factor viii inhibitors: after seven decades still a nightmare and a mystery georges e rivard centre...
TRANSCRIPT
Factor VIII Inhibitors: After Seven Decades Still a Nightmare and a Mystery
Georges E RivardCentre Hospitalier Universitaire Sainte-Justine
Montréal
November 2009
For this presentation, I declare no conflict of interest with
any pharmaceutical industry
November 2009
My Disclosure
Lozner EI, Jolliffe LS, Taylor FHL. Hemorrhagic diathesis with prolonged coagulation time associated with a circulating anticoagulant. Am J Med Sc 1940;199:318-27
A 61 Y. old man with acquired hemophilia. Died of bleeding after removal of a lymph node which showed tuberculosis. Whole blood transfusion did not stop bleeding. Normal plasma did not shorten coagulation of patient’s plasma in vitro
Munro FL, Jones MD. The detrimental effect of frequent transfusions in the treatment of a patient with hemophilia. Am J Med Sc 1943;206:710-3
A 36 Y. old man with severe hemophilia from a family with many severe hemophiliacs.Treated successfully for hematuria "with 3 successive days of 50 cc. of plasma" . Further to this success, as need arose, he was successfully treated with 25 to 50 cc. of lyophilized plasma. After about 6 months this treatment failled to control his bleeds and his plasma inhibited clotting of normal plasma in vitro.
“We feel that in view of these observations, care should be taken in treating hemophiliacs by transfusions, and that they probably should not be given them as prophylactic measure…"
Coagulation Inhibitors: Not a New Story
Coagulation Inhibitors: Still a Very Serious Problem
• FS. 8 y boy. Severe FVIII def. High titre inhibitor since age of 12 m. Severe allergic reaction to any product that has even trace of FVIII. Multiple severe haemophilic arthropathies. Wheel-chair bound…for life!
• FR. 15 y boy. Severe FIX def. High titre inhibitor since age of 6 m. Severe allergic reaction to any product that has even trace of FIX. Has had 3 IC bleeds. Last one 6 m ago…and the next one…
• CO. 15 y girl. Severe FXIII def. High titre inhibitor since age of 2 y. IC bleed at
