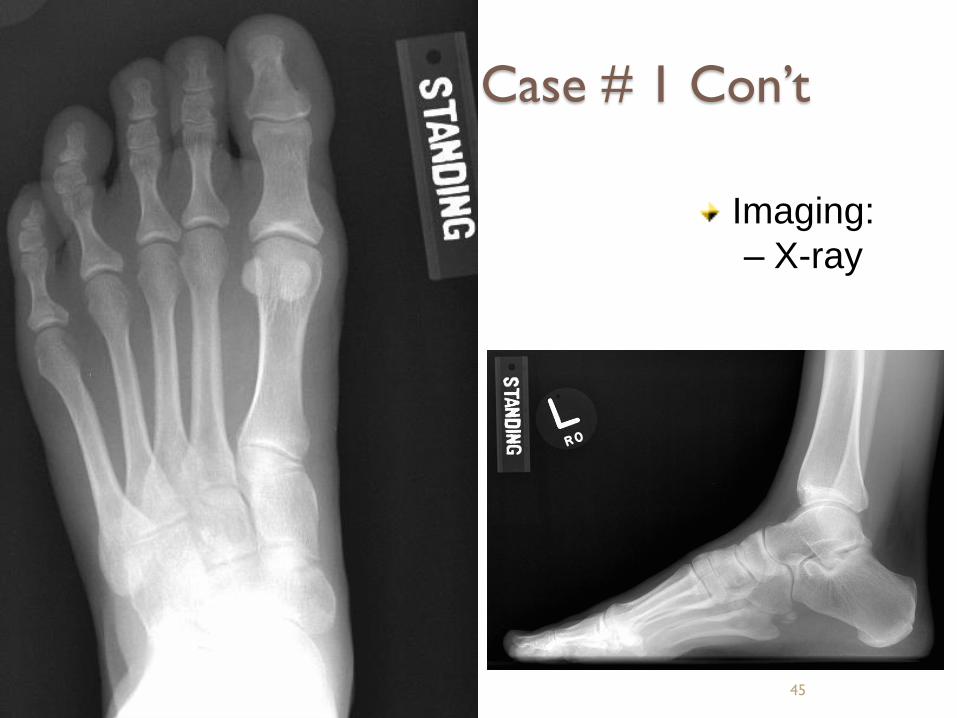
Case # 1 Con’t
45
Imaging:
– X-ray
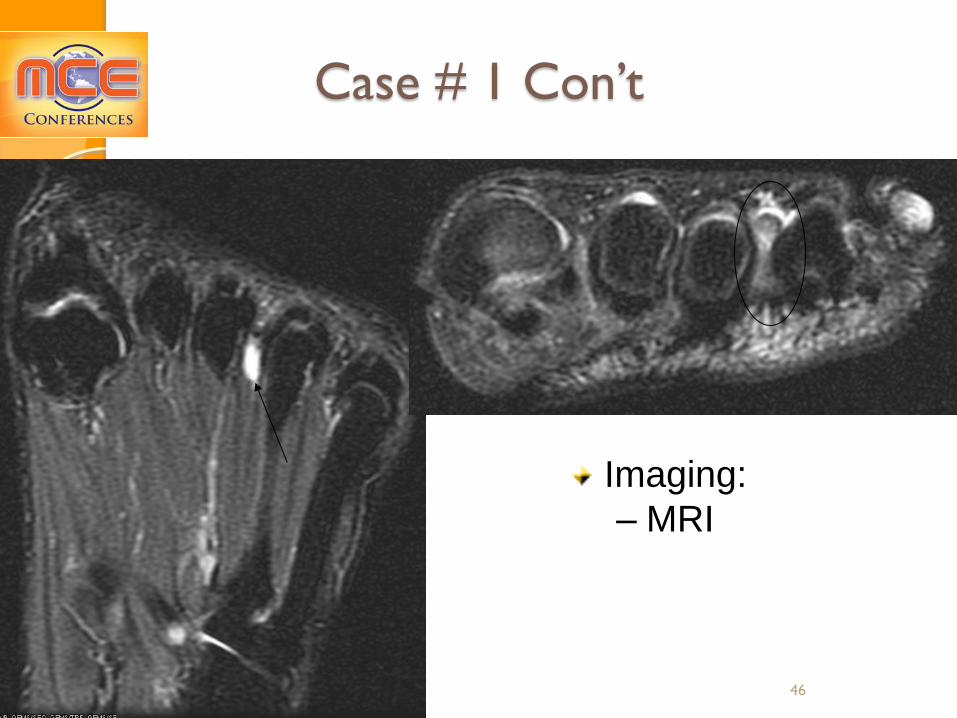
Case # 1 Con’t
46
Imaging:
– MRI

