external quality assurance in clinical trace element labs
TRANSCRIPT
11
BMTA, Teddington, 20th October 2015
Dr Chris Harrington
Deputy Director
SAS Trace Element Laboratory,
Surrey Pathology Services (SPS)
External Quality Assurance (EQA) in
Clinical Trace Element Laboratories
Overview of Presentation
• What are trace elements and why do
we measure them clinically?
• EQA in clinical laboratories – the
Barnes report 2003
• UKNEQAS for Trace Elements
Scheme run from Guildford
• ISO 17043:2010 accreditation vs CPA
• Real World EQA - hip replacements
3
Why Trace Elements ?
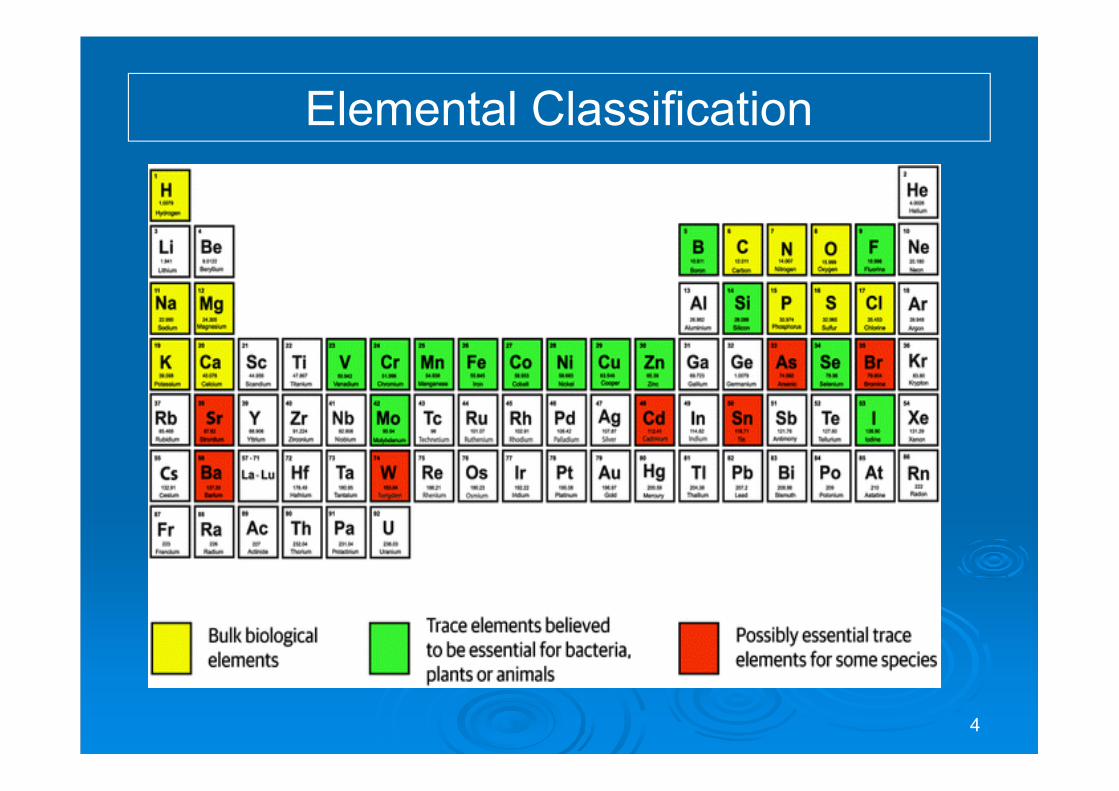
Elemental Classification
4
5
Trace Elements
� Significance:
� 14 elements are essential for bacteria, plants and
animals (including humans);
• transition elements V, Cr, Mn, Fe, Co, Ni, Cu, Mo, Zn;
• metalloids B, Si and Se;
• halogens F and I.
� Why?:
� There are three main reasons for their measurement in
a clinical-nutritional setting:
� To determine deficiency or toxicity.
� As a screening method for failing hip replacements
6
EQA in Clinical Laboratories
Clinical EQA
• Clinical science was one of the first disciplines to use
EQA and implement schemes in the hospital laboratory.
• The first proficiency survey of UK clinical pathology
laboratories was reported in 1953 and revealed a wide
spectrum of results for the common tests.
• In 1969, the National Quality Control Scheme was
initiated by the Wolfson Research Laboratories,
Birmingham
– Involved the distribution of specimens every 14 days.
• Now known as the UK National External Quality
Assessment Scheme (UKNEQAS) and is responsible
for about 30 different schemes.
• Other centres operate under the UKNEQAS structure.
Rationale
• EQA is the cornerstone of quality assurance and
laboratory accreditation in clinical testing laboratories.
• Ensures that the results of patient investigations are
reliable and comparable wherever they are produced.
• It is used to highlight poor performing laboratories.
• Where poor performance is highlighted schemes work
with the laboratory to improve testing.
• Schemes have a role to educate participants.
• Where this is unsuccessful participants will suspend
their service until good performance is restored.
Ian Barnes Report 2003
• The Review assessed current NHS quality assurance
frameworks and governance mechanisms for
pathology services.
• It gathered a diverse range of evidence; examining
expectations of pathology services; identifying areas
for improvement
• It recommended strengthening and standardising the
current quality assurance structures
– RCPath Joint Working Group for Quality Assessment
(JWGQA)
– co-ordinates and oversees the standards and performance of
EQA schemes for all schemes
10
UKNEQAS for Trace Elements
History and Development
• Established (1979) with a monthly distribution to UK
hospitals measuring Cu and Zn in serum.
• Growth in participants and inclusion of additional
analytes and specimen types (1979 – 1984).
• EU funded serum Al programme (1986) for
laboratories monitoring patients with Chronic Renal
Failure.
• UK DoH links scheme to UK NEQAS for referral of
poor performers to Clinical Chemistry Advisory Panel.
• Link formally established by the Advisory Committee
on Analytical Laboratory Standards in 1988.
• Introduction of ISO15189:2012 places emphasis on
EQA participation with ISO accredited schemes.
Rationale
• The aims of the scheme are consistent with the
intentions of UK NEQAS, to:
• Provide professionally-led and scientifically-based
scheme with a primarily educational objective.
• Provide regular distributions of specimens, 2 per
month of each matrix blood, serum and urine.
