fever of unknown origin bryan youree vanderbilt university medical center
TRANSCRIPT

Fever of Unknown OriginFever of Unknown Origin
Bryan YoureeBryan YoureeVanderbilt University Medical CenterVanderbilt University Medical Center

ObjectivesObjectives
Definition and pathophysiology of Definition and pathophysiology of feverfever
FUO: classifications and etiologyFUO: classifications and etiology
Diagnostic workup of FUODiagnostic workup of FUO
PrognosisPrognosis

Fever versus HyperthermiaFever versus Hyperthermia
FeverFever: resetting of the thermostatic set-: resetting of the thermostatic set-point in the anterior hypothalamus and the point in the anterior hypothalamus and the resultant initiation of heat-conserving resultant initiation of heat-conserving mechanisms until the internal temperature mechanisms until the internal temperature reaches the new level.reaches the new level.HyperthermiaHyperthermia: an elevation in body : an elevation in body temperature that occurs in the absence of temperature that occurs in the absence of resetting of the hypothalamic resetting of the hypothalamic thermoregulatory centerthermoregulatory center

Mechanisms of Hyperthermia and Mechanisms of Hyperthermia and Associated ConditionsAssociated Conditions
1. 1. Excessive heat productionExcessive heat production: exertional : exertional hyperthermia, thyrotoxicosis, hyperthermia, thyrotoxicosis, pheochromocytoma, cocaine, delerium pheochromocytoma, cocaine, delerium tremens, malignant hyperthermiatremens, malignant hyperthermia
2.2. Disorders of heat dissipationDisorders of heat dissipation: heat : heat stroke, autonomic dysfunctionstroke, autonomic dysfunction
3.3. Disorders of hypothalamic functionDisorders of hypothalamic function: : neuroleptic malignant syndrome, CVA, neuroleptic malignant syndrome, CVA, traumatrauma

What is the normal human body What is the normal human body temperature?temperature?
A.A. 37.537.5° C° C
B.B. 98.6° F98.6° F
C.C. 340.15 K340.15 K
D.D. Each human being is a unique individual, Each human being is a unique individual, and therefore, normal temperature and therefore, normal temperature cannot be defined.cannot be defined.

What is the normal human body What is the normal human body temperature?temperature?
A.A. 37.637.6° C° C
B.B. 98.6° F98.6° F
C.C. 340.15 K340.15 K
D.D. Each human being is a unique individual, Each human being is a unique individual, and therefore, normal temperature and therefore, normal temperature cannot be defined.cannot be defined.

Wunderlich’s MaximWunderlich’s Maxim
After analyzing >1 million axillary After analyzing >1 million axillary temperatures from temperatures from ~25,000 patients, ~25,000 patients, Wunderlich identified 37.0° C (36.2-37.5) Wunderlich identified 37.0° C (36.2-37.5) as the mean temperature in healthy adults.as the mean temperature in healthy adults.
Temperature readings >38.0° C were Temperature readings >38.0° C were deemed as “suspicious/probably febrile.”deemed as “suspicious/probably febrile.”
1Wunderlich C. Das Verhalten der Eiaenwarme in Krankenheiten. Leipzig, Germany: Otto Wigard;1868.2Mackowiak, et al., JAMA 1992;268:1578

Normal Body TemperatureNormal Body Temperature
For healthy individuals 18 to 40 years of age, For healthy individuals 18 to 40 years of age, the mean oral temperature is 36.8° ± 0.4°C the mean oral temperature is 36.8° ± 0.4°C (98.2° ± 0.7°F)(98.2° ± 0.7°F)Low levels occur at 6 A.M. and higher levels Low levels occur at 6 A.M. and higher levels at 4 to 6 P.M. at 4 to 6 P.M. The maximum normal oral temperature is The maximum normal oral temperature is 37.2°C (98.9°F) at 6 A.M. and 37.7°C 37.2°C (98.9°F) at 6 A.M. and 37.7°C (99.9°F) at 4 P.M.(99.9°F) at 4 P.M.These values define the These values define the 99th percentile99th percentile for for healthy individuals.healthy individuals.
Mackowiak, et al., JAMA 1992;268:1578

