feasibility and efficacy of a “move and learn” physical ... and efficacy of a “move ... the...
TRANSCRIPT
88
Journal of Physical Activity and Health, 2008, 5, 88-103 © 2008 Human Kinetics, Inc.
Trost is with the Dept of Nutrition and Exercise Sciences, Oregon State University, Corvallis, OR 97331. Fees is with the Dept of Family Studies and Human Services, and Dzewaltowski the Dept of Kinesiology, Kansas State University, Manhattan, KS 65606.
Feasibility and Efficacy of a “Move and Learn” Physical Activity Curriculum
in Preschool Children
Stewart G. Trost, Bronwyn Fees, and David Dzewaltowski
Background: This study evaluated the effect of a “move and learn” curriculum on physical activity (PA) in 3- to 5-year-olds attending a half-day preschool program. Methods: Classrooms were randomized to receive an 8-week move and learn pro-gram or complete their usual curriculum. In intervention classes, opportunities for PA were integrated into all aspects of the preschool curriculum, including math, science, language arts, and nutrition education. Changes in PA were measured objectively using accelerometry and direct observation. Results: At the completion of the 8-week intervention, children completing the move and learn curriculum exhibited significantly higher levels of classroom moderate-to-vigorous physical activity (MVPA) than children completing their usual curriculum. Significant dif-ferences were also noted for classroom VPA over the final 2 weeks. Conclusion: The results suggest that integrating movement experiences into an existing early childhood curriculum is feasible and a potentially effective strategy for promoting PA in preschool children.
Keywords: early childhood, intervention, exercise, movement, obesity
The prevalence of overweight among US children and adolescents has increased dramatically since the 1970s. Data from the 1999–2002 National Health and Nutri-tion Examination Survey indicate that 16% of young people between the ages of 6 and 19 years are overweight, an absolute increase of approximately 10%.1 Preschool-age children are also affected by the obesity epidemic. Data from the most recent National Health and Nutrition Examination Survey indicate that just over 10% of US children between the ages of 2 and 5 are overweight, with a fur-ther 12% considered to be at-risk for overweight.1,2 The rising trend in overweight among preschool children represents a critical public health problem. Overweight preschoolers are at significantly increased risk for child and adolescent obesity,3 and they are more likely than their nonoverweight counterparts to experience significant short- and long-term health problems such as hyperlipidemia, hypertension, insulin resistance, respiratory problems, and orthopedic complications.4,5 In addition, the adverse social consequences of childhood obesity might have long-lasting effects on psychological well-being and economic mobility.5

Promoting Physical Activity in Preschool Children 89
Lack of physical activity is an important contributing factor to the development and maintenance of childhood overweight. Overweight preschool children have been shown to be less active than their nonoverweight counterparts,6 and long-term prospective studies have shown physical activity during early childhood to be either protective of accelerated weight gain or inversely associated with increases in adiposity.7-10 Despite the importance of regular physical activity, however, the activity patterns of preschool children are not well understood. Children in the 3- to 5-year-old age range are traditionally viewed as highly active; however, objective-monitoring studies conducted in the United States and the United Kingdom suggest that preschool-age children engage in relatively little moderate- to vigorous-intensity physical activity.11,12 These findings, taken alongside the continued rise in the prevalence of overweight among preschool children, highlight the need for effective policies and programs to promote physical activity in 3- to 5-year-old children.
Early childhood education programs are an ideal setting to promote physical activity in young children. In the United States, 56% of all children between the ages of 3 and 5 attend preschools or similar early childhood education centers, most of them spending 4 or more hours per day, 5 days per week in those settings.13 Unfortunately, very little is known about how to effectively promote physical activity in preschool settings. Physical educators and clinicians have developed a number of programs and resources to promote physical fitness and fundamental movement skills in preschoolers.14,15 Because such programs are stand alone and must be added to an increasingly crowded early childhood curriculum, however, their implementation has been limited and their adoption not widespread. A more realistic and potentially more sustainable approach to promoting physical activity that has not been systematically evaluated in the scientific peer-reviewed literature, is to integrate developmentally appropriate movement experiences into the existing early childhood curriculum.16 By incorporating movement experiences into tradi-tional learning areas such as mathematics, science, and language arts, integrated physical activity curricula overcome the traditional implementation and adoption barriers associated with stand-alone physical activity programs. Moreover, there is evidence that integrating movement into everyday learning experiences can enhance learning outcomes in young children.17
The purpose of this study was to assess the effect of an integrated move and learn curriculum on objectively measured physical activity behavior in 3- to 5-year-old children attending a half-day preschool program. We hypothesized that preschoolers exposed to the move and learn curriculum would exhibit significantly greater classroom moderate-to-vigorous physical activity (MVPA) than preschool-ers completing their normal classroom curriculum.
Methods
Setting
The study was conducted at a single child-care center and involved children enrolled in an inclusive half-day preschool program. The program was run in collaboration with the local school district and serviced 3- to 5-year-olds residing within the community of Manhattan, KS. The study was conducted in 2 classrooms licensed for 12 children with morning and afternoon class groups (4 class groups in total). Each session was 2.5 hours in duration with morning and afternoon sessions offered 4 days per week.

90 Trost, Fees, and Dzewaltowski
Recruitment
All parents and caregivers were provided with a letter of introduction describing the study and an informed consent packet. Parents were asked to sign and complete the written informed consent document and return it to a designated drop box located inside each classroom. The study was approved by the child-care center advisory committee and the University’s Institutional Review Board.
Study Design
The study was conducted over a 10-week period, with the first 2 weeks serving as a baseline assessment period. After baseline assessments had been completed, the classrooms were randomized to the intervention condition or the usual care control condition. Children attending the morning or afternoon session in the intervention classroom completed an 8-week move and learn curriculum, and children attending the morning or afternoon session in the control classroom completed their usual early childhood curriculum.
