five best practices when prescribing opioids - … · o morphine ir 15-30 mg po every 4-6 hours prn...
TRANSCRIPT

First Do No Harm: Five Best Practices When You Prescribe Opioids
Rebekah Gardner, MD, FACP
Kate Mavrich, MD
Sarita Warrier, MD, FACP

Disclosures
• None

Learning Objectives
• Define universal precautions for prescribing opioids
• Identify the value of and tools for risk assessment
• Describe the main components of treatment agreements
• Identify an appropriate formulary
• Integrate urine toxicology screens into your practice

The Scope

National Vital Statistics System, 1999-2008; Automation of Reports and Consolidated Orders System (ARCOS) of the
Drug Enforcement Administration (DEA), 1999-2010; Treatment Episode Data Set, 1999-2009
Prescription Opioid Sales, Deaths and Treatment: 1999-2010
Sarah Bagley, MD, Addiction Medicine Fellow, Boston University

http://www.providencejournal.com/topics/special-reports/overdosed/

7
Drug overdose deaths outnumbered motor vehicle traffic deaths in 10 states in 2005
CDC NVSS, MCOD. 2010
More deaths from drug overdose
Sarah Bagley, MD, Addiction Medicine Fellow, Boston University

8
By 2010, drug overdose deaths outnumbered motor vehicle traffic deaths in 31 states
CDC NVSS, MCOD. 2010
More deaths from drug overdose
Sarah Bagley, MD, Addiction Medicine Fellow, Boston University

http://www.providencejournal.com/topics/special-reports/overdosed/


The 5 Best Practices
1. Use a universal precautions approach
2. Assess potential risks before prescribing
3. Use treatment agreements
4. Create a formulary
5. Use urine toxicology screens

UNIVERSAL PRECAUTIONS

When prescribing opioids, what does “universal precautions” refer to?
A. Isolating patients who require opioids from the rest
of your patients.
B. Treating each individual patient who needs opioids differently.
C. Identifying the cause for the pain syndrome, along with risks and benefits of treatment with opioids… every time you prescribe.
D. Gloving up before writing a prescription.

Universal Precautions
• Same process, every time
• Frame the encounter
– What is the medical condition we are treating?
– What are the risks and benefits of prescribing opioids?
Alford DP. Chronic back pain with possible prescription opioid misuse. JAMA 2013; 309: 919-925. Zacharoff KL. A systematic approach to the use of opioids in the treatment of chronic pain. https://www.Pain EDU.org.

http://www.health.ri.gov/healthcare/medicine/about/safeopioidprescribing/

http://www.health.ri.gov/healthcare/medicine/about/safeopioidprescribing/

RISK ASSESSMENT

Risk Assessment
• Risk factors for overdose
• Opioid risk tools

Risk Factors: Overdose

Risk Factors
• High dose per 24 hours (≥ 50-100 mg of morphine or equivalent)

Risk Factors
• High dose per 24 hours (≥ 50-100 mg of morphine or equivalent)
• Comorbid substance use disorder
• Depression or other mental health disorder
• Sedative-hypnotic use

Tools for Assessing Pain and Risk
• PEG
• AUDIT-C
• SOAPP
• Miscellaneous drug and alcohol screens – Single-item screener – NIDA Quick Screen – Family history

Tools for Mental Health Screening
• PHQ-2 or PHQ-2
• GAD-2 or GAD-7
• Primary Care PTSD Screen

TREATMENT AGREEMENTS

Which of the following is TRUE about treatment agreements?
A. They are legally binding documents.
B. Most allow several prescribers as long as the patient uses one pharmacy.
C. It is important to avoid the word “addiction” in the agreements because patients can be frightened by this.
D. They include information about what behavior might lead to discontinuation.

Rationale
• Provide a road map for physicians and patients
• Facilitate key communication
• Set expectations and obligations
• Identify responsibilities
• Outline plan for monitoring


Common Elements
Agreement between specific physician and patient
Acknowledgment that opioid unlikely to eliminate pain
One prescriber
One pharmacy
Review of risks and side effects
1

Common Elements
Instruction to take as prescribed or call doctor if change needed
No early refills
No off-hours refills
Avoidance of alcohol, benzos, illicits
Storage in a safe place
2

Common Elements
Attendance at all follow-ups
Cannot give or sell medication
Random urine drug testing
Treatment trial, not a binding contract
Consequences for not following agreement
3



Which of the following is TRUE about treatment agreements?
A. They are legally binding documents.
B. Most allow several prescribers as long as the patient uses one pharmacy.
C. It is important to avoid the word “addiction” in the agreements because patients can be frightened by this.
D. They include information about what behavior might lead to discontinuation.