• Provide rapid feedback of performance.
• Support participants where problems occur.
• Stimulate the overall improvement in performance
among all participating laboratories.
• 153 participants from 27 countries.
• 49 participants in the UK.
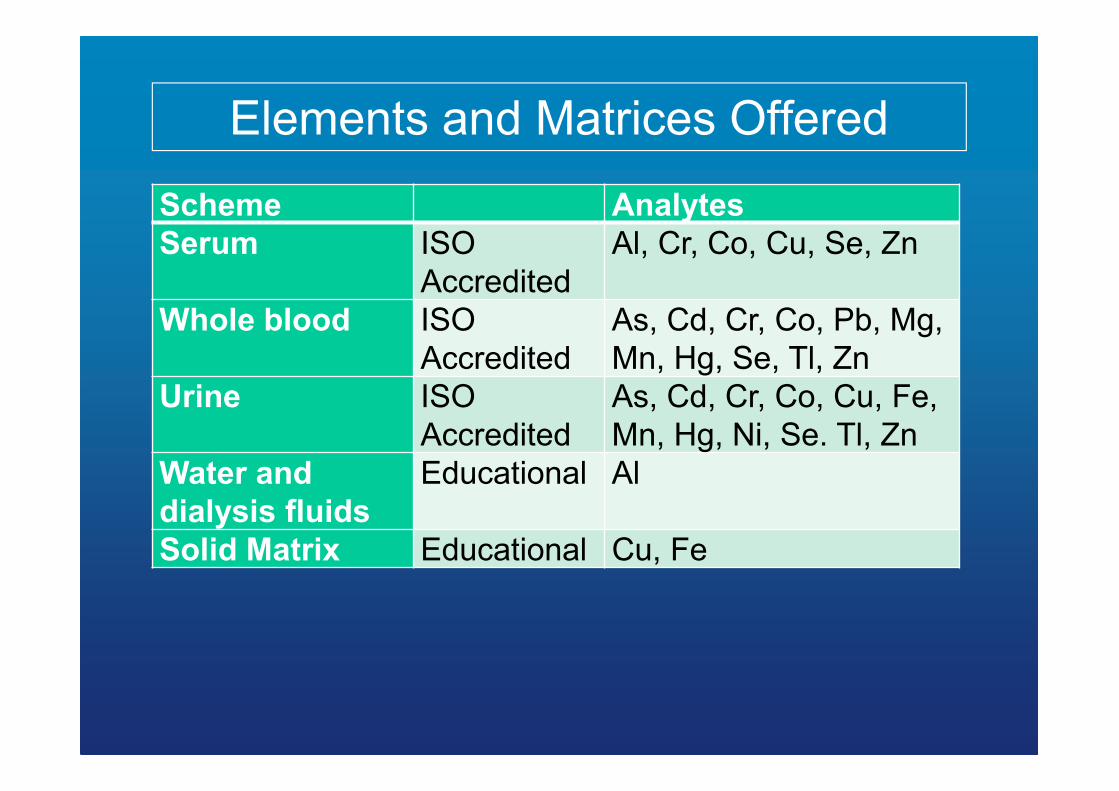
Elements and Matrices Offered
Scheme Analytes
Serum ISO
Accredited
Al, Cr, Co, Cu, Se, Zn
Whole blood ISO
Accredited
As, Cd, Cr, Co, Pb, Mg,
Mn, Hg, Se, Tl, Zn
Urine ISO
Accredited
As, Cd, Cr, Co, Cu, Fe,
Mn, Hg, Ni, Se. Tl, Zn
Water and
dialysis fluids
Educational Al
Solid Matrix Educational Cu, Fe
14
Scheme Operation
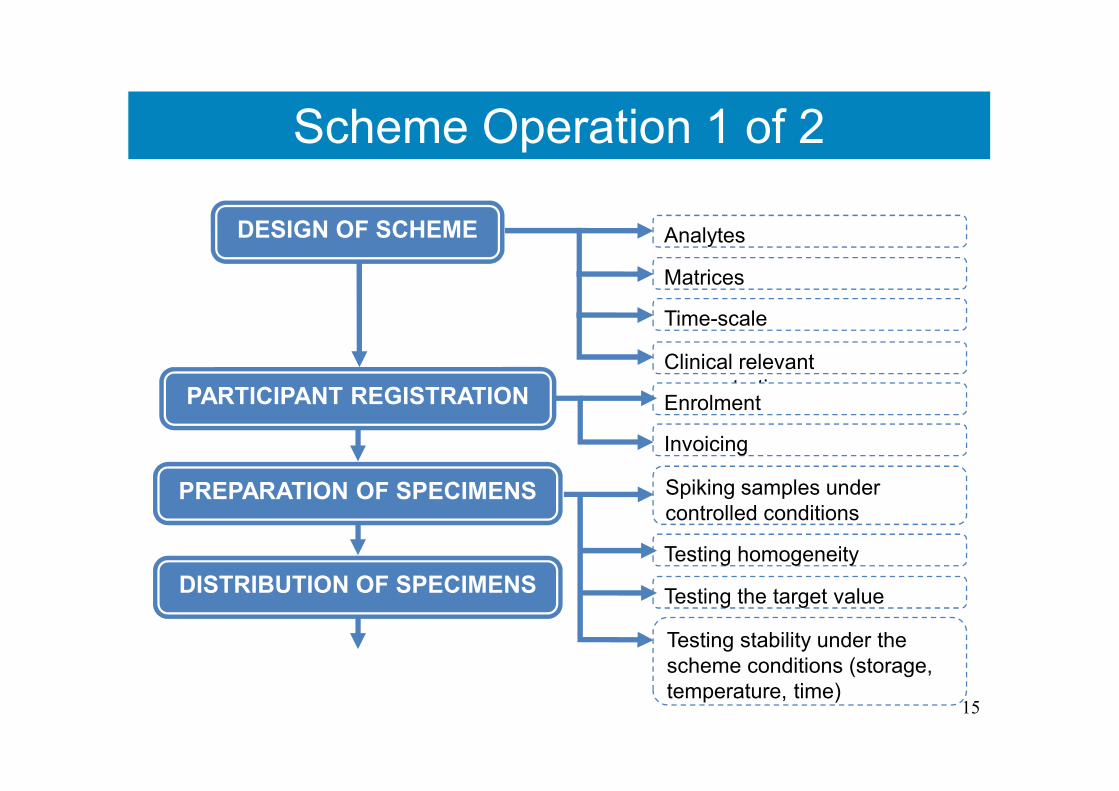
Scheme Operation 1 of 2
15
DESIGN OF SCHEME Analytes
Matrices
Clinical relevant
concentrations
Time-scale
PARTICIPANT REGISTRATION Enrolment
Invoicing
PREPARATION OF SPECIMENS
Testing homogeneity
Testing the target value
Spiking samples under
controlled conditions
Testing stability under the
scheme conditions (storage,
temperature, time)
DISTRIBUTION OF SPECIMENS
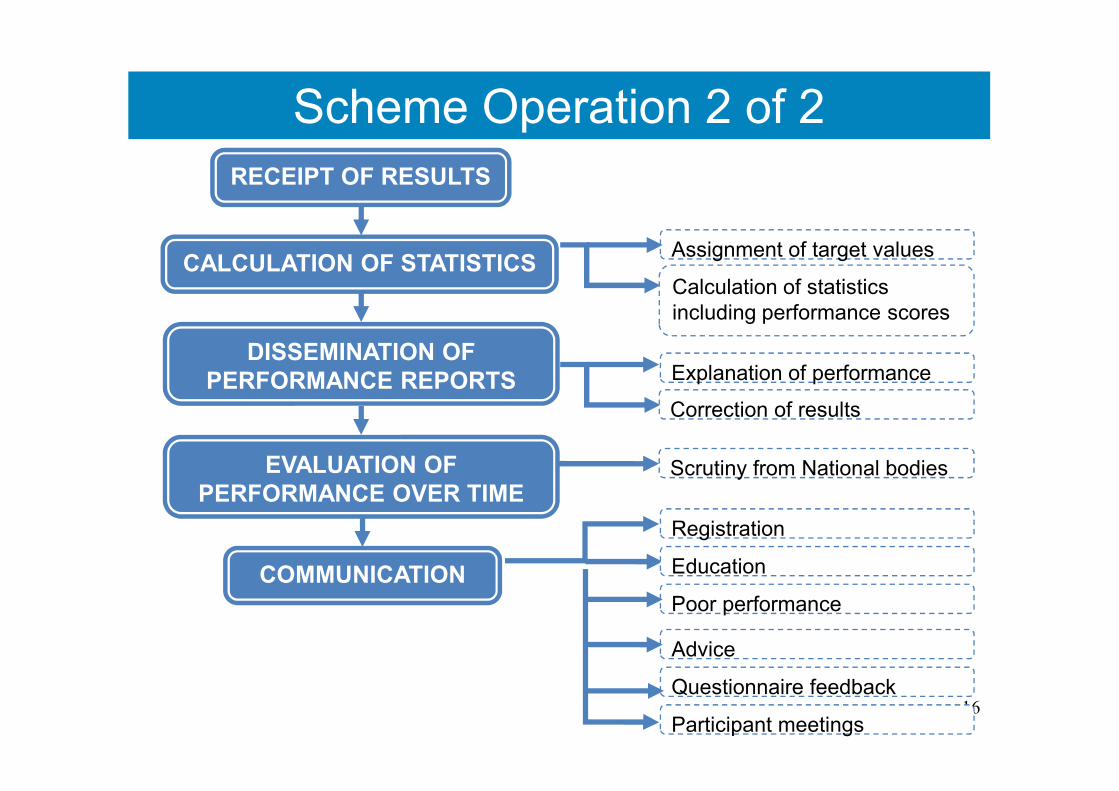
Scheme Operation 2 of 2
16
RECEIPT OF RESULTS
CALCULATION OF STATISTICSAssignment of target values
Calculation of statistics
including performance scores
DISSEMINATION OF
PERFORMANCE REPORTS Explanation of performance
Correction of results
EVALUATION OF
PERFORMANCE OVER TIMEScrutiny from National bodies
COMMUNICATION Education
Poor performance
Questionnaire feedback
Advice
Registration
Participant meetings
Evaluation of Performance
Measurements of performance are based on deviations of
results from target values. These deviations are used to
calculate a Z-score.
As EQA has developed, various organisations have
produced best practice documents.
Those from authoritative international bodies include:
• ISO 17043 (Conformity assessment - General
requirements for proficiency testing).
• ISO 13528 (Statistical methods for use in proficiency
testing by interlaboratory comparisons).
• IUPAC (The international harmonized protocol for the
proficiency testing of analytical chemistry laboratories,
Pure Appl. Chem. 2006; 78: 145–196, 2006). .
Evaluation of Performance
ISO and IUPAC recommend assessment of performance based on a
Z-score (or a derivative which takes uncertainty into consideration):
Z-score = x - X / SDPTwhere x = laboratory result
X = target value
SDPT = standard deviation for proficiency testing
• The ‘std dev for proficiency testing’ is set by the
scheme organiser.
• Value that will allow the score to demonstrate whether
or not performance is fit for the purpose.
• Set so that a Z-score of up to ±2 indicates acceptable
performance.
• Score of more than ±3 indicates unsatisfactory
performance.
