fibrate and cardiovascular disease: evident from meta-analysis
TRANSCRIPT

Fibrate and cardiovascular disease: Evident from meta-analysis
Thongchai Pratipanawatr

ยุคหินเกา
ยุคหินกลาง
ยุคหินใหม
?
?
?

ยุคหินเกา
ยุคหินกลาง
ยุคหินใหม
?
?
?
“Statin era”

CURRENT ROLE OF FIBRATE
What are the roles of fibrate in statin era.Severe hypertriglyceridemiaAllergy to statinSide effect from statin
MyopathyGI : N/VHepatitis
Combination with statin in combined dyslipidemia

DRUG AFFECTING LIPOPROTEIN METABOLISM
Drug class Lipid effects Side effects Contraindications
Statin Decrease LDL Myopathy, increase liver enzyme
Active or chronic liver disease
Fibrate Decrease TG and increase HDL
Dyspepsia, gall stones, myopathy
Severe renal and hepatic disease
Bile acid sequestrants
Decrease LDL Gastrointestinal distress, constipation, decrease absorption of other drugs
Dysbetalipoproteinemia, Hypertriglyceridemia (TG>400 mg/dl)
Ecetimide Decrease LDL increase liver enzyme Hypertriglyceridemia(TG>400 mg/dl)
Nicotinic acid
Decrease LDL Flushing, hyperglycemia, hyperuricemia, hepatotoxicity
Chronic liver disease, severe gout

เราทําไมตองรักษาโรคไขมันสูง?1.ใหผูปวยอายุยืนยาว2. ใหผูปวยไมเจ็บไมปวย3. ใหผูปวยใหผูปวยมีความสุข

THREE CATEGORIES OF RISK THATMODIFY LDL CHOLESTEROL GOALS
Risk Category LDL Goal
CHD and CHD risk equivalents
< < 100(Optional <70)
Multiple (2+) risk factors <130<130
0-1 risk factor <160<160

CHD and CHD risk equivalents
CHDDMPeripheral artery diseaseAbdominal aortic aneurysmSymptomatic carotid artery disease

ATHEROSCLEROTIC RISK FACTORS
Age : male>45 female>55 yrsSmokingHypertensionLow HDL (<40 mg/l)Family history of premature CHD(male>55, female>45 yrs)

OBJECTIVES
Efficacy of fibrate onMyocardial infarctionCoronary artery revascularizationStrokeDeath
Safety of fibrate

LIPID METABOLISM

Small bowel
Bile
Chylomicron
CE
TGTG
TGTG
TG
Chylomicronremnant
CETG
TG
TG
Lipoprotein lipase
VLDL
CE
TGTG
TGTG
TG
IDL
CE
TG
TGTGCE
LDL
CE TGCE
Lipoproteinlipase
TG
TG
Peripheralcell
B
B
B
HMG coA reductase
CHOLESTEROL TRANSPORT SYSTEM

REVERSE CHOLESTEROL TRANSPORT SYSTEM
CEC
ABC-A1A-IC
A-I
CESR-B1
A-I
CE-depletedHDL
A-I
Kidney
VLDL/LDL
CE
CE
CETP
CE
C
Bile
LCAT
Nascent HDL
MatureHDL
Peripheralcell

PPRE (DR-1)
RXR
AGGTCA X AGGTCA
retinoicPPARα
Activation of PPAR alpha alters expression of specific genes

PPRE (DR-1)
PPARα RXR
AGGTCA X AGGTCA
Gene expression-Increase LPL, A I-Decrease C III
Fibrate retinoic
Activation of PPAR alpha alters expression of specific genes

Small bowel
Bile
Chylomicron
CE
TGTG
TGTG
TG
Chylomicronremnant
CETG
TG
TG
Lipoprotein lipase
VLDL
CE
TGTG
TGTG
TG
IDL
CE
TG
TGTGCE
LDL
CE TGCE
Lipoproteinlipase
TG
TG
Peripheralcell
B
B
BDecrease apo C III
CHOLESTEROL TRANSPORT SYSTEM
HMG coA reductase