Normal Body Temperature CaveatsNormal Body Temperature Caveats
Rectal temperatures are generally 0.4°C Rectal temperatures are generally 0.4°C (0.7°F) higher than oral readings. (0.7°F) higher than oral readings.
Tympanic membrane (TM) values are Tympanic membrane (TM) values are 0.8°C (1.6°F) lower than rectal 0.8°C (1.6°F) lower than rectal temperatures when thermometer is in the temperatures when thermometer is in the unadjusted-mode. unadjusted-mode.
How does fever occur?How does fever occur?
A.A. Build up of evil humorsBuild up of evil humors
B.B. IL-1 and IL-6IL-1 and IL-6
C.C. TNFTNF
D.D. Disruption of the medulla oblongataDisruption of the medulla oblongata
E.E. A and DA and D
F.F. B and CB and C
How does fever occur?How does fever occur?
A.A. Build up of evil humorsBuild up of evil humors
B.B. IL-1 and IL-6IL-1 and IL-6
C.C. TNFTNF
D.D. Disruption of the medulla oblongataDisruption of the medulla oblongata
E.E. A and DA and D
F.F. B and CB and C

Mackowiak, P. A. Arch Intern Med 1998;158:1870-1881.
Hypothetical Model for the Febrile Response
Interleukin-1 β and TNF-α play prominent rolesin fever production by stimulating the release ofcyclic AMP from the glial cells and activatingneuronal endings from the thermoregulatory center that extend into the area.

Bacterial PyrogensBacterial Pyrogens
Lipopolysaccharide (LPS) endotoxinLipopolysaccharide (LPS) endotoxinEndotoxin binds to LPS-binding protein and is transferred to CD14 Endotoxin binds to LPS-binding protein and is transferred to CD14 on macrophages, which stimulates the release of TNFon macrophages, which stimulates the release of TNFαα. .
Staphylococcus aureusStaphylococcus aureus enterotoxins enterotoxinsStaphylococcus aureusStaphylococcus aureus toxic shock syndrome toxic shock syndrome toxin (TSST)toxin (TSST)Both Both StaphylococcusStaphylococcus toxins are superantigens and activate T cells toxins are superantigens and activate T cells leading to the release of interleukin (IL)-1, IL-2, TNFleading to the release of interleukin (IL)-1, IL-2, TNFαα and TNF and TNFββ, , and interferon (IFN)-gamma in large amounts and interferon (IFN)-gamma in large amounts
Group A and B streptococcal toxins Group A and B streptococcal toxins Exotoxins induce human mononuclear cells to synthesize not only Exotoxins induce human mononuclear cells to synthesize not only TNFTNFαα but also IL1 and IL-6 but also IL1 and IL-6

Fever of Unknown OriginFever of Unknown Origin(Historical Definition)(Historical Definition)
Fever of at least 3 weeks’ durationFever of at least 3 weeks’ duration
Temperature of 101Temperature of 101° F (38.3° C) on ° F (38.3° C) on several occasionsseveral occasions
No diagnosis after a 1 week No diagnosis after a 1 week evaluation in the hospitalevaluation in the hospital
Petersdorf and Beeson Medicine 1961;40:1

Historical Causes of FUOHistorical Causes of FUO
Hippocrates: excess of yellow bileHippocrates: excess of yellow bile
Middle Ages: demonic possession Middle Ages: demonic possession (encephalitis?)(encephalitis?)
1818thth Century: Friction associated with the Century: Friction associated with the flow of blood through the vascular system flow of blood through the vascular system and from fermentation and putrefaction and from fermentation and putrefaction occurring in the blood and intestinesoccurring in the blood and intestines

