femoroacetabular impingement in the throwing...
TRANSCRIPT

Femoroacetabular Impingement in the Throwing Athlete
Michael Banffy, MDSports Medicine, Hip PreservationKerlan Jobe Institute
Disclosures
�None

Baseball Hip Injuries - Background
�Abdominal/groin injuries
– Three season data (2011-2013)
– 5% of all injuries; 94% extra articular
– Non contact mechanism during defensive fielding (32%)
– Infielders experienced most hip and groin injuries
– Non-op treatment (12 days missed)– Operative treatment (97 days missed)
– Coleman et al 2015 (AJSM in press)

Increased Prevalence? Incidence?
�Understanding of hip anatomy has improved
�Recognition of hip pathology has improved
�Understanding of soft tissue abnormalities associated with bony morphologies
�Pathologic coping mechanisms can lead to further injuries

Hip Anatomy

Root of the Problem
�90% of patients with labral pathology have associated bony abnormalities� Trousdale et al. CORR 2004
�Alterations in Joint mechanics
�Undercoverge– “Dysplasia”
�Overcoverage– Femoroacetabular impingement (FAI)
�The two most common causes of osteoarthritis in the hips
Muscle Injury in Athletes
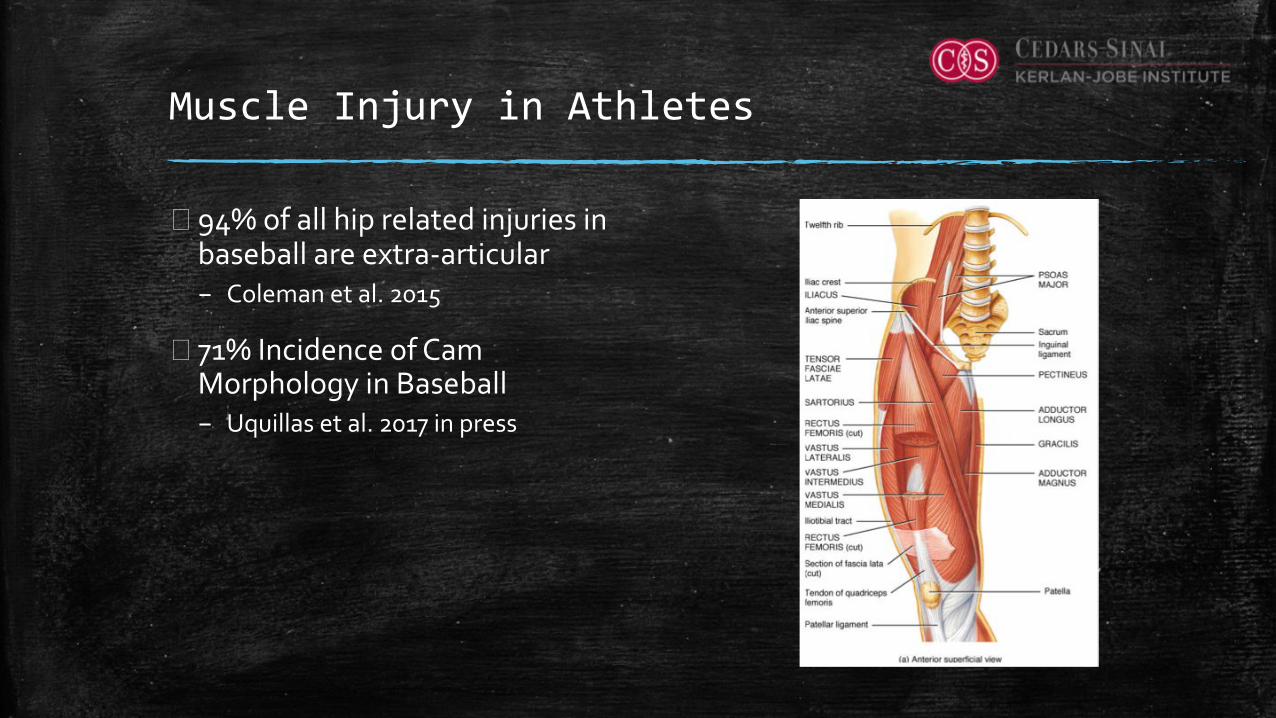
�94% of all hip related injuries in baseball are extra-articular– Coleman et al. 2015
� 71% Incidence of Cam Morphology in Baseball– Uquillas et al. 2017 in press