Intervention Overview
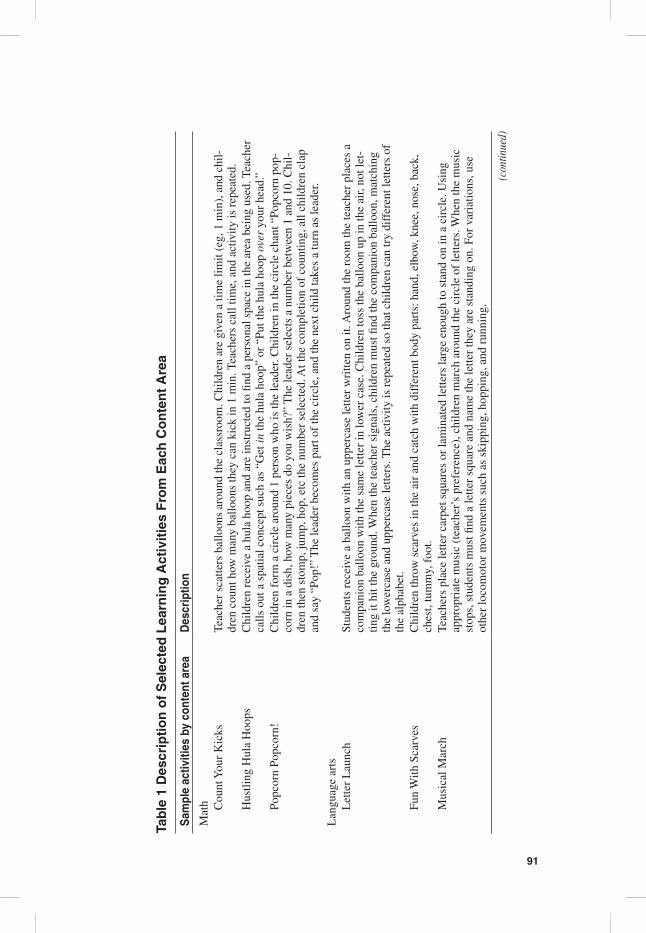
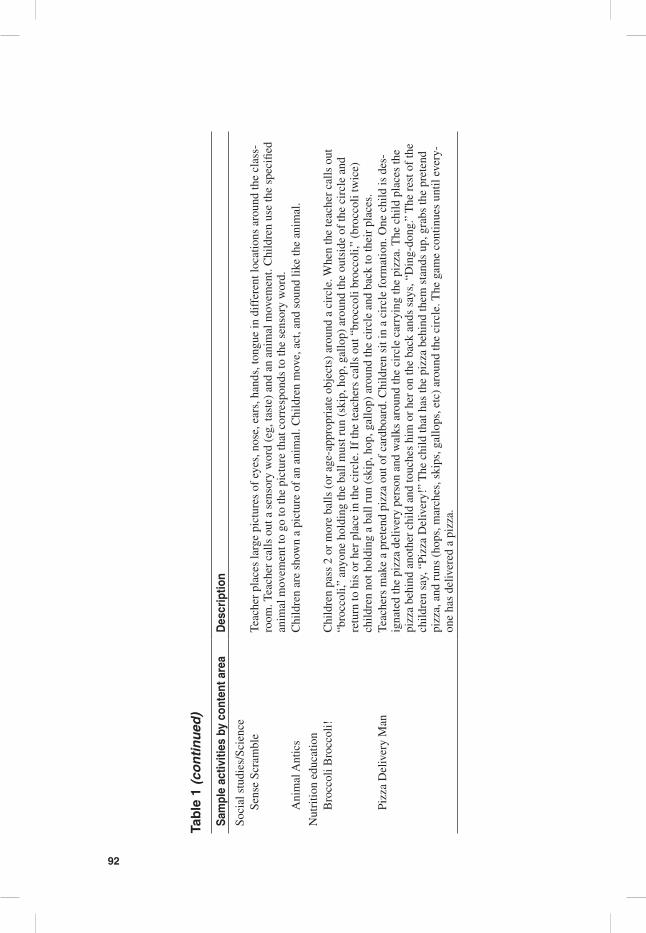
The primary aim of the intervention was to increase the amount of MVPA performed while attending preschool. To achieve this aim, opportunities for physical activity were integrated into all aspects of the preschool curriculum, including math, social studies and science, language arts, and nutrition education. Lead teachers selected activities adapted from Lets Move, Learn, and Have Fun!, the physical activity com-ponent of Nutrition: Good for You!, a comprehensive nutrition and physical activity curriculum for preschool children developed by the Kansas Nutrition Network and Kansas State University Research and Extension.18,19 Additional activities were adapted from activities developed for Class Act—an integrated physical activity curriculum developed for the Kansas Department of Health and Environment.20 Activities included counting and number-recognition games using scarves and balloons and music-based chasing and imagination games addressing concepts in language arts, science, social studies, and nutrition education (eg, letter launch, musical march, animal antics, broccoli broccoli, and pizza delivery man). Table 1 provides a detailed description of representative activities from each content area. At a minimum, teachers were required to include 2 move and learn curriculum activities lasting 10 minutes or longer in each 2.5-hour session. Activities were typically repeated several times throughout the week.
Before implementation, teachers and staff in the intervention classroom par-ticipated in a single 3-hour training session conducted by 1 of the authors of the curriculum. The training consisted of an introduction and discussion of the cur-riculum objectives, demonstration of activities, and practice of the move and learn activities. Teachers were also given a video demonstrating the different activities. The training session was typical of that given to center- and home-based child-care providers throughout the state of Kansas.
91
Tab
le 1
Des
crip
tio
n o
f S
elec
ted
Lea
rnin
g A
ctiv
itie
s F
rom
Eac
h C
on
ten
t A
rea
Sam
ple
activ
ities
by
cont
ent a
rea
Des
crip
tion
Mat
h
Cou
nt Y
our
Kic
ksTe
ache
r sc
atte
rs b
allo
ons
arou
nd th
e cl
assr
oom
. Chi
ldre
n ar
e gi
ven
a tim
e lim
it (e
g, 1
min
), a
nd c
hil-
dren
cou
nt h
ow m
any
ballo
ons
they
can
kic
k in
1 m
in. T
each
ers
call
time,
and
act
ivity
is r
epea
ted.
Hus
tling
Hul
a H
oops
Chi
ldre
n re
ceiv
e a
hula
hoo
p an
d ar
e in
stru
cted
to fi
nd a
per
sona
l spa
ce in
the
area
bei
ng u
sed.
Tea
cher
ca
lls o
ut a
spa
tial c
once
pt s
uch
as “
Get
in th
e hu
la h
oop”
or
“Put
the
hula
hoo
p ov
er y
our
head
.”
Popc
orn
Popc
orn!
