fast followers community of practice
TRANSCRIPT

WELCOME
Tuesday 24th March 2015 LTC Year of Care Commissioning:
Fast Followers Community of Practice Workshop

Long term conditions Year of care commissioning Programme
• To understand more about the fast follower community of practice and where it fits within the national NHSIQ LTC Year of Commissioning Programme and the wider LTC Framework
• To get an overview of the work of the early implementer sites • To learn and draw conclusions from the Kent whole population dataset linkages –
long term conditions and multi morbidity • To gain practical knowledge around the use and application of the LTC Year of Care
Commissioning Simulation Model • To understand direction of travel in terms of national pricing, supporting the 5 year
forward view • To network and learn from each other • To contribute to the development of the fast follower network
of Care foundation.
Outcomes from today:
Long term conditions Year of care commissioning Programme
The Long Term Conditions Year of Care Commissioning Programme...and how
the Fast Follower Community of Practice fits...

Long term conditions Year of care commissioning Programme
Launched in June 2012 under Department of Health QIPP programme
Transferred to NHS England in December 2013 and delivered by NHSIQ from April 2014
SRO is Dr Martin McShane, Medical Director for LTCs, NHSE England
LTC Year of Care Commissioning Programme:
Early Implementer Care Economy Region
Leeds North
Southend Midlands and East
Kent South
West Hampshire South
Barking, Havering and Redbridge London

Long term conditions Year of care commissioning Programme
LTC Year of Care Commissioning Deliverables:
5
• 5 Early Implementer sites
• Whole Population Datasets
• Implementation Guide
• Simulation Modelling
• Specialist Support Team

Long term conditions Year of care commissioning Programme
Developing a Community of Practice:
• The Long Term Conditions Year of Care Commissioning Model is about to complete its third year and the Early Implementer sites are well on their way to shadow testing a variety of models.
• The delivery team within NHSIQ would like to take this opportunity of welcoming the Fast Follower health and social care economies to benefit from the learning gained in the first three years.
• Creating a Learning Network

Long term conditions Year of care commissioning Programme
Introducing the Fast Followers:
• We made contact with you initially because you are:
– Doing work locally related to integration of care and starting develop processes and systems to support integrated working locally
AND – Interested in learning from others in developing LTC year
of care commissioning and capitated budgets

Long term conditions Year of care commissioning Programme
Introducing ….the Fast Followers:
Area Lead organisation Barnsley South West Yorkshire Partnership NHS FT Bracknell Bracknell & Ascott CCG Cheshire Cheshire & Merseyside CSU East Sussex East Sussex county council Great Yarmouth Great Yarmouth CCG Islington & Haringey Whittington Health (Islington & Haringey) North Hampshire Hampshire county council Northamptonshire Northamptonshire Healthcare NHS FT Sheffield Sheffield CCG Slough Slough CCG South Manchester University Hospital of South Manchester NHS FT Southwark & Lambeth Southwark & Lambeth Integrated Care Stockport Stockport CCG
Waltham Forest & East London Waltham Forest and East London Collaborative (WELC) for Integrated Care, inlcuding Tower Hamlets CCG
Whittington Whittington Health (Islington & Haringey) Wigan Wrightington, Wigan & Leigh NHS Foundation Trust Windsor Windsor Ascott & Maidenhead CCG Wolverhampton The Royal Wolverhampton NHS Trust

Long term conditions Year of care commissioning Programme
LTC Year of Care Commissioning
National Programme
team
FF
FF
FF FF
FF
Early Implementers
• Conduit • Access to specific
information / learning •Virtual facilitation
Networking and learning... From each other, the early implementer
sites and national experts in various related fields
Through... • Email updates • Our website • Facilitated Webinars with specialist
input • National workshops • Case studies
Support to fast followers... • Improve confidence and effectiveness of leaders of large
scale change, • Highlight fresh perspectives on how to plan and lead large
scale change programmes which improve patient outcomes and public value for the co morbid patient cohort,
• Present opportunities to tackle local cultural and organisational barriers to find different ways of working to improve coordinated care, across the care economy,
• Increase the ability to implement testing of new processes, tested by others in a safe environment.

Long Term Conditions Dashboard http://ccgtools.england.nhs.uk/ltcdashboard/flash/atlas.html
Long Term Conditions House of Care Toolkit www.nhsiq.nhs.uk/improvement-programmes/long-term-conditions-and-integrated-care/house-of-care.aspx
Simulation Model: http://www.simul8.com/viewer/download.htm
LTC Bulletin: http://www.nhsiq.nhs.uk/11283.aspx #LTCyearofcare #LTCimprovement @NHSIQ
LTC Improvement Programmes Tools and Resources:

