first two and half year of national screening program for colorectal cancers in republic croatia...
TRANSCRIPT

FIRST FIRST TWO AND HALF YEARTWO AND HALF YEAR OF NATIONAL SCREENING OF NATIONAL SCREENING PROGRAM FOR COLORECTAL CANCERS IN PROGRAM FOR COLORECTAL CANCERS IN REPUBLIC REPUBLIC CROATIACROATIA
Miroslava KaticicMiroslava Katicic11, , Milan KujundzicMilan Kujundzic22, , Davor StimacDavor Stimac33, , Marija StrnadMarija Strnad44, , Danica KramaricDanica Kramaric44, , Valerija StamenicValerija Stamenic44, , Nataša AntoljakNataša Antoljak55, , Mirko SamijaMirko Samija66, ,
11University Hospital Merkur, Zagreb, CroatiaUniversity Hospital Merkur, Zagreb, Croatia22University Hospital Dubrava, Zagreb, CroatiaUniversity Hospital Dubrava, Zagreb, Croatia33University Center Rijeka, CroatiaUniversity Center Rijeka, Croatia44Ministry of Health and Social Welfere, Zagreb, CroatiaMinistry of Health and Social Welfere, Zagreb, Croatia55Croatian National Insitute of Public Health, Zagreb, CroatiaCroatian National Insitute of Public Health, Zagreb, Croatia66University Hospital for tumors, Zagreb, Croatia University Hospital for tumors, Zagreb, Croatia

• Average rates of CRC incidence and mortality in Croatia are Average rates of CRC incidence and mortality in Croatia are parallel to those in developed countries with unfortunately parallel to those in developed countries with unfortunately clear increase in incidence rate during the last 30 ys, for 364 clear increase in incidence rate during the last 30 ys, for 364 percent from 1970 till 2004. percent from 1970 till 2004.
Background (I)
What makes the situation in Croatia even worse in What makes the situation in Croatia even worse in comparison to developed countries, is comparison to developed countries, is
the high mortality ratethe high mortality rate, ,
steadily reaching 60–70% of incidence rate. steadily reaching 60–70% of incidence rate.

Fig. 1. DIGESTIVE ORGAN CANCER INCIDENCE, 1970-2003- Share in
total incidence 28%
0
10
20
30
40
50
60
70
1970 1975 1980 1985 1990 1995 2000 2003
Year
Cru
de
ra
te p
er
10
0 0
00
OESOPHAGUS
VENTRICULUS
COLON & RECTUM
HEPAR (PRIM. ET NON SPEC.)
VESICA FELLEA
PANCREAS
Croatian National Institute of Public Health Prof. Croatian National Institute of Public Health Prof. Marija StrnadMarija Strnad, M.D., , M.D., Ph.D. Ph.D.
+C-433%
+R-329%
-23%
+183%
+10%
+151%
+77%
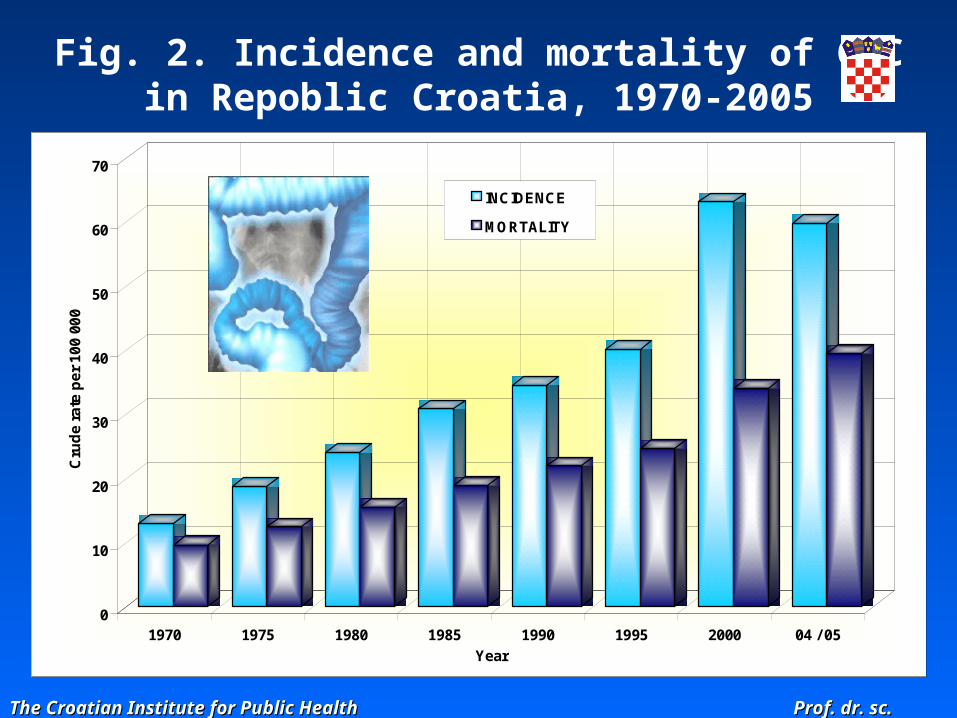
Fig. 2. Incidence and mortality of CRCin Repoblic Croatia, 1970-2005
The Croatian Institute for Public Health Prof. dr. sc. Marija Strnad The Croatian Institute for Public Health Prof. dr. sc. Marija Strnad
0
10
20
30
40
50
60
70
Cru
de
rate
pe
r 10
0 00
0
1970 1975 1980 1985 1990 1995 2000 04 / 05
Year
INCIDENCE
MORTALITY
Background (II)
• The incidence rate CRC/100 000 inhabitants The incidence rate CRC/100 000 inhabitants
65/100 000 (2005),65/100 000 (2005),
• The mortality rate The mortality rate
40.6/100 000 (2006) 40.6/100 000 (2006)
• Incidence increases rapidly for the group aged 60 and older. Incidence increases rapidly for the group aged 60 and older.
Main reason: the most cases of cancer are detectedMain reason: the most cases of cancer are detected too late at an too late at an advanced stage with poor prognosisadvanced stage with poor prognosis
Less than 10% of CRC are limited to bowel wall in the time of Less than 10% of CRC are limited to bowel wall in the time of diagnosis.diagnosis.
Five-years relative survival is only 49% for men and 50% for Five-years relative survival is only 49% for men and 50% for women.women.