Case # 1
Con’t
47
Imaging:
– MRI

Morton Neuroma
Interdigital neuroma
Common condition that involves enlargement of the interdigital nerve of the foot
Most commonly 3rd intermetatarsal space
Pathophysiology: controversial
is not a nerve tumor
no inflammatory cells or cystic components
Compression, ischemia, or intermetatarsal bursits
48
Morton Neuroma
DDx: Metatarsal stress Fx, tendon sheath ganglion, foreign body reaction, nerve sheath tumor, strain of the plantar capsule, Freiberg’s disease (infarction), and capsulitis or bursitis at the level of the plantar MTPJ
Tx: Metatarsal pad, appropriate shoes (wide toe box, adequate cushioning, and heels ≤ 1-2 cm), cortisone injection, and surgery (distal nerve excision and intermetatarsal ligament release)
49

Case # 2
Hx:
HPI: A 42 yo ♂ presents for a wk Hx of L
midfoot pain. He has been running 3-4 miles 5
times a week for the last 6 years. Pain is
worse with running. Pain starts at the
beginning of his run. He has been using the
same brand of running shoes. He mainly runs
outside.
ØPMH, ØPSH, ØFH, ØSH
PE:
Mild-Mod L 3rd dorsal metatarsal tenderness.
50

Imaging:
X-ray: AP
51
Case # 2 Con’t

Case # 2 Con’t
Imaging:
X-ray: oblique
52
Case # 2 Con’t
Dx: Distal L 3rd metatarsal stress Fx
Tx:
Eliminate running and jumping, ↓walking
Non-pain producing and non-wt bearing
activities (swimming, biking) would be ok
Crutches with partial wt-bearing may be
necessary if routine walking is painful
Some cases would need a short-leg walking
cast with advance to hard sole shoe 53

Case # 2 Con’t
Imaging:
X-ray 4 ½ wks later (AP)
54

Case # 2 Con’t
Imaging:
X-ray 4 ½ wks
later (oblique)
55

Case # 2 Con’t
Imaging:
MRI 7 wks later
56

References
• Young CC, Niedfeldt MW, Morris GA, Eerkes KJ. Clinical examination of the
foot and ankle. Prim Care. 2005 Mar;32(1):105-32
• Saleh A, Sadeghpour R, Munyak J. Foot and ankle update. Prim Care.
2013 Jun;40(2):383-406.
• Wrobel JS, Armstrong DG. Reliability and validity of current physical
examination techniques of the foot and ankle. J Am Podiatr Med Assoc.
2008 May-Jun;98(3):197-206
• Pommering TL, Kluchurosky L, Hall SL. Ankle and foot injuries in pediatric
and adult athletes. Prim Care. 2005 Mar;32(1):133-61
• David J. Magee. (2002). Orthopedic Physical Assessment (4th ed.).
Elsevier Sciences (USA)
• Wolfe MW, Uhl TL, Mattacola CG, McCluskey LC. Management of ankle
sprains. Am Fam Physician. 2001 Jan 1;63(1):93-104
• Henry Gray. Gray's Anatomy of the Human Body
• Aldridge T. Diagnosing heel pain in adults.
Am Fam Physician. 2004 Jul 15;70(2):332-8
• Tu P, Bytomski JR. Diagnosis of heel pain. Am Fam Physician. 2011 Oct
15;84(8):909-16