Long term conditions Year of care commissioning Programme
• NHSIQ LTC Implementation Guide chapter - Exploring the Commissioning of Personalisation within a Capitated Budget Model
• NHSIQ LTC Implementation Guide chapter – EIS case studies: – BHR: Health 1000 (new organisational structures)
– West Hampshire: Information and data flows
– Southend: capitated budgets
– Kent and Leeds to be published soon
• Population Level Commissioning for the Future - Kent • LTC Year of Care Simulation Model
• Workshop learning, reflections and slide-share
LTC Year of Care Commissioning publications, resources and tools: http://www.nhsiq.nhs.uk/improvement-programmes/long-term-conditions-and-integrated-care/ltc-year-of-care-commissioning-model.aspx
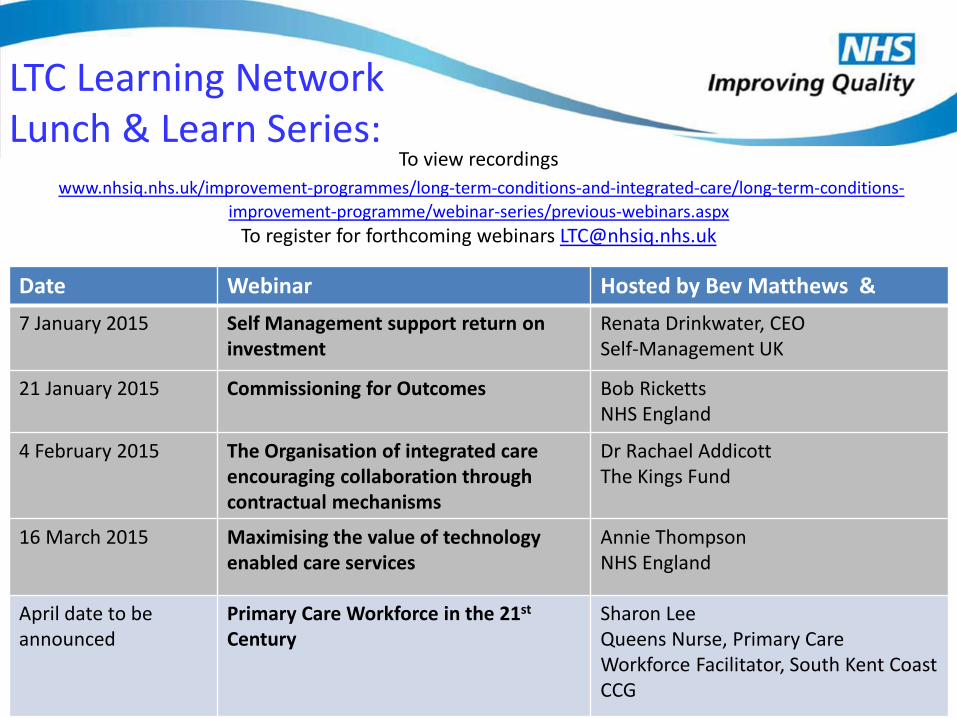
LTC Learning Network Lunch & Learn Series:
Date Webinar Hosted by Bev Matthews & 7 January 2015 Self Management support return on
investment Renata Drinkwater, CEO Self-Management UK
21 January 2015 Commissioning for Outcomes Bob Ricketts NHS England
4 February 2015 The Organisation of integrated care encouraging collaboration through contractual mechanisms
Dr Rachael Addicott The Kings Fund
16 March 2015 Maximising the value of technology enabled care services
Annie Thompson NHS England
April date to be announced
Primary Care Workforce in the 21st Century
Sharon Lee Queens Nurse, Primary Care Workforce Facilitator, South Kent Coast CCG
To view recordings www.nhsiq.nhs.uk/improvement-programmes/long-term-conditions-and-integrated-care/long-term-conditions-
improvement-programme/webinar-series/previous-webinars.aspx To register for forthcoming webinars [email protected]

Any questions….

Developing Long Term Conditions Year of Care commissioning for multi-morbidity
Dr Jamie Day
Long Term Conditions Year of Care Commissioning Programme
Improving health outcomes across England by providing
improvement and change expertise
How is it different from other programmes?
To join the programme early implementer health and social care economy teams demonstrated:
• Strong relationship between organisations
• Linked information across organisations
• Existing strategy for the development of integrated care services.
The programme is focussed on developing the support functions for integrated care:
• Finance and information
• Contracting and commissioning.

Boundaries and integrated care
Need to define boundaries
Need to overcome boundaries
• Patient cohort
• Services paid for within the capitated budget
• Relationships between commissioners and providers
• Information flows
• Payment flows
• Service continuity

Generalised patient pathway and the payment cycle for complex care patients
Select patients for
referral
Assessment of patient
need
MDT – develop and share care
plan
Deliver services to
patients
Assign to patient cohort
Patient dies or
leaves area
Change to patient cohort
Review contract
and budget
Set contract
and budget
Perform and
quality
Payment
Patient pathway
Payment cycle

Selecting patients for referral
Tested Benefits of multi-morbidity
• Decision support tool for NHS continuing care
• Risk stratification
• Multi-morbidity
• Simple method
• Identifies patients with long term conditions
• Can identify patients with acute and mental health morbidities
• Multi-morbidity is common
• Potential for early identification of patient with complex care needs
• Cost is related to complexity

Multi-morbidity is common

Cost is related to complexity

Cost can increase rapidly for patients with complex care needs
BHR health economy

Experience from early implementer teams
Common to all teams Differs between teams
• Multi-morbidity for selecting patients for referral
• Single point of access/assessment
• Shared care record
• Annual capitated budget
• Outcome-based measurement
• Services (providers) included
• Contracting model and financial governance
• Palliative / end of life
• Service specific (e.g. cancer or musculoskeletal)
• Integrated care for older persons / frail elderly / complex care

Barking & Dagenham, Havering & Redbridge health economy

Barking & Dagenham, Havering & Redbridge health economy
Complex care practice (Health 1000):
• Independent, not-for-profit organisation
• Managed by geriatrician, staffed by GPs and allied care professionals, with links to the voluntary sector
• Delivers primary and community care services, and sub-contracts acute services to a fixed population of 1,000 patients
• Situated in a hospital – A&E triage, direct access to diagnostics, outpatient clinics and consultants (transport important)
• Accountable Care Organisation managed by the Area Team and CCG through a prime provider contract
• Patients deregistered from current GP Practice

Payment
Set contract
and budget
Perform and
quality
Perform and
quality measured
Care plan reviewed
Care plan shared
with patient
Care package provided
Payment cycle
Complex care practice
Patient identified
Patient offered support
MDT assessment
Care plan drafted
Patient dies or moves
away
Patient replaced in
cohort
Patient accepts and
placed in cohort
Linked information
Service delivery
Patient pathway and cohort maintenance

Complex care practice
Issues to overcome
Fixed population of 1,000 patients (from estimated 2,000+): • Advantage - Fixed annual capitated budget (incl. primary/secondary care) • Disadvantage - Some patients currently miss out (initially)
Double running finance systems in 2015/16: • Quality of community and mental health costs are poor • Analysis of risk (impact on providers, services, workforce)
CQC registration - neither GP practice nor community provider
Regulations prevent consultant geriatrician seeing patients in the community
Convincing patients to de-register from their current GP practice without experience of what the new service will deliver
Ensuring GP engagement once patients are de-registered from their practice

Mental health care
Acute care
Voluntary care
Primary care
Social Care
Conclusions
But integrated care for the benefit of patients has begun
Community care
Self care
Change is difficult. It requires time and effort.
• Maintaining relationships and an environment that supports change
• Information Governance
• Regulations e.g. setting up new organisations
• Changing services and work patterns

Year of Care Long Term Conditions Simulation
Claire Cordeaux: Executive Director, Healthcare

SIMUL8 Corporation | SIMUL8.com | [email protected]
Agenda
• What is simulation and why use it? • The Long Term Conditions simulation • Next steps • Your questions and comments