Aim
National screening program for colorectal cancers started in National screening program for colorectal cancers started in September 2007.September 2007.
Campaign targets:Campaign targets:
1.1. Reducing colorectal cancer mortality Reducing colorectal cancer mortality
2.2. Cancer detection; Cancer detection;
3.3. Detection and cure all precancerous colorectal lesions; Detection and cure all precancerous colorectal lesions;
4.4. Detection of other colorectal diseases characterized by occult Detection of other colorectal diseases characterized by occult bleeding; bleeding;
5.5. Compliance of 60%.Compliance of 60%.
Study population:Study population: all inhabitants of Republic Croatia aged 50 – 75 who all inhabitants of Republic Croatia aged 50 – 75 who are at an average risk for CRC. are at an average risk for CRC.

PUBLIC HEALTH INSTITUTE COLONOSCOPYPATHOLOGY
(PHD)
CROATIAN PUBLIC HEALTH INSTITUTE
MINISTRY OF HEALTH AND WELFARE
GENERAL PHYSICIAN
MALE AND FEMALE AT AGE 50-74 YRS.
Croatian model for CRC screening

Croatian National program for CRC screening was established by Ministry of Health and Social Welfare and has been implemented since the September 2007.
MINISTRY OF HEALTH AND WELFARE
1.

The network of coordinators in each county institute of public health are obliged to ensure performing of fecal occult blood testing (FOBT.) The FOBT is performed by guaiac-based Hemognost card test with detection limit of 0.2 ml blood in 500 g of stool.
PUBLIC HEALTH INSTITUTE
CROATIAN PUBLIC HEALTH INSTITUTE
2.

Test and short questionnaire are delivered to home address of all citizens age 50–74 consecutively during two years. Each participant has to fulfill the questionnaire, and send it together with test specimen back to the institute for further analysis.
MALE AND FEMALE AT AGE 50-74 YRS.
3.

Colonoscopy will be offered and organised for all Colonoscopy will be offered and organised for all FOBT- positive persons. FOBT- positive persons.
COLONOSCOPYPATHOLOGY
(PHD)
4.

