extra ocular muscles ppt
TRANSCRIPT

Figure 1.
Figure 2.
Figure 3.Figure 4 .
Write down the answers
In the Figures 1-41. Which eye is abnormal ?2. What is the abnormality ?3. Name the cranial nerve involved.4. Name the muscles supplied by that cranial
nerve
EXTRAOCULAR MUSCLES
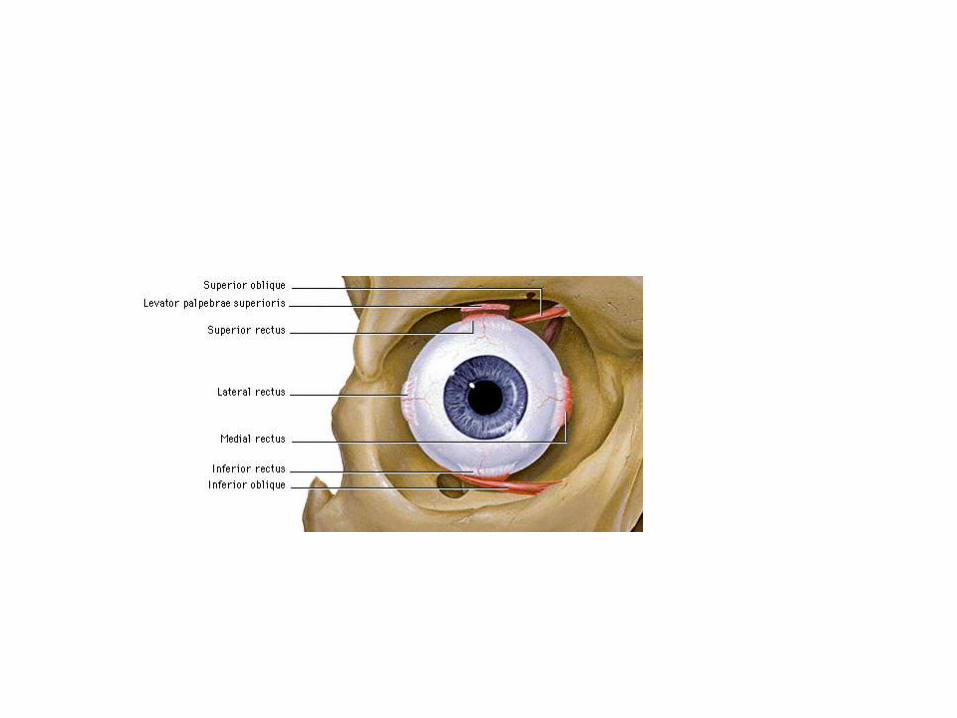
Extraocular muscles
4 Recti and 2 ObliquesSuperior rectus Superior obliqueInferior rectus Inferior obliqueMedial rectusLateral rectus
Levator palpebrae superioris

LEVATOR PALPEBRAE SUPERIORISOrigin: Undersurface of lesser wing of sphenoid above optic canal
Insertion: Skin of upper eyelidsAnterior surface of superior tarsusMuller`s muscle/Superior tarsal
muscle Superior conjunctival fornix


LEVATOR PALPEBRAE SUPERIORISNerve supply and Actions
Paralysis - PTOSIS
Oculomotor nerve, Sympathetics
Elevates upper lid

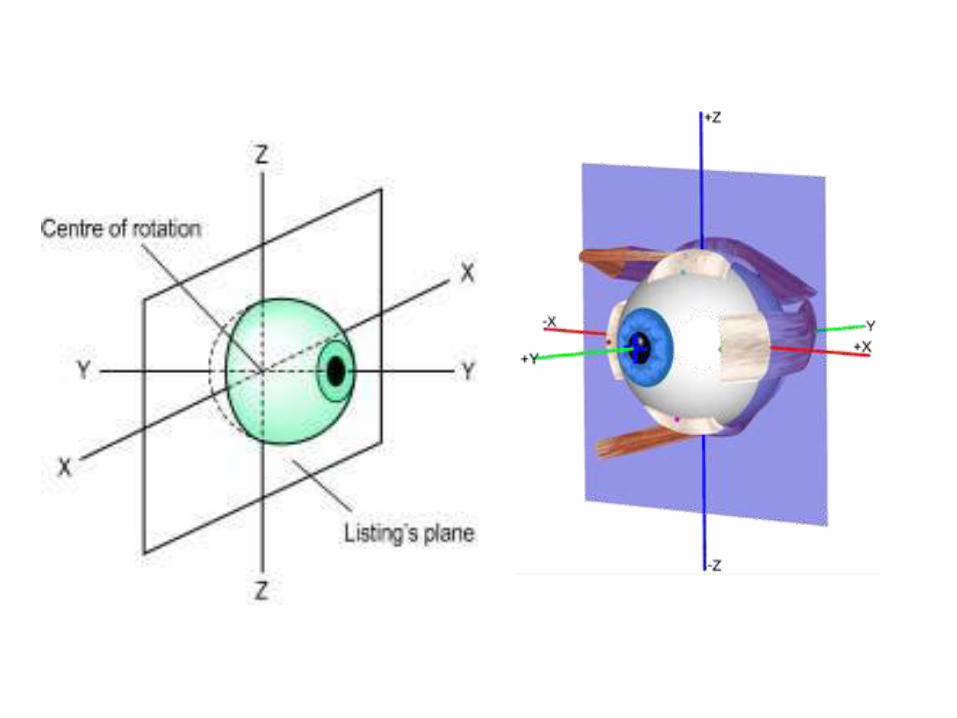
EquatorOptical axis/Axis of Gaze – direction of sight .Primary position of eye
Axis of movements
Axis of muscles