age 2 y. Died of IC bleed last summer…poor parents!
• YM. 42 y man. Severe FVII def. Father of two. High titre inhibitor for one month. No response to any treatment. Died of IC last year on Christmas eve. His 6 y old boy…when is daddy coming back?
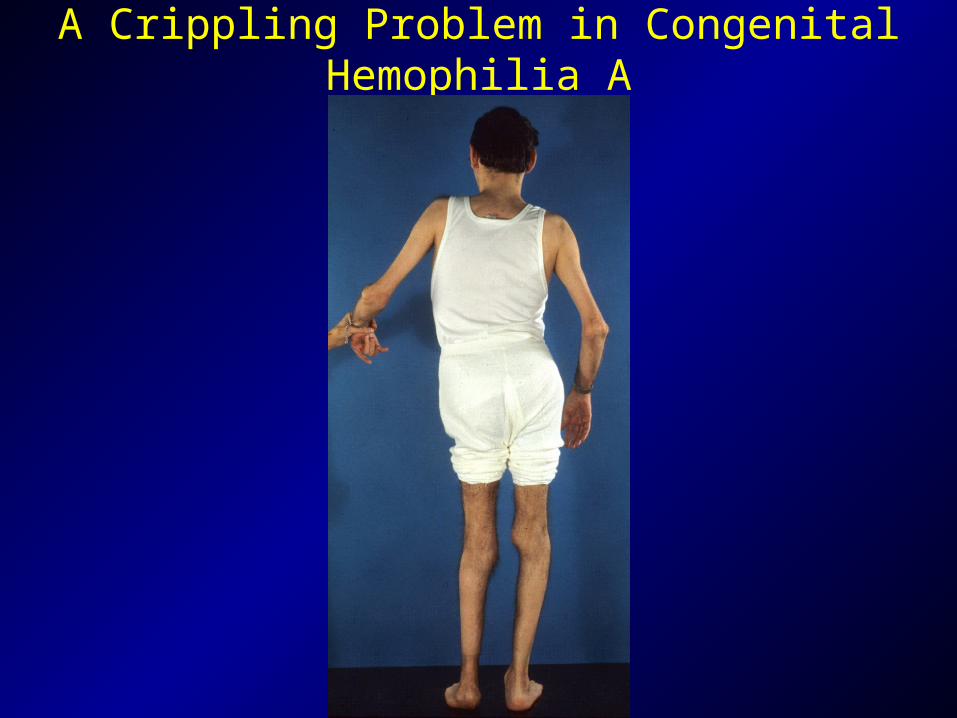
A Crippling Problem in Congenital Hemophilia A
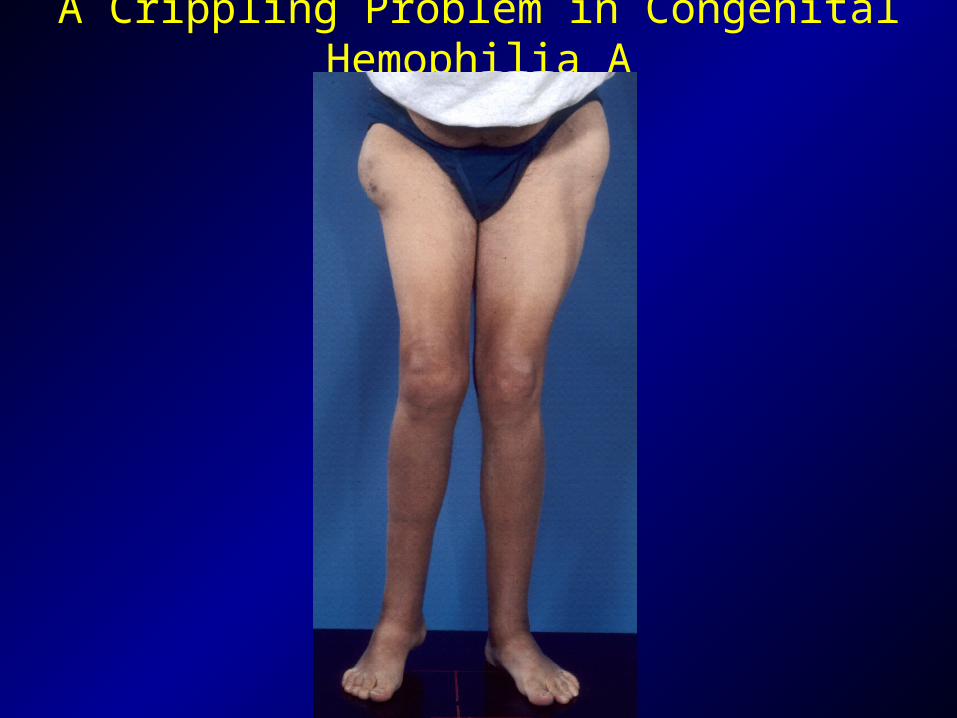
A Crippling Problem in Congenital Hemophilia A

A Major Problem in the Frail Old Subject with Acquired hemophilia A
Cas # 1 Homme de 42 ans
- $
100,000 $
200,000 $
300,000 $
400,000 $
500,000 $
600,000 $
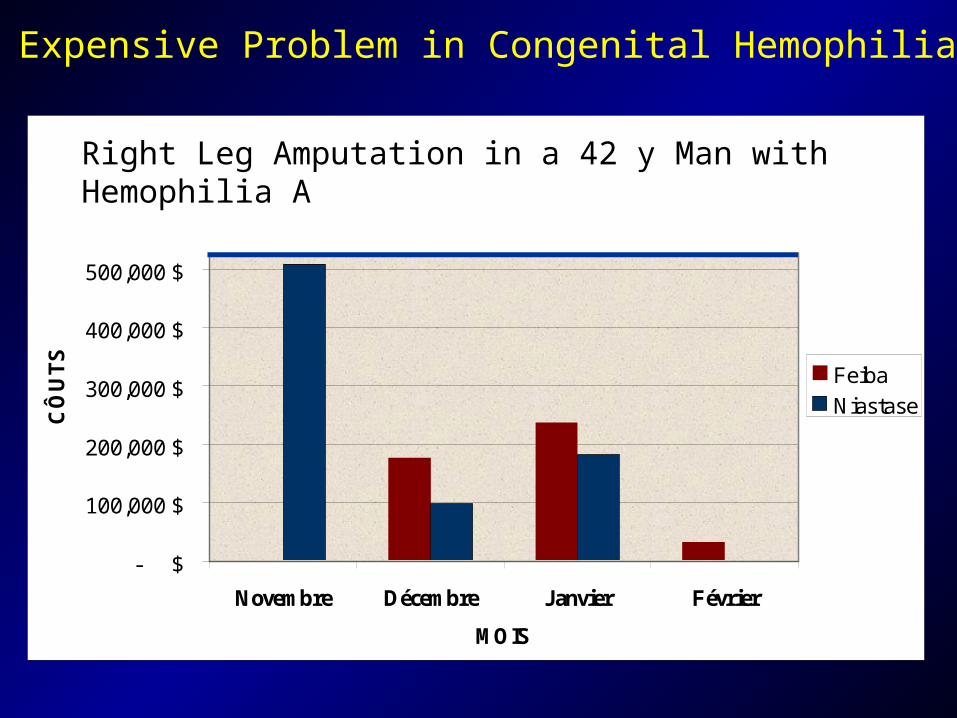
Novembre Décembre Janvier Février
MOIS
CÔ
UT
S
Feiba
Niastase
TOTAL DES COÛTS DES PRODUITS: 1 235 802
An Expensive Problem in Congenital Hemophilia A
Cost for Products: $1,285,892
Right Leg Amputation in a 42 y Man with Hemophilia A
- $100,000 $200,000 $300,000 $400,000 $500,000 $600,000 $700,000 $800,000 $900,000 $
1,000,000 $
Coût $
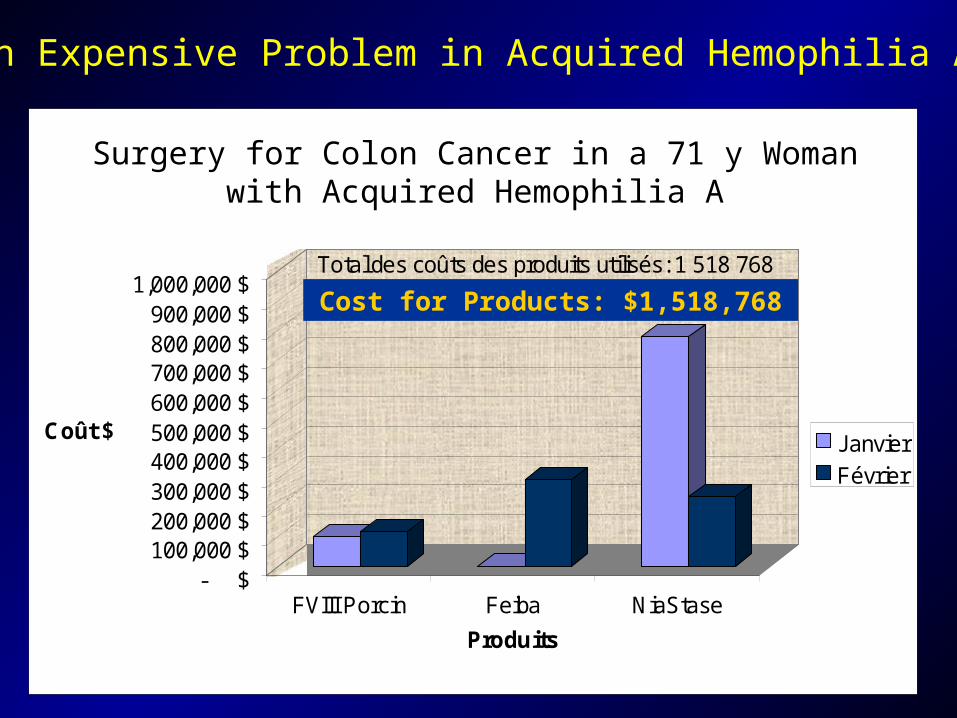
FVIII Porcin Feiba NiaStase
Produits
Cas # 2 Femme de 71 ans avec Inhibiteurs acquis en facteur VIII
JanvierFévrier
Total des coûts des produits utilisés: 1 518 768 $
An Expensive Problem in Acquired Hemophilia A
Cost for Products: $1,518,768
Surgery for Colon Cancer in a 71 y Woman with Acquired Hemophilia A
Cumulative Incidence of Factor VIII Inhibitors
HEMOPHILIACS : 10% to 30%
NON-HEMOPHILIACS : 1/106 per year
A Relatively Rare Condition

Plan of my Presentation
• Acquired hemophilia A in a nut shell
• Hemophilia A with inhibitors…in an egg shell
Plan of my Presentation
• Acquired hemophilia A in a nut shell
• Hemophilia A with inhibitors…in an egg shell
Acquired Haemophilia A UK National Surveillance Study
• From May 2001 to May 2003 with follow up until May 2004
• Data from 255/256 centers: 172 patients • Clinical information for 156/172 patients
PW Collins et al. Blood 2007

Presenting Characteristics
• Incidence: 1.48/million/y• Median age: 78 (range 2-98)• Sex: 43% men, 4/4 women in age group 21-40• Associated with pregnancy 4.3%,
