extrapyramidal disorders
TRANSCRIPT
NOTE:
To change
the image
on this
slide,
select the
picture
and delete
it. Then
click the
Pictures
icon in the
placeholde
r to insert
your own
image.
Amr Hassan, M.D. Associate professor of Neurology - Cairo University
EXTRAPYRAMIDAL
DISORDERS

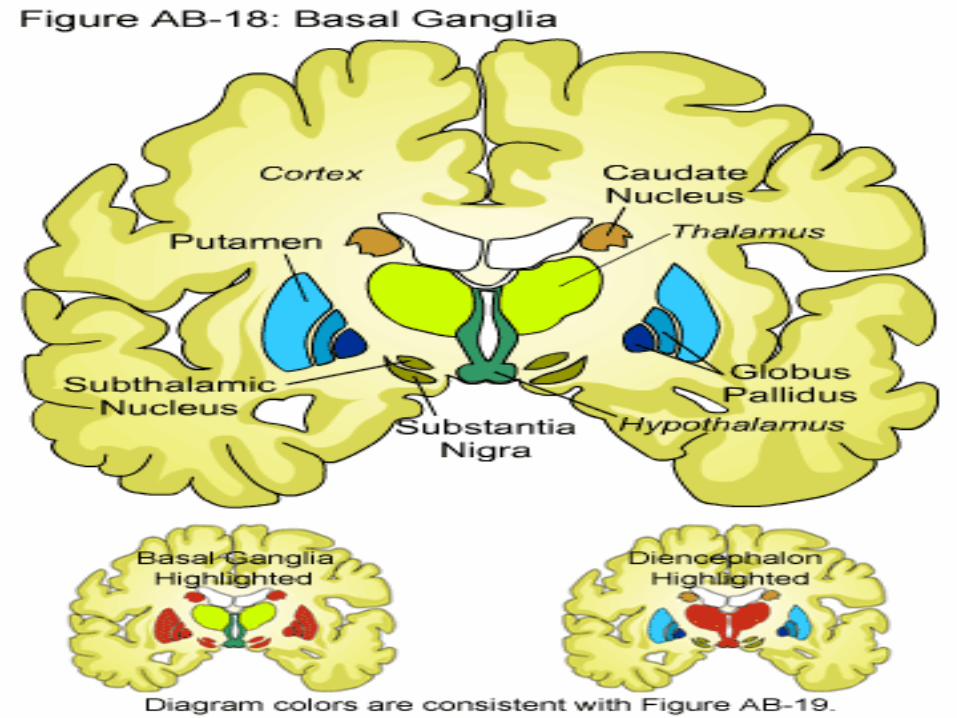
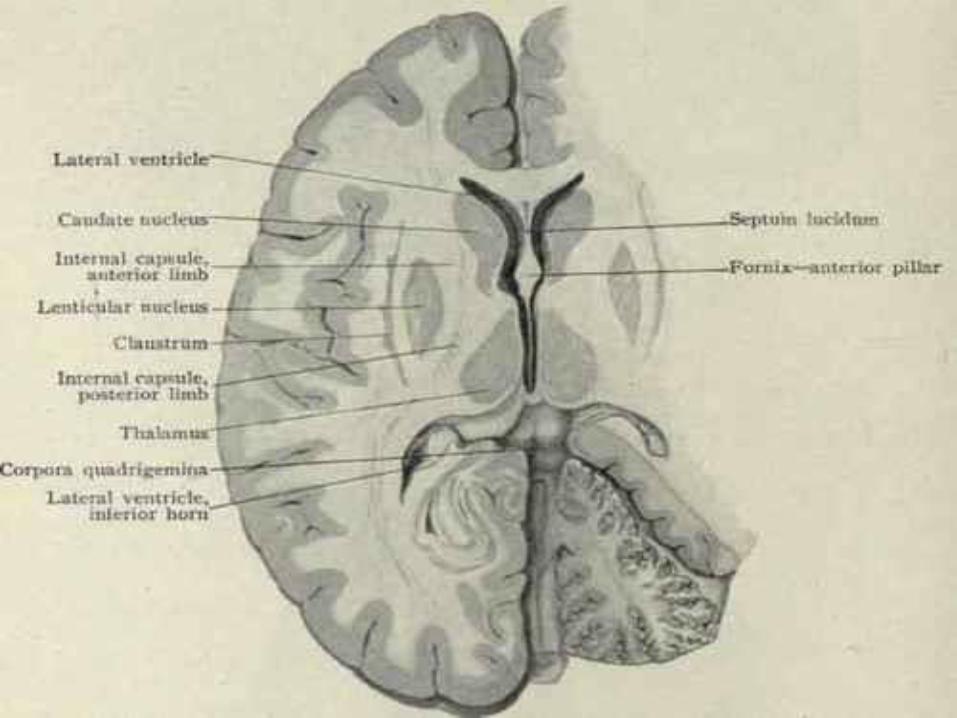
Basal ganglia Anatomy:
A group of brain nuclei are known collectively as the basal ganglia.
The basal ganglia include caudate nucleus, the putamen , the globus pallidus ,the subthalamic nucleus ,and the substantia nigra.
The motor components of the basal ganglia make up the extrapyramidal motor system that comprise fibers that influence the motor end plate activity and do not pass in the pyramidal tract.
The caudate nucleus and putamen are collectively known as the corpus striatum (i.e. striated body) because of their appearance.
Similarly, the shape of the putamen and globus pallidus resembles a lens, and they are collectively called the lentiform nucleus.