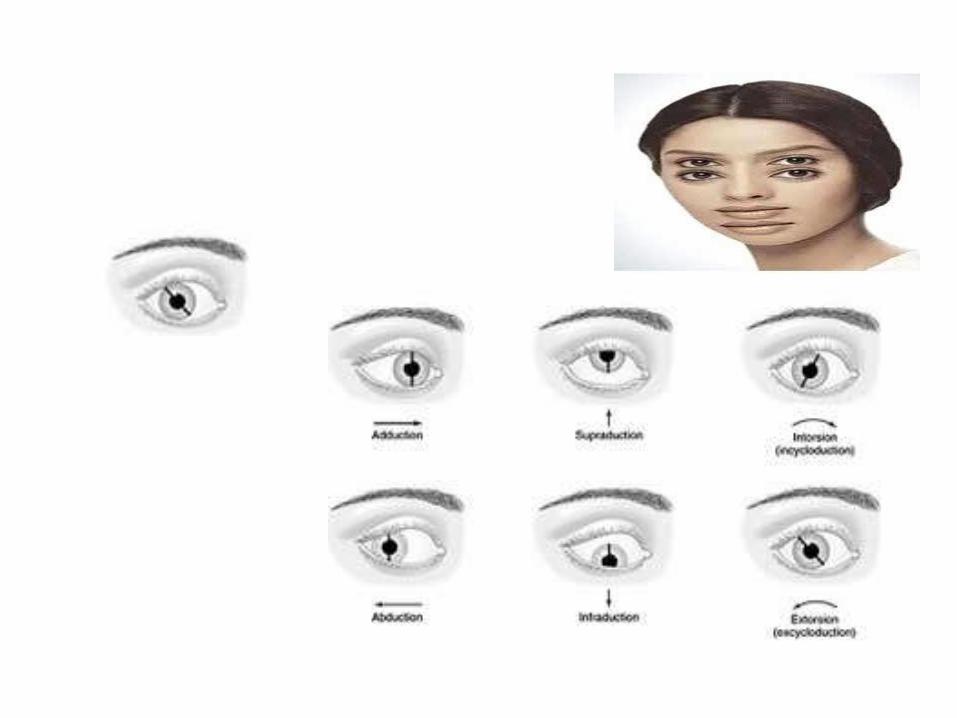
Movements
Abduction
Elevation
Depression
Adduction Intorsion
Extorsion
Elevation & Depression – Around the transverse axisAdduction & Abduction – Around the vertical axisIntortion & Extortion – Around the anteroposterior axis

And the RULE is…..(for recti and oblique)Any muscle inserting
medial to vertical axis – Adductionlateral to vertical axis - Abductionsuperior to AP axis – Intorsioninferior to AP axis – Extorsion
For muscle inserting in front of equator i.e RECTIabove transverse axis – Elevationbelow transverse axis - Depression

