fetal growth restriction
DESCRIPTION
Fetal growth restriction. Fetal growth restrictions **There are wide variety of reasons why a baby may be born small including congenital anomalies , feta infections and chromosomal abnormalities . - PowerPoint PPT PresentationTRANSCRIPT

Fetal growth Fetal growth restrictionrestriction
Fetal growth restrictionsFetal growth restrictions****There are wide variety of reasons why a baby may be born small There are wide variety of reasons why a baby may be born small
including congenital anomalies , feta infections and including congenital anomalies , feta infections and chromosomal abnormalitieschromosomal abnormalities . .
****however, most babies that are born small are either however, most babies that are born small are either constitutionally smallconstitutionally small ( i.e healthy but born to small parents and ( i.e healthy but born to small parents and fulfilling their genetic growth potential ) or are small secondary fulfilling their genetic growth potential ) or are small secondary to abnormal placental function and have to abnormal placental function and have FGRFGR..
****FGR is a major cause of neonatal and infent morbidity and FGR is a major cause of neonatal and infent morbidity and mortalitymortality . .

***In addition there is an increasing body of evidence that ***In addition there is an increasing body of evidence that certain adult disease ( such as diabetes and hypertension ) are certain adult disease ( such as diabetes and hypertension ) are most common in adult who were born with FGR.most common in adult who were born with FGR.
Definition and incidenceDefinition and incidence: : ** **FGR is defined as a failure of a fetus to achieve its genetic FGR is defined as a failure of a fetus to achieve its genetic
growth potentialgrowth potential. This is usually results in a fetus that is small . This is usually results in a fetus that is small for gestational age ( SGA )for gestational age ( SGA ) . .
****SGA means that the weight of the fetus is less than the tenth SGA means that the weight of the fetus is less than the tenth centile for its gestation. Other cut – off points ( e.g the third centile for its gestation. Other cut – off points ( e.g the third centile ) can be usedcentile ) can be used . .
****The term SGA and FGR are not synonymousThe term SGA and FGR are not synonymous..

****The neonatal mortality rate of a SGA infant born at 38 The neonatal mortality rate of a SGA infant born at 38 weeks 1% compared 0.2% in those with AGA ( appropriate weeks 1% compared 0.2% in those with AGA ( appropriate for gestational age)for gestational age)..
****Incidence is Incidence is 33 -10%-10% of infantsof infants are growth restricted are growth restricted..
****2525 --6060 % % of infants conventionally diagnosed to be SGA were of infants conventionally diagnosed to be SGA were in fact AGA when take in consideration determinant for in fact AGA when take in consideration determinant for birth weightbirth weight::
11 . .Ethnic groupEthnic group
22 . .ParityParity
33 . .WeightWeight
44 . .HeightHeight
What factors affect fetal weightWhat factors affect fetal weight??
11 . .SexSexterm males 150 gm term males 150 gm heavier and 0.9 cm heavier and 0.9 cm longer than femaleslonger than females
22 . .ParityParity1st born infants 1st born infants smallersmallereffect loss after 3rd effect loss after 3rd birthbirth
33 . .RaceRace, ethnicity, , ethnicity, nationalitynationality
44 . .AltitudeAltitude
Denver population Denver population growth curves under growth curves under estimate weights of estimate weights of infants born at sea infants born at sea levellevel
55 . .Maternal sizeMaternal size
maternal pre-pregnancy maternal pre-pregnancy weight and pregnancy weight and pregnancy weight gain correlate weight gain correlate with fetus sizewith fetus size

Normal Intrauterine GrowthNormal Intrauterine Growth
Stage 1Stage 1Stage 2Stage 2Stage 3Stage 3
HyperplasiaHyperplasia Hyperplasia/ Hyperplasia/ hypertrophyhypertrophy
HypertrophyHypertrophy
4-204-20 weeksweeks20-2820-28 weeksweeks28-4028-40 weeksweeks
Rapid mitosisRapid mitosisDeclining mitosisDeclining mitosisRapid hypertrophyRapid hypertrophy
Increasing DNA Increasing DNA contentcontent
Increasing cell sizeIncreasing cell sizeRapid increasing Rapid increasing cell sizecell size
rapid accumulation rapid accumulation of fat, muscle, of fat, muscle, connective tissueconnective tissue
SymmetricSymmetricMixed- asymmetricMixed- asymmetricAsymmetricAsymmetric


