february 2007 surgical site pain management improving outcomes
TRANSCRIPT

February 2007
Surgical Site Pain Management
Improving Outcomes

ObjectivesAt the end of the presentation, you will be able to:
Discuss current pain theories. Differentiate various types of pain. List key components of a pain management
program. Review the TJC pain standards. Describe the role of a surgical site pain
management system. Describe outcomes related to surgical site
pain management systems.

What is Pain?
Pain is a complex phenomenon derived from sensory stimuli or neurologic injury and modified by individual memory, expectations, and emotions.
Sternbach RA, ed. The Psychology of Pain. 1978. p 223-39.

Pain: Subjective Component
“whatever the experiencing person says it is and exists whenever he says it does.”
McCaffery, M. Nursing practice theories related to cognition, bodily pain, and man-environment interactions. 1968, Pg 95.

Understanding Pain Pain is different for every person. Pain is part of a historical and cultural
framework. Everyone’s experience and perceptions of
pain will differ.

Neurophysiology Of Pain Stimulation of nerve receptors for pain
(nociceptors) - free nerve endings in almost all tissue types
Mechanical, chemical, thermal sources Once stimulated, impulse travels to
spinal cord and brain Impulse becomes experience of pain

February 2007

Classification Of Pain
Acute
Chronic
Referred

Acute Pain One-dimensional
Underlying cause Acute injury, disease or
surgery. Sudden onset, defined
area, quick response Treatment goal:
Eradication of underlying disease Analgesics used as adjunctive therapy
Chronic Pain Multidimensional Persists at least one month beyond usual course Worsened by physical, psychological, social factors Types:
Chronic condition Osteoarthritis Cancer
Chronic pain from acute source Post-mastectomy chronic pain syndrome (PMCPS) Post-thoracotomy chronic pain syndrome (PTCPS)
Acute injury that results in chronic pain (back injury) No discernable cause

Referred Pain Referred pain occurs when pain
affecting one of the visceral organs is referred to the external body, not necessarily in the same location.

Are We Undertreating Pain? 217 adults in a university teaching hospital
61% pain of 7-10 during past 24 hours 49% pain of 4-10 “right now” 20% pain of 4-10 despite analgesics
Despite efforts to improve pain management, no change in patients pain ratings
Ward SE, Gordon D. Application of the American Pain Society quality assurance standards Pain 1994 Mar;56(3):299-306

Postoperative Pain Experience
80% of patients experienced acute pain after surgery
Most patients had moderate, severe or extreme pain
Ambulatory patients experienced more pain after discharge than when they were in facilities
Apfelbaum JS, et al. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be
undermanaged. Anesth Analg 2003;97:534-40.
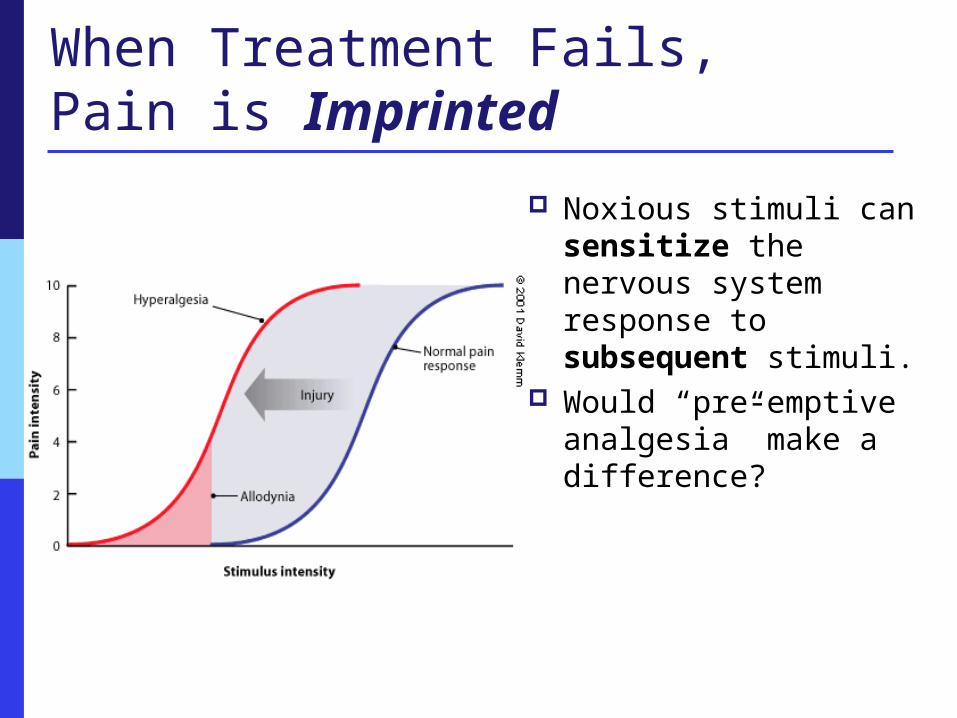
When Treatment Fails,Pain is Imprinted
Noxious stimuli can sensitize the nervous system response to subsequent stimuli.
Would “pre-emptive analgesia” make a difference?