SIMUL8 Corporation | SIMUL8.com | [email protected]
What is simulation?
Models a flow of individual patients
Small scale operations
Service operations
Whole system
Passing of time
Arrivals
Duration of treatment
Time between treatments
Waiting times and bottle necks
Experimentation
What if?....
No risk to patients through pilots
Results
Costs
Resource utilisation
Waiting times
High level flow and operational questions, individual patient variability, graphical visualisation

SIMUL8 Corporation | SIMUL8.com | [email protected]
Why simulate Year of Care?
• “Bottle” the processes of the Early Implementers
• Easily enable Fast Followers and others to understand and test impacts
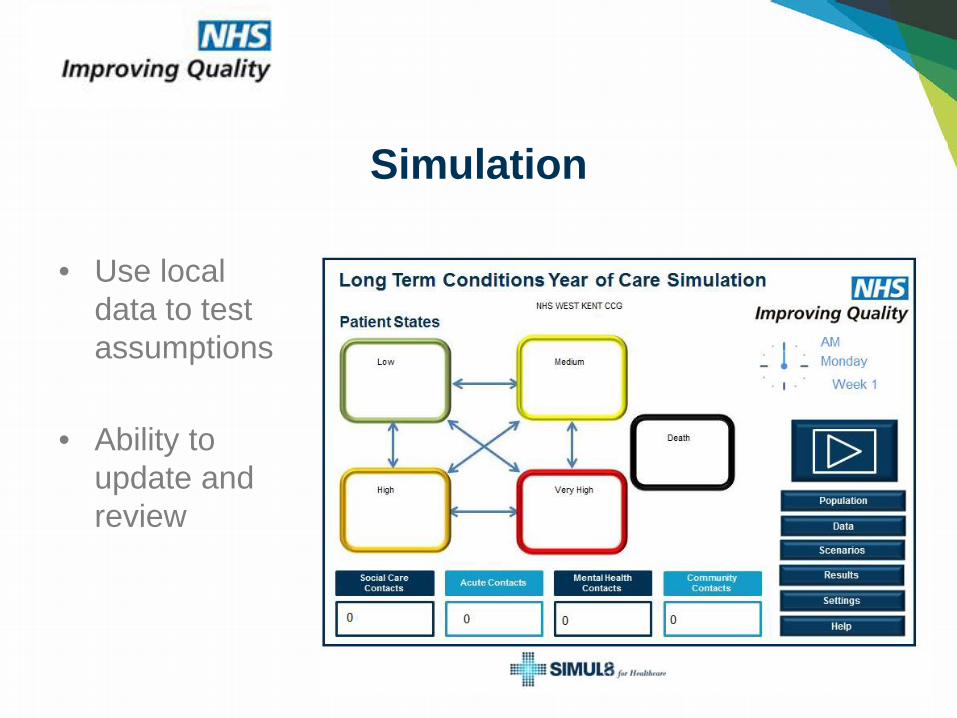
• Use local data to test assumptions
• Ability to update and review
Simulation

• Level of acuity
• Increasing numbers of long term conditions
Current Simulation
• Likelihood of patients accessing services by changing state of patients (state transition)

SIMUL8 Corporation | SIMUL8.com | [email protected]
• Patients in each “state” have – A likelihood of accessing certain types of service
(Acute, Community, Mental Health, Social Care), including accessing services more than once
• Costs associated with those services
How it works

SIMUL8 Corporation | SIMUL8.com | [email protected]
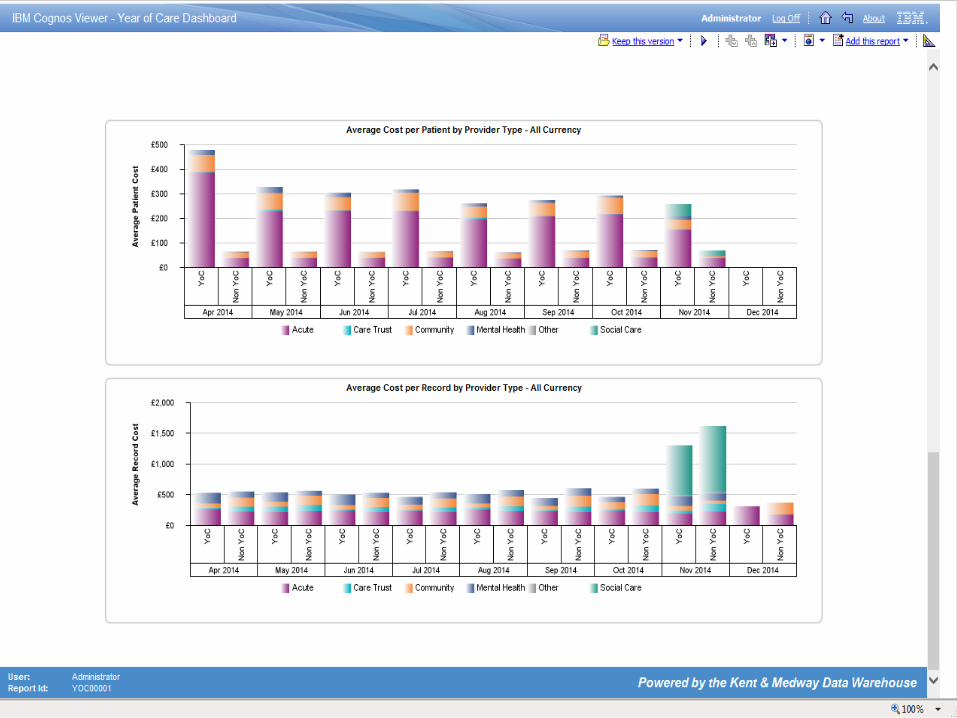
Data builds an underlying discrete event simulation model