or 1 case per 350 000 births• Underlying diagnosis: 5/5 under age 40 55% between 40 and 59 42% between 60 and 79 23% over 80 PW Collins et al. Blood 2007
Underlying Diagnosis
• None 95 (63.3%)• Autoimmune disease 25 (16.7%)• Malignancy 22 (14.7%)• Dermatologic 5 (3.3%)• Pregnancy 3 (2%)
PW Collins et al. Blood 2007

Sites of Bleeding
PW Collins et al. Blood 2007
More on Presenting Characteristics
• No hemostatic therapy required for 34%• Bleeding as cause of death in 9% (at 1-146 d)• Factor VIII level and inhibitor titer did not
predict severity of bleeding• Older patients more likely to have died during
follow up (P < 0.001) but achieved remission more quickly (P< 0.042)
PW Collins et al. Blood 2007
International Recommendations on the Diagnosis and Treatment of Patients with Acqquired Hemophilia A
• Anti-hemorrhagic treatment - rFVIIa 90 µg/kg every 2-3 h until hemostasis is achieved
OR
- aPCC 50-100 IU/kg every 8-12 h until hemostasis is achieved
• Inhibitor eradication - Corticosteroids 1 mg/kg/day for 4-6 weeks alone or with:
- Cyclophosphamide 1.5 – 2 mg/kg/day for up to 6 weeks
A Huth-Kühne et al. Haematologica 2009;94:566-75
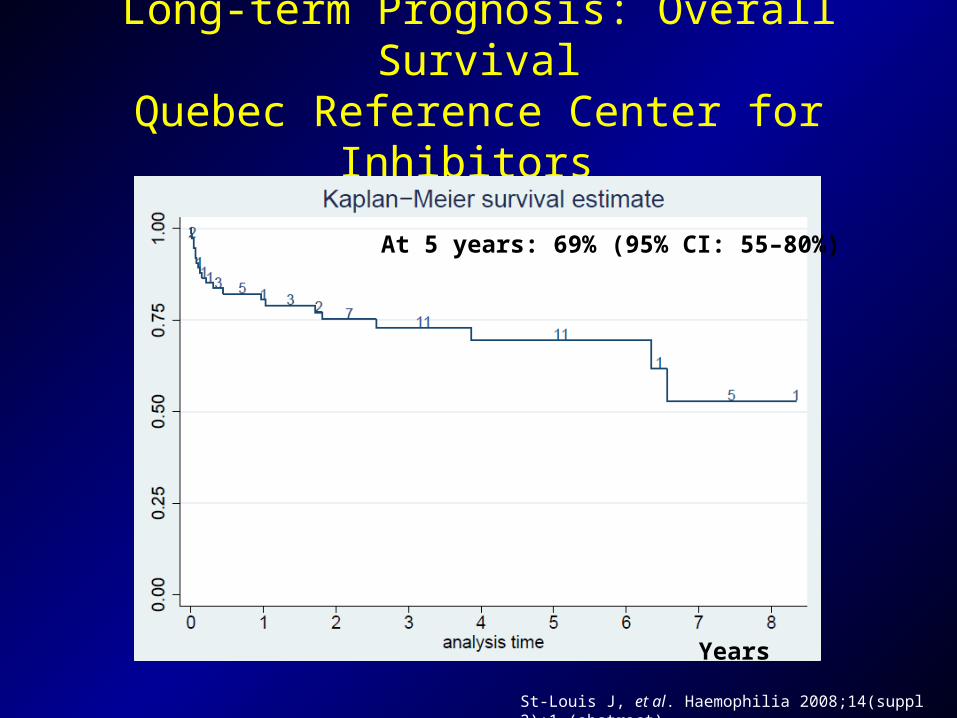
Long-term Prognosis: Overall SurvivalQuebec Reference Center for Inhibitors
Years
At 5 years: 69% (95% CI: 55–80%)
St-Louis J, et al. Haemophilia 2008;14(suppl 2):1 (abstract)
Plan of my Presentation
• Acquired hemophilia in a nut shell
• Hemophilia A with inhibitors…in an egg shell

Laboratory Investigation
• APTT: 78/34
• APTT ( 1P + 1N): 65/34
• Factor VIII inhibitor: 10 BU
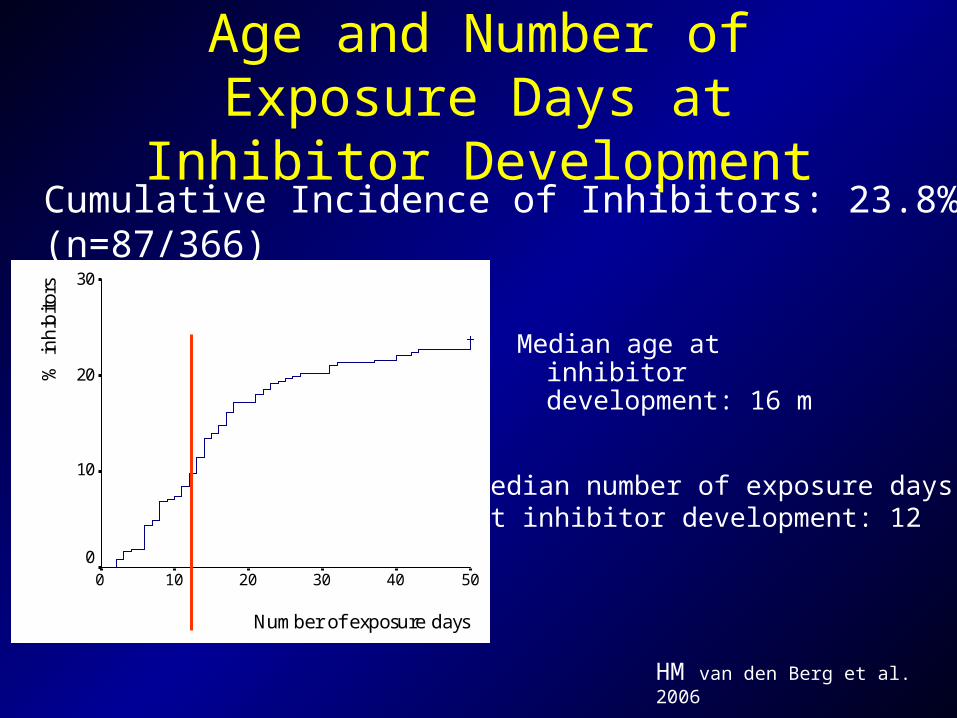
Age and Number of Exposure Days at Inhibitor Development
Median age at inhibitor development: 16 m
Cumulative Incidence of Inhibitors: 23.8% (n=87/366)
Number of exposure days
50403020100
% in
hibi
tors 30
20
10
0
HM van den Berg et al. 2006
Median number of exposure daysat inhibitor development: 12
Facteur VIII Inhibitors
Nature: Antibodies directed against one or more epitopes of factor VIII and leading to partial or complete inhibition of its procoagulant function
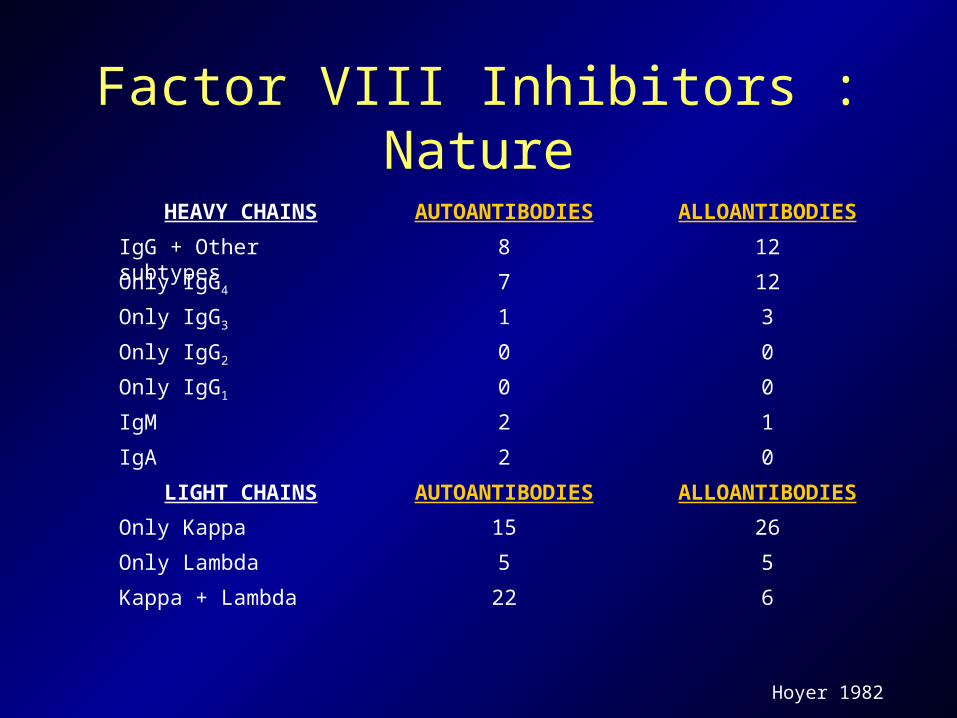