Under-Treated Acute Pain Side Effects
Increased risk of thromboembolism Catecholamine secretion
Vasoconstriction, Increased heart rate Increased myocardial oxygen
consumption Decreased oxygen delivery Increased cardiac morbidity Potential increased risk of infection
Potentially Serious
Complications
Tetzlaff JE. Cardiovascular consequences of severe acute pain. Practical pain management Mar/Apr 2004;11-13.
American Pain SocietyGuidelines for Assessment
PAIN – The Fifth Vital Sign
In 1995 the American Pain Society (APS) created this phrase to elevate awareness of pain treatment among health care professionals.

TJC Standards
Addresses the assessment and management of pain Recognize the right of patients to appropriate
assessment and management of pain Screen patients for pain during their initial
assessment and, when critically required, during outgoing periodic re-assessments
Educate patients suffering from pain & their families about pain management

Establish Institutional Nursing Protocol Acknowledge pain is real. Respect patient’s reactions and attitudes. Inform patients about pain and therapies. Administer pain medication appropriately. Explain actions and side effects. Decrease noxious stimuli. Document treatment and patient response.

Assessing Pain VAS = Visual Analogue Scale VRS = Visual Response Scale 0-10 scale 10 = worst pain imaginable 0-100 scale Wong-Baker Faces Scale
Assessment of Pain Location
Where? Does it radiate? Pattern
Does it occur at a special time? Onset
When did it begin?Was it sudden or gradual?

Assessment of Pain
Type Dull, sharp, aching, stabbing, burning
Intensity: How strong? How long does it last? Does it vary?
Causative Factors: What brings on the pain? What makes it worse?

Evolution of Pain Control
OpioidsGeneral Anesthesia
Local Anesthesia
Regional Anesthesia
Epidural/
Spinal anesthesia
Acute Pain - Control Methods Pharmacological
Opioid Non-Opioid Local anesthetics
Non-Pharmacological Change/Adjust Position Diversion Activities Relaxation Techniques Meditation Acupuncture/Acupressure Heat, cold, massage Hypnosis

Opioids
Mainstay of pain management Morphine Dilaudid Fentanyl (IV, Transdermal) Demerol Oral opioids
Percocet, Vicodin, Lortab, Oxycontin
PCA vs intermittent
injection

Opioid Side Effects
Nausea and vomiting Ileus/Constipation Urinary retention Respiratory depression Apnea Sedation Confusion Tolerance Restricted Ambulation
Longer Hospital Stays
&
Increased Costs

Opioids and Surgical Infections
Is there a link? Maybe
Two studies in particularHorn et al Surgical Infections 2002;3(2):109-18. Alverdy et al Surgical Infection Society Annual Meeting, La Jolla, CA 2006
PCA and SSI Chart review of 515 randomly selected
patients who had major rectal or intestinal surgery.
214 had PCA Results: Use of PCA significantly
associated with increased in-hospital surgical site infection (10.7% vs 4.0%)
Possibly due to suppression of natural killer cells causing immune compromise.
Horn SD et al. Association between patient-controlled analgesia pump use and postoperative surgical site infection in intestinal surgery patients. Surgical Infections 2002;3(2):109-18.