• Number of patients in each “state” by year
• Average cost per patient
Results

• Cost by each area of service/organisation
Results
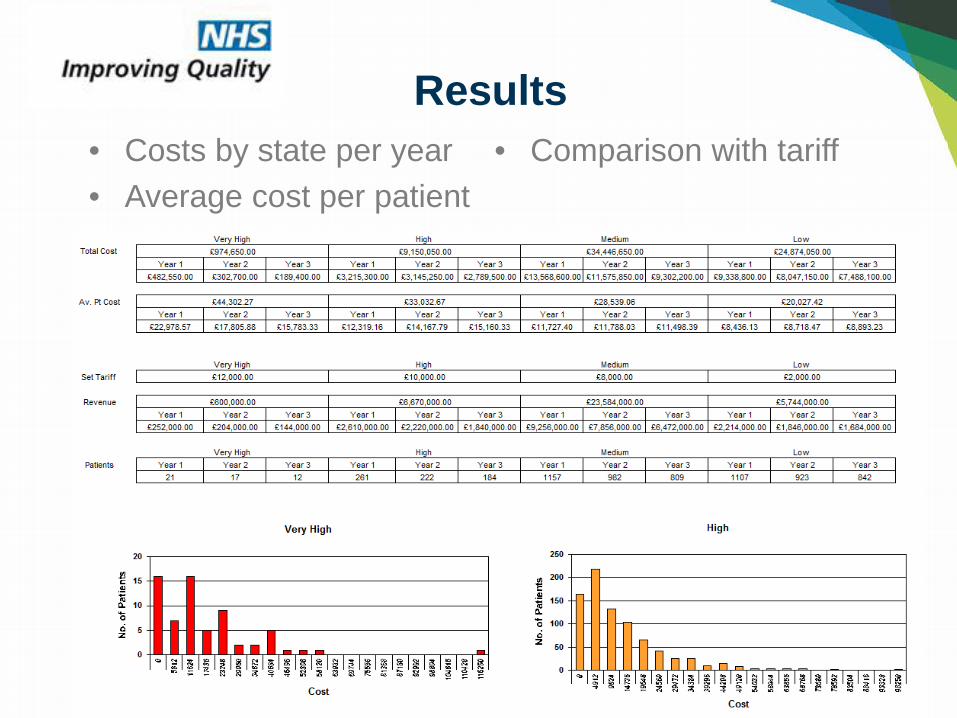
• Costs by state per year • Average cost per patient
• Comparison with tariff
Results


SIMUL8 Corporation | SIMUL8.com | [email protected]
• Known to integrated care team or not? • Test against proposed tariff? • Change variation in cost for services? • Decrease transitions through states?
Scenarios

SIMUL8 Corporation | SIMUL8.com | [email protected]
• Planning for demand • Testing an improvement scenario • Negotiation between healthcare providers
How can this help?

SIMUL8 Corporation | SIMUL8.com | [email protected]
• Building in capacity scenarios • What would you like to know?
– How many staff will I need to support people with LTC?
– What type of staff will I need for services? – How many beds will I need for the LTC cohort?
Next Steps

Click to edit Master title style Click to edit Master title style
SIMUL8 Corporation | SIMUL8.com | [email protected]
QUESTIONS?

Kent LTC Year of Care Programme: Using whole population linked
datasets to develop higher value models of care
Abraham George KCC Public Health Peter Gough KMHIS

Our key objectives • Use whole population integrated data sets to help
commissioners evaluate relative impact of different integrated care initiatives.
• Use routine administration data to develop a different method of commissioning – capitated funding model – to intervene earlier, support independent living, prevent ‘crisis’ and rehospitalisation
• Use the same routine administrative data to develop a different method of payment for services which is not cost per activity – annual tariff
• Identify individuals full personal health and social care budget to support integrated personalisation.

Why – supports strategic direction
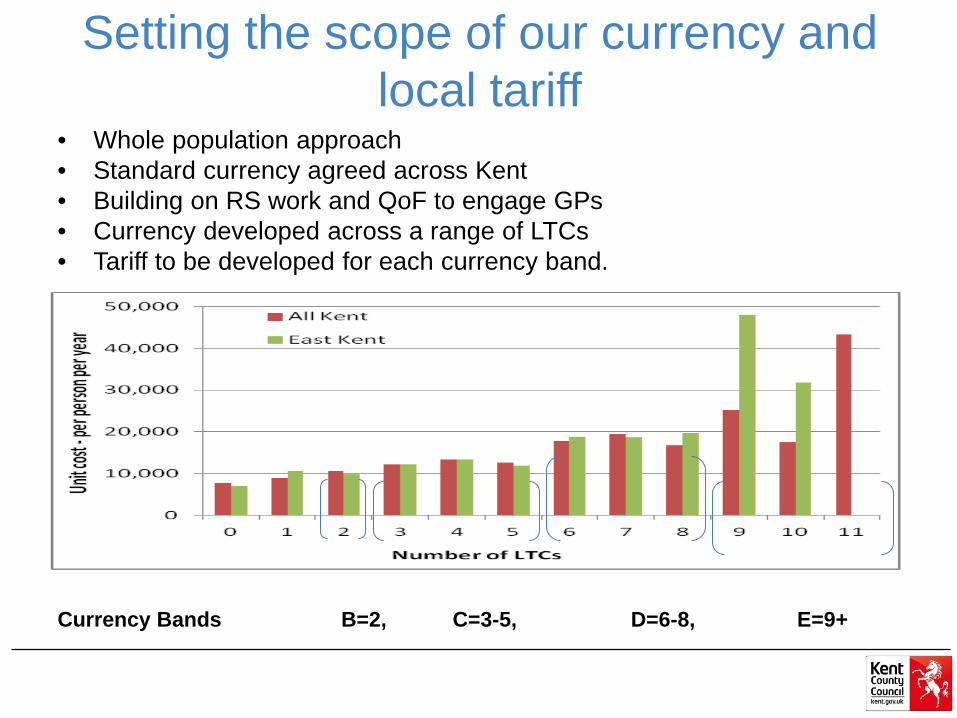
Setting the scope of our currency and local tariff
• Whole population approach • Standard currency agreed across Kent • Building on RS work and QoF to engage GPs • Currency developed across a range of LTCs • Tariff to be developed for each currency band.
Currency Bands B=2, C=3-5, D=6-8, E=9+

Numbers in Kent by Currency Dec 2014

Numbers in system at present – Dec14 • EK currently 38 GP practices pop – 352307(of 88 practices pop
752374) – Band B = 3549, Band C = 4993 Band D = 562 – Band E = 22 – total 9129 (cumulative – 1 double count)
• WK – 13 GP practices pop 141,504 (of 64 practices pop 533585) – Band B = 1097, Band C = 1702 Band D = 256 – Band E = 10 – total 3065 (2 duplicates)
• NK –DGS 33 practices pop 250999 (of 34 practices pop 253646) – Band B = 2304, Band C = 3401 Band D = 425 – Band E = 20 – total 6150
• Currently Kent totals are 18568 of 744,810