Compensatory Injury Patterns with FAI
�Anterior enthesopathy– Hip flexor strains– Psoas impingement– Subspine impingement
�Medial enthesopathy– Athletic pubalgia� Adductor tendinopathy� Rectus abdominus tendinopathy
– Osteitis Pubis

Compensatory Injury Patterns with FAI
�Posterior Compensatory Injury– Proximal hamstring strain– Deep gluteal syndrome– SI Joint dysfunction
�Lateral enthesopathies– Abductor injury– ITB Syndrome

Muscle Injury in Athletes
� “Cam avoidance”– Gait adopted by athletes with
symptomatic FAI– Increased stress on adductors– Chronic microtrauma and injury� Schilders et al JBJS 2009� Schilders et al JBJS 2007
� “Sports Hip Triad”– Labral tear, adductor strain, and a
rectus strain� Feeley et al AJSM 2008
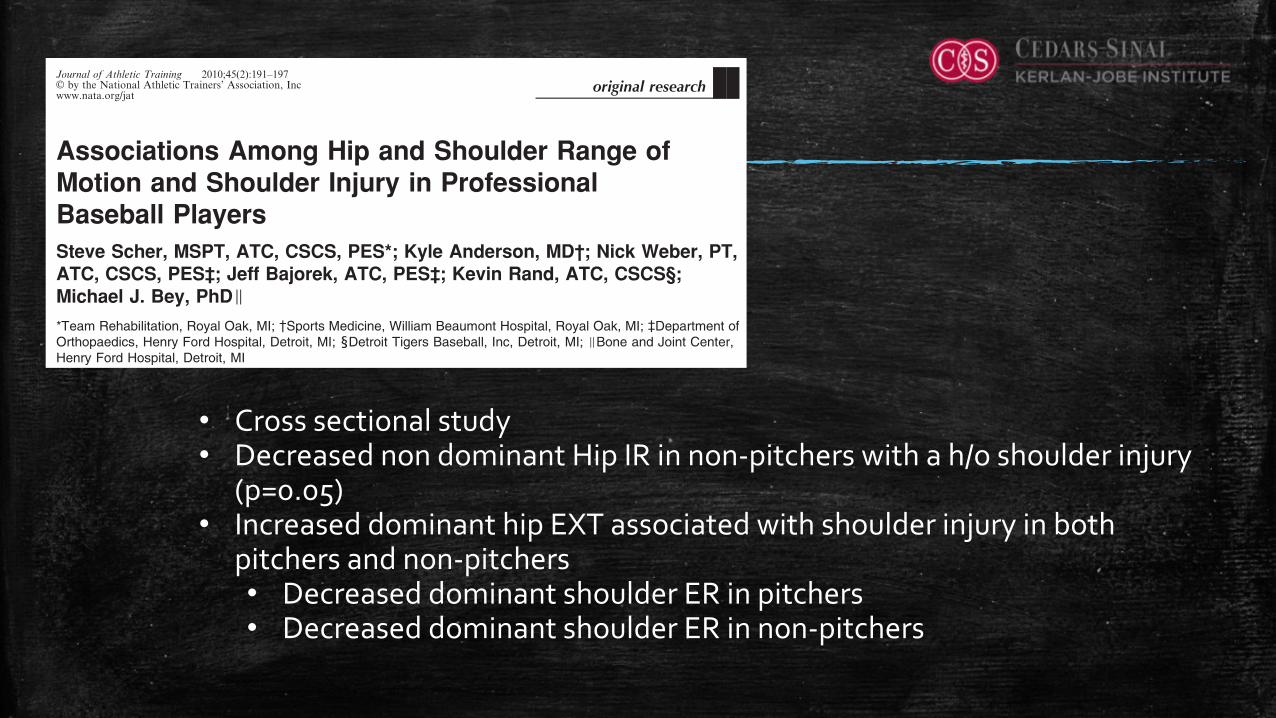
Associations Among Hip and Shoulder Range ofMotion and Shoulder Injury in ProfessionalBaseball PlayersSteve Scher, MSPT, ATC, CSCS, PES*; Kyle Anderson, MD!; Nick Weber, PT,ATC, CSCS, PES`; Jeff Bajorek, ATC, PES`; Kevin Rand, ATC, CSCS‰;Michael J. Bey, PhDI*Team Rehabilitation, Royal Oak, MI; 3Sports Medicine, William Beaumont Hospital, Royal Oak, MI; 4Department ofOrthopaedics, Henry Ford Hospital, Detroit, MI; 1Detroit Tigers Baseball, Inc, Detroit, MI; IBone and Joint Center,Henry Ford Hospital, Detroit, MI
Context: The overhead throwing motion is complex, andrestrictions in range of motion (ROM) at the hip may placeadditional demands on the shoulder that lead to injury. However,the relationship between hip and shoulder ROM in athletes withand without a history of shoulder injury is unknown.
Objective: To (1) determine if differences exist in hip andshoulder ROM between professional baseball players with ahistory of shoulder injury and those with no history of shoulderinjury and (2) assess relationships between hip and shoulderROM in these players.
Design: Cross-sectional study.Patients or Other Participants: Fifty-seven professional
baseball players.Main Outcome Measure(s): Outcome measures consisted
of hip extension and internal rotation, shoulder internal andexternal rotation, glenohumeral internal-rotation deficit, andhistory of shoulder injury. Differences in shoulder and hipROM were assessed with a 1-way analysis of variance.
Associations between hip and shoulder ROM were assessedwith linear regression.
Results: Nonpitchers with a history of shoulder injury hadmore external rotation and less internal rotation of the shoulderthan nonpitchers with no history of shoulder injury. Glenohu-meral internal-rotation deficit was greater in both pitchers andnonpitchers with a history of shoulder injury. The relationshipbetween dominant hip extension and shoulder external rotationwas significant for pitchers with a history of shoulder injury andnonpitchers with a history of shoulder injury.