FORMULARY

Which medication is NOT a good option for chronic pain treatment?
A. Acetaminophen with codeine
B. Meloxicam
C. Morphine sustained release
D. Gabapentin

Acute Pain
o Acetaminophen 325-650 mg PO every 4 hours prn
o Ibuprofen 200-800 mg PO 3-4 times daily
o Naproxen 250-500 mg PO twice daily
o Oxycodone 5-10 mg PO every 4-6 hours prn
o Morphine IR 15-30 mg PO every 4-6 hours prn

Episodic Pain [ unresponsive to non-opioids ]
o Oxycodone 5-10 mg PO every 4-6 hours prn
o Morphine IR 15-30 mg PO every 4-6 hours prn
o Oxycodone or morphine IR + acetaminophen 325-650 mg PO every 6 hours

Chronic Pain
o Ibuprofen 200-800 mg PO 3-4 times daily
o Naproxen 250-500 mg PO twice daily
o Meloxicam 7.5-15 mg PO daily
o Morphine SR 15-30 mg PO every 8-12 hours

What’s Missing?
o OxyContin®
o Dilaudid®
o Percocet®
o Vicodin®
o Tramadol

Methadone
o Effective pain med
o Long half life fewer highs and lows
o Inexpensive
o QT prolongation
o Long half life caution up-titrating
o Stigma

Adjunctive Therapies
o Gabapentin 300 mg PO at bedtime; may titrate to 600 mg three times daily
o Pregabalin 50-100 mg PO three times daily
o Amitriptyline 25-50 mg PO at bedtime daily
o Venlafaxine 37.5-150 mg PO daily
o Duloxetine 20-60 mg PO daily
Topical Therapies
o Lidocaine patch or gel
o Capsaicin patch or cream
o Diclofenac cream
o Heat and cold
“No appointment necessary.”

Which medication is NOT a good option for chronic pain treatment?
A. Acetaminophen with codeine
B. Meloxicam
C. Morphine sustained release
D. Gabapentin

URINE TOXICOLOGY SCREENING

Urine Toxicology Screening
• Understanding your lab
• Interpreting results
• Discussing with patients

Clinical Vignette
• 83-year-old woman
• Severe spinal stenosis
• Taking Tylenol #3® (acetaminophen with codeine) 1XD prn and hs
• What are the expected results of her urine drug screen?

Clinical Vignette
• Urine toxicology reveals the presence of codeine, morphine, and hydromorphone
• Is this an expected or unexpected result?
• Are the results appropriate or inappropriate?
Types of Urine Drug Testing
• Screening: enzyme-based immunoassay
– Fast and cheap, but…
– A little tricky
• Confirmatory testing: gas (or liquid) chromatography and/or mass spectrometry
– Slow and expensive, but…
– Highly sensitive and specific

Interpreting the Results: Urine Drug Testing HPI
• Last dose?
• How much?
• Any other pain medicine?
• Any other drugs?

Drugs of Abuse Screen
• Amphetamines • Barbiturates • Benzodiazepines • Cannabinoids • Cocaine • Methadone • Opiates • Oxycodone/oxymorphone • Phencyclidine • Propoxyphene

Drugs of Abuse Screen
• Amphetamines • Barbiturates • Benzodiazepines • Cannabinoids • Cocaine • Methadone • Opiates • Oxycodone/oxymorphone • Phencyclidine • Propoxyphene

Unexpectedly Negative
• False negative – Fast-metabolizer
– Last dose too long ago
• Lab error
• Diversion or deception
• Order confirmatory testing

Unexpectedly Positive
• False positive
• Metabolites
• Lab error
• Sample contamination