Categories of FUOCategories of FUOFeatureFeature NosocomialNosocomial NeutropenicNeutropenic HIV-associatedHIV-associated ClassicClassic
Patient’s Patient’s situationsituation
Hospitalized, Hospitalized, acute care, no acute care, no infection when infection when admittedadmitted
Neutrophil count Neutrophil count either <500/either <500/µL or µL or expected to reach expected to reach that level in 1-2 that level in 1-2 daysdays
Confirmed HIV-Confirmed HIV-positivepositive
All others with All others with fevers for fevers for ≥3 ≥3 weeksweeks
Duration of Duration of illness while illness while investigatedinvestigated
3 days3 daysbb 3 days3 daysbb 3 days3 daysbb (or 4 (or 4 weeks as weeks as outpatient)outpatient)
3 days3 daysbb or 3+ or 3+ outpatient outpatient visitsvisits
ExamplesExamples Septic Septic thrombophlebitis, thrombophlebitis, sinusitis, sinusitis, C. C. difficiledifficile colitis, colitis, drug feverdrug fever
Perianal infection, Perianal infection, aspergillosis, aspergillosis, candidemiacandidemia
MAIMAIcc infection, infection, TB, non-TB, non-Hodgkin’s Hodgkin’s lymphoma, drug lymphoma, drug feverfever
Infections, Infections, malignancy, malignancy, inflammatory inflammatory diseases, drug diseases, drug feverfever
aAll require temperatures of ≥38.3°C (101°F) on several occasions.bIncludes at least 2 days’ incubation of microbiology cultures.cM. avium/M. intracellulare.
Modified from DT Durack, AC Street, in JS Remington, MN Swartz (eds): Current Clinical Topics in Infectious Diseases. Cambridge, MA, Blackwell, 1991.

Etiology of FUO Over a 40 Year Etiology of FUO Over a 40 Year PeriodPeriod
Mourad, et al. Arch Intern Med. 2003;163:545

Infectious Causes of FUOInfectious Causes of FUO
Intraabdominal abscess (liver, splenic, psoas, etc)Appendicitis, cholecystitis, tubo-ovarian abscess, pyometraIntracranial abscess, sinusitis, dental abscessChronic pharyngitis, tracheobronchitis, lung abscessSeptic jugular phlebitis, mycotic aneurysm, endocarditis, intravenous catheter infection, vascular graft infectionWound infection, osteomyelitis, infected joint prosthesis, pyelonephritis, prostatitis

Infectious Causes of FUOInfectious Causes of FUO
Intraabdominal abscess (liver, splenic, psoas, etc)Appendicitis, cholecystitis, tubo-ovarian abscess, pyometraIntracranial abscess, sinusitis, dental abscessChronic pharyngitis, tracheobronchitis, lung abscessSeptic jugular phlebitis, mycotic aneurysm, endocarditis, intravenous catheter infection, vascular graft infectionWound infection, osteomyelitis, infected joint prosthesis, pyelonephritis, prostatitis

Infectious Causes of FUOInfectious Causes of FUO
Intraabdominal abscess (liver, splenic, psoas, etc)Appendicitis, cholecystitis, tubo-ovarian abscess, pyometraIntracranial abscess, sinusitis, dental abscessChronic pharyngitis, tracheobronchitis, lung abscessSeptic jugular phlebitis, mycotic aneurysm, endocarditis, intravenous catheter infection, vascular graft infectionWound infection, osteomyelitis, infected joint prosthesis, pyelonephritis, prostatitis

Infectious Causes of FUOInfectious Causes of FUO
Intraabdominal abscess (liver, splenic, psoas, etc)Appendicitis, cholecystitis, tubo-ovarian abscess, pyometraIntracranial abscess, sinusitis, dental abscessChronic pharyngitis, tracheobronchitis, lung abscessSeptic jugular phlebitis, mycotic aneurysm, endocarditis, intravenous catheter infection, vascular graft infectionWound infection, osteomyelitis, infected joint prosthesis, pyelonephritis, prostatitis