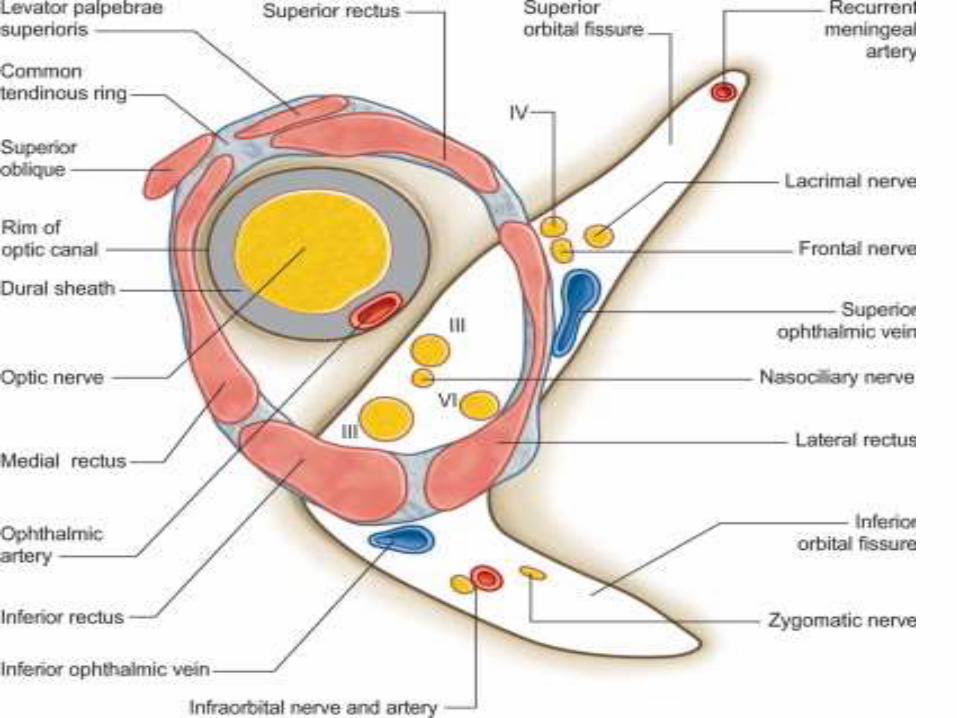
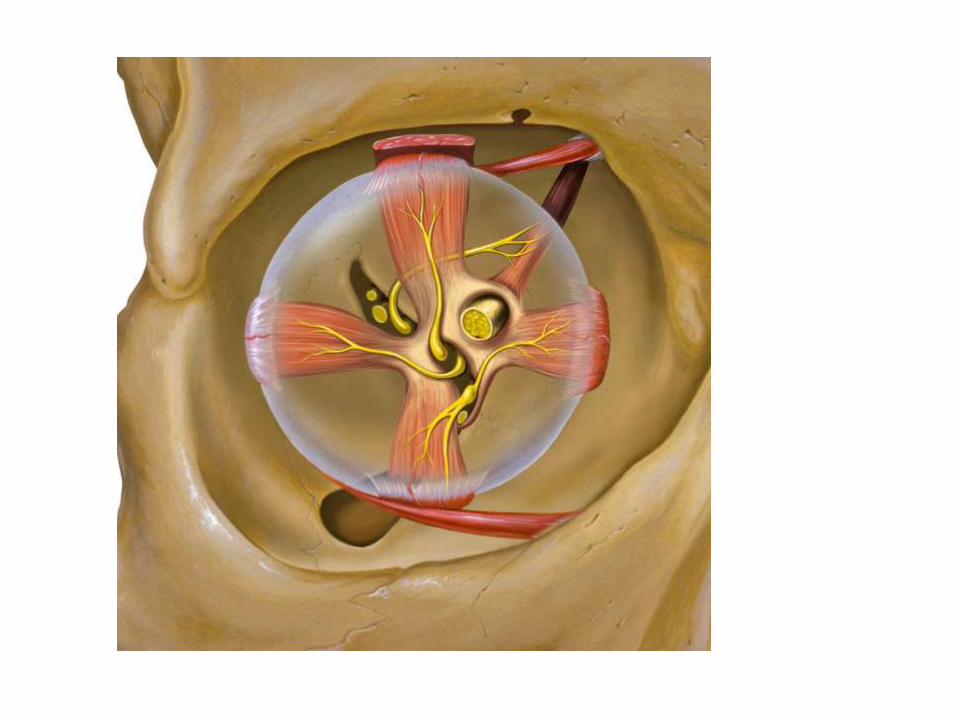
ORIGIN OF THE 4 RECTI MUSCLE
Common tendinous ring(Annulus of Zinn)
•Lateral rectus by 2 heads–Extra head from adjoining greater wing of sphenoid
LEFT EYE

COURSE OF THE 4 RECTIMuscular cone
Corresponding wall of orbit
Rectus muscle length – 40mm
Innervated from intraconalside of the muscle belly at the
junction of anterior 2/3 andposterior 1/3 of the muscle

INSERTION OF THE 4 RECTI
The line connecting the insertion of the recti in series is spiral & is known as spiral line of Tillaux
Pierce Tenon’scapsule
Sclera in front of the equator
Medial rectus is susceptible to injury during anterior segment procedures

AXES OF THE RECTI MUSCLEMedial and lateral recti in same horizontal plane
Superior and inferior recti in same oblique plane, 25⁰lateral to optical axis
In the abducted eye the axes coincide