AetiologyAetiologyThey are grouped into 2 main categoriesThey are grouped into 2 main categories: :
11 . .Reduced fetal growth potential (directly affect the intrinsic Reduced fetal growth potential (directly affect the intrinsic
growth potential of the fetus)growth potential of the fetus) .. a. Aneuploidies, e.g. trisomy 18a. Aneuploidies, e.g. trisomy 18 , ,
b. Single gene defects e.g. Seckel’s syndromeb. Single gene defects e.g. Seckel’s syndrome..
c. Structural abnormalities, e.g. renal agenesisc. Structural abnormalities, e.g. renal agenesis..
d. Intrauterine infection, Cytom egalovirus, Toxoplasmosisd. Intrauterine infection, Cytom egalovirus, Toxoplasmosis
22 . .Reduced fetal growth supportReduced fetal growth support::
a. Maternal( systemic) factorsa. Maternal( systemic) factors::
** ** Under-nutrition (globally the major cause of FGR)Under-nutrition (globally the major cause of FGR) , e.g. , e.g. poverty, eating disorderspoverty, eating disorders..
** ** Maternal hypoxia, e.g. living at altitude, cyanotic heart Maternal hypoxia, e.g. living at altitude, cyanotic heart diseasedisease..
** ** Drugs, e.g. alcohol, cigarettes, cocaineDrugs, e.g. alcohol, cigarettes, cocaine . .

Smoking,Smoking, will increase the amount of carboxyhaemoglobin in the will increase the amount of carboxyhaemoglobin in the maternal circulation, effectively reduces the amount of oxygen maternal circulation, effectively reduces the amount of oxygen available to the fetus, thus causing FGR.available to the fetus, thus causing FGR.
alcohol and cocainealcohol and cocaine, probably act through multiple mechanisms , probably act through multiple mechanisms affecting fetal enzyme systems, placental blood flow and affecting fetal enzyme systems, placental blood flow and maternal substrate levels.maternal substrate levels.
b. Placental factors:b. Placental factors: ******Reduced uteroplacental perfusionReduced uteroplacental perfusion, e.g. inadequate , e.g. inadequate
trophoblast invasion, sickle cell disease, multiple gestation.trophoblast invasion, sickle cell disease, multiple gestation.
******Reduced fetoplacental perfusionReduced fetoplacental perfusion, e.g. single umbilical artery , e.g. single umbilical artery twin-twin transfusion syndrome.twin-twin transfusion syndrome.

In developed countries, the most common cause of FGR In developed countries, the most common cause of FGR is poor is poor placental function secondary to inadequate trophoblast placental function secondary to inadequate trophoblast invasion of the spiral arteriesinvasion of the spiral arteries. This results in . This results in reduced perfusionreduced perfusion of the intracotyledon space which in turn leads to abnormal of the intracotyledon space which in turn leads to abnormal development of the terminal villi and impaired transferee of development of the terminal villi and impaired transferee of oxygen and nutrients to the fetus. oxygen and nutrients to the fetus.
Less frequently, Less frequently, reduced perfusionreduced perfusion can occur from other can occur from other conditions such as conditions such as maternal sickle cell disease and the maternal sickle cell disease and the antiphospholipid syndromeantiphospholipid syndrome. . Multiple pregnancyMultiple pregnancy usually results usually results in a sharing of the uterine vascularity, which cause a relative in a sharing of the uterine vascularity, which cause a relative reduction in the blood flow to each placenta. reduction in the blood flow to each placenta.