Infectious Causes of FUOInfectious Causes of FUO
Tuberculosis, Mycobacterium avium complex, syphilis, Q fever, legionellosisSalmonellosis (including typhoid fever), listeriosis, ehrlichiosis, Actinomycosis, nocardiosis, Whipple’s diseaseFungal (candidaemia, cryptococcosis, sporotrichosis, aspergillosis, mucormycosis, Malassezia furfur)Malaria, babesiosis, toxoplasmosis, schistosomiasis, fascioliasis, toxocariasis, amoebiasis, infected hydatid cyst, trichinosis, trypanosomiasisCytomegalovirus, HIV, Herpes simplex, Epstein-Barr virus, parvovirus B19

Collagen Vascular DiseasesCollagen Vascular Diseases
Adult Still’s disease, SLEGiant cell arteritis/polymyalgia rheumatica, ankylosing spondylitisWegener’s granulomatosisRheumatic feverPolymyositis, rheumatoid arthritisFelty’s syndrome, eosinophilic fasciitis

MalignanciesMalignancies
LymphomaLymphoma
LymphomaLymphoma
LymphomaLymphoma
Renal cell carcinomaRenal cell carcinoma
Hepatocellular carcinomaHepatocellular carcinoma

Miscellaneous Causes of FUOMiscellaneous Causes of FUO
Complex partial status epilepticus, cerebrovascular accident, brain tumour, encephalitisDrug fever, Sweet’s syndrome, familial Mediterranean feverGout, pseudogoutKawasaki’s syndrome, Kikuchi’s syndromeCrohn’s disease, ulcerative colitis, sarcoidosis, granulomatous hepatitisDeep vein thrombosisDeep vein thrombosisAtelectasis?Atelectasis?
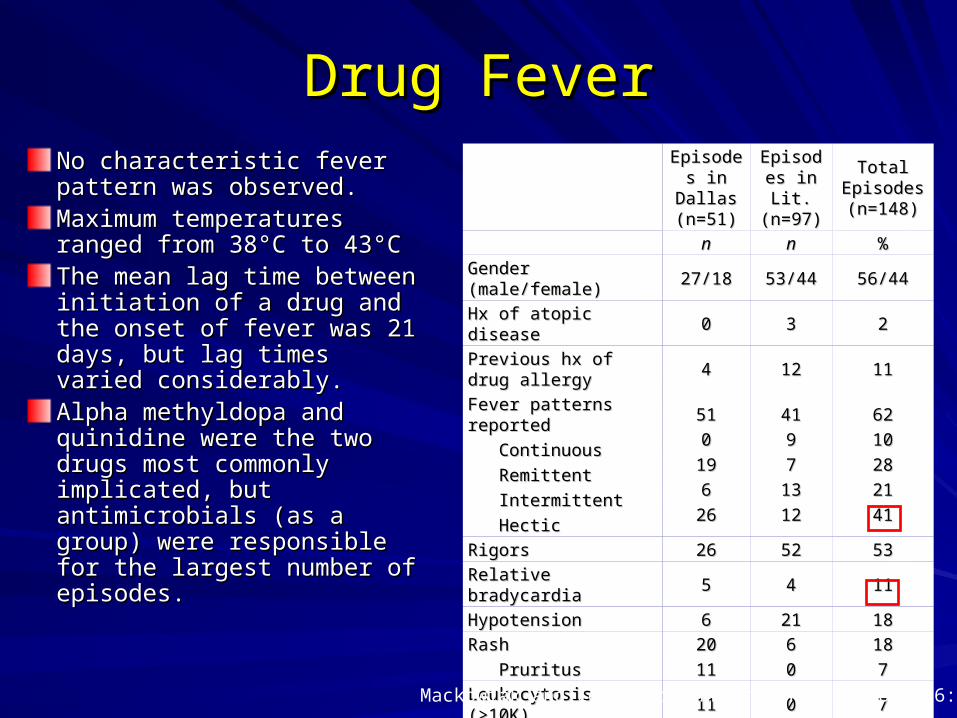
Drug FeverDrug FeverNo characteristic fever pattern No characteristic fever pattern was observed.was observed.Maximum temperatures Maximum temperatures ranged from 38ranged from 38°C to 43°C°C to 43°CThe mean lag time between The mean lag time between initiation of a drug and the initiation of a drug and the onset of fever was 21 days, onset of fever was 21 days, but lag times varied but lag times varied considerably.considerably.Alpha methyldopa and Alpha methyldopa and quinidine were the two drugs quinidine were the two drugs most commonly implicated, most commonly implicated, but antimicrobials (as a group) but antimicrobials (as a group) were responsible for the were responsible for the largest number of episodes.largest number of episodes.
Episodes Episodes in Dallas in Dallas (n=51)(n=51)
Episodes Episodes in Lit. in Lit. (n=97)(n=97)
Total Total Episodes Episodes (n=148)(n=148)
nn nn %%
Gender (male/female)Gender (male/female) 27/1827/18 53/4453/44 56/4456/44
Hx of atopic diseaseHx of atopic disease 00 33 22
Previous hx of drug allergyPrevious hx of drug allergy 44 1212 1111
Fever patterns reportedFever patterns reported
ContinuousContinuous
RemittentRemittent
IntermittentIntermittent
HecticHectic
5151
00
1919
66
2626
4141
99
77
1313
1212
6262
1010
2828
2121
4141
RigorsRigors 2626 5252 5353
Relative bradycardiaRelative bradycardia 55 44 1111
HypotensionHypotension 66 2121 1818
RashRash
PruritusPruritus
2020
1111
66
00
1818
77
Leukocytosis (>10K)Leukocytosis (>10K) 1111 00 77
Eosinophilia (>300/mmEosinophilia (>300/mm33)) 2121 1212 2222
HematologicHematologic 11 1212 99
DeathsDeaths 22 44 44
Mackowiak and LeMaistre Ann Intern Med 1987;106:728