Factor VIII Inhibitors : Nature
622Kappa + Lambda
55Only Lambda
2615Only Kappa
ALLOANTIBODIESAUTOANTIBODIESLIGHT CHAINS
02IgA
12IgM
00Only IgG1
00Only IgG2
31Only IgG3
127Only IgG4
128IgG + Other subtypes
ALLOANTIBODIESAUTOANTIBODIESHEAVY CHAINS
Hoyer 1982

The Bethesda Unit
Kasper, 1975
One Bethesda Unit:The amount of antibody thatinhibits half of the factor VIIIactivity in a 1 to 1 mixture ofpatient plasma and normalplasma incubated at 37°C for 2 hours
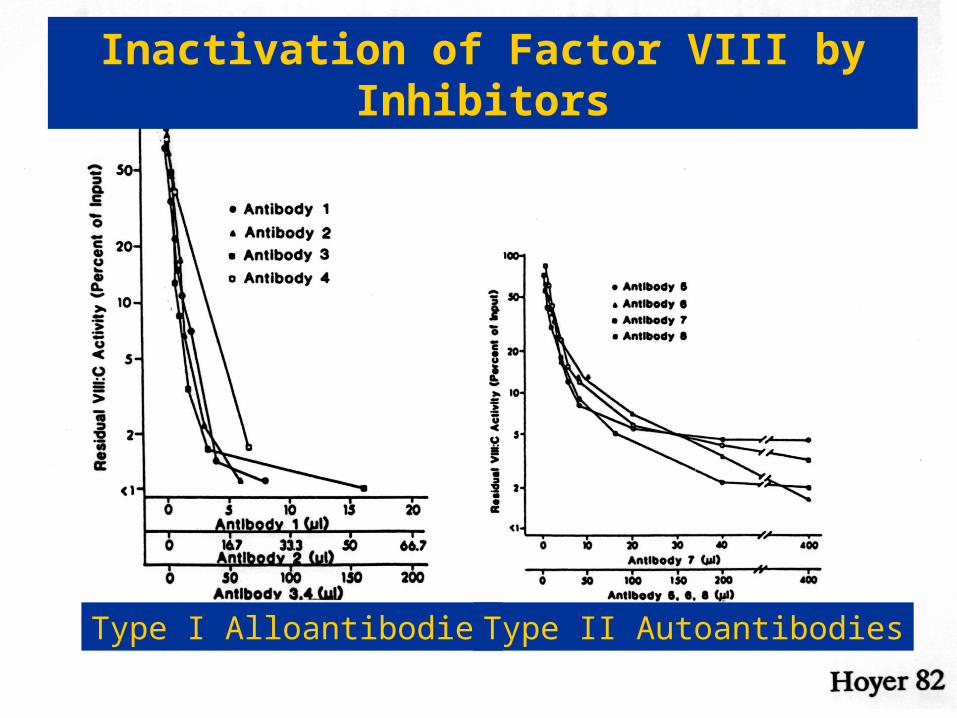
Type I Alloantibodies Type II Autoantibodies
Inactivation of Factor VIII by Inhibitors
Facteur VIII Inhibitors
Nature: Antibodies directed against one or more epitopes of factor VIII and leading to partial or complete inhibition of its procoagulant function
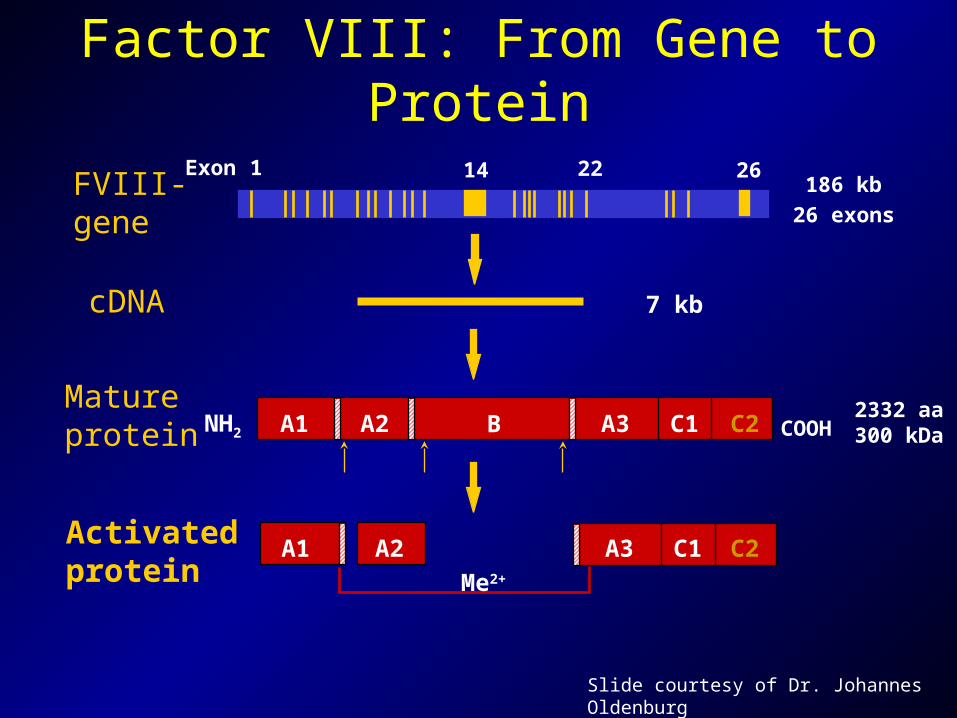
A2Activatedprotein
A1 A3 C1 C2
Me2+
Matureprotein NH2 COOHA1 A2 B C1 C2A3
2332 aa300 kDa
26 exons
186 kbFVIII-gene
Exon 2614 221
cDNA 7 kb
Factor VIII: From Gene to Protein
Slide courtesy of Dr. Johannes Oldenburg
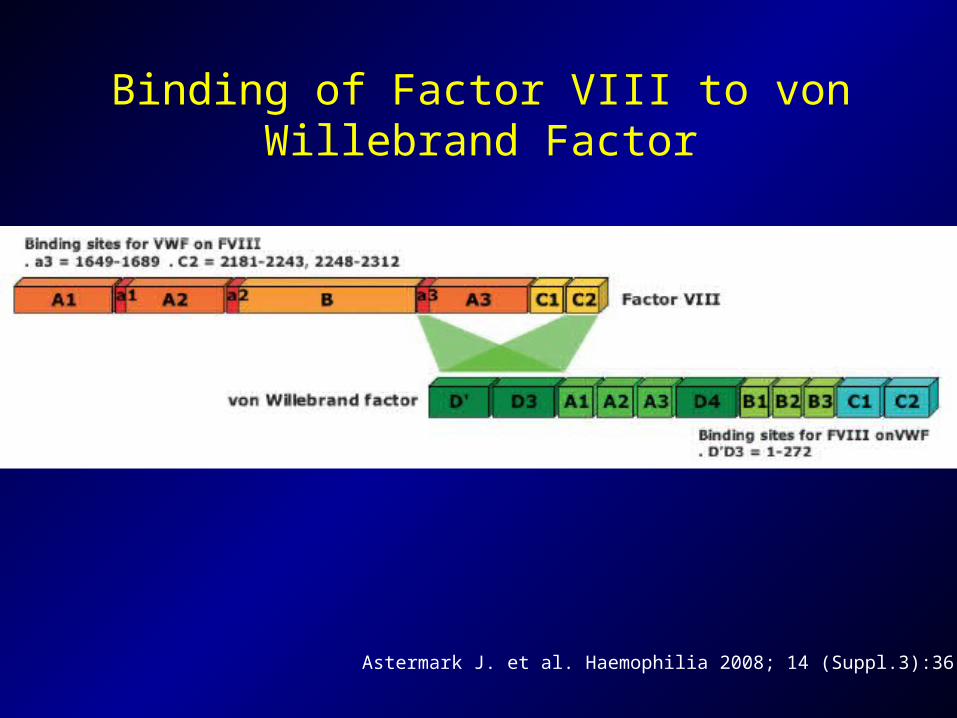
Astermark J. et al. Haemophilia 2008; 14 (Suppl.3):36-42
Binding of Factor VIII to von Willebrand Factor
vWF/PL
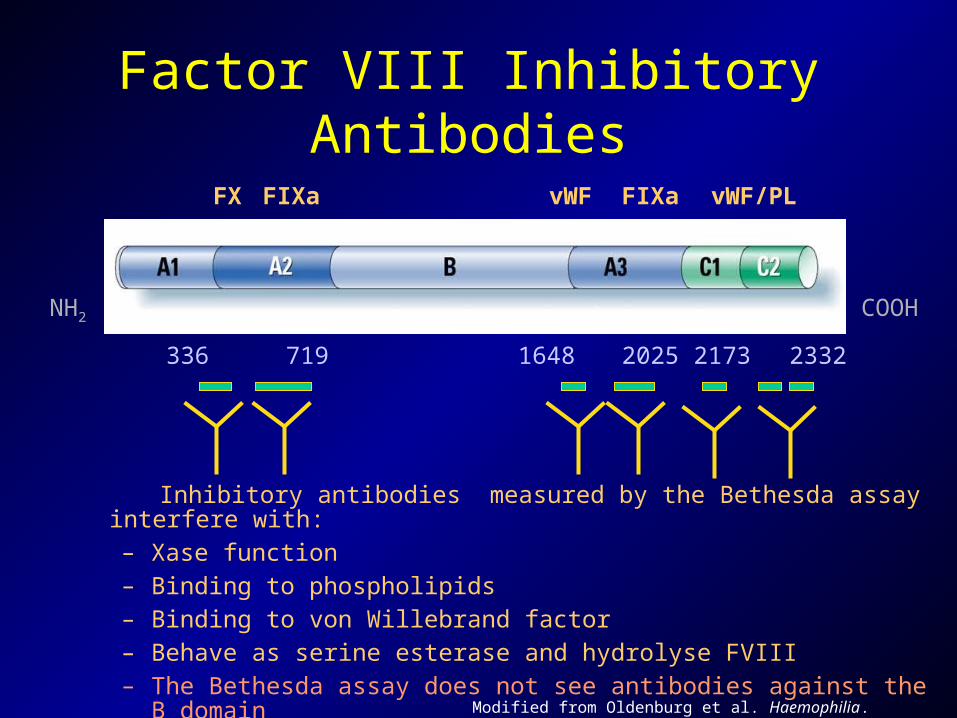
Factor VIII Inhibitory Antibodies
FIXavWFFIXaFX
COOH
2332217320251648719336
NH2
Inhibitory antibodies measured by the Bethesda assay interfere with: – Xase function– Binding to phospholipids– Binding to von Willebrand factor – Behave as serine esterase and hydrolyse FVIII– The Bethesda assay does not see antibodies against the B
domain Modified from Oldenburg et al. Haemophilia. 2002;8(suppl 2):23-29.
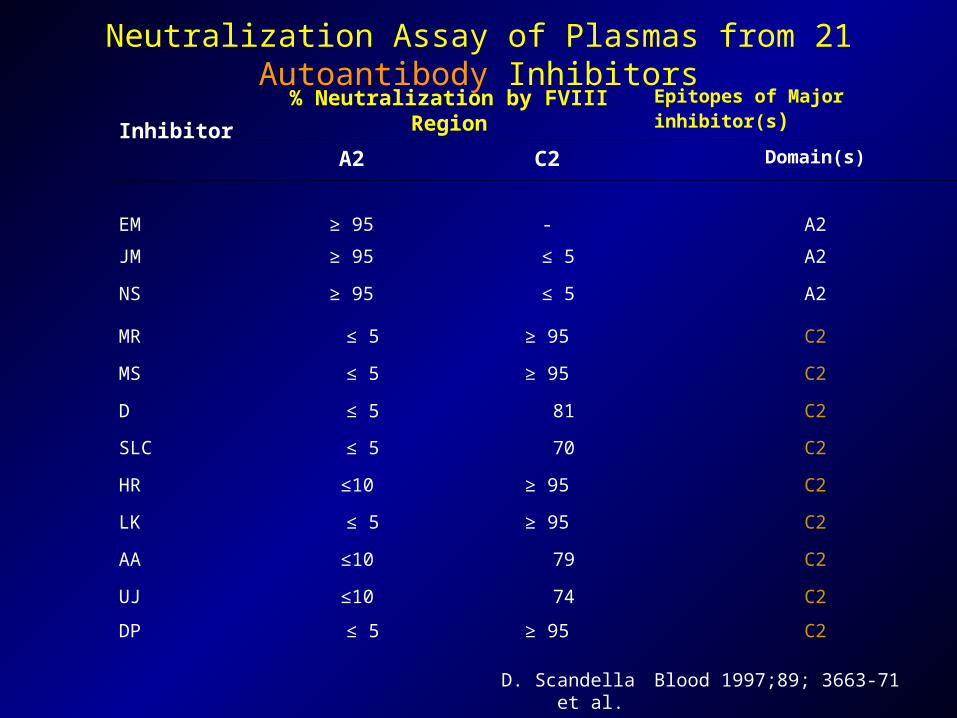
Neutralization Assay of Plasmas from 21 Autoantibody Inhibitors
Inhibitor% Neutralization by FVIII Region Epitopes of Major inhibitor(s)
A2 C2 Domain(s)
EM ≥ 95 - A2
JM ≥ 95 ≤ 5 A2
NS ≥ 95 ≤ 5 A2
MR ≤ 5 ≥ 95 C2
MS ≤ 5 ≥ 95 C2
D ≤ 5 81 C2
SLC ≤ 5 70 C2
HR ≤10 ≥ 95 C2
LK ≤ 5 ≥ 95 C2
AA ≤10 79 C2
UJ ≤10 74 C2
DP ≤ 5 ≥ 95 C2
D. Scandella et al. Blood 1997;89; 3663-71
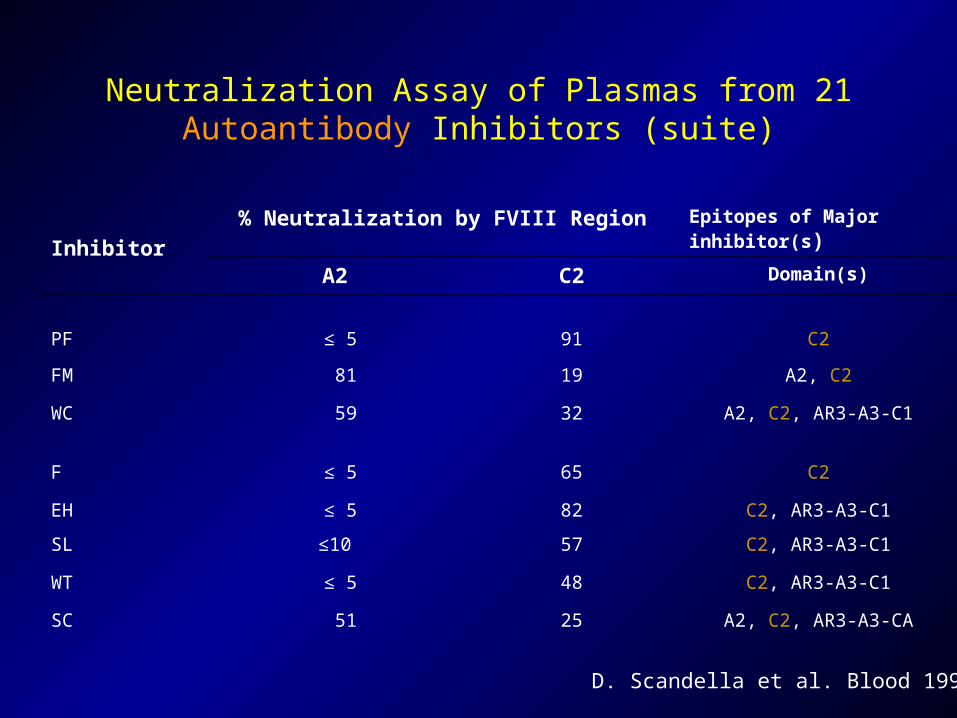
Neutralization Assay of Plasmas from 21 Autoantibody Inhibitors (suite)