Evaluation of Performance
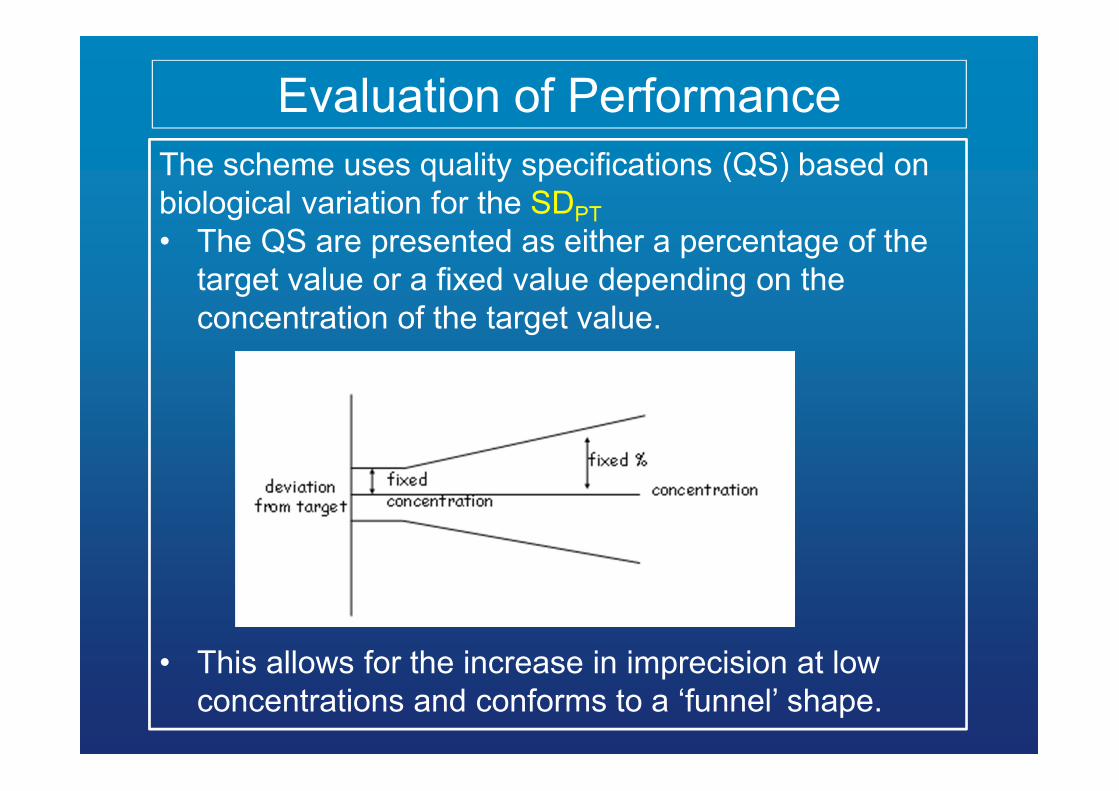
The scheme uses quality specifications (QS) based on
biological variation for the SDPT
• The QS are presented as either a percentage of the
target value or a fixed value depending on the
concentration of the target value.
• This allows for the increase in imprecision at low
concentrations and conforms to a ‘funnel’ shape.
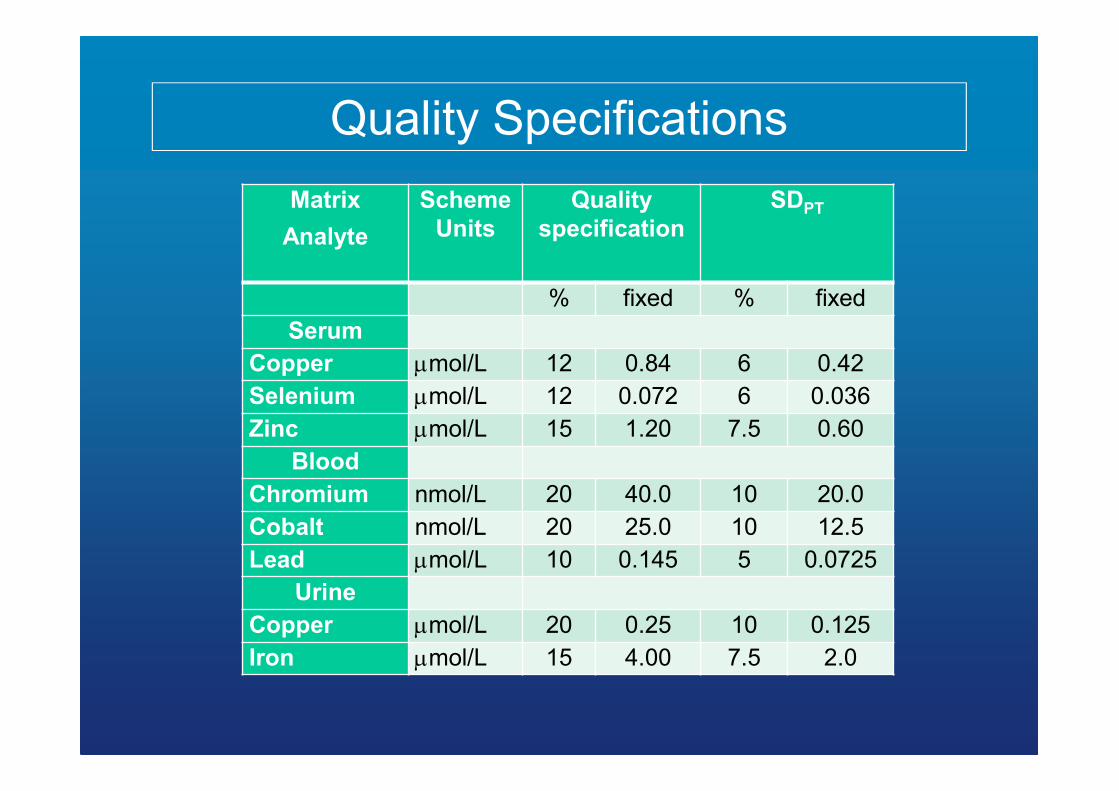
Quality Specifications
Matrix
Analyte
Scheme
Units
Quality
specification
SDPT
% fixed % fixed
Serum
Copper µmol/L 12 0.84 6 0.42
Selenium µmol/L 12 0.072 6 0.036
Zinc µmol/L 15 1.20 7.5 0.60
Blood
Chromium nmol/L 20 40.0 10 20.0
Cobalt nmol/L 20 25.0 10 12.5
Lead µmol/L 10 0.145 5 0.0725
Urine
Copper µmol/L 20 0.25 10 0.125
Iron µmol/L 15 4.00 7.5 2.0