Chi
ldre
n fo
rm a
cir
cle
arou
nd 1
per
son
who
is th
e le
ader
. Chi
ldre
n in
the
circ
le c
hant
“Po
pcor
n po
p-co
rn in
a d
ish,
how
man
y pi
eces
do
you
wis
h?”
The
lead
er s
elec
ts a
num
ber
betw
een
1 an
d 10
. Chi
l-dr
en th
en s
tom
p, ju
mp,
hop
, etc
the
num
ber
sele
cted
. At t
he c
ompl
etio
n of
cou
ntin
g, a
ll ch
ildre
n cl
ap
and
say
“Pop
!” T
he le
ader
bec
omes
par
t of
the
circ
le, a
nd th
e ne
xt c
hild
take
s a
turn
as
lead
er.
Lan
guag
e ar
ts
Let
ter
Lau
nch
Stud
ents
rec
eive
a b
allo
on w
ith a
n up
perc
ase
lette
r w
ritte
n on
it. A
roun
d th
e ro
om th
e te
ache
r pl
aces
a
com
pani
on b
allo
on w
ith th
e sa
me
lette
r in
low
er c
ase.
Chi
ldre
n to
ss th
e ba
lloon
up
in th
e ai
r, no
t let
-tin
g it
hit t
he g
roun
d. W
hen
the
teac
her
sign
als,
chi
ldre
n m
ust fi
nd th
e co
mpa
nion
bal
loon
, mat
chin
g th
e lo
wer
case
and
upp
erca
se le
tters
. The
act
ivity
is r
epea
ted
so th
at c
hild
ren
can
try
diff
eren
t let
ters
of
the
alph
abet
.
Fun
With
Sca
rves
Chi
ldre
n th
row
sca
rves
in th
e ai
r an
d ca
tch
with
dif
fere
nt b
ody
part
s: h
and,
elb
ow, k
nee,
nos
e, b
ack,
ch
est,
tum
my,
foo
t.
Mus
ical
Mar
chTe
ache
rs p
lace
lette
r ca
rpet
squ
ares
or
lam
inat
ed le
tters
larg
e en
ough
to s
tand
on
in a
cir
cle.
Usi
ng
appr
opri
ate
mus
ic (
teac
her’
s pr
efer
ence
), c
hild
ren
mar
ch a
roun
d th
e ci
rcle
of
lette
rs. W
hen
the
mus
ic
stop
s, s
tude
nts
mus
t find
a le
tter
squa
re a
nd n
ame
the
lette
r th
ey a
re s
tand
ing
on. F
or v
aria
tions
, use
ot
her
loco
mot
or m
ovem
ents
suc
h as
ski
ppin
g, h
oppi
ng, a
nd r
unni
ng.
(con
tinue
d)
92
Sam
ple
activ
ities
by
cont
ent a
rea
Des
crip
tion
Soci
al s
tudi
es/S
cien
ce
Sens
e Sc
ram
ble
Teac
her
plac
es la
rge
pict
ures
of
eyes
, nos
e, e
ars,
han
ds, t
ongu
e in
dif
fere
nt lo
catio
ns a
roun
d th
e cl
ass-
room
. Tea
cher
cal
ls o
ut a
sen
sory
wor
d (e
g, ta
ste)
and
an
anim
al m
ovem
ent.
Chi
ldre
n us
e th
e sp
ecifi
ed
anim
al m
ovem
ent t
o go
to th
e pi
ctur
e th
at c
orre
spon
ds to
the
sens
ory
wor
d.
Ani
mal
Ant
ics
Chi
ldre
n ar
e sh
own
a pi
ctur
e of
an
anim
al. C
hild
ren
mov
e, a
ct, a
nd s
ound
like
the
anim
al.
Nut
ritio
n ed
ucat
ion
B
rocc
oli B
rocc
oli!
Chi
ldre
n pa
ss 2
or
mor
e ba
lls (
or a
ge-a
ppro
pria
te o
bjec
ts)
arou
nd a
cir
cle.
Whe
n th
e te
ache
r ca
lls o
ut
“bro
ccol
i,” a
nyon
e ho
ldin
g th
e ba
ll m
ust r
un (
skip
, hop
, gal
lop)
aro
und
the
outs
ide
of th
e ci
rcle
and
re
turn
to h
is o
r he
r pl
ace
in th
e ci
rcle
. If
the
teac
hers
cal
ls o
ut “
broc
coli
broc
coli,
” (b
rocc
oli t
wic
e)
child
ren
not h
oldi
ng a
bal
l run
(sk
ip, h
op, g
allo
p) a
roun
d th
e ci
rcle
and
bac
k to
thei
r pl
aces
.
Pizz
a D
eliv
ery
Man
Teac
hers
mak
e a
pret
end
pizz
a ou
t of
card
boar
d. C
hild
ren
sit i
n a
circ
le f
orm
atio
n. O
ne c
hild
is d
es-
igna
ted
the
pizz
a de
liver
y pe
rson
and
wal
ks a
roun
d th
e ci
rcle
car
ryin
g th
e pi
zza.
The
chi
ld p
lace
s th
e pi
zza
behi
nd a
noth
er c
hild
and
touc
hes
him
or
her
on th
e ba
ck a
nds
says
, “D
ing-
dong
.” T
he r
est o
f th
e ch
ildre
n sa
y, “
Pizz
a D
eliv
ery!
” T
he c
hild
that
has
the
pizz
a be
hind
them
sta
nds
up, g
rabs
the
pret
end
pizz
a, a
nd r
uns
(hop
s, m
arch
es, s
kips
, gal
lops
, etc
) ar
ound
the
circ
le. T
he g
ame
cont
inue
s un
til e
very
-on
e ha
s de
liver
ed a
piz
za.
Tab
le 1
(co
nti
nu
ed)

Promoting Physical Activity in Preschool Children 93
Process Evaluation Methods
To monitor implementation of the curriculum, teachers and staff from the interven-tion classroom completed a structured checklist at the end of each session. The checklist recorded the day and time of implementation, the learning context in which move and learn activities were implemented, the number of children participating that day, and children’s responses during and after the move and learn activity. Children’s responses were evaluated in the following dimensions using a 1 to 5 Likert scale: enthusiasm, attention, persistence, verbal self-regulation, and physi-cal self-regulation. In addition, teachers and staff met briefly with the investigators on a weekly basis to receive feedback and to discuss any problems related to the curriculum implementation.