REVERSE CHOLESTEROL TRANSPORT SYSTEM
CEC
ABC-A1A-IC
A-I
CESR-B1
A-I
CE-depletedHDL
A-I
Kidney
VLDL/LDL
CE
CE
CETP
CE
C
Bile
LCAT
Nascent HDL
MatureHDL
Peripheralcell

META-ANALYSIS:THE EFFECT OF FIBRATE ON CARDIOVASCULAR DISEASE

Search methodology

PUBMED SEARCH
#1. cardiovascular disease [ Mesh ] 63,052 papers#2. fibrate 74 papers#3. fibric acid 44 papers#4. gemfibrozil 316 papers#5. bezafibrate 185 papers#6. fenofibrate 1,256 papers#7. #1 OR #2 177 papers#8. #1 OR #3 115 papers#9. #1 OR #4 379 papers#10. #1 OR #5 230 papers#11. #1 OR #6 274 papers
INCLUDE STUDY
1. Randomized control trials2. Intervention :
fenofibrate, bezafibrate, gemfibrozil3. Outcome :
death, cardiovascular disease (CVD) death, myocardial infarction, stroke, side effects
4. Duration of study more than 6 month

META ANALYSIS OF FIBRATE STUDIES
Study year Treatment Control
Helsigki 1987 2051 2030
BECAIT 1997 42 39
SENDCAP 1998 81 83
VA HIT 1999 1264 1267
BIP 2000 1548 1542
DAIS 2001 207 211
Leader 2002 783 785
FIELD 2005 4895 4900
Total 10664 10644

META ANALYSIS OF FIBRATE STUDIES
Study year Treatment Control
Helsigki 1987 Gemfibrozil Primary
BECAIT 1997 Bezafibrate Secondary
SENDCAP 1998 Bezafibrate Primary
VA HIT 1999 Gemfibrozil Secondary
BIP 2000 Bezafibrate Secondary
DAIS 2001 Fenofibrate Mix
Leader 2002 Bezafibrate Primary
FIELD 2005 Fenofibrate Mix
Total 10664 10644

HETEROGENEITY
Statistic : chi2
Subgroup analysisPrimary vs secondaryDrugs

RESULTS

Myocardial infarction

Pratipanawatr T MD , unpublished
Study Treatment Control
Genfibrozil
Helsigki 51/2051 79/2030
VA HIT 219/1264 275/1267
Fenofibrate
DAIS 9/207 11/211
FIELD 158/4895 207/4900
Bezalifrate
BECAIT 3/42 11/39
SENDCAP 6/81 17/83
BIP 168/1548 189/1542
Leader 90/783 111/785
Total 10664 10644
0.72 (0.61-0.86)
0.76 (0.62-0.93)
1 2 5 10.5.20.1
Favours treatment Favours control
0.79 (0.66-0.94)
0.76 (0.68-0.84)
FATAL AND NON-FATAL MYOCARDIAL INFARCTION

Pratipanawatr T MD , unpublished
Study Treatment Control
Primary
Helsigki 51/2051 79/2030
SENDCAP 6/81 17/83
Leader 90/783 111/785
Secondary
BECAIT 3/42 11/39
BIP 168/1548 189/1542
VA HIT 219/1264 275/1267
Mix
DAIS 9/207 11/211
FIELD 158/4895 207/4900
Total 10664 10644
0.69 (0.55-0.86)
0.79 (0.68-0.91)
1 2 5 10.5.20.1
Favours treatment Favours control
0.76 (0.62-0.93)
0.76 (0.68-0.84)
FATAL AND NON-FATAL MYOCARDIAL INFARCTION

CORONARY REVASCULIZATION
Pratipanawatr T MD , unpublished
Study Treatment Control
Genfibrozil
VA HIT 284/1264 320/1267
Fenofibrate
DAIS 19/207 31/211
FIELD 290/4895 364/4900
Bezalifrate
BIP 72/1548 77/1542
Total 7914 7920
0.86 (0.71-1.03)
0.77 (0.68-0.90)
1 2 5 10.5.20.1
Favours treatment Favours control
1.05 (0.82-1.35)
0.84 (0.76-0.93)

OBJECTIVES
Efficacy of fibrate onMyocardial infarctionCoronary artery revascularizationStrokeDeath
Safety of fibrate

OBJECTIVES
Efficacy of fibrate onMyocardial infarctionCoronary artery revascularizationStrokeDeath
Safety of fibrate