Pathophysiology :Pathophysiology :FGR is frequently classified asFGR is frequently classified as
11 . .Symmetrical small fetusesSymmetrical small fetuses are normally associated with are normally associated with factors that directly impair fetal growth. Such as chromosomal factors that directly impair fetal growth. Such as chromosomal disorders and fetal infectionsdisorders and fetal infections . .
22 . .Asymmetrical growth restrictionAsymmetrical growth restriction is classically associated with is classically associated with uteroplacental insufficiency which leads to reduced oxygen uteroplacental insufficiency which leads to reduced oxygen transfer to the fetus and impaired excretion of CO2 by the transfer to the fetus and impaired excretion of CO2 by the placentaplacenta..
****A fall in PO2 and a rise in A fall in PO2 and a rise in ppCO2 in the fetal blood induces a CO2 in the fetal blood induces a chemoreceptors response in the fetal cadrotid bodies with chemoreceptors response in the fetal cadrotid bodies with resulting vasodilatation in the fetal brain, myocardium and resulting vasodilatation in the fetal brain, myocardium and adrenal glands and vasoconstriction in the kidneys, splanchnic adrenal glands and vasoconstriction in the kidneys, splanchnic
vessels, limbs and subcutaneous tissuesvessels, limbs and subcutaneous tissues..

****The The liver circulationliver circulation is also severely is also severely reducedreduced. Normally, 50% of . Normally, 50% of the well oxygenated blood in the umbilical vein passes to the the well oxygenated blood in the umbilical vein passes to the right atrium through the ductus venosus, eventually to reach right atrium through the ductus venosus, eventually to reach the fetal brain. With the reminder going to the portal the fetal brain. With the reminder going to the portal circulation in the livercirculation in the liver . .
****When there is fetal hyoxia, more of the well-oxygenated blood When there is fetal hyoxia, more of the well-oxygenated blood from the umbilical vein is diverted through the ductus venosus, from the umbilical vein is diverted through the ductus venosus, which means that the liver receives lesswhich means that the liver receives less . .
****The result of all these circulatory changes is an asymmetrical The result of all these circulatory changes is an asymmetrical fetus with fetus with relative brain sparing, reduced abdominal girth and relative brain sparing, reduced abdominal girth and skin thicknessskin thickness. The vasoconstriction in the fetal kidneys results . The vasoconstriction in the fetal kidneys results in impaired urine production and in impaired urine production and oligohydramniosoligohydramnios. The fetal . The fetal hypoxaemia also leads to hypoxaemia also leads to severe metabolic changes in the fetus severe metabolic changes in the fetus reflecting intrauterine starvationreflecting intrauterine starvation . .

****Antenatal fetal blood sampling has shown Antenatal fetal blood sampling has shown reduced levels of reduced levels of nutrients such as glucose and amino acidsnutrients such as glucose and amino acids ( especially essential ( especially essential amino acids ) and of amino acids ) and of hormons such as thyroxin and insulinhormons such as thyroxin and insulin. . There are There are increased levels of corticosteroids and increased levels of corticosteroids and catecholaminescatecholamines, which reflect the increased perfusion of the , which reflect the increased perfusion of the adrenal gland. adrenal gland.
**Haematological changes also reflects the chronic hypoxia, with **Haematological changes also reflects the chronic hypoxia, with increased levels of erythropoietin and nucleated red blood increased levels of erythropoietin and nucleated red blood cellscells..
**Chronic fetal hypoxia in FGR may eventually lead to fetal **Chronic fetal hypoxia in FGR may eventually lead to fetal academia, both respiratory and metabolicacademia, both respiratory and metabolic which if prolonged which if prolonged can lead to intrauterine death if the fetus is not removed from can lead to intrauterine death if the fetus is not removed from its hostile environment. its hostile environment.

****FGR fetuses are especially at risk from FGR fetuses are especially at risk from profound asphyxia in profound asphyxia in labourlabour due to further compromised of ther uteroplacental due to further compromised of ther uteroplacental
circulation by uterine contractioncirculation by uterine contraction..
ManagementManagement: : The detection of the SGA infant contains 2 elementsThe detection of the SGA infant contains 2 elements : :
11 . .the accurate assessment of gestational agethe accurate assessment of gestational age . .
22 . .the recognition of fetal smallnessthe recognition of fetal smallness..
** ** Early measurement of the Early measurement of the fetal crown – rump lengthfetal crown – rump length before before 13 weeks pulse 6 days gestation or 13 weeks pulse 6 days gestation or head circumferencehead circumference between 13 + 6 and 20 weeks remains the method of choice for between 13 + 6 and 20 weeks remains the method of choice for
confirming gestational ageconfirming gestational age . .