Non-Opioid Analgesics
NSAIDs Aspirin, ibuprofen, naproxen, acetominophen Toradol® ketorolac (injection)
Side Effects: Gastrointestinal distress, clotting disorders, dependence, kidney failure (ibuprofen) liver failure (acetominophen)
COX-2 Inhibitors Vioxx® - rofecoxib Bextra® - valdecoxib Celebrex® - celecoxib
Less gastrointestinal and bleeding issues
Not Available

The abolition of painful impulses from any region or regions of the body by temporarily interrupting the sensory nerve conductivity with local anesthetics.
Motor function may or may not be involved.
The patient does not lose consciousness.
Regional-Local Anesthesia

Types of Regional Anesthesia Peripheral nerve block
Types of Procedures Ortho: Upper, Lower & Spine (including trauma Rib & Hip
Fractures) General: Mastectomy & Abdominal Procedures CV/CT & Cath Lab: VATs, Thoracotomies, TAVR OB/GYN: C-Sections
Single injection or continuous infusion of local anesthetic near nerve
Performed by anesthesiologist
Surgical site Can be used for multiple types of surgery Catheter placed by surgeon Can be incisional or near incision

Surgical Site Pain Management
A continuous, regulated flow of local anesthetic through a fenestrated antimicrobial Soaker® catheter directly into or near an intra-operative site
Soaker® catheters provide wider, more even distribution of local to incisional area
Portable, easy-to-use, disposable for outpatient or inpatient
Therapy continues up to five days

Surgical Site Pain Management Procedure Landscape
Spine ALIF, PILF, TLIF Iliac Crest
General Colectomy/Ventral
Hernia Hemorrhoidectomy
CV/CT Thoracotomy Open Heart/AAA Vascular Amputation
Bariatric Open/Laparoscopic
Plastic Surgery Breast Surgery Abdominoplasty
Urology Prostatectomy Nephrectomy/Kidney
transplants OB/GYN
Hysterectomy/Oncology C-Section

Local Anesthetics
Bupivacaine (Marcaine®, Sensorcaine®) 0.25% or 0.5%
Lidocaine (Xylocaine®) 0.5% or 1%
Ropivacaine (Naropin™) 0.2%, 0.1% or 0.5%
Levobupivacaine (Chirocaine®) 0.25% or 0.5%
Avoid local with epinephrine!!!

Filling the Pump USP 797 Pharmaceutical
Compounding – Sterile Preparations Prior January 2008: Pumps
were filled anywhere & everywhere, most common was the Back Table in the OR
HIGH RISK Post January 2008:Filled in
Pharmacy under a hood by a trained Personnel OR by a Third Party Vendor and shipped to the Hospital’s Pharmacy
LOW RISK