Measurement Protocol
Over the course of the 10-week study, each class group had its physical activity levels monitored twice a week. On each monitoring day, all participating students in the class wore an accelerometer for the duration of the program. Accelerometers were attached on the child’s arrival to the classroom and taken off just before leav-ing the program. In addition, all participating preschoolers were observed for 15 minutes using a previously validated direct observational system. To avoid bias related to the time of day, participating students were randomly assigned to 15-minute time segments. To control for potential order effects related to the day of the week, the activity-monitoring schedule was rotated and counterbalanced on a 2-week cycle.
Instrumentation
Accelerometry. Physical activity during the preschool program was quantified using the Actigraph accelerometer (WAM 7164). Consistent with previous stud-ies, the Actigraph was attached to an adjustable elastic belt and worn on the right hip. Because the typical 1-minute sampling interval might mask the short inter-mittent bursts of activity characteristic of young children, a 15-second sampling interval was used.21 Activity counts for each 15-second interval were uploaded to a customized data-reduction software program for the determination of minutes of vigorous physical activity (VPA) and minutes of MVPA. Counts were classified as moderate-intensity (3–5.9 METs) or vigorous-intensity (≥6 METs) activity using the age-specific count cut-offs derived by Sirard and colleagues.22 The Actigraph accelerometer has been shown to provide valid assessments of physical activity in preschool-age children.
Observational System. To determine the effect of the curriculum on instructional practices, physical activity levels during specific learning contexts were character-ized using a direct-observation system known as OSRAP—Observational System for Recording Activity in Preschoolers.11 In short, the OSRAP uses a momentary time-sampling procedure to collect contextual and behavioral information in a vari-ety of common preschool settings. The observation system is a focal child system

94 Trost, Fees, and Dzewaltowski
in which a designated child serves as the focus of data collection for a specified time interval, and all coding decisions about contextual and behavioral information are made in reference to that focal child. OSRAP measures the following major variables: (1) children’s physical activity level (5 levels ranging from inactive [sed-entary] to vigorous); (2) type of activity (eg, running, walking, crawling, climbing); (3) physical location (outside versus indoors); (4) learning context (circle or group time, free choice, snack time, transition); and (5) social grouping (solitary, one-on-one with adult, one-on-one with peer, group with adult, group without adult). All observational data were entered directly into a PDA with the aid of a customized data-entry form. For the current study, the physical activity variables of interest were percent of total observations with an activity rating of moderate intensity or greater (%MVPA) in the following preschool locations or learning contexts: circle time, outdoor free choice, indoor free choice, snack time, and transitions. In addition, because the PDA and accelerometers were synchronized to the same computer clock, the observational system was used to identify the times children were in the classroom or outdoors on the playground. This information was used in the processing of the accelerometer data files to delineate classroom-only activity from overall activity (classroom and outdoor time combined).
Observations were completed by 2 of the investigators and 2 research assistants. Before data collection, all observers completed the training procedures recom-mended by McKenzie.23 These included (1) observer orientation, (2) study of the observational manual and familiarization with the coding scheme, (3) direct practice using videotaped segments, (4) assessments and feedback using a reference video tape, (5) practice in the observational setting with feedback, and (6) field practice with concurrent reliability assessment with a certified assessor. Interobserver agree-ment for each component of the OSRAP were as follows: activity level (83.9%), activity type (83.9%), physical location (100%), learning context (100%), and social context (80.6%).
Statistical Analysis
All statistical analyses were conducted using SAS version 9.1. The effects of the intervention on the accelerometer-derived activity variables were tested using a mixed-model repeated-measures ANOVA (PROC Mixed), which accounted for the use of intact class groups. Within each model, condition, time, and the condition by time interaction were included as fixed effects with children nested with classroom nested within treatment included as a random effect. Tests of simple effects were used to evaluate the significance of differences between intervention and control participants at each 2-week interval. Because the primary goal of the interven-tion was to integrate physical activity into the existing classroom curriculum, we analyzed classroom-only accelerometer data as well as data collected during classroom time and normally scheduled outdoor time. For the observational data, logistic regression analyses was used to calculate the relative likelihood of MVPA occurring during circle time, indoor free-choice time, snack time, transitions, and outdoor free-choice time. Statistical significance was set at an alpha level of .05
Promoting Physical Activity in Preschool Children 95
Results
Participants
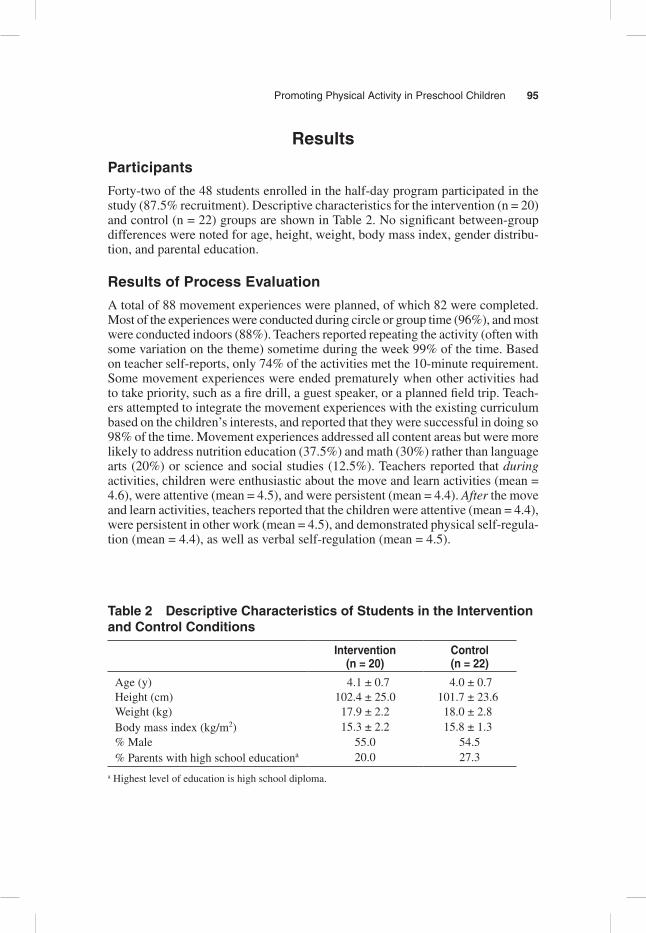
Forty-two of the 48 students enrolled in the half-day program participated in the study (87.5% recruitment). Descriptive characteristics for the intervention (n = 20) and control (n = 22) groups are shown in Table 2. No significant between-group differences were noted for age, height, weight, body mass index, gender distribu-tion, and parental education.