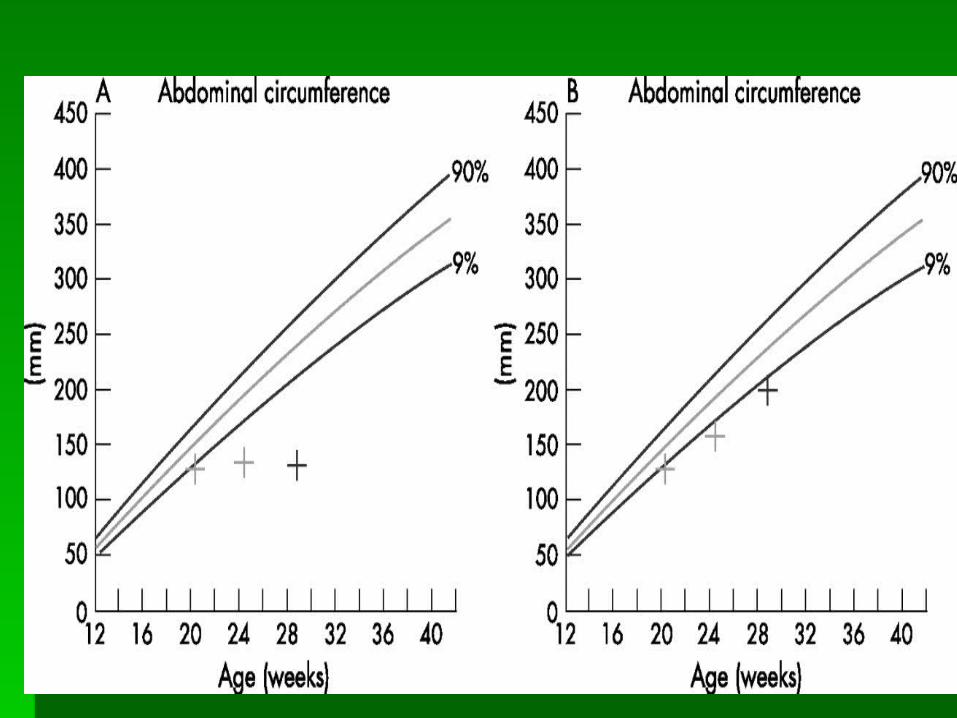
** ** Thereafter, the most precise way of assessing fetal growth is by Thereafter, the most precise way of assessing fetal growth is by ultrasound biometryultrasound biometry ( biparietal diameter, head ( biparietal diameter, head circumference, abdominal circumference and femur length ) circumference, abdominal circumference and femur length ) seriously at set time intervals ( usually of 4 weeks and no less seriously at set time intervals ( usually of 4 weeks and no less than 2 weeks ).than 2 weeks ).
Pregnancies at riskPregnancies at risk: : 11 . .Multiple pregnanciesMultiple pregnancies..
22 . .History of FGR in previous pregnancyHistory of FGR in previous pregnancy..
33 . .Current heavy smokersCurrent heavy smokers..
44 . .Current drug usersCurrent drug users..
55 . .Women with underlying medical disordersWomen with underlying medical disorders::
a/ hypertensiona/ hypertension . .
b/ Diabetesb/ Diabetes . .
c/ Cyanotic heart diseasec/ Cyanotic heart disease . .
d/ Antiphospholipid syndromed/ Antiphospholipid syndrome . .
66 . .Pregnancies where the symphysis – fundal height is less than Pregnancies where the symphysis – fundal height is less than expectedexpected..