Action of the RECTI• Medial & lateral recti lie in the same horizontal plane
Around a vertical axis
Medial rectus - adduction Lateral rectus -abduction
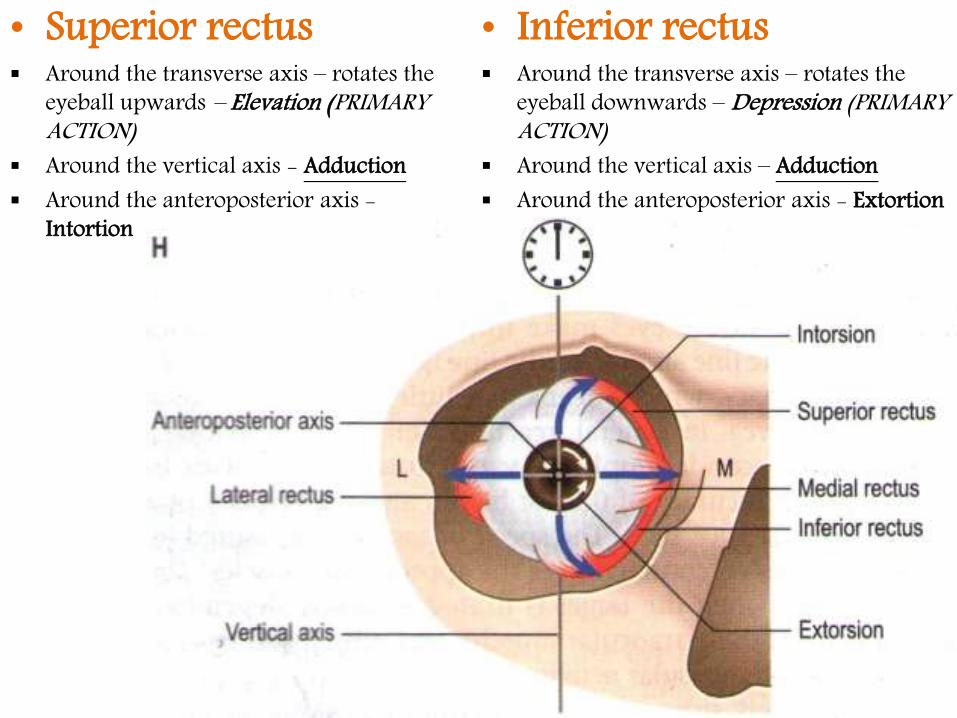
• Superior rectus Around the transverse axis – rotates the
eyeball upwards – Elevation (PRIMARY ACTION)
Around the vertical axis - Adduction Around the anteroposterior axis -
Intortion
• Inferior rectus Around the transverse axis – rotates the
eyeball downwards – Depression (PRIMARY ACTION)
Around the vertical axis – Adduction Around the anteroposterior axis - Extortion
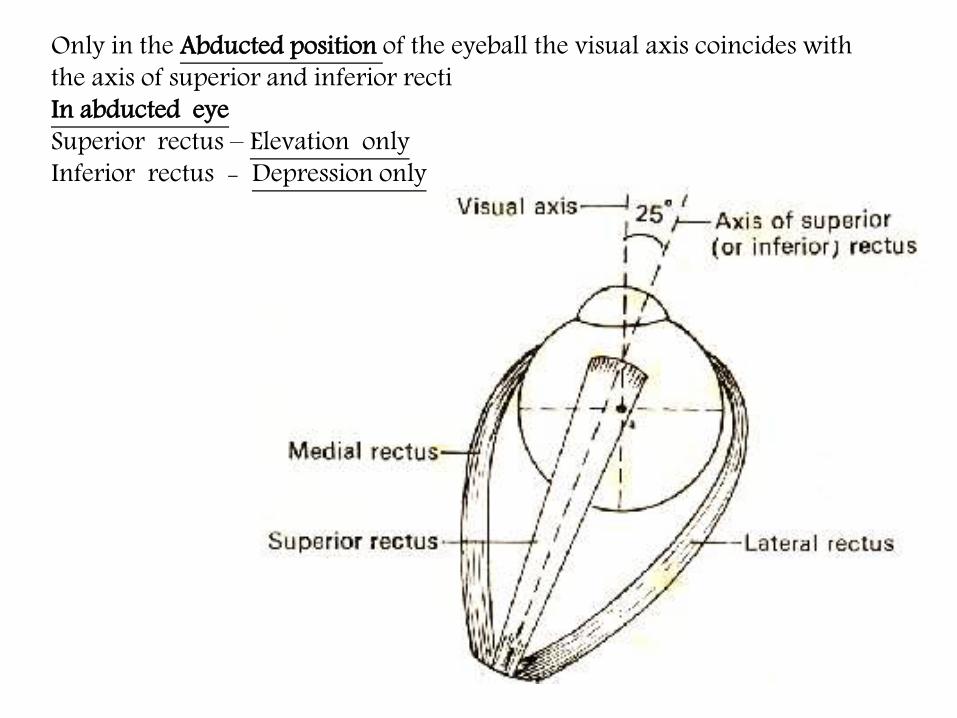
Only in the Abducted position of the eyeball the visual axis coincides with the axis of superior and inferior rectiIn abducted eyeSuperior rectus – Elevation onlyInferior rectus - Depression only