Results of Process Evaluation
A total of 88 movement experiences were planned, of which 82 were completed. Most of the experiences were conducted during circle or group time (96%), and most were conducted indoors (88%). Teachers reported repeating the activity (often with some variation on the theme) sometime during the week 99% of the time. Based on teacher self-reports, only 74% of the activities met the 10-minute requirement. Some movement experiences were ended prematurely when other activities had to take priority, such as a fire drill, a guest speaker, or a planned field trip. Teach-ers attempted to integrate the movement experiences with the existing curriculum based on the children’s interests, and reported that they were successful in doing so 98% of the time. Movement experiences addressed all content areas but were more likely to address nutrition education (37.5%) and math (30%) rather than language arts (20%) or science and social studies (12.5%). Teachers reported that during activities, children were enthusiastic about the move and learn activities (mean = 4.6), were attentive (mean = 4.5), and were persistent (mean = 4.4). After the move and learn activities, teachers reported that the children were attentive (mean = 4.4), were persistent in other work (mean = 4.5), and demonstrated physical self-regula-tion (mean = 4.4), as well as verbal self-regulation (mean = 4.5).
Table 2 Descriptive Characteristics of Students in the Intervention and Control Conditions
Intervention (n = 20)
Control (n = 22)
Age (y) 4.1 ± 0.7 4.0 ± 0.7Height (cm) 102.4 ± 25.0 101.7 ± 23.6Weight (kg) 17.9 ± 2.2 18.0 ± 2.8Body mass index (kg/m2) 15.3 ± 2.2 15.8 ± 1.3% Male 55.0 54.5% Parents with high school educationa 20.0 27.3
a Highest level of education is high school diploma.

96 Trost, Fees, and Dzewaltowski
Accelerometer Data
Over the course of the 10-week study, 769 (91.5%) of the 840 possible accelerom-eter assessments (42 participants × 2 times/wk × 10 weeks = 840) were success-fully completed. Twenty-one accelerometer assessments were missing because of absenteeism, with a further 50 accelerometer-data files lost as the result of downloading errors or accelerometer malfunctions. All 42 participants completed at least 15 of the 20 scheduled days of objective monitoring, with over 80% of the participants completing 18 or more days of accelerometry. The average days of monitoring for participants in the intervention and control classrooms were 18.1 and 18.6, respectively.
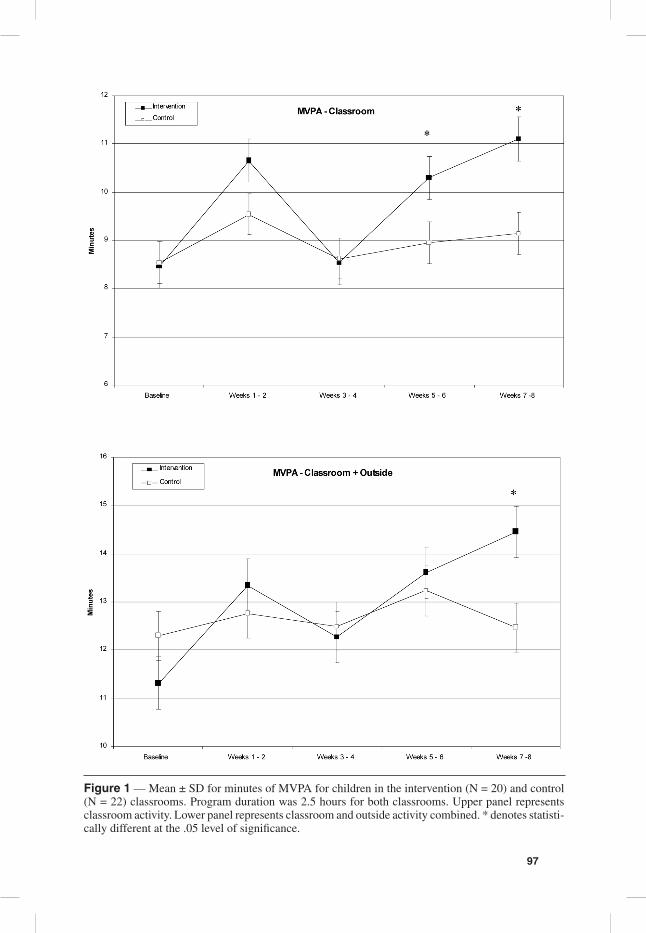
The effects of the curriculum on objectively measured MVPA are shown in Figure 1. For classroom and outdoor time combined, preschoolers in the interven-tion classroom exhibited similar MVPA levels to controls, with the exception of weeks 7 and 8, during which intervention preschoolers exhibited significantly higher levels of MVPA. When only classroom time was examined, preschoolers in the intervention classroom exhibited significantly higher levels of MVPA than controls during weeks 5 and 6 and weeks 7 and 8 (P < .05).