** ** When a diagnosis of SGA has been made, the next step is to When a diagnosis of SGA has been made, the next step is to clarify whether the baby is clarify whether the baby is normal and simply constitutionally normal and simply constitutionally small or whether it is FGRsmall or whether it is FGR. .
**A comprehensive ultrasound examination of the fetal anatomy **A comprehensive ultrasound examination of the fetal anatomy should be made looking for fetal abnormalities that may should be made looking for fetal abnormalities that may explain the size. explain the size. Even if the anatomy appears normal, the Even if the anatomy appears normal, the presence of a normal amniotic fluid volume raises the suspicion presence of a normal amniotic fluid volume raises the suspicion of a fetal genetic defect and the parents should be counseled of a fetal genetic defect and the parents should be counseled accordinglyaccordingly. Amniocentesis and rapid fetal karyotype should . Amniocentesis and rapid fetal karyotype should be offered. be offered.
**Features suspicious of uteroplacental insufficiency are an **Features suspicious of uteroplacental insufficiency are an asymmetrically growth restricted fetus with a relatively small asymmetrically growth restricted fetus with a relatively small abdominal circumference, oligohydramnios and a high abdominal circumference, oligohydramnios and a high umbilical artery resistanceumbilical artery resistance. .
****At present, there are At present, there are no widely accepted treatment available no widely accepted treatment available for FGR related to uteroplacental insufficiencyfor FGR related to uteroplacental insufficiency . .
11 . .Obvious Obvious contributing factorscontributing factors, such as smoking , alcohol and , such as smoking , alcohol and drug abuse, should be optimizeddrug abuse, should be optimized . .
22 . .Low – dose Low – dose aspirinaspirin may have a role in the prevetion of FGR in may have a role in the prevetion of FGR in high – risk pregnancies but is not effective in the treatment high – risk pregnancies but is not effective in the treatment of established casesof established cases..
33 . .When growth restriction is severe and the fetus is too immature When growth restriction is severe and the fetus is too immature to be delivered safely, to be delivered safely, bed restbed rest in hospital is usually advised in hospital is usually advised in an effort to maximize placental blood flow although the in an effort to maximize placental blood flow although the
evidence supporting this practice is limitedevidence supporting this practice is limited..
****The aim of these interventions is to The aim of these interventions is to gain as much maturity as gain as much maturity as possible before delivering the fetuspossible before delivering the fetus, thereby reducing the , thereby reducing the modbidity associated with prematurity. modbidity associated with prematurity.
**However, timing the delivery in such a way that maximizes **However, timing the delivery in such a way that maximizes gestation without risking the baby dying in utero demands gestation without risking the baby dying in utero demands intensive fetal surveillanceintensive fetal surveillance..
1. Serial biometry and amniotic fluid volume measurement 1. Serial biometry and amniotic fluid volume measurement performed at performed at no less than 2 weekly intervalsno less than 2 weekly intervals..

22 . .In the FGR fetus In the FGR fetus dynamic tests of fetal well – beingdynamic tests of fetal well – being including including: :
A.A. Umbilical artery Doppler wave form analysis Umbilical artery Doppler wave form analysis..
B.B. Absence or reversed flow of blood in the umbilical artery Absence or reversed flow of blood in the umbilical artery during fetal diastole requires delivery in the near futureduring fetal diastole requires delivery in the near future..
C.C. In extremely pre-term or pre-viable infants with absent or In extremely pre-term or pre-viable infants with absent or reversed end diastolic flow in the umbilical artery, other fetal reversed end diastolic flow in the umbilical artery, other fetal arterial and venous Doppler studies can be performed arterial and venous Doppler studies can be performed although their use has not yet been proven by large although their use has not yet been proven by large prospective trialsprospective trials..
D.D. Fetal cardiotocography Fetal cardiotocography
An IUGR infant is at risk forAn IUGR infant is at risk for HypothermiaHypothermia??
HypoglycemiaHypoglycemia??
OrOr
HypocalcemiaHypocalcemia??
decreased subcutaneous fat, decreased subcutaneous fat, increased surface- volume ratio, increased surface- volume ratio, decreased heat productiondecreased heat production
decreased glycogen stores/ decreased glycogen stores/ glycogenolysis/ gluconeogenesisglycogenolysis/ gluconeogenesis
increased metabolic rateincreased metabolic rate
deficient catecholamine releasedeficient catecholamine release
Associated with perinatal stress, Associated with perinatal stress, asphyxia, prematurityasphyxia, prematurity