Conclusions: Shoulder injury may be associated withspecific measures of hip and shoulder ROM, and hip extensionand shoulder external rotation may be related in baseballplayers with a history of shoulder injury. Additional research isnecessary to understand the specific mechanisms of shoulderinjury in the throwing athlete.
Key Words: throwing athletes, injuries, glenohumeral inter-nal-rotation deficit, kinetic chain
Key Points
N Shoulder internal rotation, nondominant hip internal rotation, and glenohumeral internal-rotation deficit were different innonpitchers with and without a history of shoulder injury.
N Dominant hip extension and shoulder external rotation were associated with a history of shoulder injury in both pitchersand nonpitchers.
Shoulder injuries in baseball players are common.McFarland and Wasik1 reported that upper extrem-ity injuries were responsible for 75% of the total time
lost because of injury in a collegiate baseball population,with rotator cuff tendinitis cited as the most frequentinjury. Previous researchers2 have demonstrated significantstresses on the shoulder during the overhead throwingmotion, and it is generally believed that these stresses,combined with the innate repetition of the overhead armmotion in baseball, can lead to shoulder injuries.
Investigations2–6 of the biomechanics of the pitchingmotion have focused almost exclusively on the shoulderand elbow. However, the pitching motion is very complexand involves an elaborate transfer of energy throughoutthe entire body. For example, the scapula and trunk arebelieved to play an important role in overhead athletic
activity.7,8 Thus, large forces are not restricted to theshoulder alone but rather are imparted across all theanatomical joints involved in the throwing motion.
Forces at the shoulder may be greater in an athlete whois compensating for injuries or range-of-motion (ROM)restrictions at joints some distance from the shoulder (eg,lower back, hip, ankle).9 For instance, we hypothesize thatpoor extension (EXT) of the dominant hip (ie, the hip onthe same side as the throwing shoulder) during the maximalcocking or acceleration phases of the pitching motioncould cause the pitcher to increase the amount of shoulderexternal rotation (ER) in an attempt to achieve the desiredthrowing motion.
We further hypothesize that this phenomenon—com-monly referred to as ‘‘flying open’’ in baseball—couldincrease stress on the anterior shoulder structures and
Journal of Athletic Training 2010;45(2):191–197g by the National Athletic Trainers’ Association, Incwww.nata.org/jat
original research
Journal of Athletic Training 191
• Cross sectional study• Decreased non dominant Hip IR in non-pitchers with a h/o shoulder injury
(p=0.05)• Increased dominant hip EXT associated with shoulder injury in both
pitchers and non-pitchers• Decreased dominant shoulder ER in pitchers• Decreased dominant shoulder ER in non-pitchers