Basal ganglia Functions:
Regulation and integration of voluntary motor activity.
Regulation and maintenance of the muscle tone.
Regulation and maintenance of emotional and associative
movements.
Basal ganglia Extrapyramidal disorders (=movement disorders):
Parkinsonism..
Chorea.
Dystonia.
Athetosis.

Parkinsonism
Definition:
The term parkinsonism is used for a motor syndrome whose main symptoms are rest tremor, rigidity, bradykinesia and postural instability.
Types:
Parkinsonian syndromes can be divided into four subtypes according to their origin:
Primary or idiopathic (Parkinson’s disease).
Secondary or acquired.
Hereditary parkinsonism.
Parkinson plus syndromes.
Parkinson’s disease
It is a "primary" parkinsonism, meaning parkinsonism with
no external identifiable cause.
Pathogenesis:
There is degeneration of the pigmented cells of the substantia nigra, which becomes pale deficiency of dopamine in the brain imbalance between the levels of acetylcholine and dopamine in the basal ganglia and substantia nigra.
Clinical picture:
The age of onset is above 50 years. Both sexes are equally affected.

Rest (static) tremors:
•Due to disturbance in the integration and regulation of voluntary motor activity. •Rhythmic and regular, occur at the rate of 4-8/second. •↑ With emotional stress, anxiety and fatigue. •Disappear during sleep and during active voluntary movements. •Begin unilaterally in the U.L. and spread to all 4 limbs. •They give the hand the pill-rolling posture with the thumb moving rhythmically back and forward on the palm.

Rigidity:
Due to disturbance in the regulation and
maintenance of normal muscle tone resulting in
hypertonia.
Affecting the proximal more than the distal
muscles.
Affecting more the flexors of the neck, trunk
limbs resulting in the gorilla-like attitude.
It may be present throughout the act to the
same degree & is then described as lead pipe
rigidity; it may be interrupted by the tremors
& is then described as cog wheel rigidity.
Causing difficulty in starting the act of
walking leading to a slow, shuffling
(festinanting or short steppage) gait with
propulsion.

Bradykinesia:
Due to disturbance in the regulation
and maintenance of emotional
and associated movements.
Mask face= expressionless face
with
infrequent blinking.
Loss of swinging of arms during
walking.
Monotonus speech.
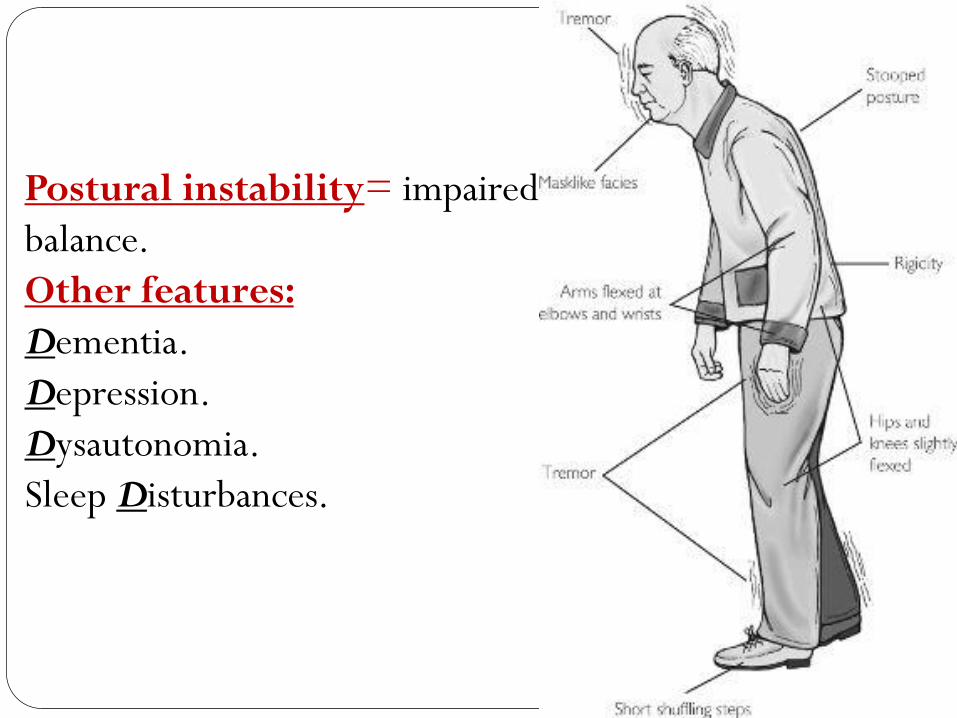
Postural instability= impaired
balance.
Other features:
Dementia.
Depression.
Dysautonomia.
Sleep Disturbances.