Minimal Initial Diagnostic Workup Minimal Initial Diagnostic Workup For FUOFor FUO
Comprehensive historyComprehensive historyPhysical examinationPhysical examinationCBC + differentialCBC + differentialBlood film reviewed by hematopathologistBlood film reviewed by hematopathologistRoutine blood chemistryRoutine blood chemistryUA and microscopyUA and microscopyBlood (x 3) and urine culturesBlood (x 3) and urine culturesAntinuclear antibodies, rheumatoid factorAntinuclear antibodies, rheumatoid factorHIV antibodyHIV antibodyCMV IgM antibodies; heterophile antibody test (if c/w mono-like CMV IgM antibodies; heterophile antibody test (if c/w mono-like syndrome)syndrome)Q-fever serology (if risk factors)Q-fever serology (if risk factors)Chest radiographyChest radiographyHepatitis serology (if abnormal LFTs)Hepatitis serology (if abnormal LFTs)
Mourad, et al. Arch Intern Med. 2003;163:545

Liver Biopsy and Bone Marrow Liver Biopsy and Bone Marrow BiopsyBiopsy
Diagnostic yield of liver Diagnostic yield of liver biopsy has ranged from biopsy has ranged from 14% to 17%.14% to 17%.
Physical exam finding of Physical exam finding of hepatomegaly or hepatomegaly or abnormal liver profile are abnormal liver profile are not helpful in predicting not helpful in predicting abnormal biopsy result.abnormal biopsy result.
Complication rate is Complication rate is 0.06% to 0.32%0.06% to 0.32%
The diagnostic yield of bone marrow cultures in immunocompetent individuals has been found to be 0% to 2%1,2
Mourand et al. Arch Intern Med 2003;163:545
1Volk et al. J Clin Pathol 1998;110:150 2Riley et al. J Clin Pathol 1995:48:706
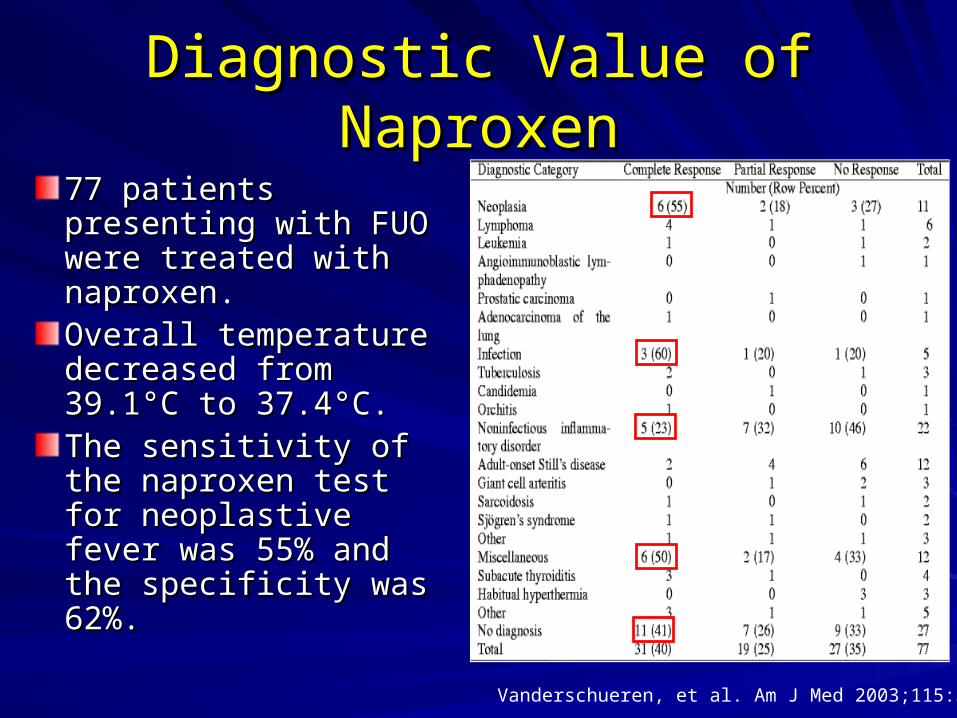
Diagnostic Value of NaproxenDiagnostic Value of Naproxen