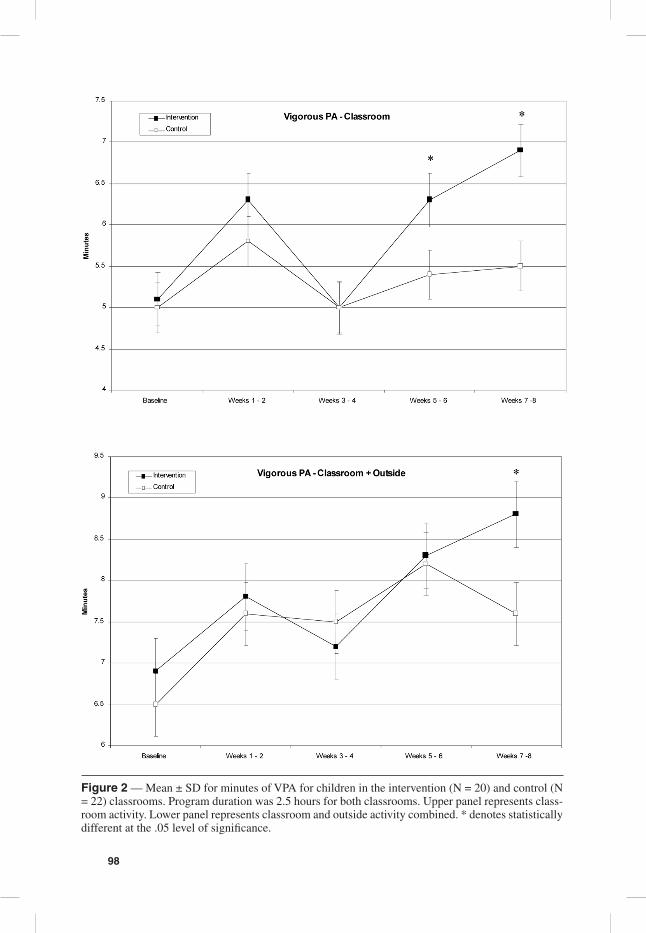
A similar pattern of findings emerged for objectively measured VPA. Pre-schoolers in the intervention classroom exhibited significantly higher levels of classroom-based VPA than preschoolers in the control classroom during the last 4 weeks of the intervention period (P < .05, Figure 2).
Observational Data
Over the course of the 10-week study, project staff completed approximately 168 hours of direct observation. Intervention and control classrooms were equally observed, with 10,060 and 10,114 30-second coded observation epochs completed in the intervention and control classrooms, respectively. On average, preschoolers in intervention classroom were observed on 17 occasions (range 13–20), with each observation session lasting, on average, 14:47 minutes (29.6 30-second observation epochs). Preschoolers in the control classroom were observed on 16.1 occasions (range 10–20), with each observation session lasting, on average, 14:15 minutes (28.5 30-second observation epochs). The percentage of observations occurring outdoors for the intervention and control classrooms was 13.7% and 14.9%, respectively.
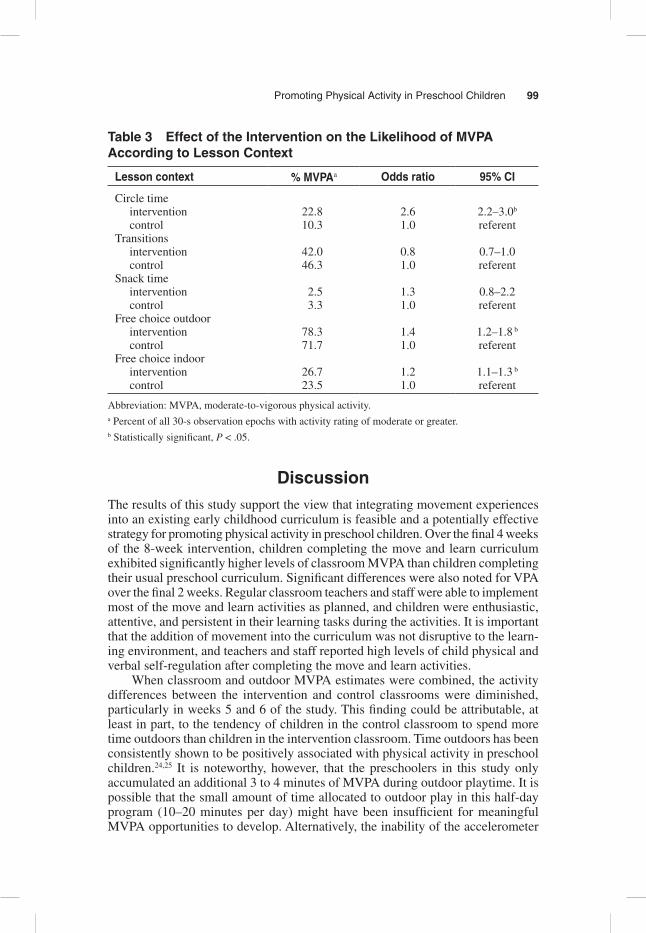
Logistic regression analyses were used to calculate the relative likelihood of MVPA occurring during specific segments of the preschool day (circle time, indoor free-choice time, snack time, transitions, and outdoor free-choice time) in the inter-vention versus the control classroom. Results are shown in Table 3. Preschoolers in the intervention classroom were significantly more likely than preschoolers in the control condition to exhibit MVPA during circle time (OR = 2.6), free-choice time outdoors (OR = 1.4), and free-choice time indoors (OR = 1.2; P < .05). During transitions and snack time, the proportion of observations with at least moderate-intensity physical activity did not differ between the 2 groups.
97
Figure 1 — Mean ± SD for minutes of MVPA for children in the intervention (N = 20) and control (N = 22) classrooms. Program duration was 2.5 hours for both classrooms. Upper panel represents classroom activity. Lower panel represents classroom and outside activity combined. * denotes statisti-cally different at the .05 level of significance.
98
Figure 2 — Mean ± SD for minutes of VPA for children in the intervention (N = 20) and control (N = 22) classrooms. Program duration was 2.5 hours for both classrooms. Upper panel represents class-room activity. Lower panel represents classroom and outside activity combined. * denotes statistically different at the .05 level of significance.
Promoting Physical Activity in Preschool Children 99
Table 3 Effect of the Intervention on the Likelihood of MVPA According to Lesson Context
Lesson context % MVPAa Odds ratio 95% CI
Circle time intervention 22.8 2.6 2.2–3.0b
control 10.3 1.0 referentTransitions intervention 42.0 0.8 0.7–1.0 control 46.3 1.0 referentSnack time intervention 2.5 1.3 0.8–2.2 control 3.3 1.0 referentFree choice outdoor intervention 78.3 1.4 1.2–1.8 b
control 71.7 1.0 referentFree choice indoor intervention 26.7 1.2 1.1–1.3 b
control 23.5 1.0 referent
Abbreviation: MVPA, moderate-to-vigorous physical activity.a Percent of all 30-s observation epochs with activity rating of moderate or greater.b Statistically significant, P < .05.