Surgical Site Pumps

Benefits of a Soaker™ Catheter for Surgical Site
Infuses local anesthetic over a broader area compared to point-source catheters
Greater versatility in catheter placement
More even distribution of medication
5”
2.5”
Standard
24 holes
11 holes
3 holes
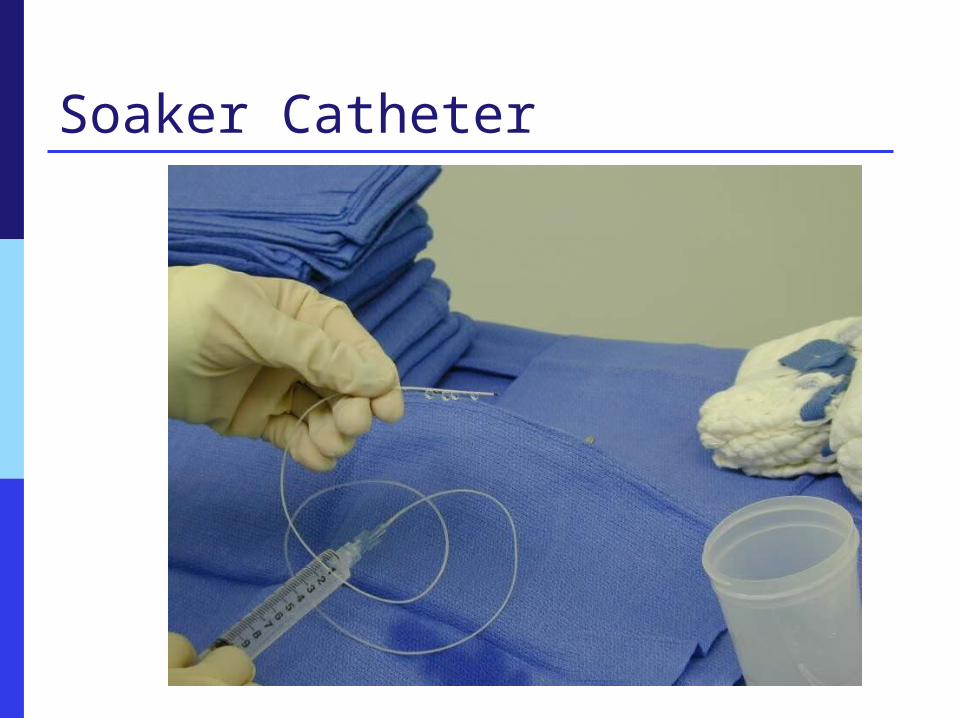
Soaker Catheter
New Techniques: Tunneling Benefits:
Catheter(s)are placed deeper and closer to key nerves May eliminate the need to close a separate layer –
peritoneum Minimizes risk of nerve damage and bleeding Blunt tunneling minimizes needle stick risk to the
surgeon Less leakage Better pain results because of proximity to
innervations Catheter are placed further away from the incision
(fear of fluid build up or infection) Catheters can now be placed pre-incision

Tunneler

Tunneling Through Rectus Sheath The catheter is
placed in the pre-peritoneal space using a tunneler.
This places the catheter near larger nerves and away from the incision.

Demonstrated Clinical Evidence Many published and presented studies Typical Results
1 to 3 day length of stay reduction 40-70% reduction in narcotics 8-30% reduction in treatment costs 90%+ patient satisfaction Infection rates less than national averages Substantial reductions in pain scores

Clinical Research Results
CV/CT Surgeries: Decrease in PCA requirements by 63% Length of stay reduced PACU time reduced 12% Significant decrease in pain No infections Serum levels <30% of toxicity Decrease in costs by 8% Increase in lung volume – spirometry
White PF, et al. Anesthesiology 2003; 99(4): 918-23Dowling R, et al. J Thoracic CV Surgery 2003; 126(5): 1271-8.

Paravertebral Approach
Can be approached
either Anterior or Posterior

Extrapleural Placement

MastectomyNarcotic Use
0
10
20
30
40
50
60
70
80
No Post op Narcotics No Narcotics > Day 1
% o
f P
atie
nts
Placebo ON Q
Morrison JE, Jacobs VR. Zentralblatt fur Gynakologie 2003;125:17-22.

Mastectomy

Lumbar Laminectomy & Fusion Paraspinal Muscle of the
back Multifidus Longissimu Interspinous Intertransverse