PrognosisPrognosis::******The prognosis of FGR is highly dependent uponThe prognosis of FGR is highly dependent upon
11 . .The causeThe cause , , 22 . .Severity andSeverity and,,
33 . .The gestation at deliveryThe gestation at delivery . .
****When FGR is related to a When FGR is related to a congenital infection or chromosomal congenital infection or chromosomal abnormalityabnormality, subsequent development of the child will be , subsequent development of the child will be determined by the determined by the precise abnormalityprecise abnormality..
****Of babies with FGR secondary to Of babies with FGR secondary to uteroplacental insufficiencyuteroplacental insufficiency, , some babies will suffer morbidity or mortality as a result of some babies will suffer morbidity or mortality as a result of prematurity for the survivors, the prematurity for the survivors, the long - term prognosis is long - term prognosis is good with low incidences of mental and physical disabilitygood with low incidences of mental and physical disability and and most infants demonstrate ‘ most infants demonstrate ‘ catch-up growthcatch-up growth ‘ after delivery ‘ after delivery when feeding is establishedwhen feeding is established..
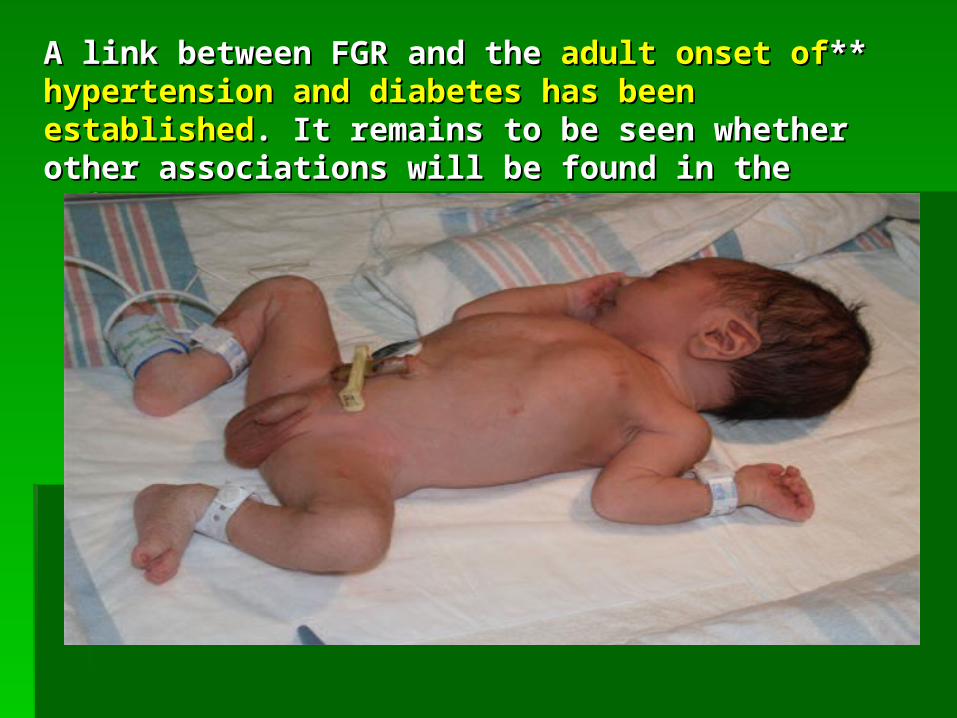
****A link between FGR and the A link between FGR and the adult onset of hypertension and adult onset of hypertension and diabetes has been establisheddiabetes has been established. It remains to be seen whether . It remains to be seen whether other associations will be found in the futureother associations will be found in the future . .

Thanks Thanks