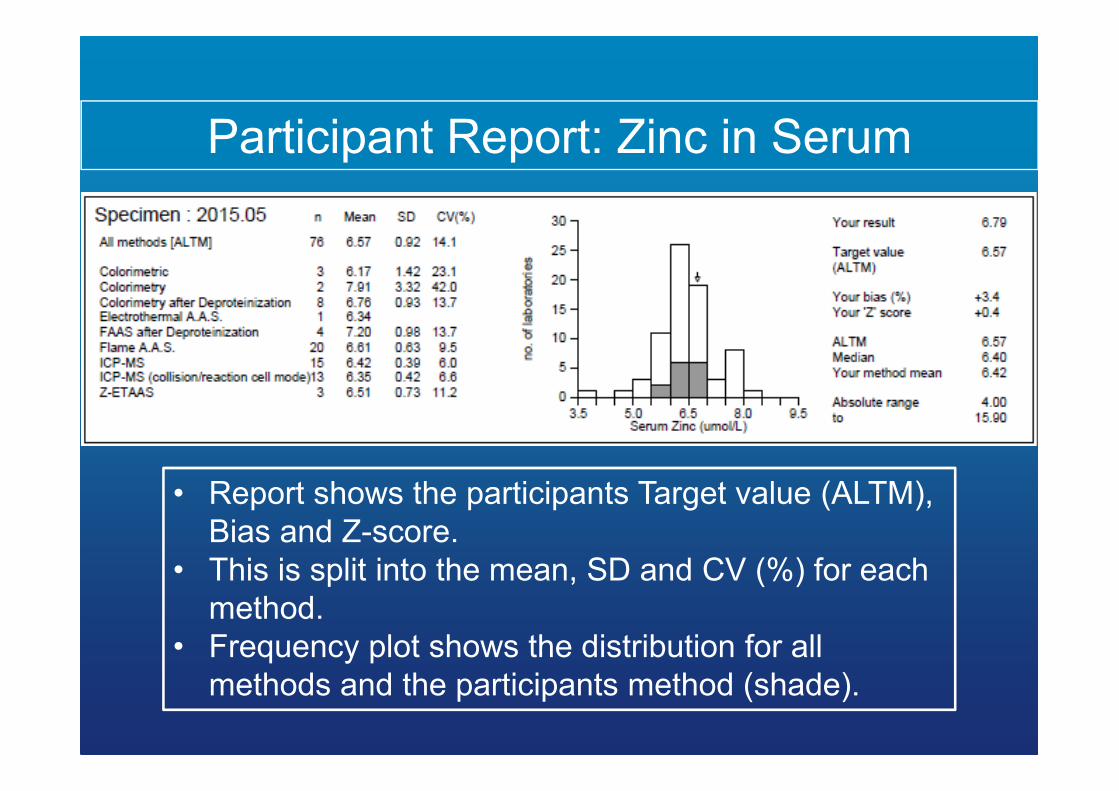
Participant Report: Zinc in Serum
• Report shows the participants Target value (ALTM),
Bias and Z-score.
• This is split into the mean, SD and CV (%) for each
method.
• Frequency plot shows the distribution for all
methods and the participants method (shade).
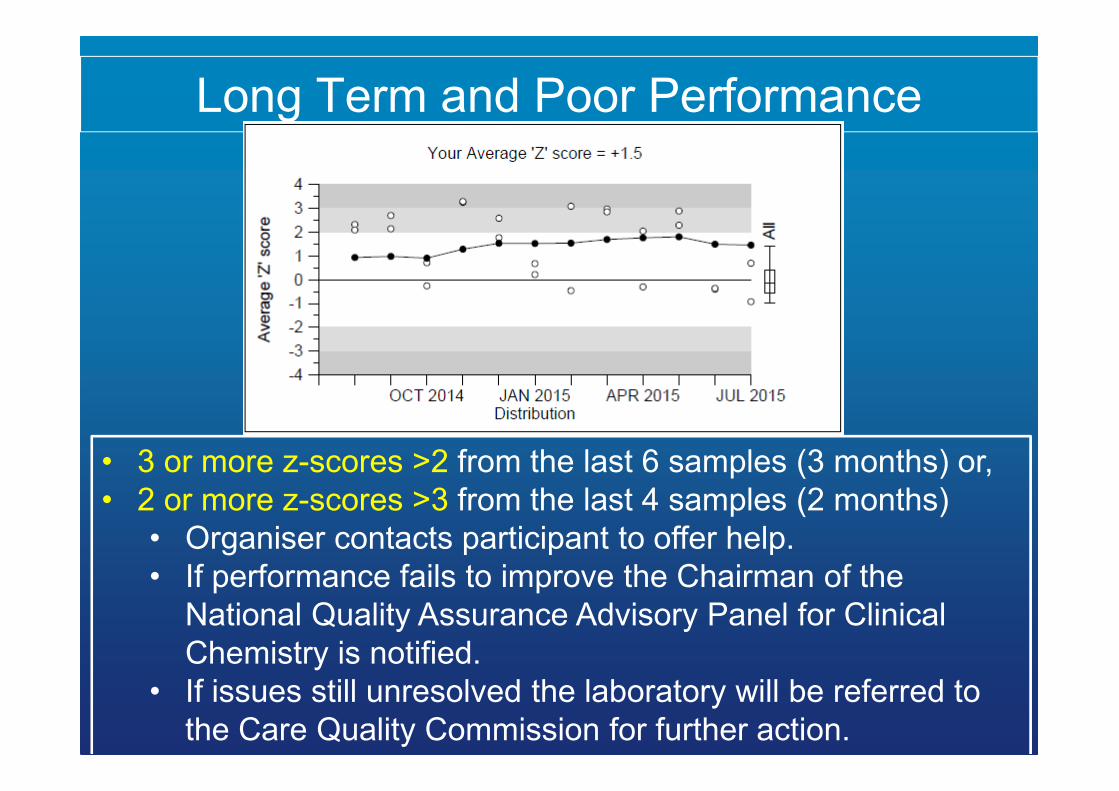
Long Term and Poor Performance
• 3 or more z-scores >2 from the last 6 samples (3 months) or,
• 2 or more z-scores >3 from the last 4 samples (2 months)
• Organiser contacts participant to offer help.
• If performance fails to improve the Chairman of the
National Quality Assurance Advisory Panel for Clinical
Chemistry is notified.
• If issues still unresolved the laboratory will be referred to
the Care Quality Commission for further action.