“ Treatment with fibrate significantly reduced myocardial infarction (by 24%) and coronary artery revascularization (by 16%).”
Conclusions

Stroke

STROKE
Pratipanawatr T MD , unpublished
Study Treatment Control
Genfibrozil
Helsigki 6/2051 4/2030
VA HIT 64/1264 88/1267
Fenofibrate
Shiming et al 13/115 24/110
FIELD 158/4895 175/4900
Bezalifrate
BIP 72/1548 77/1542
Leader 60/783 49/785
Total 10664 10644
0.75 (0.54-1.03)
0.85 (0.69-1.05)
1 2 5 10.5.20.1
Favours treatment Favours control
1.05 (0.82-1.35)
0.89 (0.77-1.02)

Pratipanawatr T MD , unpublished
Study Treatment Control
Primary
Helsigki 6/2051 4/2030
Leader 60/783 49/785
Shiming et al 13/115 24/110
Secondary
BIP 72/1548 77/1542
VA HIT 64/1264 88/1267
Mix
FIELD 158/4895 175/4900
Total 10656 10634
1.02 (0.73-1.41)
0.81 (0.65-1.03)
1 2 5 10.5.20.1
Favours treatment Favours control
0.90 (0.72-1.12)
STROKE
0.89 (0.77-1.02)

OBJECTIVES
Efficacy of fibrate onMyocardial infarctionCoronary artery revascularizationStrokeDeath
Safety of fibrate

OBJECTIVES
Efficacy of fibrate onMyocardial infarctionCoronary artery revascularizationStrokeDeath
Safety of fibrate

“ Treatment with fibrate reduced incidence of stroke by 11%.”
Conclusions

Compared with statin:
MI, revascularization and Stroke
Cholesterol Treatment Trialists’ (CTT) Collaborators.Lancet 2005; 366: 1267–78


Death

Pratipanawatr T MD , unpublished
Study Treatment Control
Genfibrozil
Helsigki 45/2051 42/2030
VA HIT 198/1264 220/1267
Fenofibrate
DAIS 6/207 9/211
FIELD 356/4895 323/4900
Bezalifrate
BIP 161/1548 152/1542
Leader 204/783 195/785
Total 10664 10644
0.92 (0.76-1.11)
1.10 (0.94-1.28)
1 2 5 10.5.20.1
Favours treatment Favours control
1.06 (0.90-1.25)
1.04 (0.94-1.14)
TOTAL DEATH

Pratipanawatr T MD , unpublished
Study Treatment Control
Primary
Helsigki 45/2051 42/2030
Leader 204/783 195/785
Secondary
BIP 161/1548 152/1542
VA HIT 219/1264 275/1267
Mix
DAIS 6/207 9/211
FIELD 356/4895 323/4900
Total 10664 10644
1.07 (0.87-1.30)
0.96 (0.82-1.12)
1 2 5 10.5.20.1
Favours treatment Favours control
1.10 (0.94-1.28)
TOTAL DEATH
1.04 (0.94-1.14)

Pratipanawatr T MD , unpublished
Study Treatment Control
Genfibrozil
Helsigki 14/2051 19/2030
VA HIT 93/1264 118/1267
Fenofibrate
FIELD 140/4895 127/4900
Bezalifrate
BIP 95/1548 88/1542
Leader 64/783 65/785
Total 10541 10541
0.77 (0.59-1.00)
1.11 (0.87-1.41)
1 2 5 10.5.20.1
Favours treatment Favours control
1.04 (0.83-1.31)
0.97 (0.84-1.12)
CVD DEATH

Pratipanawatr T MD , unpublished
Study Treatment Control
Primary
Helsigki 14/2051 19/2030
Leader 64/783 65/785
Secondary
BIP 95/1548 88/1542
VA HIT 93/1264 118/1267
Mix
FIELD 140/4895 127/4900
Total 10541 10541
0.92 (0.67-1.27)
0.91 (0.74-1.11)
1 2 5 10.5.20.1
Favours treatment Favours control
1.11 (0.87-1.41)
CVD DEATH
0.97 (0.84-1.12)

OBJECTIVES
Efficacy of fibrate onMyocardial infarctionCoronary artery revascularizationStrokeDeath
Safety of fibrate