Femoroacetabular Impingement
�Pathologic hip structure effects the loading characteristics of the hip
�Loss of femoral head-offset (cam type lesion)
�Focal or global acetabularovercoverage (pincer type lesion)
�Combined impingement

Pincer Lesions
�Abnormal contact between acetabular rim and femur
�Acetabular Overcoverage– Cephalad Retroversion� Focal Rim Lesion
– Total Acetabular Retroversion
�Global Overcoverage– Profunda and Protrusio
�Labral degeneration and posteroinferior countrecouppattern

Cam Lesions
�Loss of femoral head and neck offset
� “Bump on the femur”
� Increased radius
�Cam Type lesions lead to shear forces against the acetabulum
�Chondral delamination and labraldetachment

Presentation of FAI
�Decreased Range of Motion
�Groin Pain
�Mechanical symptoms, stiffness, weakness, instability
�History of recurrent adductor strains/groin pulls
�History of Hip Flexor/Hamstring Strains/Athletic Pubalgia
�65% present with insidious onset of symptoms with no inciting event or trauma
� 30% present with symptoms after acute injury
Presentation of FAI
�Decreased Range of Motion
�Groin Pain
�Mechanical symptoms, stiffness, weakness, instability
�History of recurrent adductor strains/groin pulls
�History of Hip Flexor/Hamstring Strains/Athletic Pubalgia
�65% present with insidious onset of symptoms with no inciting event or trauma
� 30% present with symptoms after acute injury

Player Evaluation – Physical Exam
• Log Roll• Suggests intra-articular pathology
• C-sign• Hand cupped above greater trochanter gripping into the groin• Suggest intra-articular pathology
• Anterior Impingement Test• Flexion with internal rotation
• FABER• Anterior pain – tight anterior capsule/psoas impingment/interal snapping• Compare to contralateral side.

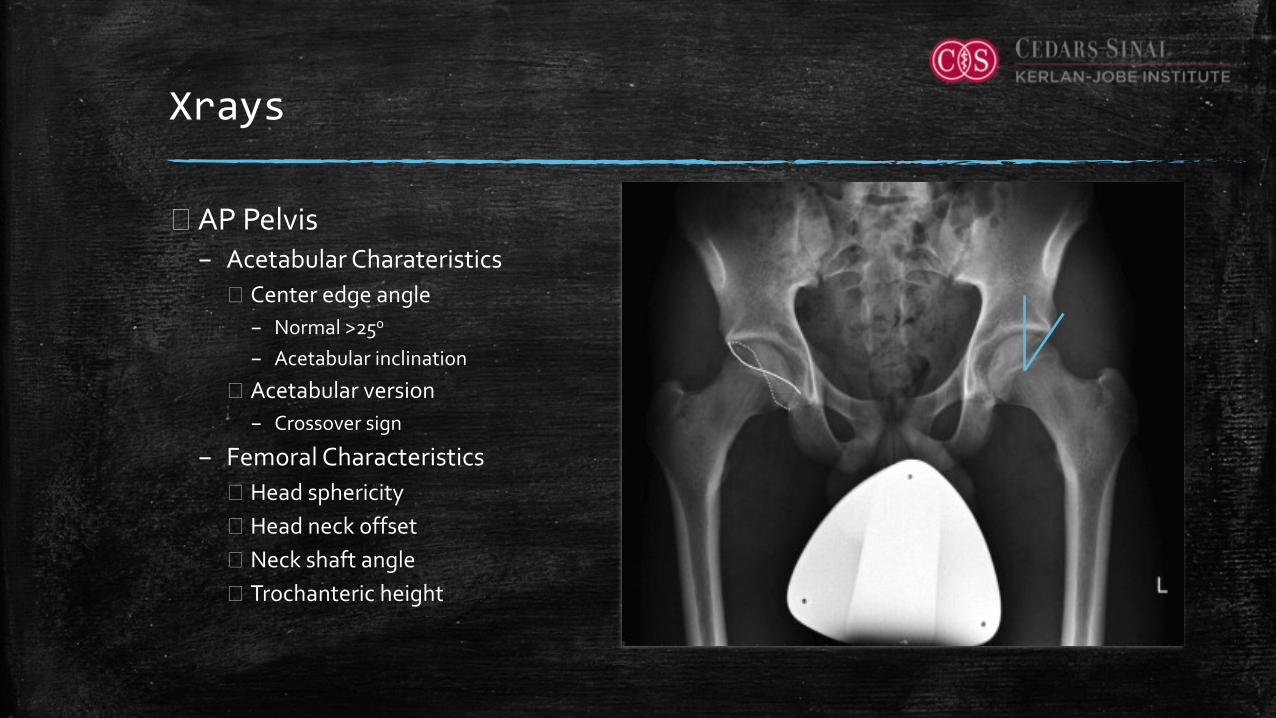
Xrays
�AP Pelvis– Acetabular Charateristics� Center edge angle
– Normal >25o
– Acetabular inclination
� Acetabular version– Crossover sign
– Femoral Characteristics� Head sphericity� Head neck offset� Neck shaft angle� Trochanteric height