EK- 38 GP practices pop – 352307(of 88 practices pop 752374) Band B = 3549, Band C = 4993 Band D = 562 Band E = 22 – total 9129 (cumulative – 1 double count) WK – 13 GP practices pop 141,504 (of 64 practices pop 533585) Band B = 1097, Band C = 1702 Band D = 256 Band E = 10 – total 3065 (2 duplicates) NK – DGS 33 practices pop 250999 (of 34 practices pop 253646) Band B = 2304, Band C = 3401 Band D = 425 Band E = 20 – total 6150 Currently Kent totals are 18568 of 744,810
Key achievements • Currency developed using RS and LTCs
• Linked Data for 18k people
• Linked and costed for 18k people
How we identify potential “at risk” people (a preventative approach)
• Risk stratification tool applied • LTC codes applied (18 in total - QoF) • List segmented by LTC currency (Bands B – E applied -
B=2,C=3-5,D=6-8,E=9+), • Risk Score over time mapped (looking for rise in risk score
in last 6 mths – 4 of 6 show an increase) or • Rapid Riser in last 3 mths (mthly increase in risk score
over past 3 mths and overall increase of >15pts). • Kent – 86 GP practices (15 coming on line), Band B = 7019,
Band C= 10238, Band D =1259, Band E= 52 Total 18558 of approximately 744,810 (9th Jan 2015)

Linked at GP practice level
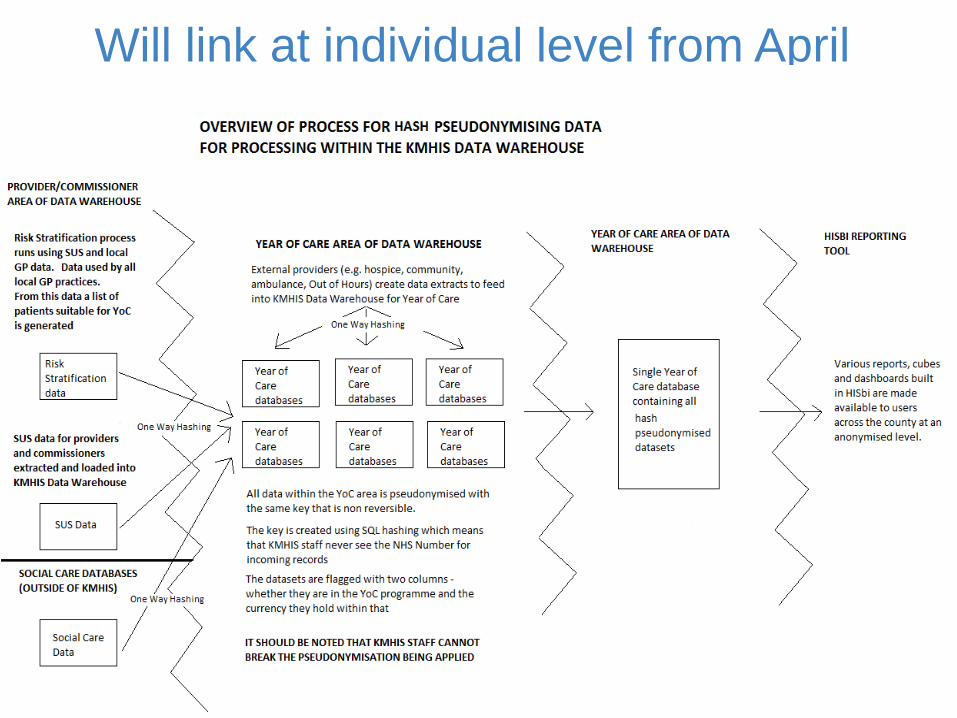
Will link at individual level from April

Distribution of Multi-morbidity in YOC cohort



Next steps – towards evaluation - how does this support Outcomes?
• Identify “proxy” measures systematically collected to support evaluation – (integrated care plans)
• Identify where other services/organisations are collecting the same or similar proxy measure
• What is being done that could support outcomes that is not recorded?
• Identify how it could be systematically collected? All of the above is intended to move us towards outcome focused specifications and aid contracting.



Long term conditions Year of care commissioning Programme
Transitioning to new payment designs
to support delivery of the 5 year forward view
Sue Nowak Pricing team NHS England

Long term conditions Year of care commissioning Programme
Over to you… Sharing experiences, learning and identifying key challenges…

Integrated Care The story so far.... Giles West

Challenged Health and Social Care Economy Outlier for number of people entering residential care Rising rate of NEL admissions to two acute hospitals within
county Large scale CIPs don’t exist anymore - requires major
transformation QIPP schemes often move pressure points within the health
& social care system – need simultaneous change at all points in the pathway
Changing landscape – Forward View, Vanguards, Emerging role of GP Federations

Healthier Northamptonshire Established – Three Programmes o Clinical Collaboration o Integrated Care Closer to Home o Combined Resource Management
Weekly Operational Executive meetings occur Proof of concept phase (summer 2014) – Regulator agreement High level models established –
o First Check Waterfall o Evidence Base o Primary Care Risk Stratification o Model 180 Day in / 180 Day out o Track to HRG activity

Arrival of BCF Granularity of scheme detail (who, what, when, how many…) Calculation of cashable savings Reforecast for anticipated delivery Track the impact of changes across all touch points All parties agreement reflected in BCF and in contract plans
for 2015/2016

Community Case Management
Collaborative Care Teams* Care Home support service*
End of Life Pathway COPD pathway
Telehealth & telecare* Carer Support*
Acute Hospitals
Crisis Intervention & Admission Avoidance
Primary care streaming Ambulatory care
Acute Psychiatric Liaison* Falls Crisis Response Service*
Alcohol Treatment unit Dementia step up*
GP Extended Hours service
Discharge & Reablement
Intermediate care team* Discharge to Assess*
Domiciliary care capacity* START Reablement service*
Community Hospitals* Specialist care centres* Dementia Step Down &
Reablement* Community Nursing*
Stepping Stones*