OBJECTIVES
Efficacy of fibrate onMyocardial infarctionCoronary artery revascularizationStrokeDeath
Safety of fibrate

“ Fibrate did not reduce rate of death and cardiovascular death. However, gemfibrozil may reduce risk of cardiovascular death”
Conclusions

Compared with statin:
Death and CVD death
Cholesterol Treatment Trialists’ (CTT) Collaborators.Lancet 2005; 366: 1267–78

Microvascular complications
(FIELD tertiary endpoints)

Microvascular diseaseRetinopathy
Cum
ula
tive
ris
k (%
)
Years from randomization
HR = 0.7095% CI = 0.58–0.85p = 0.0003
4,900
4,895
4,775
4,792
4,664
4,701
4,573
4,618
4,472
4,502
2,518
2,529
Placebo
Fenofibrate835
841
10
8
6
4
2
0
0 1 2 3 4 5
Fenofibrate
Placebo
6
Number of patients still followed-up at the given year
FIELD Study Investigators. Lancet 2005 ; 366 (9500) : 1849-61

5.2%
3.6%
0
1
2
3
4
5
6
Placebo Fenofibrate
Perc
enta
ge
of pat
ieNeed for laser treatment
for retinopathy
“This effect cannot be explained by changes in HbA1c or concomitant
medications, or by the minor reduction in blood pressure in the fenofibrate group”
P=0.0003
-30%
Microvascular diseaseRetinopathy
FIELD Study Investigators. Lancet 2005 ; 366 (9500) : 1849-61

Progression of microalbuminuria(baseline to study close)
Regression No change Progression
Placebo(n=4900)
400(8.2%)
3654(74.6%)
539(11.0%)
Fenofibrate(n=4895)
462(9.4%)
3583(73.2%)
466(9.5%)
Mann-Whitney test:P=0.002Albuminuria status categories:Normal: <3.5 mg/mmol; microalbuminuria:3.5-<35 mg/mmol;macroalbuminuria: > 35 mg/mol
“This effect cannot be explained by changes in HbA1c or concomitant medications, or by the minor reduction in blood pressure in the
fenofibrate group”
FIELD Study Investigators. Lancet 2005 ; 366 (9500) : 1849-61

PATHOGENESIS OF PROLIFERATIVE DIABETIC RETINOPATHY
Retinal cell ischemia
Microvascular obstruction
Vascular Endothelium Growth Factor
Endothelium proliferation(Neovascularization)

POSSIBLE EFFECT OF FIBRATE ON DIABETIC RETINOPATHY
Retinal cell ischemia
Microvascular obstruction
Vascular Endothelium Growth Factor
Endothelium proliferation(Neovascularization)
Decrease lipotoxicity
Decrease lipid utility(14% less O2 consumption)
Decrease VEGF via inhibition of activate protein1(Grau R Biocehm J (2006) 395;81)

Safety results

Pratipanawatr T MD , unpublished
Study Treatment Control
Genfibrozil
Helsigki 11/2051 11/2030
VA HIT 126/1264 138/1267
Fenofibrate
DAIS 5/207 7/211
FIELD 393/4895 373/4900
Bezalifrate
BIP 161/1548 152/1542
Total 9965 9950
0.91 (0.71-1.16)
1.05 (0.91-1.22)
1 2 5 10.5.20.1
Favours treatment Favours control
0.93 (0.68-1.26)
1.00 (0.89-1.12)
CANCER

Compared with statin:
Cancer
Cholesterol Treatment Trialists’ (CTT) Collaborators.Lancet 2005; 366: 1267–78


Pratipanawatr T MD , unpublished
Study Treatment Control
FIELD 11/4895 7/4900
BIP 4/1548 1/1542
Total 6443 6442
1 2 5 10.5.20.1
Favours treatment Favours control
1.88 (0.8-4.43)
ELEVATED CK