Lumbar Results
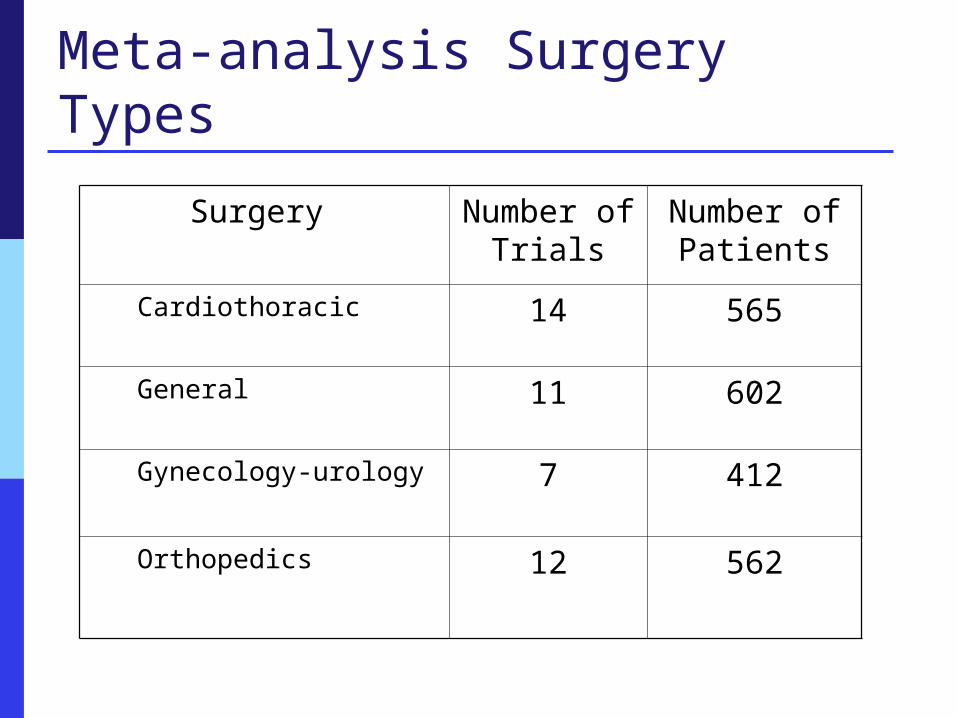
Meta-analysis Surgery Types
Surgery Number of Trials
Number of Patients
Cardiothoracic 14 565
General 11 602
Gynecology-urology 7 412
Orthopedics 12 562

Meta-analysis of Wound Catheters
Meta-analysis of 44 randomized controlled trials (RCTs)
Published in peer-reviewed journal. 2141 patients Studies used a variety of infusion devices
and methods. Studies covered multiple types of
surgeries. Studies published during 1983 - 2006
Liu SS, Richman JM, Thirlby RC, Wu CL. J Am Coll Surg 2006; 203(6): 914-32.
Clinical Research Results Orthopedic Surgery
Total Joint Replacement Decreased length of stay Decreased nausea and vomiting Earlier return to physical therapy More abmulatory
Rotator Cuff-ACL Repair Earlier return to physical therapy Decreased narcotic use
Gottschalk A et al. Anesth Analg 2003;97:1086-91.
Ford PJ, Slavagno RT, Pianta T, Dine A. Presented at NAON 2004

Total Joint Replacement
0
0.5
1
1.5
2
2.5
1997 1998 1999 2000 2001 2002 2003
Yearp<0.05 Years 2001-2003 compared to previous
Mea
n d
ays
Ford PJ, Slavagno RT, Pianta T, Dine A. Presented at NAON 2004.
Postop Nausea and Vomiting
Began using therapy

Meta-analysis Results Pain scores at rest: lower in all groups
combined (p< 0.001) 10mm reduction
Pain scores with activity: lower in all groups combined (p < 0.001) 22 mm reduction
Opioid rescue medication: Fewer patients required in all groups (p< 0.001) 41% vs. 66%
Total opioid required: less in all groups combined (p< 0.001) reduction of 11 mg/day

Results continued
Postoperative nausea and vomiting (PONV): less in all groups combined (p< 0.001) 24% vs. 40%
Patient satisfaction better in all groups combined (p< 0.007) 43% vs. 13% had excellent satisfaction
No local anesthetic toxicity Infection rates 0.7% in active group and
1.2% in control group

Potential Cost Savings
Narcotic reduction savings 50% on average reduction in narcotics Pharmacy charges to fill PCA orders
Narcotic complication treatments Anti-emetic medications reduction Elimination of foley catheter
Decrease UTI Reduction in Benadryl
Minimized ICU and PACU times $800 per hour

Potential Cost Savings Minimize or eliminate electronic pump usage
$20-50/day with supplies and labor to maintain Minimize nurse labor to teach, monitor and
maintain narcotic delivery Viscusi Study
$1240 cost for 3 days of PCA Cost Drivers are time spent – not drugs or
devices
Viscusi E, et al. A multidimensional model for evaluating the key cost drivers associated with perioperative pain.