DiscussionThe results of this study support the view that integrating movement experiences into an existing early childhood curriculum is feasible and a potentially effective strategy for promoting physical activity in preschool children. Over the final 4 weeks of the 8-week intervention, children completing the move and learn curriculum exhibited significantly higher levels of classroom MVPA than children completing their usual preschool curriculum. Significant differences were also noted for VPA over the final 2 weeks. Regular classroom teachers and staff were able to implement most of the move and learn activities as planned, and children were enthusiastic, attentive, and persistent in their learning tasks during the activities. It is important that the addition of movement into the curriculum was not disruptive to the learn-ing environment, and teachers and staff reported high levels of child physical and verbal self-regulation after completing the move and learn activities.
When classroom and outdoor MVPA estimates were combined, the activity differences between the intervention and control classrooms were diminished, particularly in weeks 5 and 6 of the study. This finding could be attributable, at least in part, to the tendency of children in the control classroom to spend more time outdoors than children in the intervention classroom. Time outdoors has been consistently shown to be positively associated with physical activity in preschool children.24,25 It is noteworthy, however, that the preschoolers in this study only accumulated an additional 3 to 4 minutes of MVPA during outdoor playtime. It is possible that the small amount of time allocated to outdoor play in this half-day program (10–20 minutes per day) might have been insufficient for meaningful MVPA opportunities to develop. Alternatively, the inability of the accelerometer
100 Trost, Fees, and Dzewaltowski
to accurately measure certain types of playground activities (eg, riding bikes, playing on the swings, climbing and hanging on fixed equipment) might have led to an underestimation of the amount of MVPA performed outdoors. Considering that only 25% of the 30-second observation epochs taking place outdoors had an activity rating of moderate or higher, it appears that the children were not highly active during outdoor time. The relatively small amount of time spent outdoors by all 4 class groups in this study reinforces the needs for program directors and teachers to monitor and enforce policies related to time for outdoor free play or free play.26
The mostly null findings observed during the first 4 weeks of the intervention suggest that teachers were experiencing difficulty implementing the movement experiences as planned. Although process-evaluation data indicated that teachers had successfully implemented most of the move and learn experiences and rated them favorably, classroom observations during the first 4 weeks of the intervention suggested that teachers were not consistently meeting the project requirements of implementing 2 or more move and learn curriculum activities lasting 10 minutes or longer. To rectify the situation, the investigators met with the classroom teach-ers to reiterate project requirements and to reexamine the concepts covered in the initial training session. The apparent success of this strategy over the final 4 weeks of the intervention confirms that a single group training session is not adequate for effective implementation. A training model that includes on-site or online booster sessions and opportunities for individual evaluation and feedback is, therefore, strongly recommended.
To our knowledge, only 2 published studies have formally evaluated programs to promote physical activity in preschool children. Reilly and McDowell27 tested the effects of a 12-week program of structured physical activity that aimed to increase habitual levels of physical activity and improve motor skills. The 30-minute physical activity sessions were delivered 3 times per week in nursery schools in Glasgow, Scotland. The intervention was supplemented with a home-based educational component that targeted reductions in sedentary behavior. The weekly program was associated with a significant increase in objectively measured physical activity, both on the days the program (40% increase) was offered and on the days when it was not (29% increase). A significant improvement in motor-skill performance was also noted.
The Hip-Hop to Health Junior study tested the effects of a culturally proficient diet and physical activity intervention in a Head Start preschool program in Chicago, Illinois.28 The intervention was implemented over a 14-week period and consisted of three 45-minute lessons weekly. Half of the 45-minute lesson focused on healthy eating through the use of age-appropriate puppets that represented different food groups. The remaining half focused on physical activity and involved structured exercise to music. The child intervention was complemented by an intensive parent component consisting of a weekly newsletter, homework assignments, and twice-weekly aerobic classes conducted at the children’s Head Start center. After 1- and 2-year follow-ups, children receiving the intervention exhibited significantly smaller increases in body mass index than children in the control centers. With the exception of saturated-fat intake at the 1-year follow-up, however, there were no significant differences for any of the dietary or physical activity outcomes.29 The
Promoting Physical Activity in Preschool Children 101
absence of positive findings for physical activity might be related, in part, to the use of self-reported rather than objectively measured physical activity.
Although both of the aforementioned studies represent stand-alone programs that must be added to the existing early childhood curriculum, their generally posi-tive findings, along with our own, suggest that programs to promote healthy eating and regular physical activity in early childhood settings have strong potential to curb the continued rise in childhood obesity rates.
A major strength of this study was the use of 2 independent objective measures of physical activity to rigorously assess change in classroom- and individual-level physical activity behavior. Over the course of the 10-week study, participants com-pleted, on average, 18 to 19 days of objective monitoring with an accelerometer. In addition, each child’s physical activity behavior was directly observed in a variety of learning contexts and social groupings on 16 to 17 occasions. The combination of these 2 methods allowed us to examine the effect of the curriculum in specific learning contexts and segments of the preschool program. A further strength was our use of existing classroom teachers and staff to implement the curriculum. This approach was in contrast to previously conducted obesity-prevention studies that have used outside early childhood professionals or trained research staff to implement the intervention.27,29 Although conducted as an efficacy study in a single child-care center, the positive results achieved by the teachers and staff in this study suggest that the move and learn approach has strong potential for dissemination to other child-care settings.
Opposing these strengths were a number of limitations. First and foremost, the study was conducted as a preliminary efficacy study and involved a relatively small number of children attending a single child-care center. Although providing evidence of feasibility and efficacy are important first steps in developing effec-tive translatable intervention programs, it is imperative that the move and learn approach be evaluated in other child-care centers that offer greater racial/ethnic diversity and provide both half-day and full-day programs. Second, because the move and learn curriculum was specifically designed to increase physical activity while attending preschool, we did not monitor physical activity levels outside of the program. As a result, we cannot rule out the possibility that the more active children in the intervention classrooms might have compensated for this increase by decreasing activity levels at home or elsewhere. Observational studies involving elementary school children suggest, however, that this is an unlikely possibility.30 Third, although teachers in the intervention classroom reported consistently high levels of child self-regulation after completing the move and learn activities, we did not directly evaluate the effect of the curriculum on academic performance or learning-related outcomes such as time on task. Future investigations should rigorously evaluate the potential for move and learn curricula to positively enhance learning outcomes in addition to promoting physical activity.
In conclusion, an 8-week curriculum integrating opportunities for physical activity into all aspects of the preschool curriculum, including math, science, language arts, and nutrition education, was effective in promoting greater MVPA in preschool children. The curriculum was well-received by teachers, staff, and students and did not adversely affect child behavior or the learning environment. These promising findings suggest that the move and learn approach to physical
102 Trost, Fees, and Dzewaltowski
activity promotion is worthy of replication and should be tested in the context of a larger group-randomized trial.