23
Accreditation: ISO vs CPA
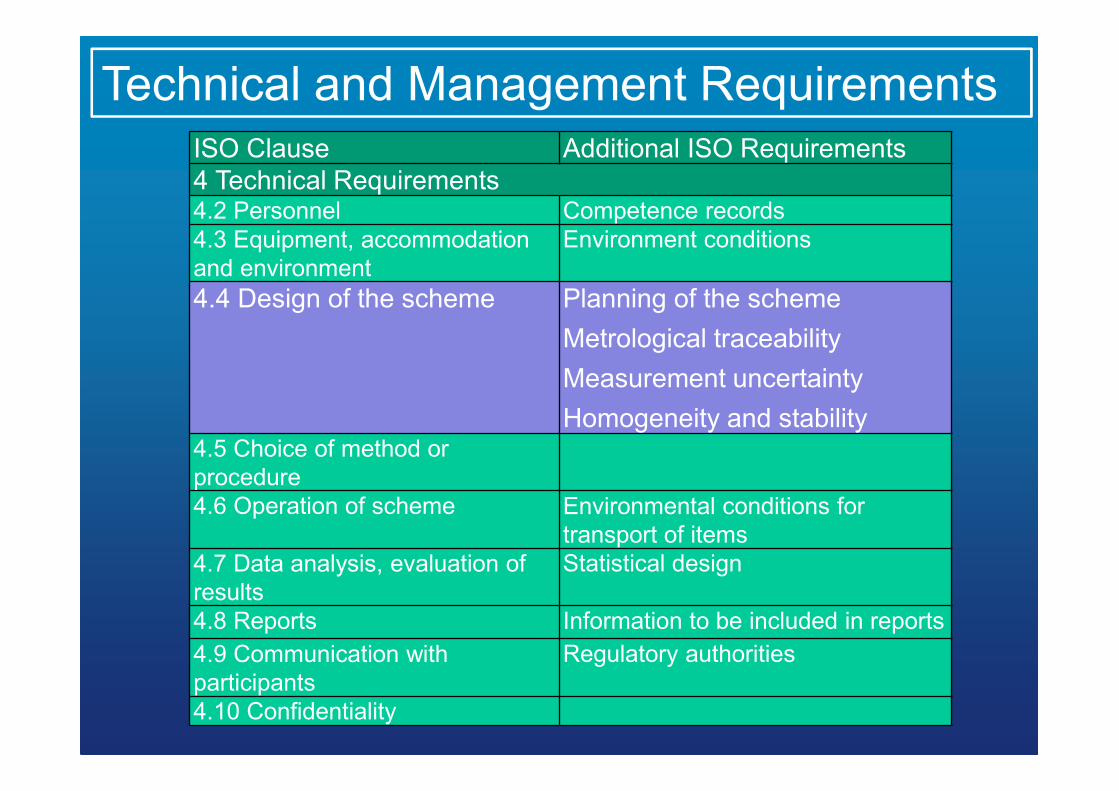
ISO Clause Additional ISO Requirements
4 Technical Requirements4.2 Personnel Competence records
4.3 Equipment, accommodation
and environment
Environment conditions
4.4 Design of the scheme Planning of the scheme
Metrological traceability
Measurement uncertainty
Homogeneity and stability4.5 Choice of method or
procedure
4.6 Operation of scheme Environmental conditions for
transport of items
4.7 Data analysis, evaluation of
results
Statistical design
4.8 Reports Information to be included in reports
4.9 Communication with
participants
Regulatory authorities
4.10 Confidentiality
Technical and Management Requirements
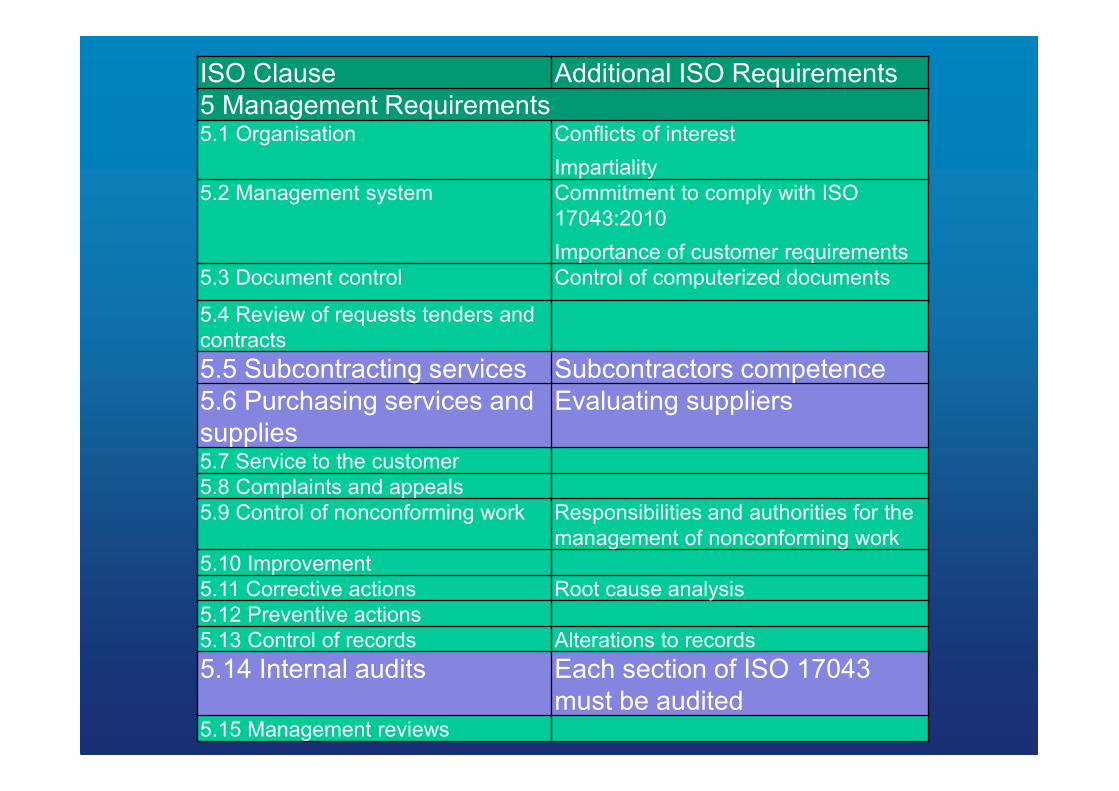
ISO Clause Additional ISO Requirements
5 Management Requirements5.1 Organisation Conflicts of interest
Impartiality
5.2 Management system Commitment to comply with ISO
17043:2010
Importance of customer requirements
5.3 Document control Control of computerized documents