Inhibitor% Neutralization by FVIII Region Epitopes of Major
inhibitor(s)
A2 C2 Domain(s)
PF ≤ 5 91 C2
FM 81 19 A2, C2
WC 59 32 A2, C2, AR3-A3-C1
F ≤ 5 65 C2
EH ≤ 5 82 C2, AR3-A3-C1
SL ≤10 57 C2, AR3-A3-C1
WT ≤ 5 48 C2, AR3-A3-C1
SC 51 25 A2, C2, AR3-A3-CA
D. Scandella et al. Blood 1997
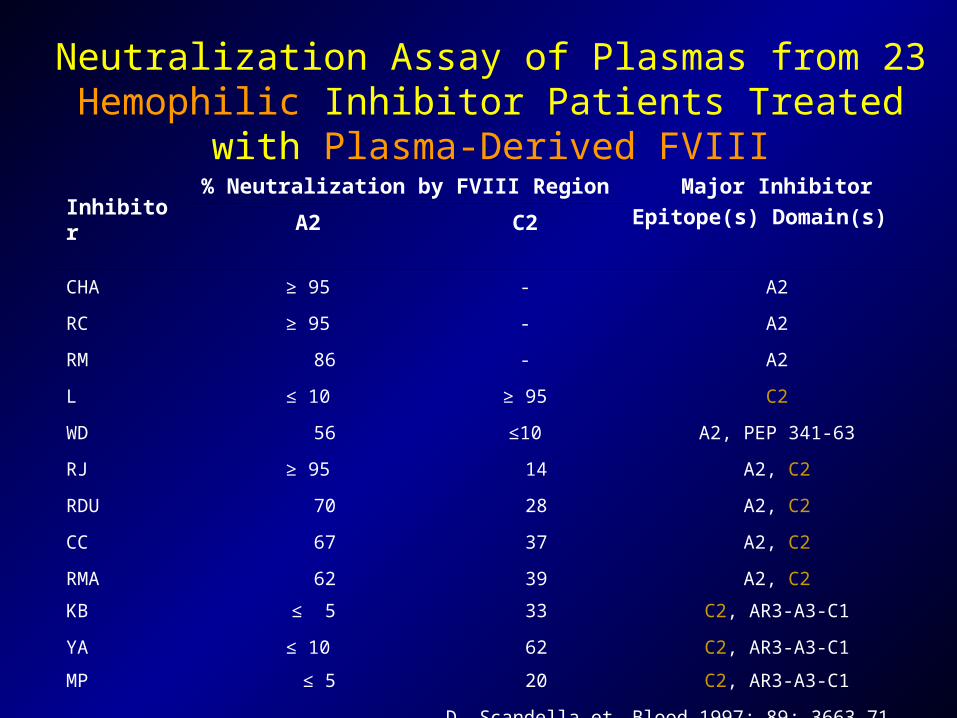
Neutralization Assay of Plasmas from 23 Hemophilic Inhibitor Patients Treated with Plasma-Derived FVIII
Inhibitor
% Neutralization by FVIII Region Major Inhibitor
Epitope(s) Domain(s)A2 C2
CHA ≥ 95 - A2
RC ≥ 95 - A2
RM 86 - A2
L ≤ 10 ≥ 95 C2
WD 56 ≤10 A2, PEP 341-63
RJ ≥ 95 14 A2, C2
RDU 70 28 A2, C2
CC 67 37 A2, C2
RMA 62 39 A2, C2
KB ≤ 5 33 C2, AR3-A3-C1
YA ≤ 10 62 C2, AR3-A3-C1
MP ≤ 5 20 C2, AR3-A3-C1
D. Scandella et al. Blood 1997; 89; 3663-71
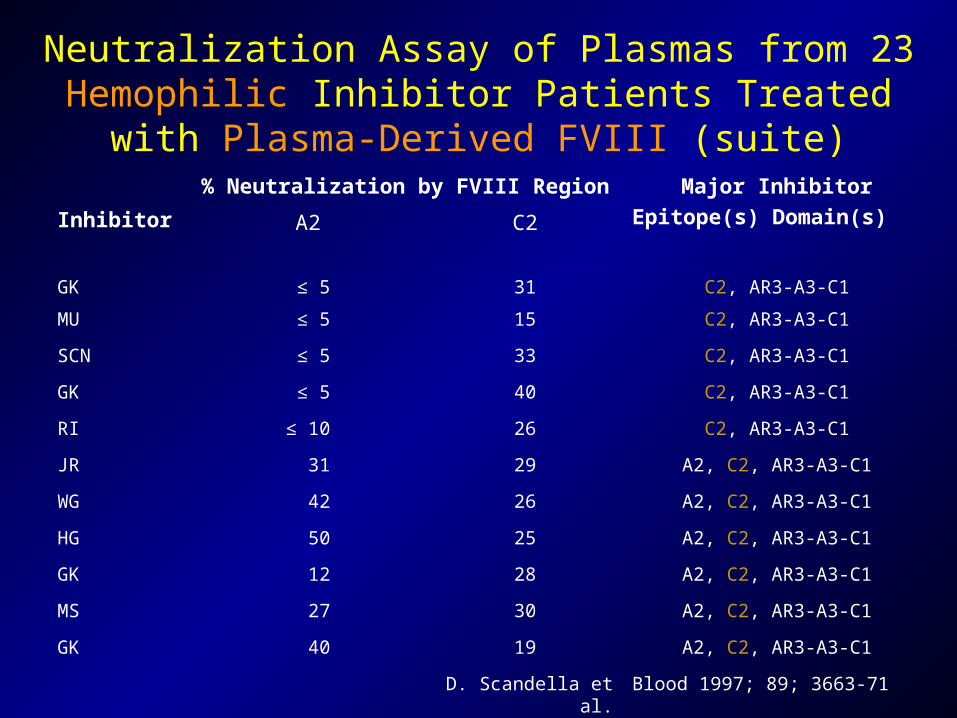
Neutralization Assay of Plasmas from 23 Hemophilic Inhibitor Patients Treated with Plasma-Derived FVIII
(suite)
Inhibitor
% Neutralization by FVIII Region Major Inhibitor
Epitope(s) Domain(s)A2 C2
GK ≤ 5 31 C2, AR3-A3-C1
MU ≤ 5 15 C2, AR3-A3-C1
SCN ≤ 5 33 C2, AR3-A3-C1
GK ≤ 5 40 C2, AR3-A3-C1
RI ≤ 10 26 C2, AR3-A3-C1
JR 31 29 A2, C2, AR3-A3-C1
WG 42 26 A2, C2, AR3-A3-C1
HG 50 25 A2, C2, AR3-A3-C1
GK 12 28 A2, C2, AR3-A3-C1
MS 27 30 A2, C2, AR3-A3-C1
GK 40 19 A2, C2, AR3-A3-C1
D. Scandella et al. Blood 1997; 89; 3663-71
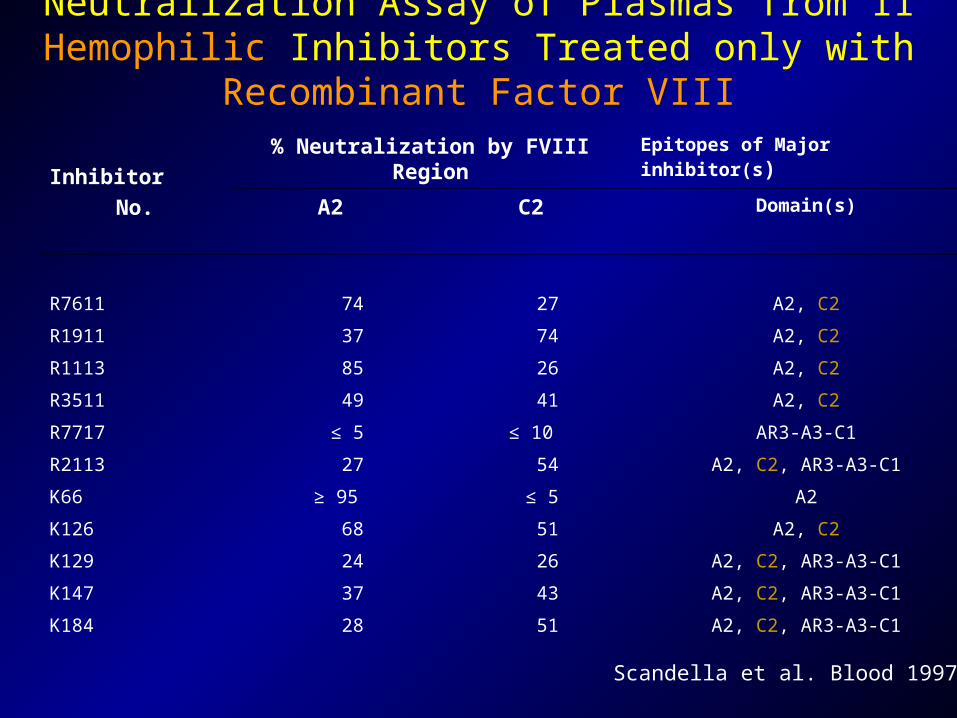
Neutralization Assay of Plasmas from 11 Hemophilic Inhibitors Treated only with Recombinant Factor VIII
Inhibitor
No.
% Neutralization by FVIII Region Epitopes of Major inhibitor(s)
A2 C2 Domain(s)
R7611 74 27 A2, C2
R1911 37 74 A2, C2
R1113 85 26 A2, C2
R3511 49 41 A2, C2
R7717 ≤ 5 ≤ 10 AR3-A3-C1
R2113 27 54 A2, C2, AR3-A3-C1
K66 ≥ 95 ≤ 5 A2
K126 68 51 A2, C2
K129 24 26 A2, C2, AR3-A3-C1
K147 37 43 A2, C2, AR3-A3-C1
K184 28 51 A2, C2, AR3-A3-C1
Scandella et al. Blood 1997

vWF/PL
Factor VIII Inhibitory AntibodiesFIXavWFFIXaFX
COOH
2332217320251648719336
NH2
The Bethesda assay does not see antibodies against the B
domainModified from Oldenburg et al. Haemophilia. 2002;8(suppl 2):23-29.