Postop Nursing Care Assess surgical site pain.
Distinguish from other sources of pain. Provide adjunct analgesia prn.- THIS IS A MULTIMODAL THERAPY
Check that clamps are open and tubing not kinked. Verify label(s) Verify flow rate are set properly OR secure flow
restrictor (if present) to skin. Check pump for remaining drug. Check site for redness, drainage, intact dressing. Observe for signs of local anesthetic toxicity. When removed, check for intact tip.

REMEMBER…Safety is Key! Assessment
Fall Risk Pts who have lower extremity surgery are High Fall
Risk (with or without a RA) Do pts have the proper precautions (knee
stabilizers)?
Does It Make A Difference?? Reduced time in PACU Reduced time to discharge readiness Reduced PONV Reduced concerns for opioid induced
respiratory depression Better pain management w/ fewer side
effects Improved pain scores Great satisfaction

HCAHPS

HCAHPS
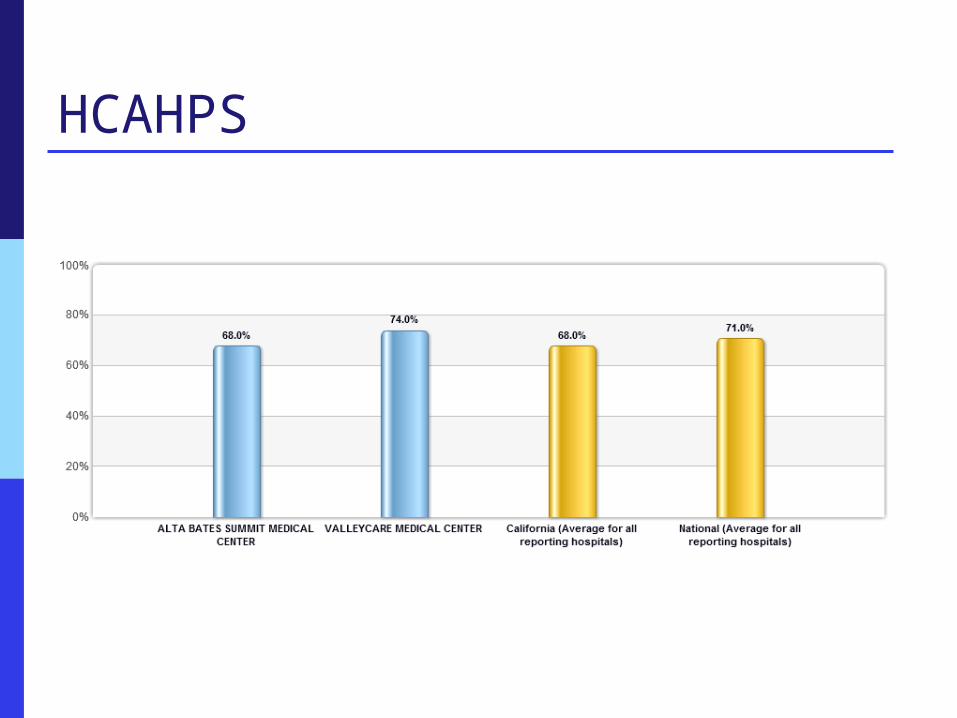
HCAHPS

Why Regional Anesthesia???
Patient Decreased narcotic
usage = less side effects
Earlier ambulation Shortened recovery
time Less incidence of
breakthrough pain Decreased length of
stay Better patient outcomes Higher patient
satisfaction
Hospital Decreased PONV Increase through put Controlled pain =
happier pts = better experience
Higher HCAHP Scores Lower readmissions
rates

Summary
New modalities exist that improve traditional pain management by providing site-specific, non-narcotic relief of pain.
Undertreatment of acute pain persists despite decades of efforts to improve clinician knowledge.

Thanks for your attention!
Questions?