5.4 Review of requests tenders and
contracts
5.5 Subcontracting services Subcontractors competence
5.6 Purchasing services and
supplies
Evaluating suppliers
5.7 Service to the customer
5.8 Complaints and appeals
5.9 Control of nonconforming work Responsibilities and authorities for the
management of nonconforming work
5.10 Improvement
5.11 Corrective actions Root cause analysis
5.12 Preventive actions
5.13 Control of records Alterations to records
5.14 Internal audits Each section of ISO 17043
must be audited5.15 Management reviews
26
Real World Clinical EQA:
Hip Replacements
27
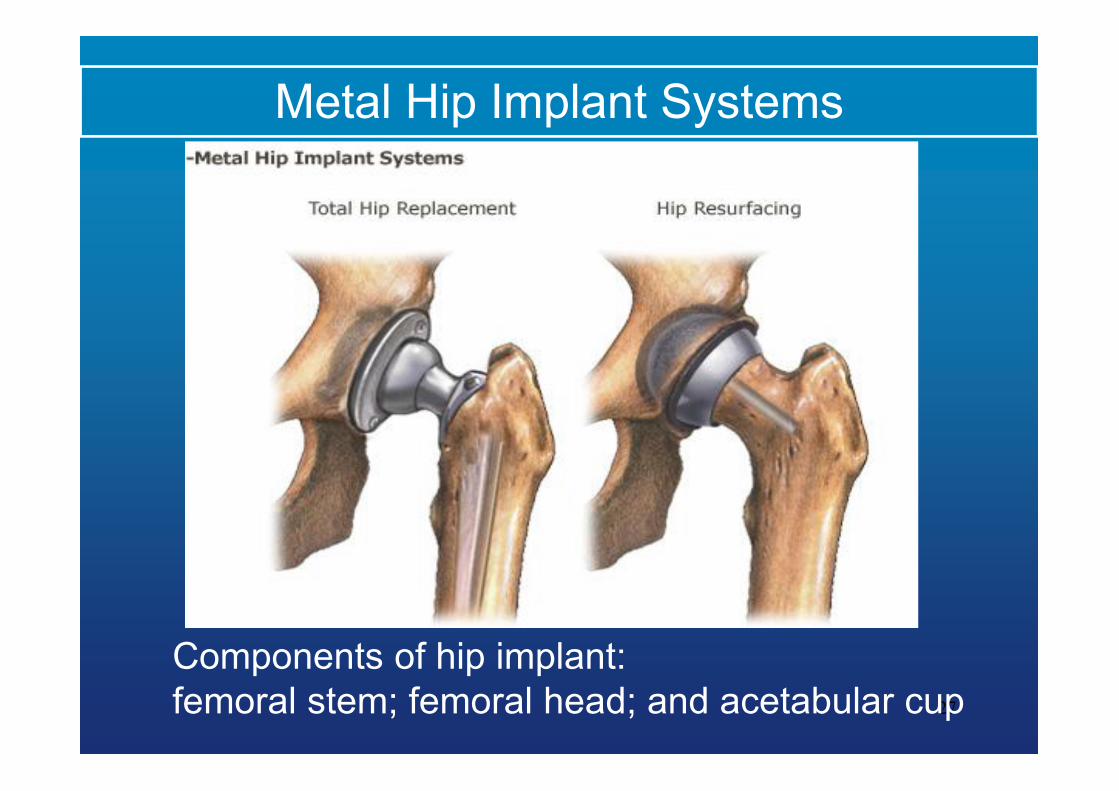
Metal Hip Implant Systems
Components of hip implant:
femoral stem; femoral head; and acetabular cup
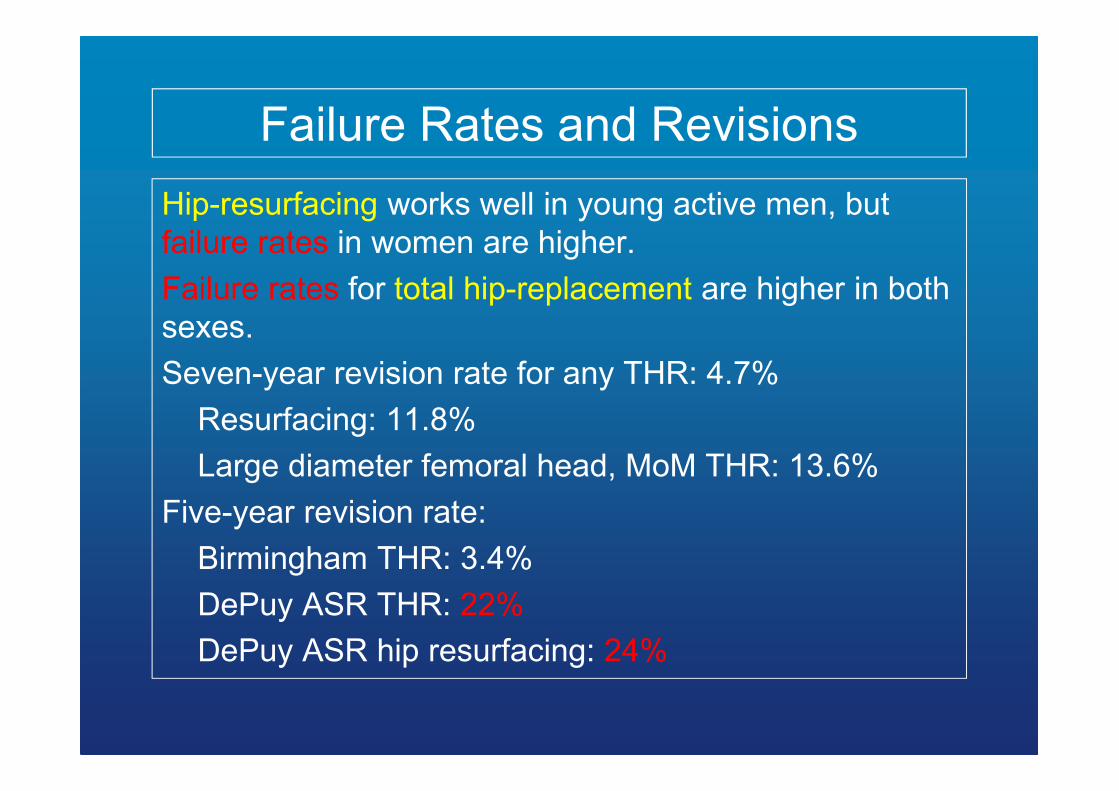
Failure Rates and Revisions
Hip-resurfacing works well in young active men, but
failure rates in women are higher.
Failure rates for total hip-replacement are higher in both
sexes.