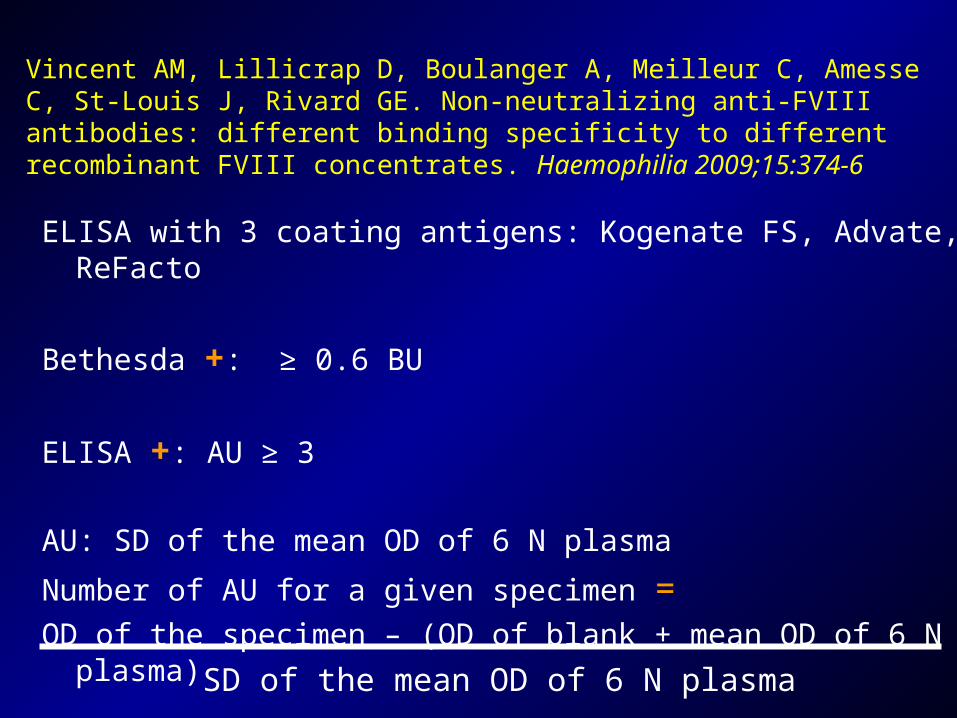
Vincent AM, Lillicrap D, Boulanger A, Meilleur C, Amesse C, St-Louis J, Rivard GE. Non-neutralizing anti-FVIII antibodies: different binding specificity to different recombinant FVIII concentrates. Haemophilia 2009;15:374-6
ELISA with 3 coating antigens: Kogenate FS, Advate, ReFacto
Bethesda +: ≥ 0.6 BU
ELISA +: AU ≥ 3
AU: SD of the mean OD of 6 N plasma
Number of AU for a given specimen =OD of the specimen – (OD of blank + mean OD of 6 N plasma)
SD of the mean OD of 6 N plasma
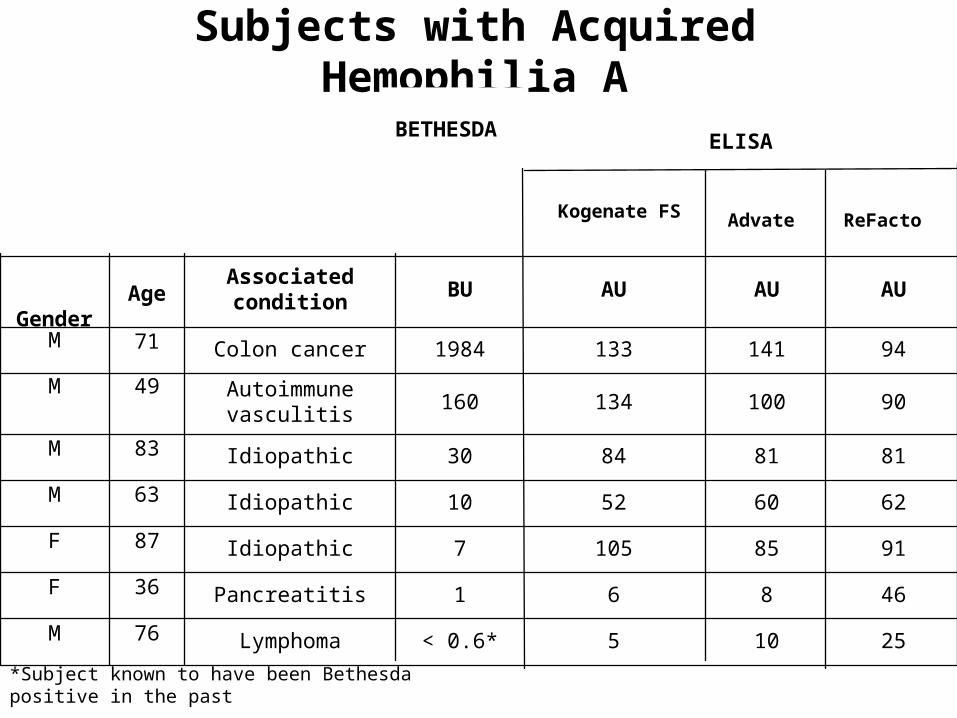
Subjects with Acquired Hemophilia A
25105< 0.6*Lymphoma76M
46861Pancreatitis36F
91851057Idiopathic87F
62605210Idiopathic63M
81818430Idiopathic83M
90100134160Autoimmune
vasculitis49M
941411331984Colon cancer71M
AUAUAUBUAssociated condition Age
Gender
ReFacto
Advate
Kogenate FS
ELISABETHESDA
*Subject known to have been Bethesda positive in the past

4114< 0.6*5< 0,016
1837460.64< 0,015
136111.5> 20< 0,0147
23764.210< 0,0112
30192782< 0,012
509251166< 0,018
8514591366< 0,017
1019510678> 20< 0,0160
971131211654< 0,015
9580130512> 20< 0,0134
125711185703< 0,015
AUAUAUBUDuration of inhibitor
(years)Baseline
FVIIIAge
ReFactoAdvateKogenate FS
ELISABETHESDA
*Subject known to have been Bethesda positive in the past.
Subjects with Congenital Hemophilia A and Inhibitor

0.223 < 0.60,03
0.124< 0.6< 0,01
0310< 0.6< 0,01
-12321 < 0.6< 0,01
-0.54436 < 0.6< 0,01
0.26366< 0.60,05
AUAUAUBUBaseline FVIII
ReFacto Advate Kogenate FS
ELISABETHESDA
Subjects with Congenital Hemophilia A without Inhibitor
Contributing Factors to Development of FVIII Inhibitors
• Genetic Related to factor VIII Unrelated to factor VIII
• Environmental Conditions of treatment Therapeutic product

Contributing Factors to Development of FVIII Inhibitors
• Genetic Related to factor VIII Unrelated to factor VIII
• Environmental Conditions of treatment Therapeutic product
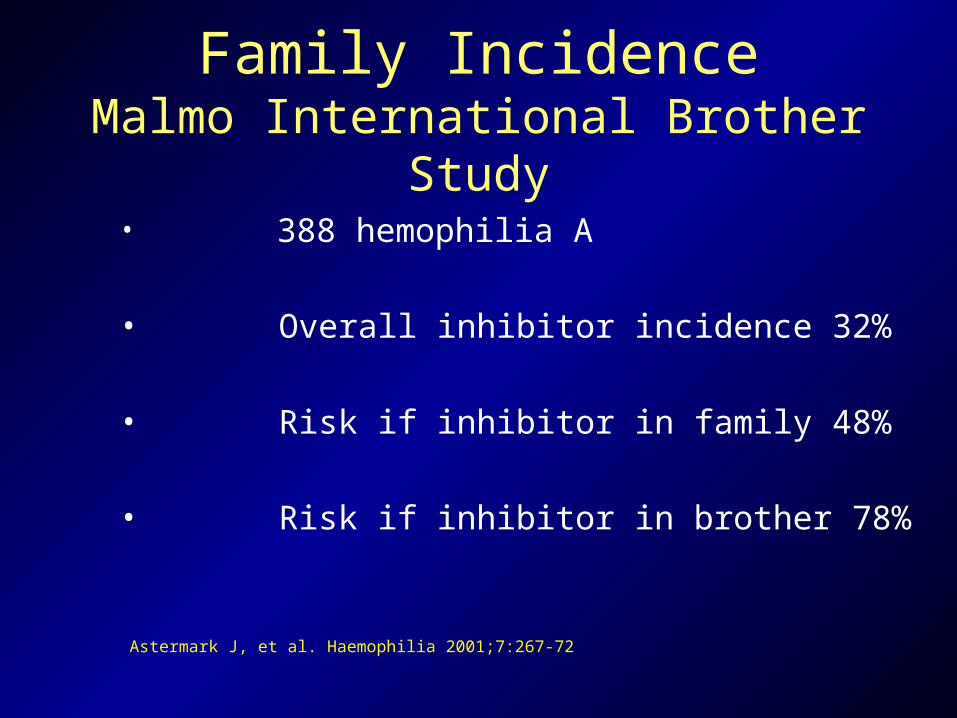
Family IncidenceMalmo International Brother Study
• 388 hemophilia A
• Overall inhibitor incidence 32%
• Risk if inhibitor in family 48%
• Risk if inhibitor in brother 78%
Astermark J, et al. Haemophilia 2001;7:267-72
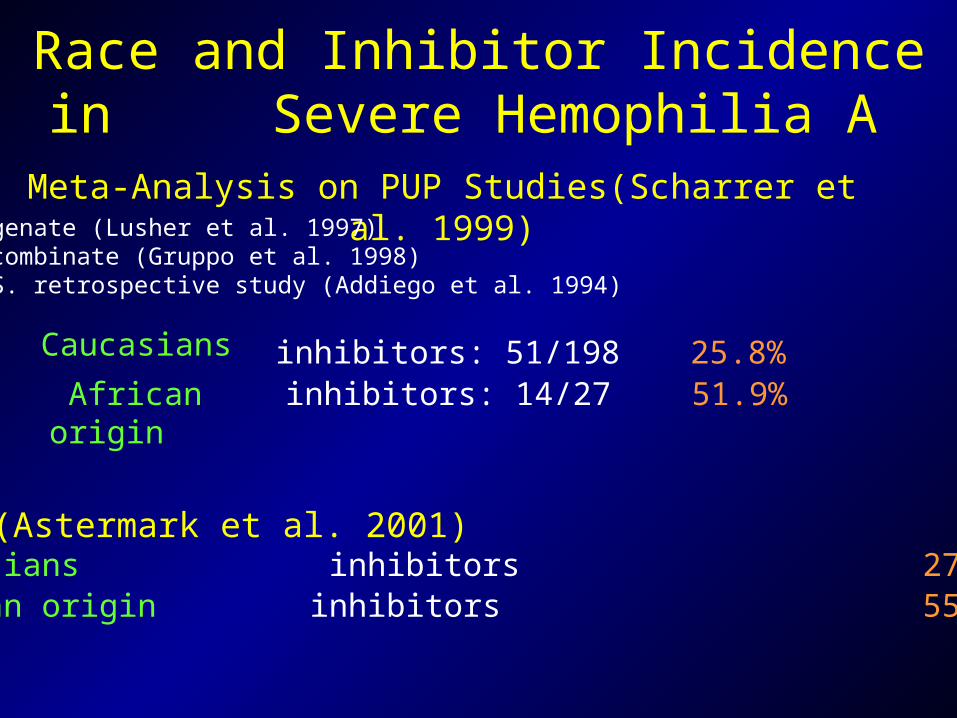