Methods
Anticipated numeric data of campaign: Anticipated numeric data of campaign:
Total Croatian inhabitants - 4 Total Croatian inhabitants - 4 600 000; 600 000;
aged 50aged 50–74 - 1 200 000. –74 - 1 200 000.
According screening results of other authors, it was expected According screening results of other authors, it was expected that 4% FOBT positive cases would be found in normal risk that 4% FOBT positive cases would be found in normal risk population and model calculations pointed out a need for population and model calculations pointed out a need for 24000 colonoscopies per year.24000 colonoscopies per year.

From study will be excluded patients with:From study will be excluded patients with:
already known CRCalready known CRC
other tumours spread to the colorectumother tumours spread to the colorectum
benigne tumours such as lipoma, fibroma, benigne tumours such as lipoma, fibroma,
haemangioma...haemangioma...
already detected polyps who had undergone already detected polyps who had undergone
polypectomy and who are under regular follow-uppolypectomy and who are under regular follow-up

Results
Distributed Distributed (since September 2007.)(since September 2007.) letters letters
(epidemiological questioner, FOBT tester)(epidemiological questioner, FOBT tester) 307.206307.206
Returned Returned 23,3%23,3% 10,2 – 36,8 10,2 – 36,8%%
Positive FOBT Positive FOBT 9,1% 9,1% 3,8 – 29,9% 3,8 – 29,9%
ColonoscopyColonoscopy
already donealready done 2651 (compliance 70,3%)2651 (compliance 70,3%)

23,3%23,3%
34,7%34,7%28,9%28,9%
16,0%16,0%
25,8%25,8%
16,8%16,8%25,1%25,1%31,2%31,2%
30,0%30,0%
36,8%36,8%
10,2%10,2%
23,4%23,4% 22,2%22,2%
28,1%28,1%25,0%25,0%
20,9%20,9%
22,1%22,1%
20,0%20,0%
29,0%29,0%
26,0%26,0%
23,7%23,7%
Fig. 3. Number of rFig. 3. Number of returned eturned FOBT FOBT from different countiesfrom different counties

Colonoscopy findings (Preliminary report)Colonoscopy findings (Preliminary report)
Normal Normal 564 (21,3%) 564 (21,3%) 10 10 – – 4242%%
Noduli haemorrh.Noduli haemorrh. 477 (17,8%) 477 (17,8%) 14 – 32% 14 – 32%
DiverticulosisDiverticulosis 318 (12,1) 318 (12,1) 8 – 34% 8 – 34%
PolypsPolyps 928 (34,2%)928 (34,2%) 23 – 60% 23 – 60%
CancersCancers 182 (4,1%)182 (4,1%) 2 – 2 – 12%12%

Characteristics of Croatian campaign in Characteristics of Croatian campaign in first yearfirst year::
low percentage of returned FOBTlow percentage of returned FOBT
high number of pathologic findings (polyps and cancers)high number of pathologic findings (polyps and cancers)
Main problems: Main problems:
very old population (population aged very old population (population aged over 65 over 65 ys) ys)
low Programs budget low Programs budget
The ultimate goal:The ultimate goal:
to increase general awareness about CRC and the value of screening. to increase general awareness about CRC and the value of screening.
to increase compliance to increase compliance
to decreasing the fear from examinationto decreasing the fear from examination
Conclusion

CRC Screening Program CommitteeCRC Screening Program Committee
Prof. Dr. Milan Kujundžić – gastroenterologist (President)Prof. Dr. Milan Kujundžić – gastroenterologist (President) Prof. Dr. Miroslava Katičić – gastroenterologistProf. Dr. Miroslava Katičić – gastroenterologist Prof. Dr. Davor Štimac – gastroenterologistProf. Dr. Davor Štimac – gastroenterologist Prof. Dr. Marija Strnad - epidemiologistProf. Dr. Marija Strnad - epidemiologist Prof. Dr. Mirko Šamija – oncologistProf. Dr. Mirko Šamija – oncologist Prof. Dr. Zdravko Ebling – general practitionerProf. Dr. Zdravko Ebling – general practitioner Doc. Dr. Nataša Antoljak – epidemiologistDoc. Dr. Nataša Antoljak – epidemiologist Dr. Valerija Stamenić – Ministry od Health RC representativeDr. Valerija Stamenić – Ministry od Health RC representative Dr. Danica Kramarić – Dr. Danica Kramarić – Ministry od Health RC representativeMinistry od Health RC representative
Public Health Institutes are responsible for Public Health Institutes are responsible for Program coordination. Program coordination.