Xrays – Modified Dunn Lateral
�Hip Flexed to 45o and 20o
abduction
�Evaluates CAM lesion in area of impingement
�Assess alpha angle– Normal <50o
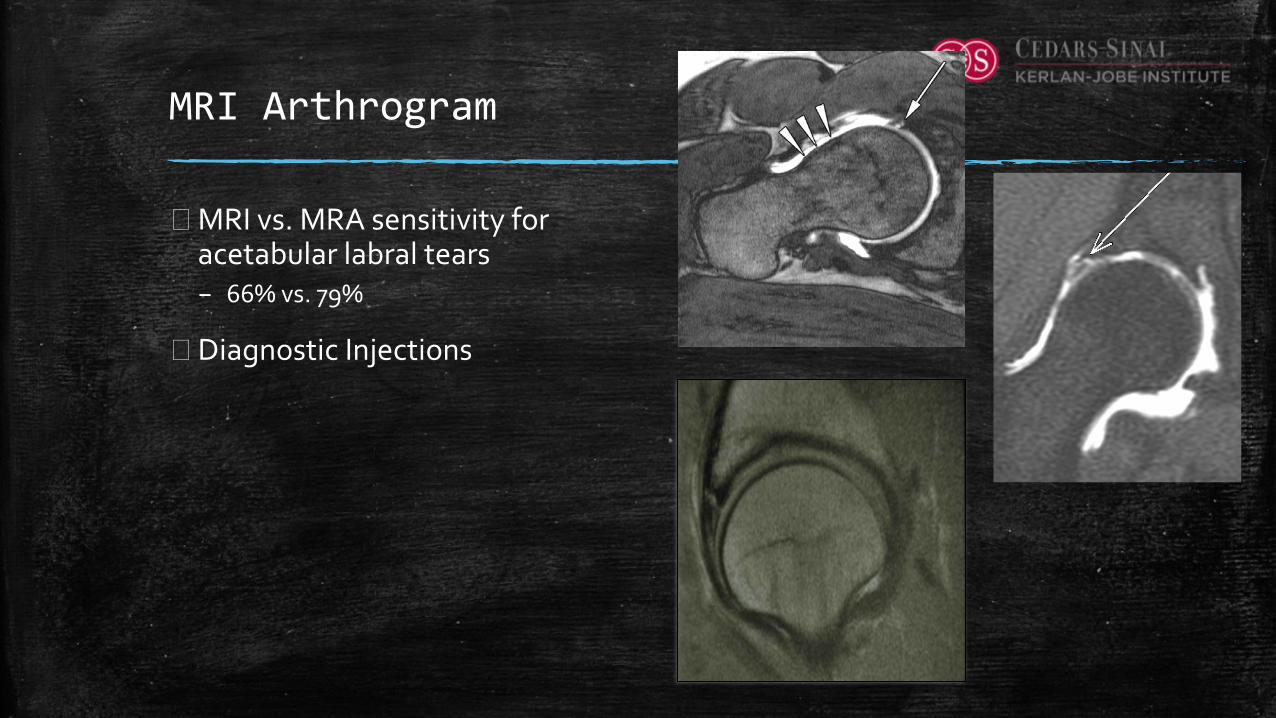
MRI Arthrogram
�MRI vs. MRA sensitivity for acetabular labral tears – 66% vs. 79%
�Diagnostic Injections

Nonoperative Treatment
�Activity Modification
�Anti-Inflammatory Medications
�Anesthetic/Corticosteroid/Biologic Injections –Diagnostic? Therapeutic?
�Abductor strengthening
�Hip-motion excercises
�Physical Therapy– Improve soft tissue mobility– Restore strength of abductors and peri-articular musculature– Improve neuromuscular control and postural balance
AVOID IMPINGEMENT TYPE STRECHES WHILE TRYING TO
OBTAIN GREATER ROM