Race and Inhibitor Incidence in Severe Hemophilia A
Meta-Analysis on PUP Studies(Scharrer et al. 1999)Kogenate (Lusher et al. 1997) Recombinate (Gruppo et al. 1998) U.S. retrospective study (Addiego et al. 1994)
Caucasians inhibitors: 51/198 25.8% African origin inhibitors: 14/27 51.9%
MIBS (Astermark et al. 2001)Caucasians inhibitors 27.4%African origin inhibitors 55.6%

Contributing Factors to Development of FVIII Inhibitors
• Genetic Related to factor VIII Unrelated to factor VIII
• Environmental Conditions of treatment Therapeutic product
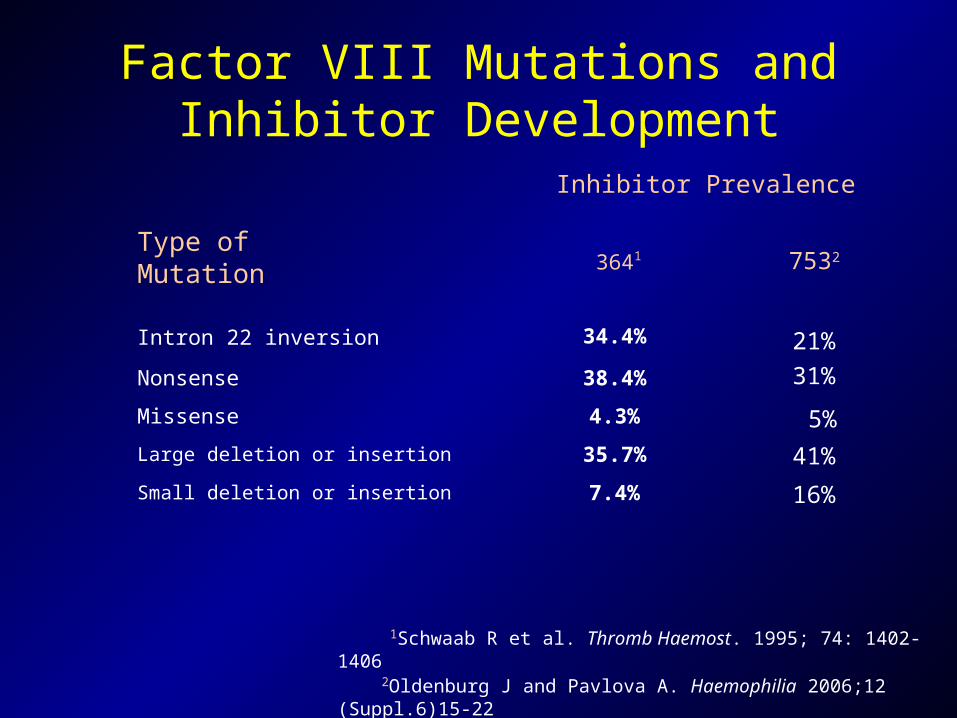
3641
7.4%Small deletion or insertion
35.7%Large deletion or insertion
4.3%Missense
38.4%Nonsense
34.4%Intron 22 inversion
Inhibitor Prevalence
Type of Mutation
1Schwaab R et al. Thromb Haemost. 1995; 74: 1402-1406 2Oldenburg J and Pavlova A. Haemophilia 2006;12 (Suppl.6)15-22
Factor VIII Mutations and Inhibitor Development
7532
21%
31%
5%
41%
16%
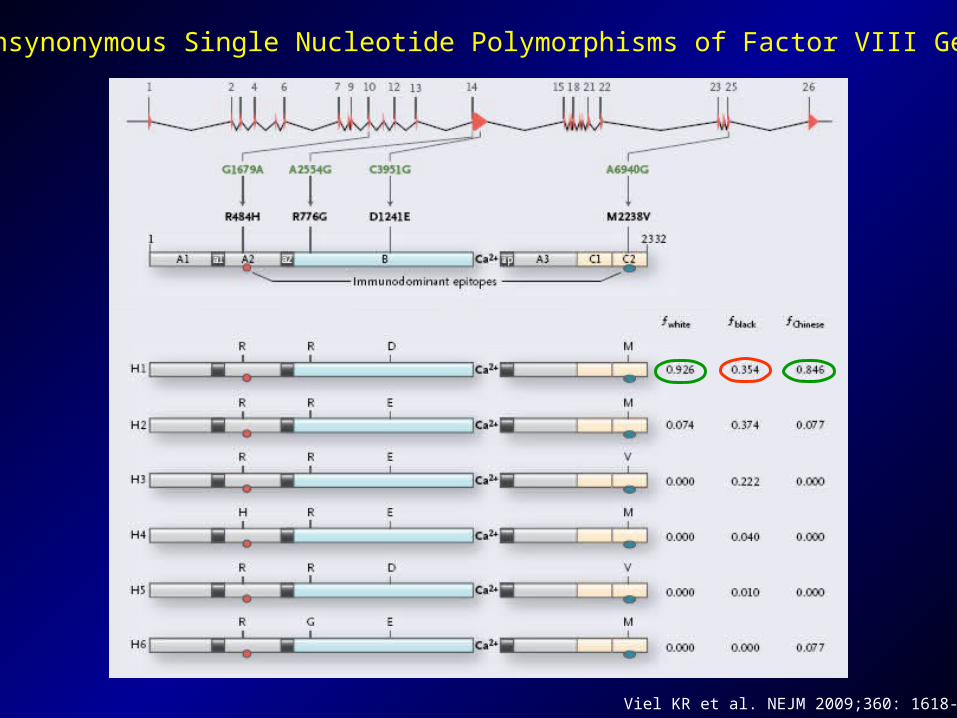
Nonsynonymous Single Nucleotide Polymorphisms of Factor VIII Gene
Viel KR et al. NEJM 2009;360: 1618-27

Inhibitor of Factor VIII in Black Patients with Hemophilia Kevin R. Viel et al. NEJM 2009; 360: 1618-27
Nonsynonymous Single Nucleotide Polymorphisms of Factor VIII Gene and Risk of Inhibitor Development
Contributing Factors to Development of FVIII Inhibitors
• Genetic Related to factor VIII Unrelated to factor VIII
• Environmental Conditions of treatment Therapeutic product
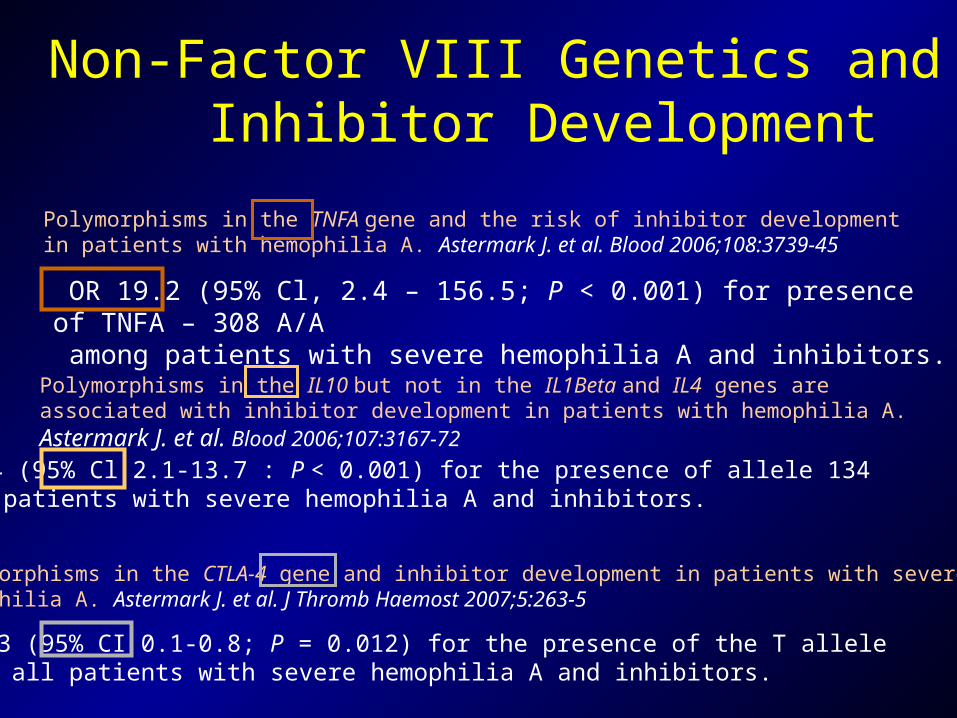
Non-Factor VIII Genetics and Inhibitor Development
OR 19.2 (95% Cl, 2.4 – 156.5; P < 0.001) for presence of TNFA – 308 A/A among patients with severe hemophilia A and inhibitors.
Polymorphisms in the TNFA gene and the risk of inhibitor development in patients with hemophilia A. Astermark J. et al. Blood 2006;108:3739-45
OR 5.4 (95% Cl 2.1-13.7 : P < 0.001) for the presence of allele 134 among patients with severe hemophilia A and inhibitors.
Polymorphisms in the IL10 but not in the IL1Beta and IL4 genes are associated with inhibitor development in patients with hemophilia A. Astermark J. et al. Blood 2006;107:3167-72
OR 0.3 (95% CI 0.1-0.8; P = 0.012) for the presence of the T allele among all patients with severe hemophilia A and inhibitors.