Seven-year revision rate for any THR: 4.7%
Resurfacing: 11.8%
Large diameter femoral head, MoM THR: 13.6%
Five-year revision rate:
Birmingham THR: 3.4%
DePuy ASR THR: 22%
DePuy ASR hip resurfacing: 24%
29
The Regulator
• April 2010 MHRA issued an advisory notice
regarding MoM hip replacements:
• Follow up annually for 5 years post operatively.
• “put in place systems for the follow up of patients
receiving MoM hip replacements where appropriate
blood metal ion measurements and sectional
imaging”.
• If either Co or Cr levels are elevated above 7 ppb
then further testing should be performed.
• MHRA alerts stated that labs should be part of
UKNEQAS for Trace Elements scheme.
• Orthopedic consultants were unsure of test results
from one year to the next.
• Q”how do I know any change in value is not due to
the testing labQ”
• The scheme decided to look back over participant
performance between April 2011 and March 2012
for Co and Cr in whole blood EQA specimens.
• Results obtained by the participants (n = 23) were
assessed.
• The concentrations ranged from 10 to 60 µg L-1 for
Co and 10 to 35 µg L-1 for Cr.
• Letter published in British Medical Journal – BMJ 2012; 344:e4017
The Clinicians
• The mean recovery for the analysis of all 20 specimens:
• Co was 96.4% (SD 2.2, CV% 2.3)
• Cr was 96.1% (SD 3.2, CV% 3.3).
• The excellent agreement between the amounts in the
specimens (endogenous plus spike) and the mean
values indicates that results reported are accurate.
• The agreement between the pools distributed on
different occasions shows that results are also
reproducible.
• These results should reassure surgeons and patients
that the laboratories carrying out the measurement of Co
and Cr are producing results that are fit for purpose.
Long Term Performance
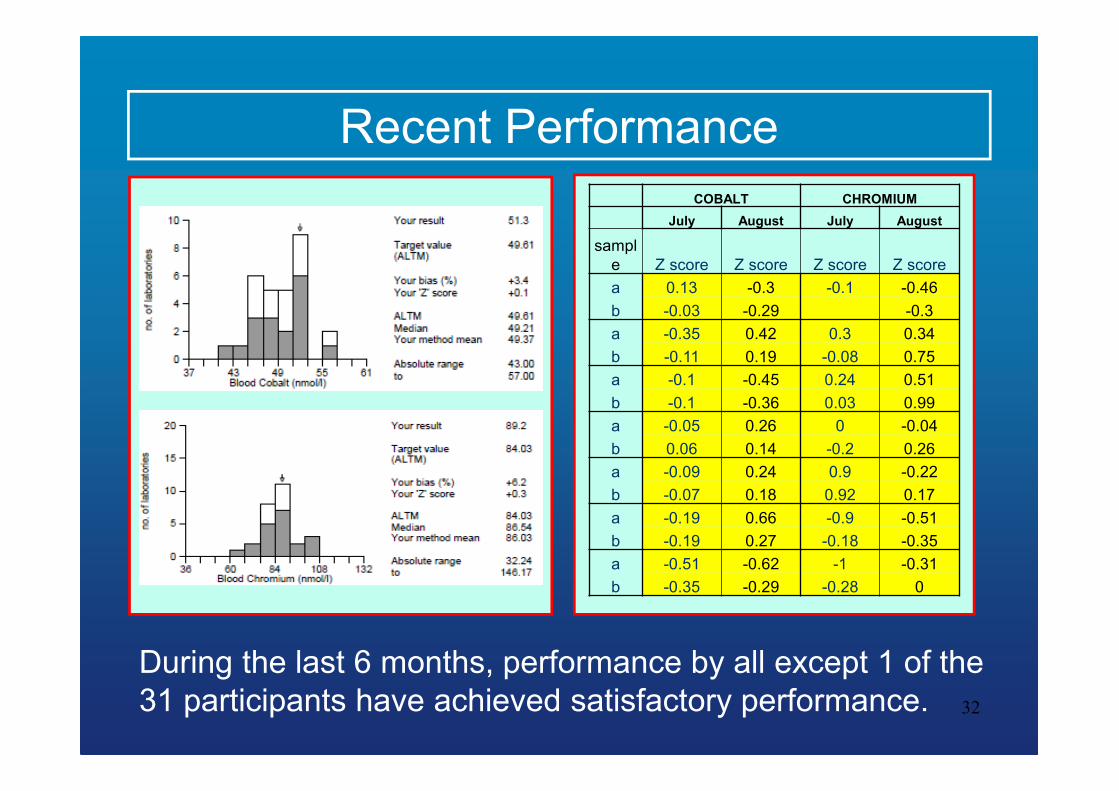
Recent Performance
32
COBALT CHROMIUM
July August July August
sampl
e Z score Z score Z score Z score
a 0.13 -0.3 -0.1 -0.46
b -0.03 -0.29 -0.3
a -0.35 0.42 0.3 0.34
b -0.11 0.19 -0.08 0.75
a -0.1 -0.45 0.24 0.51
b -0.1 -0.36 0.03 0.99
a -0.05 0.26 0 -0.04
b 0.06 0.14 -0.2 0.26
a -0.09 0.24 0.9 -0.22
b -0.07 0.18 0.92 0.17
a -0.19 0.66 -0.9 -0.51
b -0.19 0.27 -0.18 -0.35
a -0.51 -0.62 -1 -0.31
b -0.35 -0.29 -0.28 0
During the last 6 months, performance by all except 1 of the
31 participants have achieved satisfactory performance.
Summary
• EQA is paramount to clinical laboratories.
• The aim is to improve performance by regular testing
and education, referral through professional bodies as
a fall back.
• Accreditation of laboratories to ISO ISO15189:2012
places emphasis on EQA participation with ISO
accredited schemes.
• Performance evaluation requires an understanding of
biological and analytical variation.
• Many clinical examples showing EQA helps clinicians
make decisions about the treatment of patients.
34
Acknowledgements
• Andrew Taylor, Director UKNEQAS for Trace
Elements, Guildford, UK.
• Sarah-Jane Bainbridge, EQA Quality Manager,
Surrey Pathology Services, UK.
• Thermo X2-Series ICP-MS and iCAP ICP-OES
funded by UK National Health Service and
Department of Health.
The organisers for inviting me.