Ruby’s Story: Ruby is 76 and lives with her husband in a village outside of Northampton. She has a history of bronchial infections and increasingly limited mobility which have resulted in several hospital admissions over past few years. Her husband her main carer has recently been diagnosed with type II diabetes. Outcome in current service Ruby is feeling unwell and seeks an appointment with her GP. She sees her GP two days later. Her GP reviews and prescribes antibiotics. During the night her breathing worsens. After a call to the 111 service the on-call doctor is contacted who decides she needs to be admitted to Hospital. On arrival the hospital does not have access to her primary care record and her husband has to provide information again. She spends five days being stabilised but there is a delay in her return home as the community nursing team have not confirmed they are ready to visit meaning she does not leave until the seventh day. Once home her husband thinks that having a stairlift would help but doesn’t know who to contact for help. They don’t want to use their limited savings for this. Outcome in future service Ruby is beginning to feel unwell. She has already been identified by her GP as a patient at high risk and has a care plan agreed with her GP. As part of this plan she has been given home based diagnostic equipment which is monitored remotely. Her readings are out of range and this has already been flagged to her care coordinator. As a result she is visited that afternoon by a locality specialist nurse practitioner. Escalation options available include provision of IV antibiotics at home under the care of the Hospital at Home Service or admission to the step-up facility in the local community hospital. On this occasion use of the local hospital is agreed. The receiving team at the community hospital can view the electronic care plan, and know what are expected ranges to be achieved for Ruby. After 72 hours Ruby returns home. In discussion with Ruby and her husband it is agreed that a stairlift would be helpful and her care co-ordinator links with the locality wellbeing team to organise installation and who help access the appropriate grants etc.

Revised Best Case County
Scheme Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Total
CCT 43 43 73 103 133 133 133 187 187 187 187 187 1597
Res Care Homes 31 31 31 31 31 31 31 31 31 31 31 31 375
Telehealth 0 0 0 0 28 28 40 40 55 62 75 75 403
EOL 4 4 4 13 13 13 27 27 27 27 27 27 214
COPD 9 9 9 9 9 9 9 9 10 10 9 9 107
Cmty Prevention & Wellbeing 0 0 0 0 0 0 0 3 3 4 4 5 19
Additional Crisis 0 0 0 0 0 0 0 0 0 0 0 0 0
Released Crisis 13 13 25 25 43 43 47 47 47 66 66 66 501
Falls Ambulance 14 13 13 13 13 13 13 14 15 15 14 14 164
Acute Liaison 27 28 27 27 27 27 28 28 28 28 28 28 330
Community Hospital Step Up 0 0 49 64 69 72 73 73 74 74 74 74 696
Dementia Step Up 2 2 2 2 2 2 2 2 2 2 2 2 24
Integrated Alcohol Working 0 0 0 0 16 16 16 16 16 16 16 16 127
533 4557

Programme / Project Project Status Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
A M J J A S O N D J F M
PORTFOLIO: Integrated Care Closer to HomeSRO: Angela Hillery/ Carole Dehghani
Programme: Wellbeing & Prevention
Community Prevention & WellbeingNCC Wellbeing Tender cancelled. New route of Community Interest Company proposed. Assumption is potential benefits from increased wellbeing checks and support given to making lifestyle change
0 3 3 4 4 5
Programme: Community Case Management
Collaborative Care Teams. To include; Care Homes Support and deployment of telehealth solutions for identified risk stratified cohort
Corby Scheme live since October focussing initially on care homes with roll out to primary care scheduled for 2015/2016. Integrated model 13 13 13 13 13 13 13 13 13 13 13 13
161
East Northants Scheme live mid February. Integrated model being deployed 2 2 7 11 15 15 15 21 21 21 21 21
172
Wellingborough Scheme live mid February. Integrated model being deployed 2 2 7 11 15 15 15 21 21 21 21 21
172
Kettering Scheme live March. Integrated model being deployed Mobi l i sation live 3 3 10 17 22 22 22 34 34 34 34 34
269
Daventry GP led schemes not yet inclusive of care homes requires update and further agreement to revised plan 7 7 7 7 11 11 11 15 15 15 15 15
136
South Northants GP led schemes inclusive of care homes requires update and further agreement to revised plan 9 9 9 9 12 12 12 18 18 18 18 18
162
Northampton Central Scheme expected to be live in March. Not yet based on integrated model 2 2 7 12 15 15 15 22 22 22 22 22
178
Northampton West Scheme expected to be live in March. Not yet based on integrated model 3 3 7 12 15 15 15 22 22 22 22 22
180
Northampton East & Sth
Scheme expected to be live in March. Not yet based on integrated model 2 2 6 11 15 15 15 21 21 21 21 21
171
TelehealthBT identified as preferred supplied using G Cloud 6 Government approved procurement route. Deployment of telehealth equipment to 1300 risk stratified persons and remote monitoring service provided by BT CQC approved centre team linked back to our local CCT and North / South Gateways. Mobilisation period based on order being placed by second week of March.
28 28 40 40 55 62 75 75
403
Falls Strategy This is a pipeline project to identify further solutions that cen be deployed to reduce volume of falls. Scoping 0 0 00
End of Life RegisterInitial savings are based on impact on better end of life care planning from CCT becoming fully live. Step change in Q2 is initial impact from deployment of systmone module solution improving sharing on EoL status between agencies with three month bedding in period before second step change as system becomes increasingly effective
4 4 4 13 13 13 27 27 27 27 27 27
214
Community Nursing review Project underway working with steering group to plan redesign recommendations for community nursing service Scoping0
Carer SupportPipeline scheme to identify opportunities for further outcome improvements based on better use of carer support and possible further investment
Scoping
0
2nd phase PMH saving Pipeline scheme during 2015/2016 to identify second wave QIPP schemes based on impact of Primary Mental Health Roll Out phase one Scoping reccomendations 0 0 0
LTC Focus - COPD Cmty Support
Proposal scoped to provide COPD link worker for psychological support. Working as part of the extended AHL service and supporting the pulmonary teams at each acute to identify the patients at greatest risk of admission and ensuring access to range of support materials and media including on-line groups, 1:1 psychological therapy support and working with practice and community staff to increase skills in local management of persons and escalations
Scoping 9 9 9 9 9 9 9 9 10 10 9 9
107Programme: Crisis, Escalation & Admission Avoidance 0
Acute Liaison MHService launched in October 14 and early positive signs being evidenced in stemming increase in demand and in reducing ALOS. Expanded service option now prepared and within affordability envelope provided. Expectation to implement extended service during March.
27.3 27.8 26.8 26.8 26.8 26.8 27.8 27.8 27.8 27.8 27.8 27.8
330
Community Hospital Step-up
Service specification being developed to provide flexible bed reource to better respond to system demand. Next phase of transformation is to launch 18 step-up beds in association with launch of the North and South Gateways. New staffing requirement being costed to ensure delivery within identified envelope. Further transformation will then be planned in accordance with overall system bed review. Scoping
49 64 69 72 73 73 74 74 74 74
696
Primary Care Streaming & Amb pathway PCS operational in both acutes. No NEL reduction modelled for 15/16. NGH now launched formal procurement processCurrently l ive 0
Realigning GP Extended Hours Scheme in scoping phase at present. A&E benefits included in financial plan but at risk of delayed delivery Scoping 0
Released Crisis / Escalation capacityThis is expected benefit from release in existing ICT capacity as result of effectiveness of CCT / CareHomes / Telehealth. Profile would be at risk of delay if there is delay in CCT implementation.
13 13 25 25 43 43 47 47 47 66 66 66501
Additional Crisis / Escalation capacityNo NEL benefits modelled. Current assumption is that investment should be made to maintain current level of performance as result of winter funding. Removing funding will worsen position of system. Current check is level of winter funding on FYE is greater than current investment pot. Need to look at how 15/16 winter funds are planned for spend.
0 0 0 0 0 0 0 0 0 0 0 0
0
Falls ambulanceThe Falls Ambulance was reinstated in January 2015 under winter pressure monies and new contract negotiations are taking place for this to be part of revised 2015/2016 contract.
14 13 13 13 13 13 13 14 15 15 14 14164
Integrated working Alcohol focus Difficulties in engaging with Public Health team to confirm source and value of funds to support this sheme. 15.9 15.9 15.9 15.9 15.9 15.9 15.9 15.9127
Dementia step-up Service currently being provided via winter funding. Business Case developed for continued funding. Currently live 2 2 2 2 2 2 2 2 2 2 2 2 24
Creation of an Integrated Intermediate Care Service Specification
Project underway led by David McKee and Lisa Riddaway. Currently in stakeholder scoping but with expectation to move swiftly to creation of specification for discussion / agreement and then move to mobilisation to implement new model. No NELs included in 15/16 plan Scoping
Gateway ProjectCreation of Gateway Functions North and South to deliver co-ordination of complex patient care packages and swift response and management of crisis. Based on PMCF North model of 8-8, 7 day rapid response. Links to short term discharge project and creation of control room function.
Single Patient RecordProject scope yet to be agreed. Project to address IG issues between organisations being managed by NCC Public Health as mandated by H&WB
Scoping
Programme: Discharge and Reablement
Implementation of wider Discharge to Assess approach
Scoping underway within short term project led by D Hardisty to assess benefits and VFM of implementing the Staffordshire model. Full plan to be developed once initial analysis has been completed.
Scoping
Additional Dom Care CapacityAdditional investment through winter funding supporting system delivery. Recurrent impact of winter commissioned packages and growth funding to support system changes currently being modelled Currently l ive
Integrated Discharge Process / TeamsOperational through winter pressure funding. Currently being reviewed as part of short term discharge project. Deliverable target of integrated HPT/CPT/ICT assessment function of 1st June 2015. Currently l ive
Dementia step down and reanablement - (Older Persons Mental Health Reablement Pathway)
Current live service utilising Angela Grace unit and Southfield units. Scoping now to look at reacurrent funding.
Currently l ive
Review to identify how to better utilise community bed stock
Project yet to commence. NCC review of PFI contract opportunity changes underway. Review will consider all bed stock, SCC & Community Hospital. Review willl need to take into account the future demand modelling produced from the discharge to assess short term project
Scoping
Healthier Northamptonshire5 Year Implementation Plan
2014/15 2015/16 2016/17
Reliant on winter funding
Complexity of transformation with component parts all at different stages of scoping, mobilisation, go-live, evaluation, pathway development and where changes elsewhere will impact.