Adverse event Placebo(n = 4,900)
Fenofibrate(n = 4,895)
ALT 3–5 × ULN 26 (< 1%) 11 (< 1%)
> 5 × ULN 12 (< 1%) 11 (< 1%)
CPK 5–10 × ULN 7 (< 1%) 11 (< 1%)
> 10 × ULN 3 (< 1%) 4 (< 1%)
Elevated creatinine (> 200 μmol/L) 48 (1%) 73 (2%)
Laboratory variable measurements occurring in < 2 % of patients
Abbreviations: ALT = alanine aminotransferase; CPK = creatine phosphokinase; ULN = upper limit of normal.
FIELD Study Investigators. Lancet 2005 ; 366 (9500) : 1849-61
Adverse event Placebo(n = 4,900)
Fenofibrate(n = 4,895)
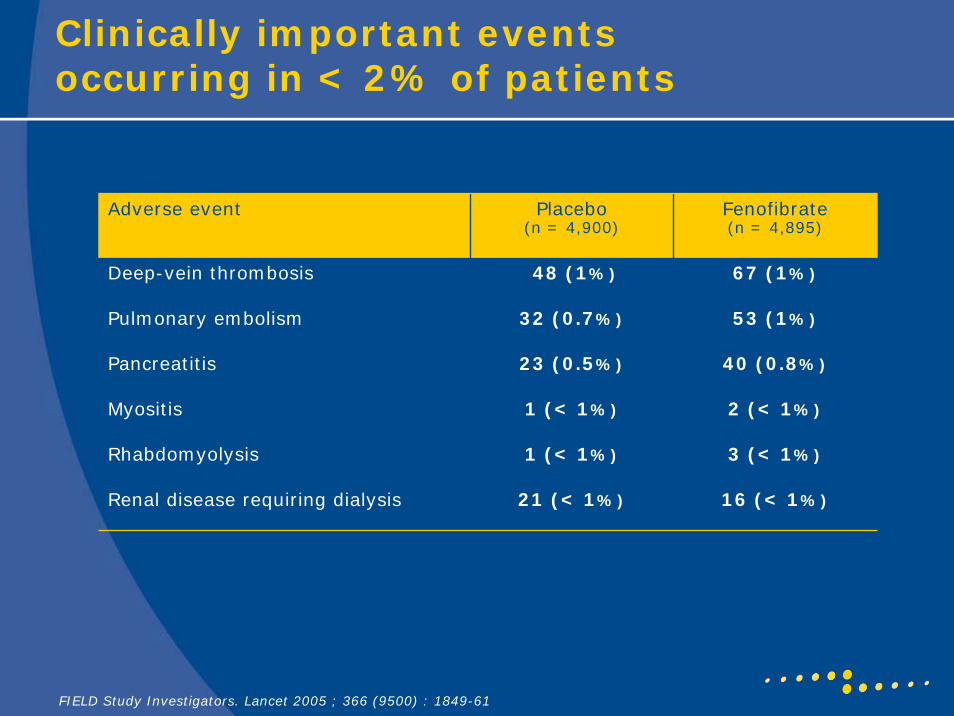
Deep-vein thrombosis 48 (1%) 67 (1%)
Pulmonary embolism 32 (0.7%) 53 (1%)
Pancreatitis 23 (0.5%) 40 (0.8%)
Myositis 1 (< 1%) 2 (< 1%)
Rhabdomyolysis 1 (< 1%) 3 (< 1%)
Renal disease requiring dialysis 21 (< 1%) 16 (< 1%)
Clinically important events occurring in < 2% of patients
FIELD Study Investigators. Lancet 2005 ; 366 (9500) : 1849-61

Pratipanawatr T MD , unpublished
Study Treatment Control
Genfibrozil
Helsigki 225/2051 142/2030
VA HIT 505/1264 430/1267
Fenofibrate
DAIS 1/207 4/211
FIELD 975/4895 927/4900
Total 9965 9950
1.64 (1.32-2.04)
1.06 (0.96-1.71)
1 2 5 10.5.20.1
Favours treatment Favours control
1.18 (1.09-1.28)
GI SIDE EFFECT

OBJECTIVES
Efficacy of fibrate onMyocardial infarctionCoronary artery revascularizationStrokeDeath
Safety of fibrate

OBJECTIVES
Efficacy of fibrate onMyocardial infarctionCoronary artery revascularizationStrokeDeath
Safety of fibrate

“ Fibrate did not increase incidence of cancer. However, it may increase incidence of myopathy”
Conclusions

THANK YOU