The UPDRS (Unified Parkinson’s Disease Rating Scale)has
long been the major rating scale that is used to assess severity
of symptoms of Parkinson's disease. It can assess:
Daily activities.
Motor skills.
Mental capacity (including behavior and mood).
Complication of therapy.

Treatment of Parkinsonism
A. Medical
Aims to restore the balance between acetylcholine & dopamine by decreasing acetylcholine and/or elevating dopamine levels. Anticholinergic drugs.
Dopaminergic drugs: i.e. Levo-Dopa + Carbi-Dopa (Sinemet) and Dopamine agonists.
Amantadine hvdrochloride.
Physical therapy
Supportive treatment:
Good nutrition.
Regular rest periods and avoiding stress.
Speech therapy.
Occupational therapy.
Interventional therapy
Deep brain stimulation involves placing electrical stimulators in specific areas of the brain that control movement.
Stem cell transplantation.
Surgery e.g. pallidotomy.

II. Chorea
Involuntary
Static
Irregular
Dysrhythmic
Sudden
Jerky
Pseudopurposive
Of any part of the body
II. Chorea
Causes:
I. Herido-familial: Huntington's chorea.
II. Acquired :
Autoimmune: Rheumatic chorea.
Infective: Post encephalitic chorea.
Vascular: Hemiballismus.
Toxic: Chorea gravidarum.
Idiopathic: Senile chorea.

II. Chorea Clinical picture:
1. Choreic movements: Affecting the tongue, facial, trunk and extremities muscles, being more proximal than distal.
Grimacing, jerking of the shoulders, shaking of the hands and feet.
↑ With emotional stress and anxiety. Disappear during sleep.
2. Hypotonia.
Treatment: Dopamin blocking agent. Treatment of the cause.

III. Athetosis
Involuntary
Static
Irregular
Slow
Snake-like movemets
Mainly extremities and face
hypertonia

III.Athetosis
Causes:
Congenital: e.g. hypoxic neonatal brain damage.
Acquired: Post-encephalitic.
Treatment:
Anticholinergic drugs
Dystonia
Definition:
It is abnormal involuntary, static, very slow, torsion or twisting
like movements commonly involve the neck, trunk &. the
proximal muscles of the extremities. They are associated with
hypertonia during the movement & normal tone in between.

Dystonia
Causes:
Primary or idiopathic dystonia: dystonia occurs as a solitary
symptom and is not associated with an underlying disorder
e.g. Early-onset primary dystonia are due to a mutation in the
dyt-1 gene.
Secondary or symptomatic dystonia: dystonia occurs because
of another underlying disease process e.g. Wilson disease,
stroke, brain trauma or medications.

Dystonia Classification: Dystonia may also be classified as follows, according
to the bodily distribution of symptoms:
Focal dystonia: limited to one region of the body e.g. neck (see
fig. 57) or an arm or a leg.
Segmental dystonia: affecting two adjacent areas of the body e.g.
the head and neck.
Multifocal dystonia: affecting two areas of the body that are not
next to each other, such as the two arms, or an arm and a leg.
Generalized dystonia: symptoms begin in an arm or a leg and
advance, becoming more widespread. Eventually, the trunk and
the rest of the body are involved.