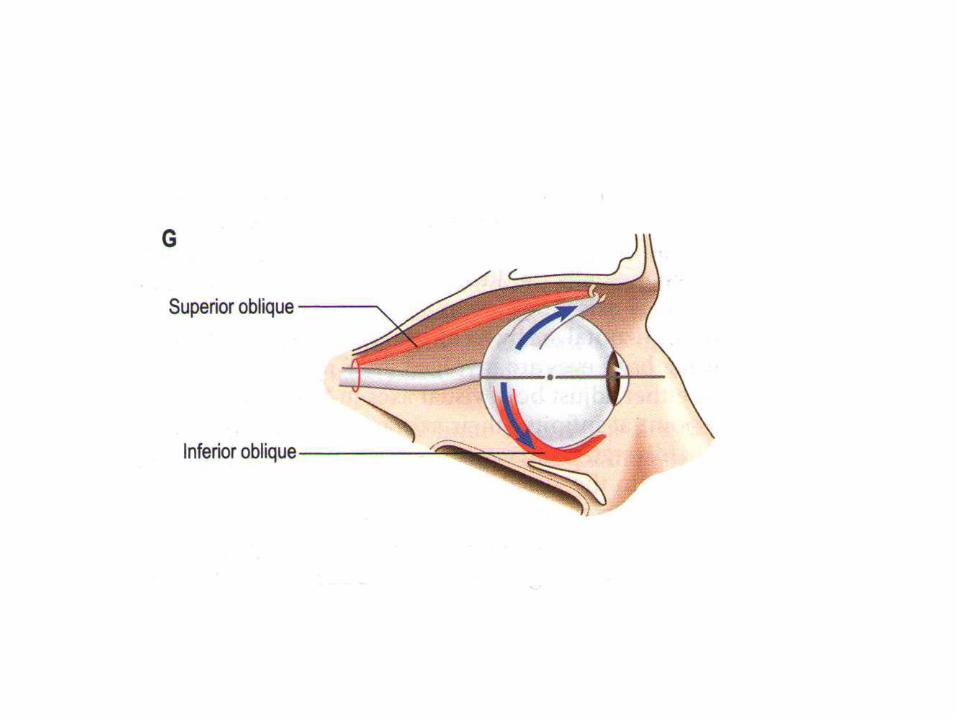
Superior Oblique muscleBody of sphenoid above and medialto optic canal
Winds around trochlea at superomedial part of orbit(functional origin)
Insertion behind the equatorPostero‐superior quadrant
Only eye muscle innervated on the outer surface of muscle belly.
Retrobulbar anaesthetic block

Origin from orbital surface of maxilla
Passes backward and laterally below inferior rectus
Insertion behind equator parallel to superior obliquePostero‐superior quadrant
Inferior Oblique Muscle
The oblique muscles always course below the corresponding vertical rectus muscle

Axis of the Oblique MusclesThe obliques lie in the same oblique plane 51⁰medial to optical axis
In the adducted eye axes coincide with the optical axis

• Superior oblique Around the anteroposterior axis –
Intorsion(primary action) Around the vertical axis Abduction Around the transverse eaxis –
Depression
• Inferior oblique Extortion(primary action) Abduction Elevation
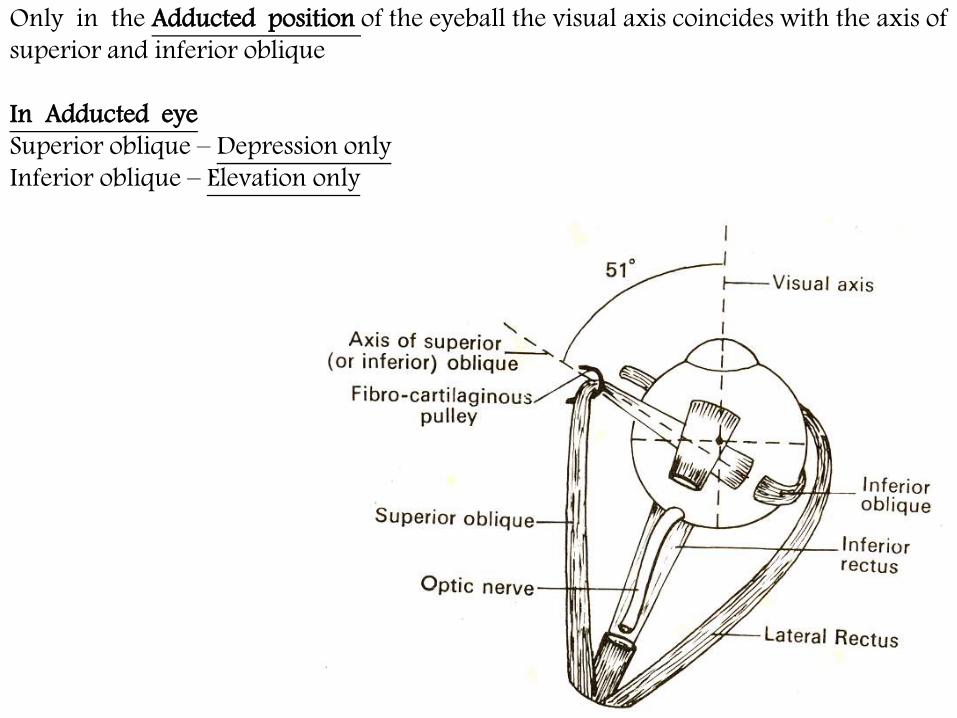
Only in the Adducted position of the eyeball the visual axis coincides with the axis of superior and inferior oblique
In Adducted eyeSuperior oblique – Depression onlyInferior oblique – Elevation only