Opioid Metabolism Basics
• Active and inactive metabolites
• Drug-drug interactions
• Some opioids produce metabolites chemically identical to other opioid medications
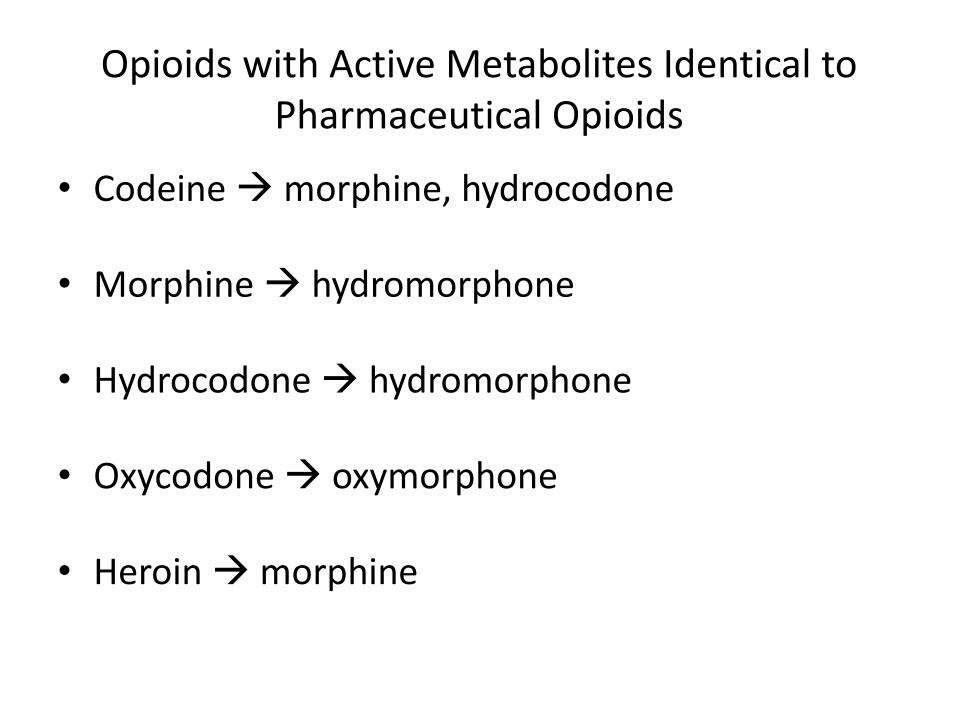
Opioids with Active Metabolites Identical to Pharmaceutical Opioids
• Codeine morphine, hydrocodone
• Morphine hydromorphone
• Hydrocodone hydromorphone
• Oxycodone oxymorphone • Heroin morphine

Back to the Clinical Vignette
• Prescribed Tylenol #3® (acetaminophen with codeine)
• Tested positive for codeine, morphine, and hydromorphone
– Expected or unexpected?
– Appropriate or inappropriate?

Language For Introducing Drug Testing
• As part of treating [pain] with medications like [X], I order urine tests to get more information about how safe they are for my patients.
• The test measures a number of medications and drugs that could interfere with your treatment.
• This is something that I do with all patients on these medications.
• If I find something unexpected, we’ll talk about it and work together to address it.

PUTTING IT TOGETHER

THE MULTIDISCIPLINARY PAIN COMMITTEE
Goals
Development/Recruitment
Members
Practices
Goals
• Resident education/support
• Safe prescribing practices
• Monitoring
• Connection to resources

Development/Recruitment
• Initially funded by hospital-based risk management grant
• Recruitment of members
• Policy development

Members
• Internal medicine clinic providers (attending physicians, nurse practitioners, residents)
• Clinical social worker
• Substance abuse social worker
• Psychiatry nurse practitioner
• Clinical pharmacist with pain management background

Reasons to Refer
• Age< 40
• History of substance use
• Unclear pain disorder
• Opioid use >50mg morphine daily
• Concerned? Uncomfortable? Refer!

Ongoing Practices
• Monthly meetings
• Review of chart/imaging/outside records/urine toxicology results
• Review prescription monitoring program
• Documentation of recommendations
• Communication with providers


Challenges
• Communicating with emergency department and other disciplines
• Electronic health record
• Physician familiarity with prescribing policies
• Legacy regimens

Opportunities

The EHR
• Alert pop-ups
• Built-in risk assessment tools
• Checkbox in/near medication list
• Order sets for pain management
• Treatment agreement in EHR
• Agree on an ICD code

Summary
• Use the same process (identify pain syndrome, discuss risks and benefits) every time you prescribe opioids for chronic pain.
• Assess risks for misuse.
• Use a treatment agreement.
• Identify an appropriate formulary for your practice.
• Integrate urine toxicology screens into your prescribing patterns.