77 patients presenting 77 patients presenting with FUO were treated with FUO were treated with naproxen.with naproxen.Overall temperature Overall temperature decreased from decreased from 39.139.1°C to 37.4°C.°C to 37.4°C.The sensitivity of the The sensitivity of the naproxen test for naproxen test for neoplastive fever was neoplastive fever was 55% and the 55% and the specificity was 62%.specificity was 62%.
Vanderschueren, et al. Am J Med 2003;115:572

Copyright restrictions may apply.
Mourad, O. et al. Arch Intern Med 2003;163:545-551.
Proposed Approach to FUO
Mourad, et al. Arch Intern Med. 2003;163:545

Marik, P. E. Chest 2000;117:855-869
Approach to Fever in the ICU

PrognosisPrognosis
Prognosis is determined primarily by the Prognosis is determined primarily by the underlying disease.underlying disease.
Outcome is worst for neoplasms.Outcome is worst for neoplasms.
FUO patients who remain undiagnosed FUO patients who remain undiagnosed after extensive evaluation generally have a after extensive evaluation generally have a favorable outcome and the fever usually favorable outcome and the fever usually resolves after 4-5 weeks.resolves after 4-5 weeks.
Larson et al. Medicine 1982;61:269

SummarySummary
FUO is often a diagnostic dilemmaFUO is often a diagnostic dilemma
Infections comprise Infections comprise ~30% of cases~30% of cases
Bone marrow biopsies are of low Bone marrow biopsies are of low diagnostic yielddiagnostic yield
Diagnostic approach should occur in a Diagnostic approach should occur in a step-wise fashion based on the H&Pstep-wise fashion based on the H&P
Patient’s that remain undiagnosed Patient’s that remain undiagnosed generally have a good prognosisgenerally have a good prognosis