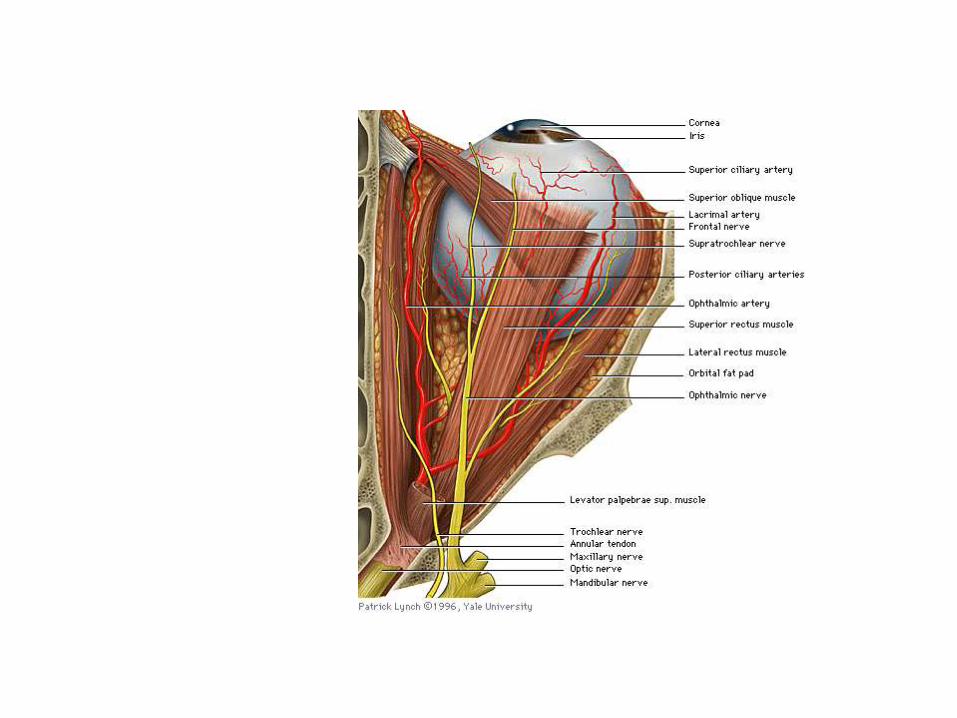
Superior division of oculomotor:- levator palpebrae superioris, superior rectusInferior division of oculomotor:- medial rectus, inferior oblique, inferior rectusTrochlear nerve - superior obliqueAbducent nerve - lateral rectus
Nerve Supply of Extraocular Muscles