Operative Treamtment
�Address all contributory mechanical factors causing impingement
�Secondarily address intra-articular pathology– Labral Tear
– Chondral delamination
�Open surgical dislocation– Requires trochanteric osteotomy� Ganz et al JBJS Br. 2001
�Hip Arthroscopy– Techniques have evolved to allow for effective and comprehensive treatment of
various impingement patterns
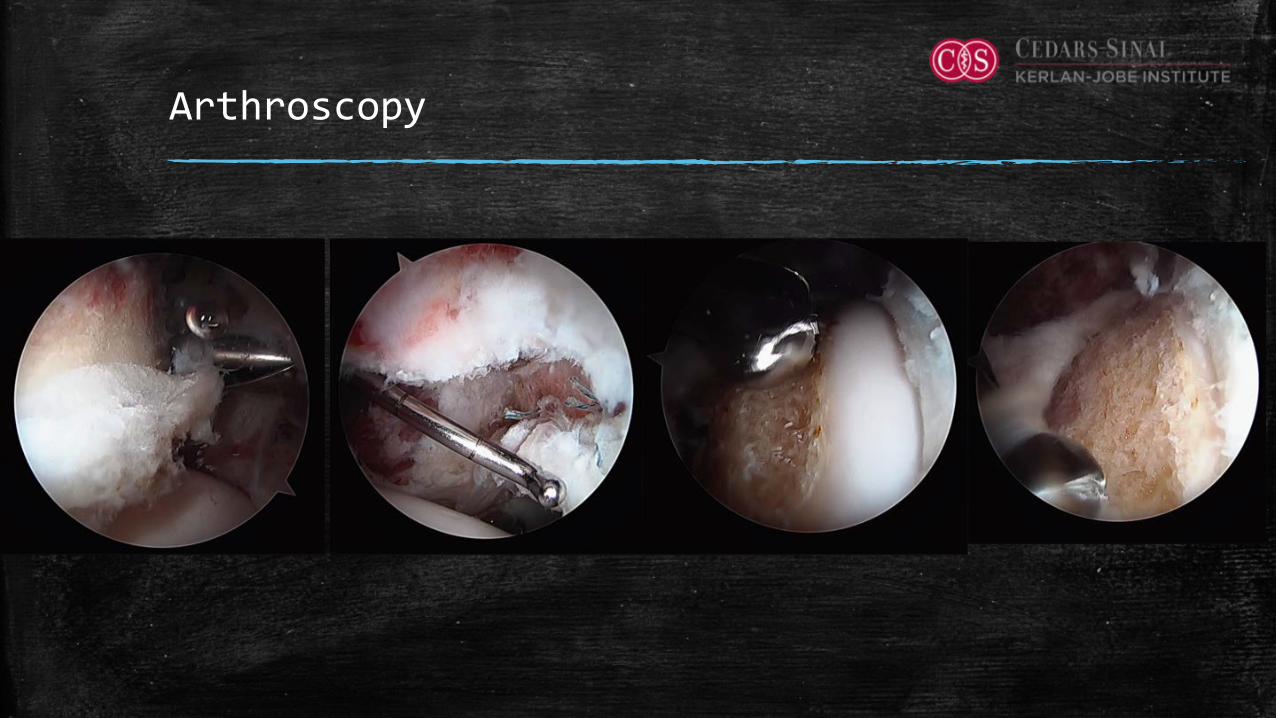
Arthroscopy
Outcomes
�Good to excellent outcomes – 70 – 90%
�87% - 93% of athletes return to sports
�82% return to same level of sport– Bizzini et al. Br J Sports Med 2015– Pillippon et al. Knee Surg Sports Traum Arthros 2007
Hip Arthroscopy in High-Level Baseball PlayersJ.W. Thomas Byrd, M.D., and Kay S. Jones, M.S.N., R.N.
Purpose: To report the results of hip arthroscopy among high-level baseball players as recorded by outcome scores andreturn to baseball. Methods: All patients undergoing hip arthroscopy were prospectively assessed with the modifiedHarris Hip Score. On review of all procedures performed over a 12-year period, 44 hips were identified among 41intercollegiate or professional baseball players who had achieved 2-year follow-up. Results: Among the 41 players,follow-up averaged 45 months (range, 24 to 120 months), with a mean age of 23 years (range, 18 to 34 years). There were23 collegiate (1 bilateral) and 18 professional (2 bilateral) baseball players, including 10 Major League Baseball players. Ofthe 8 Major League Baseball pitchers, 6 (75%) also underwent ulnar collateral ligament elbow surgery. Improvement inthe modified Harris Hip Score averaged 13 points (from 81 points preoperatively to 94 points postoperatively); a paired-samples t test determined that this mean improvement of 13 points was statistically significant (P < .001). Players returnedto baseball after 42 of 44 procedures (95%) at a mean of 4.3 months (range, 3 to 8 months), with 90% regaining theability to participate at their previous level of competition. There were no complications. Three players (1 bilateral) un-derwent repeat arthroscopy. Conclusions: This study supports the idea that arthroscopic treatment for a variety of hippathologies in high-level baseball players provides a successful return to sport and improvement in functional outcomescores. Level of Evidence: Level IV, therapeutic case series.
Hip disorders are increasingly recognized as asource of disability and dysfunction among ath-
letes.1 Femoroacetabular impingement has a particularproclivity for creating joint damage among young adultathletes.2 Compensatory disorders accompanying hippathology are also increasingly recognized as a sourceof disability.3
Acceleration during the pitching motion is precededby a stride toward home plate.4 Initial velocity, devel-oped in the lower extremities, is then transformedthrough the hips into rotational velocity of the trunkand is ultimately delivered to the upper extremity,culminating in ball speed. Similarly, during batting,velocity is initiated from the step of the lower extrem-ities, transformed through the hips to trunk rotation,culminating in bat speed through the upper
extremities.5 In baseball the hip is part of the complexkinematic linkage for both pitching and batting.5-11
The purpose of this study was to report the results ofhip arthroscopy among high-level baseball players asrecorded by outcome scores and return to baseball. Wehypothesized that hip disorders may be problematic inhigh-level baseball players, and some may potentiallybenefit from arthroscopic intervention as reflected byimproved outcome scores.