Avoiding Investment Paralysis Achieving whole system savings not commissioner spend
reduction How to evidence / measure success – sub programme level Data changes – increasing activity, acuity, long term complexity,
ageing… Tracking real spend at patient level across health & social care Limited evidence base – do we believe we are seeking to deliver
the right outcomes External market capacity – domiciliary care, residential care Communications and Stakeholder engagement System Fatigue
4557 NEL reduction in 2015/2016 Solution to track persons across Care First, Systmone, Epex etc using
NHS Number Develop a partnership approach with domiciliary care market Creation of zone, area, multiple area approach to community delivery Greater understanding of our complex discharges Calculate the true transformation costs – programme delivery and
double running Expanding psychological therapy support to persons with LTCs Deployment of technology to risk stratified cohort Creating a truly unified intermediate care offer Profiling the future community bed base required and creating a road
map for this change Maintaining the belief of all partners and providing the energy for
change


Integrated Care
The story so far!
Robert Wilson

Integrated Neighbourhood Teams 2013/14
• Commenced April 2013 • Rapid roll out to 64 of 65 practices
• Aim to deliver case management to the highest risk patients across the borough
• Local risk stratification
• 2500 high risk patient assessed in primary care identified by risk stratification.

INT 2013/14
• 950 patient with case management plans • MDT Approach to case management
• 64 individual meetings clustered together • After initial set up varied support
• Case managers from across health and social care
• In reality majority were community matrons

Combined No of Patients
above X
Non Elective
Bed Days
Non Elective Zero Bed
Days
Elective Bed Days
Elective Zero Bed
Days
53 53 496 1483 141 90 175 75 663 1010
85 138 546 2467 165 399 108 376 1176 800
101 239 553 2383 188 194 283 173 1555 835
103 342 469 2321 132 219 147 192 1417 733
142 484 590 3351 157 403 382 354 2101 877
146 630 539 2672 131 308 276 255 1950 715
156 786 554 2756 141 258 198 214 1995 738
227 1013 697 3450 180 798 369 762 3054 959
257 1270 722 4180 177 995 386 923 3124 1027
287 1557 727 4191 186 931 381 862 3449 1045
838 2395 1884 9796 481 1980 1458 1788 10055 2668
1640 4035 2712 13777 768 2563 1833 2250 17954 4224
4035 10489 52827 2847 9138 5996 8224 48493 15631Total
40-50%
30-40%
55-60%
50-55%
65-70%
60-65%
75-80%
70-75%
85-90%
80-85%
95% +
90-95%
Patient Risk Score
No of Patients in
BandNon Elective Elective OP Appoints A & E Visits
Data Processed Date: 2013-11-30 - All PatientsIndicator Arrows show Comparison of Figure to Previous Month
Total Activity All Providers Dec 12 - Nov 13

The GP Interface.