Blood supplyOphthalmic artery
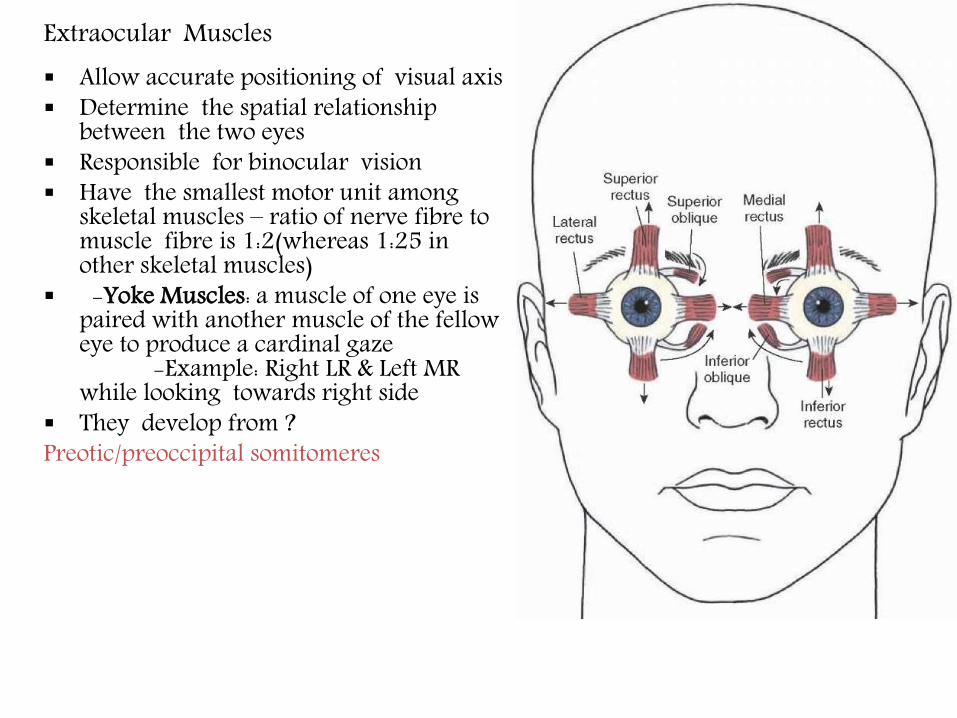
Extraocular Muscles Allow accurate positioning of visual axis Determine the spatial relationship
between the two eyes Responsible for binocular vision Have the smallest motor unit among
skeletal muscles – ratio of nerve fibre to muscle fibre is 1:2(whereas 1:25 in other skeletal muscles)
-Yoke Muscles: a muscle of one eye is paired with another muscle of the fellow eye to produce a cardinal gaze
-Example: Right LR & Left MR while looking towards right side
They develop from ?Preotic/preoccipital somitomeres

Fascial expansions of Extraocular muscles

RECTI -AdductOBLIQUES – AbductSUPERIORS – IntortINFERIORS -Extort

Clinical Testing
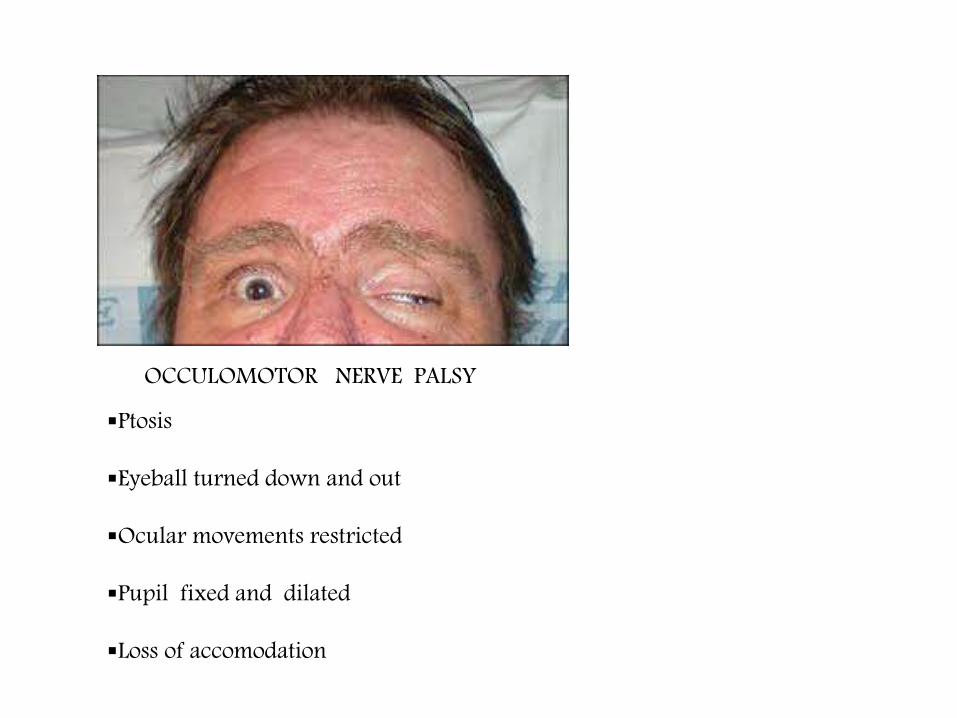
Ptosis
Eyeball turned down and out
Ocular movements restricted
Pupil fixed and dilated
Loss of accomodation
OCCULOMOTOR NERVE PALSY
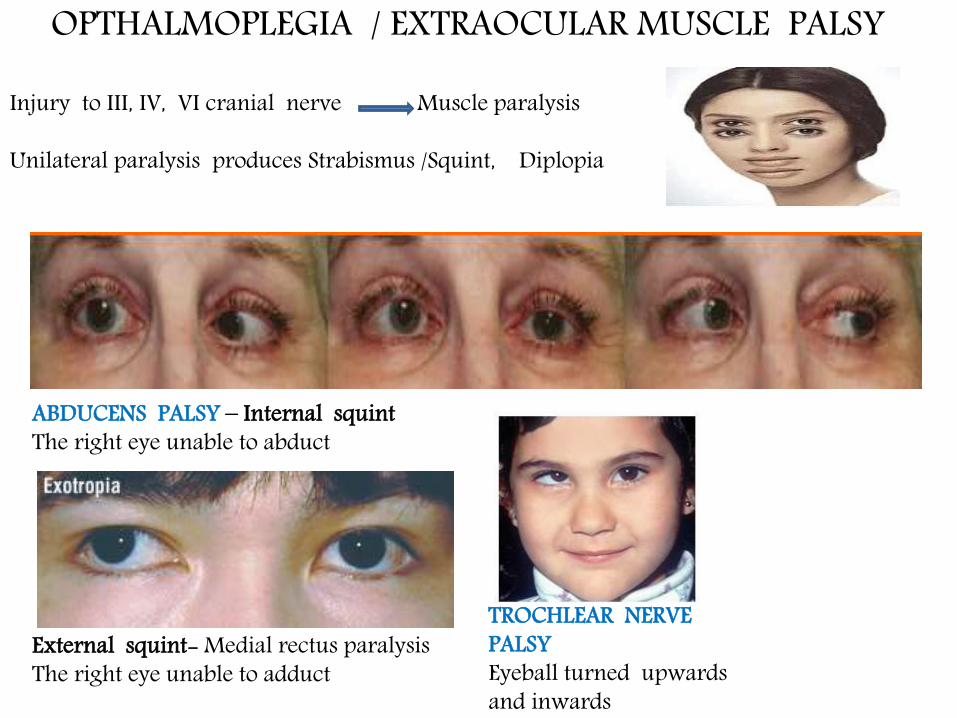
ABDUCENS PALSY – Internal squintThe right eye unable to abduct
External squint- Medial rectus paralysisThe right eye unable to adduct
OPTHALMOPLEGIA / EXTRAOCULAR MUSCLE PALSY
Injury to III, IV, VI cranial nerve Muscle paralysis
Unilateral paralysis produces Strabismus /Squint, Diplopia
TROCHLEAR NERVE PALSYEyeball turned upwards and inwards