Polymorphisms in the CTLA-4 gene and inhibitor development in patients with severehemophilia A. Astermark J. et al. J Thromb Haemost 2007;5:263-5
Contributing Factors to Development of FVIII Inhibitors
• Genetic Related to factor VIII Unrelated to factor VIII
• Environmental Conditions of treatment Therapeutic product
– Associated inflammatory reactions
– Continuous infusion1
– Age at first treatment2
– Episodes of intensive treatment
1Sharathkumar 2003; 2van der Bom 2003
Contributing Factors to Development of FVIII Inhibitors: Conditions of Treatment

Contributing Factors to Development of FVIII Inhibitors
• Genetic Related to factor VIII Unrelated to factor VIII
• Environmental Conditions of treatment Therapeutic product
Contributing Factors to Development of FVIII Inhibitors:Therapeutic Product
• In vivo human data
• In vivo animal data
• In vitro data
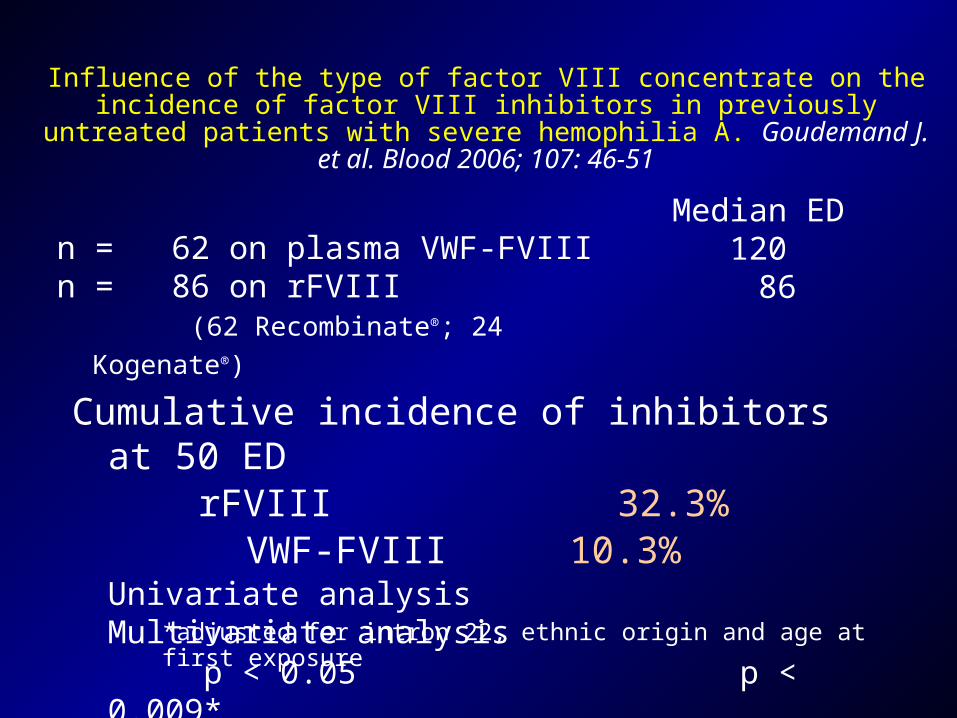
Influence of the type of factor VIII concentrate on the incidence of factor VIII inhibitors in previously untreated patients with severe hemophilia A.
Goudemand J. et al. Blood 2006; 107: 46-51
Cumulative incidence of inhibitors at 50 ED rFVIII 32.3%VWF-FVIII 10.3%
Univariate analysis Multivariate analysis p < 0.05 p < 0.009*
*adjusted for intron 22, ethnic origin and age at first exposure
n = 62 on plasma VWF-FVIII n = 86 on rFVIII (62 Recombinate®; 24 Kogenate®)
Median ED120 86
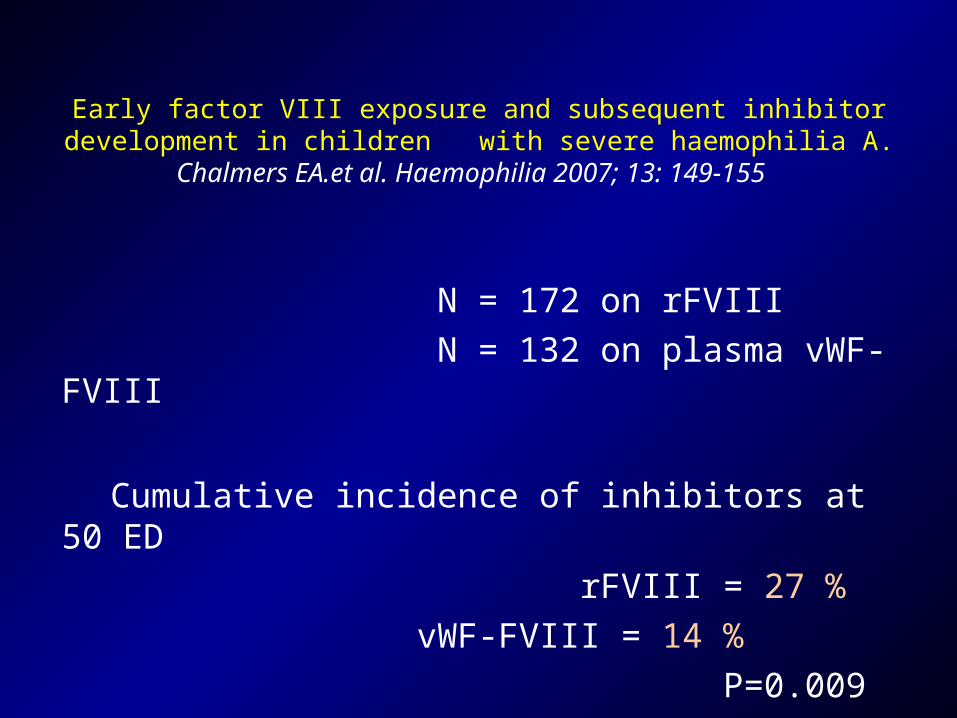
Early factor VIII exposure and subsequent inhibitor development in children with severe haemophilia A. Chalmers EA.et al. Haemophilia 2007; 13: 149-155
N = 172 on rFVIII
N = 132 on plasma vWF- FVIII
Cumulative incidence of inhibitors at 50 ED
rFVIII = 27 %
vWF-FVIII = 14 %
P=0.009
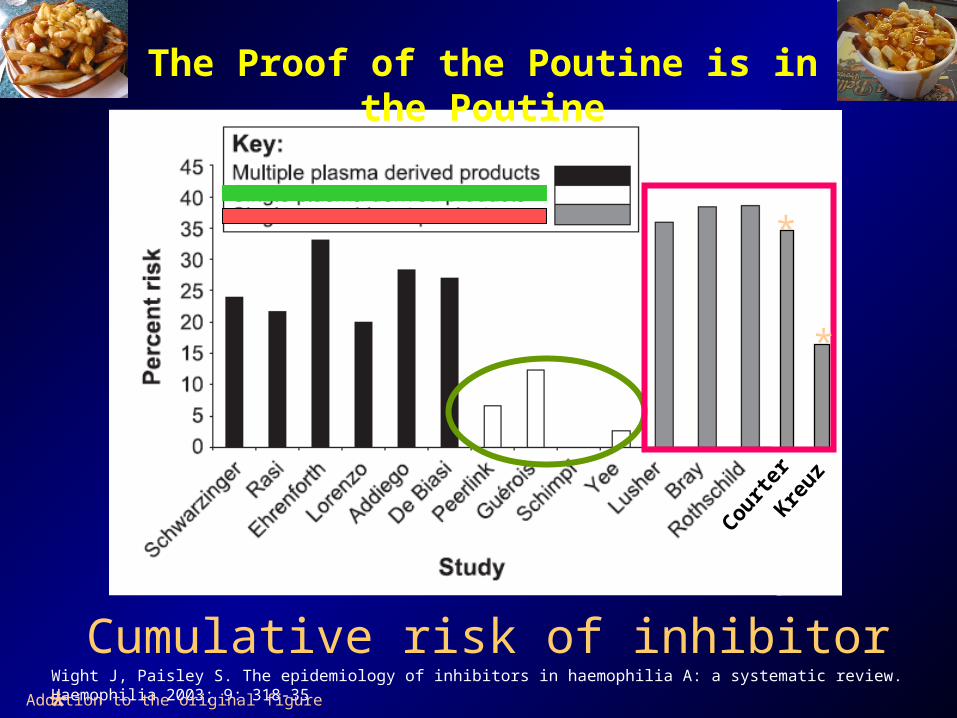
Kreuz
Courte
r
Wight J, Paisley S. The epidemiology of inhibitors in haemophilia A: a systematic review. Haemophilia 2003; 9: 318-35
Cumulative risk of inhibitor
The Proof of the Poutine is in the Poutine
*
*
* Addition to the original figure
Treatment of Subjects with Hemophilia A and FVIII Inhibitors: General Comments
• Control of hemostasis: Human FVIII, not effective except in low titres
Porcine FVIII, no longer available
Activated Prothrombin Concentrates (FEIBA)
Recombinant Activated FVII (NiaStase)
• Elimination of inhibitors: Immune Tolerance Induction
Immunosuppression/Immunomodulation
Summary
• Acquired hemophilia A is a rare but serious condition with a peak of incidence in elderly subjects; it could be life threatening but usually responds well to appropriate treatment
• Factor VIII inhibitor development is a common and severe complication of hemophilia A treatment
• There are many genetic and environment factors that contribute to development of inhibitors in hemophilia A
• There are some reasonably effective treatment for the control of hemostasis and the eradication of inhibitors: both aspects of treatment are extremely expensive
• Better strategies for prevention and treatment of this condition are badly needed; more research is needed…
An Interesting Bed Time Story…
Interesting???