MethodsSince 1993, all patients undergoing hip arthroscopy at
our institution by a single surgeon (J.W.T.B.) have beenprospectively assessed using the modified Harris HipScore preoperatively and then postoperatively at 3, 12,24, 60, and 120 months.12 From this prospectivelygathered database, we selected all athletes whocompeted in baseball at the intercollegiate or profes-sional levels and had achieved a minimum of 2 years’follow-up. All such athletes were included, and therewere no exclusion criteria. This group of baseballplayers represents the substance of this report. The dataobtained and presented in this article have been gran-ted exemption status by the institutional review board.The indications for arthroscopywere clinicalfindings of
joint pathology amenable to arthroscopic interventionthat had failed conservative treatment, which variouslyincluded training modifications, rehabilitation, oral
From Nashville Sports Medicine Foundation, Nashville, Tennessee, U.S.A.The authors report the following potential conflict of interest or source of
funding: During the study period, Nashville Sports Medicine Foundationreceived research support (a restricted grant) from Smith & Nephew Endos-copy. J.W.T.B. receives support from Smith & Nephew and A3 Surgical. K.S.J.receives support from Smith & Nephew.
Received June 24, 2014; accepted March 5, 2015.Address correspondence to J.W. Thomas Byrd, M.D., Nashville Sports
Medicine Foundation, 2011 Church St, Ste 100, Nashville, TN 37203, U.S.A.E-mail: [email protected]
! 2015 by the Arthroscopy Association of North America0749-8063/14529/$36.00http://dx.doi.org/10.1016/j.arthro.2015.03.002
Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol -, No - (Month), 2015: pp 1-4 1
Hip Arthroscopy in High-Level Baseball PlayersJ.W. Thomas Byrd, M.D., and Kay S. Jones, M.S.N., R.N.
Purpose: To report the results of hip arthroscopy among high-level baseball players as recorded by outcome scores andreturn to baseball. Methods: All patients undergoing hip arthroscopy were prospectively assessed with the modifiedHarris Hip Score. On review of all procedures performed over a 12-year period, 44 hips were identified among 41intercollegiate or professional baseball players who had achieved 2-year follow-up. Results: Among the 41 players,follow-up averaged 45 months (range, 24 to 120 months), with a mean age of 23 years (range, 18 to 34 years). There were23 collegiate (1 bilateral) and 18 professional (2 bilateral) baseball players, including 10 Major League Baseball players. Ofthe 8 Major League Baseball pitchers, 6 (75%) also underwent ulnar collateral ligament elbow surgery. Improvement inthe modified Harris Hip Score averaged 13 points (from 81 points preoperatively to 94 points postoperatively); a paired-samples t test determined that this mean improvement of 13 points was statistically significant (P < .001). Players returnedto baseball after 42 of 44 procedures (95%) at a mean of 4.3 months (range, 3 to 8 months), with 90% regaining theability to participate at their previous level of competition. There were no complications. Three players (1 bilateral) un-derwent repeat arthroscopy. Conclusions: This study supports the idea that arthroscopic treatment for a variety of hippathologies in high-level baseball players provides a successful return to sport and improvement in functional outcomescores. Level of Evidence: Level IV, therapeutic case series.
Hip disorders are increasingly recognized as asource of disability and dysfunction among ath-