Initial Findings
• HSJ award winner • Good reductions in hospital admissions • Very medical model • Poor support from provider partners
outwith health after initial set up. • Takes time and money to engage primary
care • Patient stories

Extended INT
• Supported through AUA enhanced service • CCG enhanced services >75 screening
• Fragility scores, Frat scores
• Identified 1 in 4 or 1000 patients not deemed suitable for case management.
• Alcohol/Substance abuse • Chaotic life styles • Not engaged in primary care

Perfect week
• It is right to focus Integrated Care around primary care
• Wider conversations • What is achievable if we break
boundaries • Played a pivotal part in developing
primary care link workers

Digital summary care record sharing

Different models of care • Start well
• Proportion of children school ready • Childhood asthma Children's INT
• Live well • People of working age active case
management • Troubled families 2
• Age Well • Business as usual • End Of Life care/Frail Elderly
Different models of care • Substance misuse
• pro active case management
• Below statutory level support • Primary care link workers • Volunteer coordinators
• Currently 6000 active case management plans in place
• Questions are they the right ones • Do we have too many

Challenges still to do • Prove each scheme is making a
difference • Perfect week (health and social care) in a
school • Culture
• Breaking rules and boundaries of professions and organisations
• Northwest education grant

Challenges still to do
• Risk stratification development • Shared records across all parties • 7 Different single points of access • Community Nursing and Therapy
specification implementation • Provider partnerships
• Primary care transformation • Mental Health Strategy

Integrated Care The story so far!
Any Questions?

46
Fast Followers Workshop 24th March 2015
Integrated care teams in North Hampshire –
experience, lessons and vision!
Dr Richard Coppin ICT GP Lead
North Hampshire CCG Basingstoke

Drivers • Rising costs • Frailty agenda • Quality agenda -
QIPP • Better EoLC • Find the 1%
Patient
Community Care
Primary Care
Secondary Care
Mental Health
Care
Social Care
Voluntary Care
Integrated care 2011
. Vision • Patient focus – self
care • More out of
hospital care • Integrated teams –
remove silos • Care planning with
joined-up records • Risk profiling
48
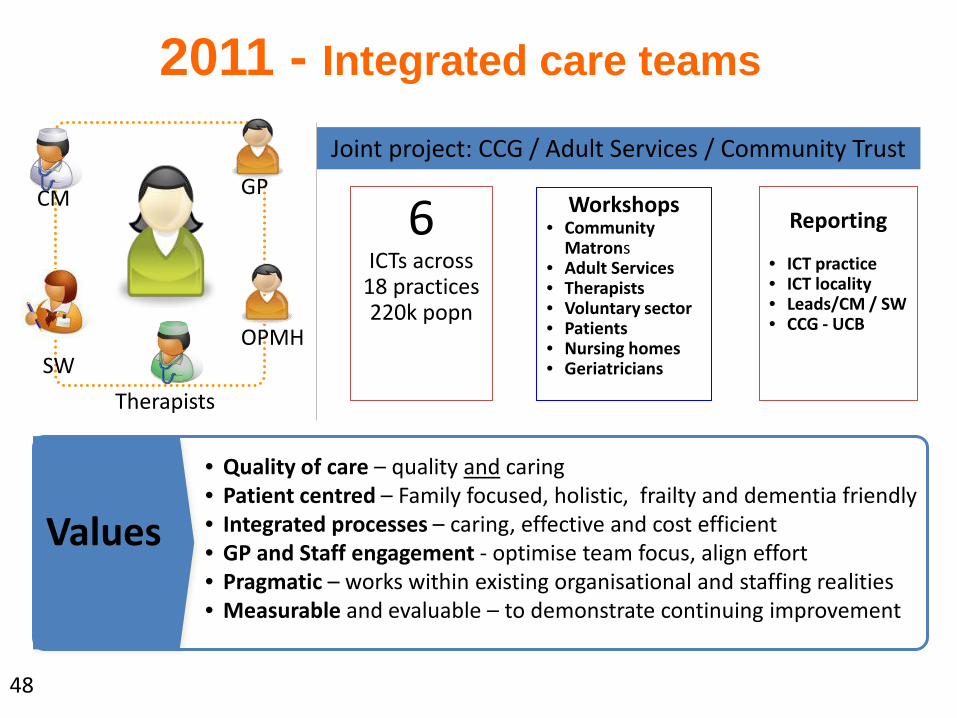
2011 - Integrated care teams
Values
• Quality of care – quality and caring • Patient centred – Family focused, holistic, frailty and dementia friendly • Integrated processes – caring, effective and cost efficient • GP and Staff engagement - optimise team focus, align effort • Pragmatic – works within existing organisational and staffing realities • Measurable and evaluable – to demonstrate continuing improvement
Joint project: CCG / Adult Services / Community Trust
Workshops • Community
Matrons • Adult Services • Therapists • Voluntary sector • Patients • Nursing homes • Geriatricians
Reporting
• ICT practice • ICT locality • Leads/CM / SW • CCG - UCB
GP CM
SW Therapists
OPMH
6 ICTs across
18 practices 220k popn

49
2014 Challenges
• Mostly enthusiastic teams, but….
• Variation in: Who? What? How?
• Lack of engagement - therapists etc
• Rural/urban mix unhelpful
• 6 teams unwieldy / uneconomic?
• Patchy 24/7 cover
• Poor IT, poor data!

50
2014 Values • Fair – geography and need
• Quality and safety
• Measurable
• Sustainable
• Cost effective

51
2015 - Integrated care teams
Issues
• WHO? – cost and need • WHAT? – quality: standardised and measurable • HOW? - Integrated team with clear interfaces, IT, care plans • Staff – leadership, team, development/mix • Measures –patient satisfaction/outcomes, costs, morale • Contracts
Joint project: CCG / Adult Services / Community Trust / Public Health
4 ICTs across
18 practices 220k popn
Interfaces • General Practice • Specialist nurses • Secondary care • Voluntary sector • Public health • Nursing homes
GP CM
SW
Therapists
OPMH
Opportunities!
• MSPO • GP alliance • Social services • Geri buy-in • Deficit!
Geriatrician
Voluntary sector

52
Thanks for listening!
Questions about contracts and incentives? Ask Philip!

Long term conditions Year of care commissioning Programme
Structuring and developing the fast follower learning network
Your thoughts on…. • Learning from each other • Case study development
• Webinar programme development

Long term conditions Year of care commissioning Programme
LTC year of care commissioning programme Fast Follower Community of Practice
Next steps after today…