Acknowledgments
Funding for this project was provided by a grant from the United Methodist Health Ministry Fund, Hutchinson, Kansas. The authors would like to thank the teachers, parents, and children who participated in the study.
References 1. Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence
of overweight and obesity among US children, adolescents, and adults, 1999–2002. J Am Med Assoc. 2004;291(23):2847-2850.
2. Sherry B, Mei Z, Scanlon KS, Mokdad AH, Grummer-Strawn LM. Trends in state-specific prevalence of overweight and underweight in 2- through 4-year-old children from low-income families from 1989 through 2000. Arch Pediatr Adolesc Med. 2004;158(12):1116-1124.
3. Mei Z, Grummer-Strawn LM, Scanlon KS. Does overweight in infancy persist through the preschool years? an analysis of CDC Pediatric Nutrition Surveillance System data. Soz Praventivmed. 2003;48(3):161-167.
4. Dietz WH. Health consequences of obesity in youth: childhood predictors of adult disease. Pediatrics. 1998;101(3 Pt 2):518-525.
5. Must A, Strauss RS. Risks and consequences of childhood and adolescent obesity. Int J Obes Relat Metab Disord. 1999;23(suppl 2):S2-S11.
6. Trost SG, Sirard JR, Dowda M, Pfeiffer KA, Pate RR. Physical activity in overweight and nonoverweight preschool children. Int J Obes Relat Metab Disord. 2003;27(7):834-839.
7. Kimm SY, Glynn NW, Obarzanek E, et al. Relation between the changes in physical activity and body-mass index during adolescence: a multicentre longitudinal study. Lancet. 2005;366(9482):301-307.
8. Moore LL, Gao D, Bradlee ML, et al. Does early physical activity predict body fat change throughout childhood? Prev Med. 2003;37(1):10-17.
9. Berkowitz RI, Agras WS, Korner AF, Kraemer HC, Zeanah CH. Physical activity and adiposity: a longitudinal study from birth to childhood. J Pediatr. 1985;106(5):734-738.
10. Klesges RC, Klesges LM, Eck LH, Shelton ML. A longitudinal analysis of accelerated weight-gain in preschool-children. Pediatrics. 1995;95(1):126-130.
11. Pate RR, Pfeiffer KA, Trost SG, Ziegler P, Dowda M. Physical activity among children attending preschools. Pediatrics. 2004;114(5):1258-1263.
12. Jackson DM, Reilly JJ, Kelly LA, Montgomery C, Grant S, Paton JY. Objectively measured physical activity in a representative sample of 3- to 4-year-old children. Obes Res. 2003;11(3):420-425.
13. Federal Interagency Forum on Child and Family Statistics. America’s Children: Key National Indicators of Well-Being 2005. Washington, DC: US Government Printing Office; 2005.
14. Williams CL, Strobino BA, Bollella M, Brotanek J. Cardiovascular risk reduction in preschool children: the “Healthy Start” project. J Am Coll Nutr. 2004;23(2):117-123.
15. McCall RM, Craft DH. Moving With a Purpose. Champaign, IL: Human Kinetics; 2000.

Promoting Physical Activity in Preschool Children 103
16. Pica R. Moving and Learning Across the Curriculum: More Than 300 Activities and Games to Make Learning Fun. 2nd ed. Albany, NY: Delmar Thomson Learning; 2006.
17. Pica R. Your Active Child: How to boost physical, emotional, and Cognitive Develop-ment Through Age-Appropriate Activity. New York, NY: McGraw-Hill; 2003.
18. Roths B, Fees BS, Bailey G, Fitzgerald K. Let’s move, learn and have fun! J Nutr Educ Behav. 2002;34:343.
19. Kansas Nutrition Network. Nutrition: Good For You! Manhattan, KS: Kansas State University Press; 2002.
20. Kansas Department of Health and Environment. Class Act—Kansas LEAN Physical Activity Guide. Kansas Dept of Health and Environment; 1998.
21. Nilsson A, Ekelund U, Yngve A, Sjostrom M. Assessing physical activity among children with accelerometers using different time sampling intervals and placements. Pediatr Exerc Sci. 2002;14:87-96.
22. Sirard JR, Trost SG, Pfeiffer KA, Dowda M, Pate RR. Calibration and evaluation of an objective measure of physical activity in preschool children. J Phys Act Health. 2005;3:345-357.
23. McKenzie TL. Use of direct observation to assess physical activity. In: Welk GJ, ed. Physical Activity Assessments for Health-Related Research. Champaign, IL: Human Kinetics; 2002:179-195.
24. Sallis JF, Prochaska JJ, Taylor WC. A review of correlates of physical activity of children and adolescents. Med Sci Sports Exerc. 2000;32(5):963-975.
25. Baranowski T, Thompson WO, DuRant RH, Baranowski J, Puhl J. Observations on physical activity in physical locations: age, gender, ethnicity, and month effects. Res Q Exerc Sport. 1993;64(2):127-133.
26. Burdette HL, Whitaker RC. Resurrecting free play in young children: looking beyond fitness and fatness to attention, affiliation, and affect. Arch Pediatr Adolesc Med. 2005;159(1):46-50.
27. Reilly JJ, McDowell ZC. Physical activity interventions in the prevention and treat-ment of paediatric obesity: systematic review and critical appraisal. Proc Nutr Soc. 2003;62(3):611-619.
28. Fitzgibbon ML, Stolley MR, Dyer AR, VanHorn L, KauferChristoffel K. A community-based obesity prevention program for minority children: rationale and study design for Hip-Hop to Health Jr. Prev Med. 2002;34(2):289-297.
29. Fitzgibbon ML, Stolley MR, Schiffer L, Van Horn L, KauferChristoffel K, Dyer A. Two-year follow-up results for Hip-Hop to Health Jr: a randomized controlled trial for overwieght prevention in preschool minority children. J Pediatr. 2005;146(5):618-625.
30. Dale D, Corbin CB, Dale KS. Restricting opportunities to be active during school time: do children compensate by increasing physical activity levels after school? Res Q Exerc Sport. 2000;71(3):240-248.