letes.1 Femoroacetabular impingement has a particularproclivity for creating joint damage among young adultathletes.2 Compensatory disorders accompanying hippathology are also increasingly recognized as a sourceof disability.3
Acceleration during the pitching motion is precededby a stride toward home plate.4 Initial velocity, devel-oped in the lower extremities, is then transformedthrough the hips into rotational velocity of the trunkand is ultimately delivered to the upper extremity,culminating in ball speed. Similarly, during batting,velocity is initiated from the step of the lower extrem-ities, transformed through the hips to trunk rotation,culminating in bat speed through the upper
extremities.5 In baseball the hip is part of the complexkinematic linkage for both pitching and batting.5-11
The purpose of this study was to report the results ofhip arthroscopy among high-level baseball players asrecorded by outcome scores and return to baseball. Wehypothesized that hip disorders may be problematic inhigh-level baseball players, and some may potentiallybenefit from arthroscopic intervention as reflected byimproved outcome scores.
MethodsSince 1993, all patients undergoing hip arthroscopy at
our institution by a single surgeon (J.W.T.B.) have beenprospectively assessed using the modified Harris HipScore preoperatively and then postoperatively at 3, 12,24, 60, and 120 months.12 From this prospectivelygathered database, we selected all athletes whocompeted in baseball at the intercollegiate or profes-sional levels and had achieved a minimum of 2 years’follow-up. All such athletes were included, and therewere no exclusion criteria. This group of baseballplayers represents the substance of this report. The dataobtained and presented in this article have been gran-ted exemption status by the institutional review board.The indications for arthroscopywere clinicalfindings of
joint pathology amenable to arthroscopic interventionthat had failed conservative treatment, which variouslyincluded training modifications, rehabilitation, oral
From Nashville Sports Medicine Foundation, Nashville, Tennessee, U.S.A.The authors report the following potential conflict of interest or source of
funding: During the study period, Nashville Sports Medicine Foundationreceived research support (a restricted grant) from Smith & Nephew Endos-copy. J.W.T.B. receives support from Smith & Nephew and A3 Surgical. K.S.J.receives support from Smith & Nephew.
Received June 24, 2014; accepted March 5, 2015.Address correspondence to J.W. Thomas Byrd, M.D., Nashville Sports
Medicine Foundation, 2011 Church St, Ste 100, Nashville, TN 37203, U.S.A.E-mail: [email protected]
! 2015 by the Arthroscopy Association of North America0749-8063/14529/$36.00http://dx.doi.org/10.1016/j.arthro.2015.03.002
Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol -, No - (Month), 2015: pp 1-4 1
• 44 Hips in 41 Athletes (college and professional)• Pitchers – push leg involved in 12, stride leg in 6• Position Players – batting front leg in 8, back leg in 12, both in 2
• mHHS: 81 pre op to 94 post op (o<.001)
• 42/44 returned to baseball (95%) at mean 4.3 months (3-8mo)• 90% returned to previous level of competition

Conclusions
�Hip pathology is prevalent in athletes of all sports including baseball– Kinetic Linkage– Increased prevalence of FAI in athletes
�Majority of hip pathology in baseball presents as extra-articular soft tissue injuries
�Femoroacetabular Impingement likely predisposes athletes to both intra-articular as well as extra-articular injuries– “Cam Avoidance”
� If required, operative treatment is highly successful in pain relief and return to sport

Thank You