Dystonia
Treatment:
]In 2ry dystonia: treatment of the cause
Treatment of dystonia:
Oral medications e.g. benzodiazepine.
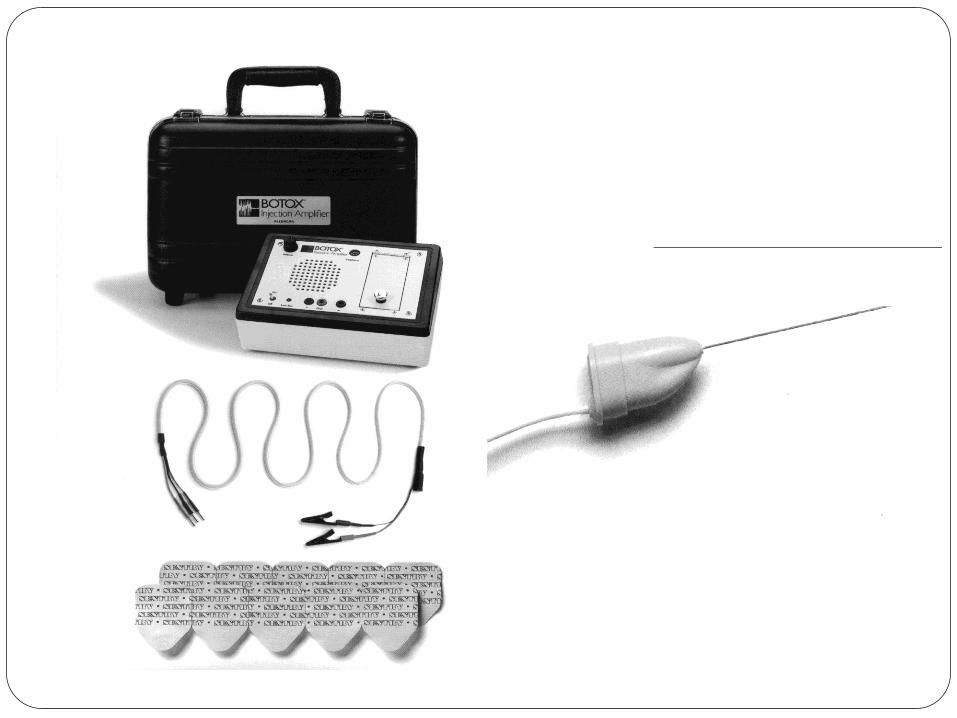
Botulinum toxin injection (Botox):

Dystonia Botulinum toxin injection (Botox):
Botulinum toxin is a toxic protein that is produced by the bacterium Clostridium botulinum. This toxin is known to cause botulism, a deadly form of food poisoning that is contracted through the ingestion of contaminated food products.
However, when a minute amount of commercially prepared Botulinum toxin (Botox) is injected directly into an overactive muscle block the release of acetylcholine relaxes that muscle decreases inappropriate or excessive muscle contractions allowing the affected area (e.g., arm, neck, leg, eyelid, etc.) to assume a more normal position or posture.
Surgery.
Deep brain stimulation.
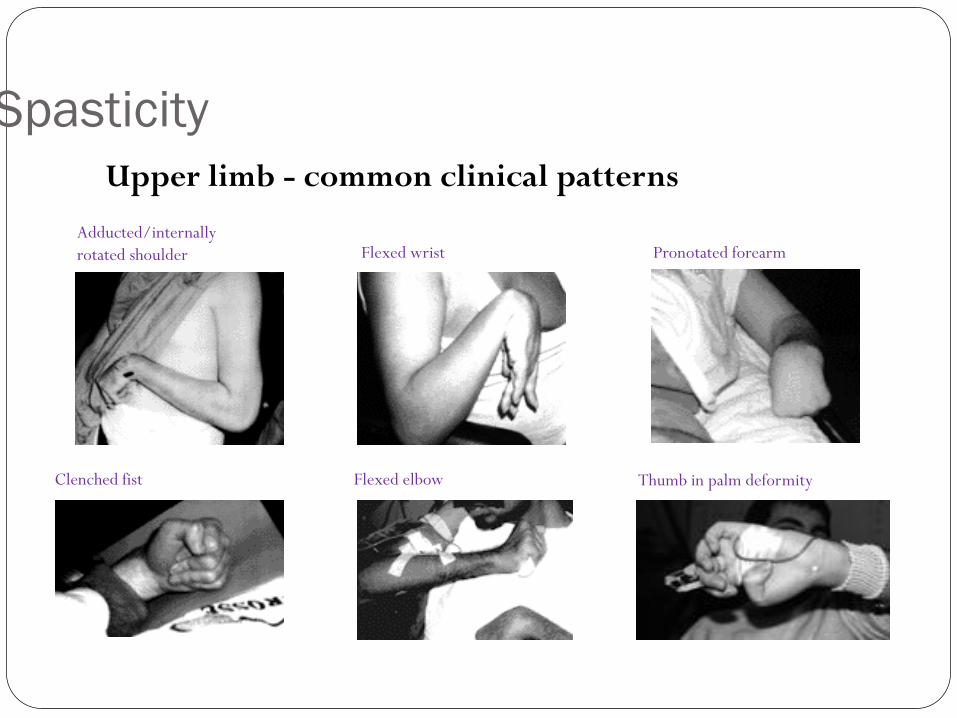
Spasticity
Upper limb - common clinical patterns
Adducted/internally
rotated shoulder Flexed wrist Pronotated forearm
Clenched fist Flexed elbow Thumb in palm deformity

Spasticity
Lower limb – common clinical patterns
Equinovarus Striatal toe
Stiff knee Flexed knee Adducted thighs



Thank you