TROCHLEAR NERVE PALSY
Affected eye rotated up and in.
Attempts to compensate lead to the patient tilting their head to the contralateral side.

ABDUCENS PALSY





Third nerve palsy results in an inability to move the eye normally in all directions. Injury to the third nerve can occur anywhere along its path, from where it originates within the brain to where it innervates the muscles that move the eyeball. Third nerve palsy prevents the proper functioning of the medial, superior, and inferior recti, and inferior oblique muscles. As a result, the eye cannot move up, down, or in. When at rest, the eye tends to look down and to the side, due to an inequality of muscle functioning. The muscle responsible for keeping the upper eyelid open (levatorpalpebrae superioris) is also affected, resulting in a drooping upper eyelid (ptosis


Movements
Elevation
Depression
Adduction
Abduction
Intortion extortion

phthalmoplegia, also called extraocular muscle palsy, paralysis of the
extraocular muscles that control the movements of the eye. Ophthalmoplegia usually involves the third (oculomotor), fourth (trochlear), or sixth (abducens)cranial nerves. Double vision is the characteristic symptom in all three cases


The optical axis of the eye (the line from the center of the cornea to the fovea) points straight ahead during straight-ahead gaze, but the axis of the orbit points about 23 degrees laterally. The superior and inferior rectioriginate from the back of the orbit, and so their direction of pulling is not parallel to the optical axis. As a result, although the superior rectus primarily elevates the eye, it also has smaller adducting and intorting effects. (Similarly, although not indicated in the Þgure, the inferior rectus primarily depresses but also adducts and extorts a little.)

The pulling direction of the obliques is not aligned with either the optical axis or the orbital axis, and their actions change with the direction of gaze. The superior oblique inserts in the posterior half of the eye and pulls diagonally forward. A, As a result, during straight-ahead gaze, although it primarily intorts the eye, it also pulls the back of the eye a little bit medially and upward (i.e., abducts and depresses a little). B, During adduction, the direction of pull is more nearly in line with the optical axis, and the same muscle depresses more and intorts less. C, During abduction, the direction of pull can wind up perpendicular to the optical axis, and the action becomes purely intorsion. (Similarly, although not indicated in the Þgure, the inferior oblique primarily extorts when the eye is abducted, but it also elevates and abducts in other directions of gaze.)

